Noninvasive Tests
Electrocardiography is one of the two oldest, most widely used, and least expensive tests in the diagnosis of heart disease. The electrocardiogram , developed for practical use at the turn of the century, records the electrical potential generated by each heartbeat. The contraction and relaxation of the heart muscle is caused by a flow of electrolytes (sodium, potassium, and calcium) in and out of each muscle cell through the surrounding membrane. This flow generates a week electrical current. Each muscle cell of the heart is a miniature battery discharging electricity with each contraction (depolarizing), and recharging itself during relaxation (repolarizing). The electrocardiograph is an amplifier capable of picking up this weak current from the surface of the body. The electrical potential generated over time by the millions of heart muscle cells—between 0.1 and 2.0 millivolts, or about one millionth the voltage of household current—displayed continuously on a roll of graph paper, is the standard electrocardiogram. It consists of 12 leads recorded with electrodes placed on various points on the chest, both arms, and the left leg, thus providing electrical "views" of the heart from various angles.
An electrocardiographic image produced by a single heartbeat is shown in figure 12. Any deviation from the horizontal line, or baseline , whether above (positive potential ) or below (negative potential ), denotes electrical activity. Each change of potential is called a wave . The first is a positive, broad, triangular wave called the P wave , representing depolarization of the two atria and signaling their contraction. It is followed by a return to the baseline, called the P-R interval . Next comes a complex consisting of three sharp waves: a small, negative Q wave , a tall, positive R wave , and a small, negative S wave . These three waves together constitute the QRS complex , which shows depolarization of the two ventricles
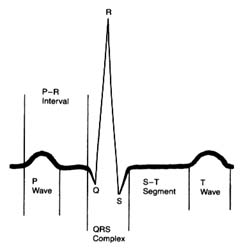
Figure 12. A typical electrocardiographic lead showing the various
components of the electrocardiogram.
coinciding with the onset of ventricular contraction. A flat, electrically inert baseline follows (the S-T segment ), after which the slower and lower T wave appears, indicating repolarization of the two ventricles. The section of the electrocardiogram including the QRS complex, the S-T segment, and the T wave is referred to as the ventricular complex . The end of the T wave is referred to as the ventricular complex . The end of the ventricular contraction occurs during the descending part of the T wave. Absence of electrical activity is displayed by the horizontal baseline between the end of the T wave and the beginning of the P wave of the next beat, during which time the ventricles relax.
The normal electrocardiogram shows a sequence of evenly spaced complexes. Experience has established the limits of normal variation in the height and direction of the five waves in healthy persons according to age group. The abnormal electrocardiogram may indicate two types of deviation from these norms: abnormalities of the sequence of beat (arrhythmias) and abnormalities of the waves and the baseline segments between them (abnormalities of electrocardiographic contour). The normal heart beats evenly at a rate ranging between 60 and 150 beats a minute. Irregular spacing of heartbeats demonstrates an arrhythmia, a disturbance of the rhythm of the heart. The electrocardiogram is the principal tool for
diagnosing cardiac arrhythmias, since it shows the rate and regularity of heartbeats; the shape, direction, and relationship of the P waves to the other complexes, including the absence of P waves; and deviations in the contour of the QRS complexes and T waves in the abnormally spaced beats.
The electrocardiogram is an indispensable tool in recognizing and analyzing arrhythmias. An equally important role of the electrocardiogram is to provide information concerning the state of the heart muscle on the basis of certain alterations in the electrocardiographic complexes, especially the QRS-T part. This feature of the electrocardiogram, however, requires more cautious interpretation because alterations produced by changes in the heart muscle are less specific than those produced by arrhythmias. Alterations in the electrocardiogram helpful to the physician may result from myocardial infarction and from enlargement of one or both cardiac ventricles or atria. These changes tend to be a permanent feature of a given person's electrocardiogram. In addition, daily and hourly variations may suggest acute changes in the state of the heart muscle, such as ischemia, acute pericarditis, and imbalance of electrolytes. In some healthy persons electrocardiograms may deviate from the norm without indicating any heart problem; these are referred to as normal variants. By contrast, many electrocardiographic abnormalities—perhaps the majority—are inconclusive, or "nonspecific." Here the significance of the changes has to be evaluated by means other than the electrocardiogram.
Electrocardiography is the most universally and frequently used aid in the diagnosis of heart disease. Yet it has its limitations: a normal electrocardiogram can be present in patients with a serious heart problem, and an abnormal electrocardiogram does not automatically indicate significant heart disease.
