Chapter One
The Normal Heart:
Structure
General Definitions
The circulatory apparatus is a closed system filled with blood, consisting of the heart and blood vessels; it is the principal supply line between various organs and parts of the body. The circulation delivers fuel to the body, namely oxygen and other essential substances; it also removes carbon dioxide and other products of metabolism. Blood is circulated in two separate circuits: the smaller circuit is known as the lesser circulation or the pulmonary circulation ; and the larger circuit, the greater circulation or the systemic circulation . The former supplies the lungs, the latter all other organs of the body. Figure 1 is a diagrammatic outline