Electrocardiographic techniques are also incorporated in certain other cardiac tests. The treadmill stress test helps evaluate the effect of increased work on the heart by monitoring it electrocardiographically while the patient exercises on a treadmill. The principal indication for this test is a suspicion of coronary-artery disease, which may reduce the oxygen supply to some part of the heart muscle (ischemia) during exercise. Occasionally exercise may provoke arrhythmias (see chap. 8), and this test is used to detect them. The Holter monitor test is a 24-hour survey of heart rhythm. The
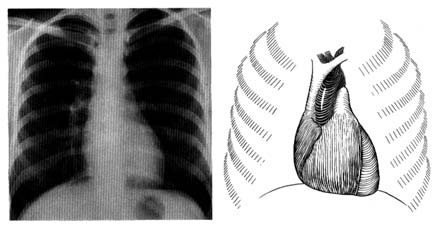
Figure 13. A radiograph (X-ray) of the chest in the anteroposterior view in a healthy person (left).
A reference diagram (right) shows the heart and the great vessels in relation to the rib cage.
Compare with figure 2 to identify cardiovascular structures.
patient wears a specialized tape recorder that registers every heartbeat. A computer analysis of the recording reveals any disturbances of heart rhythm. Newer, high-fidelity recording equipment may pick up indications of ischemia of the heart muscle. The electrocardiogram is an important aid in diagnosing some acute diseases of the heart or monitoring the heart during surgical procedures (cardiac or noncardiac). In such cases the heart rhythm is sensed by one or two electrocardiographic leads and is displayed continuously on an oscilloscope. This procedure is standard in intensive-care wards, including coronary-care units.
Radiography is the second traditional diagnostic aid in heart diseases. Because X rays penetrate certain tissues better than others, X-ray photography permits considerable differentiation of body structures. The chest X ray displays three types of shadows: the heavy shadow of bony structures (spine, ribs), the light shadow of lungs filled with air, and the intermediate shadow of the heart and blood vessels (fig. 13).
Radiographic examination can display enlargement of the heart and the great vessels arising from it as well as the distribution of blood vessels throughout the lungs. Newer technology (especially echocardiography) provides a more accurate method of recognizing
enlargement of the individual heart chambers or other structures in the X-ray shadow of the heart. Today cardiac radiography is used more as a screening technique and a means of assessing changes occurring between examinations than as a way of definitively diagnosing cardiac enlargement. This test, however, is indispensable in displaying fluid in the lungs, an important feature of heart failure. (Current technology has produced some specialized radiological techniques in diagnosing heart disease. These will be discussed later in the chapter in connection with invasive tests.)
Blood tests usually play an important role in diagnosing diseases, but not in the case of heart ailments. Only three sets of blood tests are a regular part of diagnostic work in cardiology: measurement of cardiac enzymes in acute myocardial infarction; measurement of cardiac drug levels in the blood to regulate dosage; and blood culture for discovery of bacteria if infection of the heart is suspected.
Echocardiography has revolutionized the diagnosis of heart disease since it was first applied in the 1960s. Like other ultrasound techniques, it produces an image by transmitting high-frequency sound waves (ultrasound), which reflect off different structures of the body with varying intensity; the resulting data show the interface of those structures.
In the original echocardiographic technique, an electronic wand—a transducer—is pressed against the patient's chest and pointed in the direction of the heart, toward which it sends ultrasonic waves. The heart muscle, its neighboring structures, and cavities filled with blood vary in density, and the transducer picks up those variations in the reflected sound, which it converts into an electronic signal that is recorded on moving paper. The echocardiographic record shows not only changes in the size of the cardiac chambers during ventricular contraction and relaxation but also the rapidity of contraction and relaxation—points of some importance in evaluating heart function. This method, M-mode echocardiography , displays a one-dimensional view of the portion of the heart at which the transducer is aimed. It is often referred to as the "icepick" view of the heart because the narrow sound beam drives straight through the heart like an icepick through a solid block (fig. 14). M-mode echocardiographic display provides some information that previously required invasive tests, such as the size (width) of each heart chamber, the thickness of the muscle
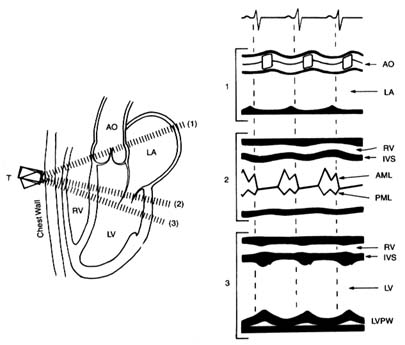
Figure 14. A normal M-mode (unidimensional) echocardiographic image.
The left side of the diagram presents three standard directions of the ultrasonic
beam, with cardiac structures identified. The right side shows a record of
the echocardiographic images in each position as recorded on moving paper.
Abbreviations: AO, aorta; LA, left atrium; RV, right ventricle; LV, left ventricle;
IVS, interventricular septum; AML, anterior leaflet of the mitral valves; PML,
posterior leaflet of the mitral valves; LVPW, posterior wall of the left ventricle.
(Reprinted, by permission, from Arthur Selzer, Principles and Practice
of Clinical Cardiology [Philadephia: W. B. Saunders, 1983].)
of the ventricle, change in the size of the left ventricle between systole and diastole (the rate of change reflects its efficiency), the presence of fluid between the two layers of the pericardium, and the presence of abnormal structures (clots, tumors) within the cavities of the heart.
In the late 1970s a new technology was developed in the field of echocardiography permitting two-dimensional imaging. Instead of sending a single ultrasonic beam, the transducer now sends an oscillating series of beams along a single plane shaped like a large
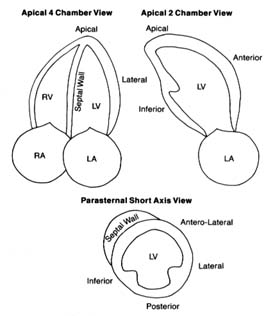
Figure 15. The three standard views of two-dimensional echocardiographic images.
The various structures are identified, including five segments of the left ventricular
walls. The images are recorded on a videotape, which permits viewing cardiac structure
in real-time motion. Abbreviations: LV, left ventricle; LA, left atrium; RV, right ventricle;
RA, right atrium. (Reprinted, by permission, from Arthur Selzer, Principles and
Practice of Clinical Cardiology [Philadelphia: W. B. Saunders, 1983].)
slice of pie (60° to 90° of a circle). The information obtained from these echoes is processed by computer, then displayed on an oscilloscope and recorded on videotape. This technique has widened the application of echocardiography by displaying details of the interior of the heart and its various parts in motion in real time (fig. 15). It allows the cardiologist to detect abnormalities in the size, shape, and mode of contraction of each cardiac chamber, in the contraction of specific portions of the ventricular muscle, and in the thickness of cardiac valves and the size of their opening. It also can reveal
clots, vegetations, or tumors inside the heart and aid in the diagnosis of certain congenital abnormalities of the heart.
Further technological advances have applied the Doppler effect to echocardiography as a means of studying blood flow through the heart. This physical principle describes the effect of motion on sound waves: a person listening to a sound will perceive a rise in pitch if the source of the sound is approaching and a fall in pitch if the source is receding. In echocardiography the Doppler effect lets us measure the velocity of blood flow toward or away from the transducer. On the videotape these changes in velocity and direction of blood flow are displayed as variations in color. Doppler echocardiography can show the presence and approximate volume of backflow through incompetent heart valves. It also aids in evaluating shunts through abnormal communications within the heart in some types of congenital heart disease and in gauging the severity of stenosis (narrowing) of a cardiac valve as well as approximate pressures in certain parts of the heart and great vessels. Doppler echocardiography has introduced an entirely new approach to noninvasive diagnosis: whereas conventional echocardiography opened up the field of noninvasive diagnosis of structural abnormalities of the heart, Doppler echocardiography has made it possible to evaluate the dynamics of blood flow through the heart.
Another echocardiographic technique is transesophageal echocardiography , in which the transducer is placed at the end of a tube similar to that used in endoscopic examination of the stomach and esophagus. This tube is swallowed by the patient, and the transducer is lowered to the level of the heart. Since the esophagus lies immediately behind the heart, the beam does not have to pass through outer structures of the chest. Transesophageal echocardiography is thus capable of displaying images in much greater detail than conventional echocardiography. The procedure has its disadvantages, however; it cannot properly be considered noninvasive, and it causes the patient some discomfort. This technique is sometimes used to monitor the heart and its responses during certain open-heart operations. Its value in diagnostic work has not yet been completely defined, but at present it is used to evaluate some special problems when conventional techniques are inconclusive.
Echocardiography has radically altered the approach to diagnosing
heart disease. However, it is a very expensive test; hence it is used to evaluate specific problems and is not included in a routine examination. Many problems previously requiring complex invasive tests can now be adequately reviewed by echocardiography.
Other diagnostic tools involve injecting radioactive substances into the bloodstream. Such testing is the responsibility of a separate medical specialty, nuclear medicine . Although the field got its start in the 1920s, the primary application of nuclear techniques to heart disease was in research until the 1970s, when diagnostic tests were developed. Today nuclear cardiology is used extensively in diagnosis as well as research. Two important tests are myocardial isotopic perfusion imaging , in connection with exercise or pharmacological stress tests, and nuclear ventriculography , a method of studying the contraction and relaxation of the ventricles.
Perfusion tracer agents such as thallium-201 or Technetium 99m Sestamibi are injected into the bloodstream and enter the heart muscle along with the coronary blood flow. The radioactivity disappears within a few days. Their presence in the heart muscle can be detected by a special camera. Thus, if a portion of the heart muscle is receiving less blood or is totally deprived of blood, it will show in the photographs as an area of lighter contrast or as a blank space.
The myocardial stress perfusion test discriminates between areas of the heart muscle permanently deprived of blood supply and those rendered temporarily ischemic (fig. 16). It is usually performed in connection with a treadmill test. Just before the end of the exercise, the liquid containing the thallium isotope is injected into the bloodstream. It may be performed by using a drug stress, such as diphridamole or adenosine, in patients who are unable to do a treadmill stress test. A symmetrical, full distribution of radioactive isotopes indicates good blood supply to the heart. If an area of abnormally reduced flow is found, another count is performed four hours later (occasionally a third count is taken 24 hours later). If the defect in the image remains unchanged, the physician can conclude that the area is permanently deprived of blood flow, probably a scar from a previous myocardial infarction. If, however, the abnormality has disappeared, the proper diagnosis is ischemia, temporary blockage of blood supply, usually owing to significant coronary-artery disease.
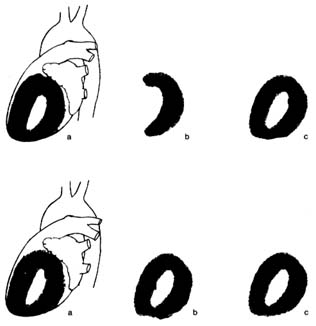
Figure 16. Thallium perfusion scintigram (image of thallium content of the
heart used in thallium treadmill stress tests). The upper row shows a test
positive for myocardial ischemia; the lower row shows results of such a test in a
healthy person. (a) Lateral thallium image of the left ventricle superimposed on
the heart. (b) Thallium images taken immediately after exercise. The upper
drawing shows a large defect (absence of blood flow) of the anterior wall of the
heart. The lower drawing shows normal perfusion. (c) Thallium images taken
four hours after the exercise test, showing restoration of blood flow to a normal
level. If the defect in the upper row present in b would persist in c, the test
would be interpreted as showing a scar from past myocardial infarction rather
than myocardial ischemia.
Nuclear ventriculography is a method of recording the motion of the heart chambers. The blood is made temporarily radioactive by injecting into the bloodstream an isotope with a very short half-life (a few hours). The isotope in the blood lining the cavities of the cardiac chambers permits observation, on videotape, of the heart in motion during the cardiac cycle. The function of each ventricle can be assessed from the extent of the motion of its walls. The test helps in calculating an important index of ventricular function, the ejection fraction , the ratio of the blood ejected during systole to the greatest volume of the ventricle in diastole. In addition, if the
motion of the ventricular wall is abnormal, the test can reveal whether the entire ventricle is contracting sluggishly or only some parts of it. This wall motion abnormality is central to the diagnosis of coronary-artery disease.
The field of diagnostic imaging—cardiac imaging in particular—shows rapid advances. New isotopes are being developed in radiopharmacology that may refine the diagnostic value of present methods and introduce new tests. Most of the new techniques are first applied in research; only if their value in diagnosing individual cases of heart disease is demonstrated do they become generally available. The new technologies often require complex equipment costing millions of dollars. Two imaging techniques are widely used. Computed axial tomography (CAT scan ) is an X-ray technique that allows the photographing of two-dimensional "slices" through parts of the body. The resulting image is assembled and enhanced by computer. At present, the CAT scan has little application in diagnosing abnormalities of the heart itself, but it is of value in addressing certain problems of the great vessels or the pericardium. Magnetic resonance imaging generates images of internal body structures by picking up changes in cells produced by exposure to a powerful magnet. This method, too, is limited in its application to cardiac diagnosis, though it may reveal tumors of the heart and abnormalities of the pericardium. Further developments in imaging are now being tested for research purposes, such as magnetic resonance spectroscopy and positron emission tomographic imaging, both of which may help in studying metabolic changes in the heart muscle and may lead to improvements in diagnosing special cardiac problems.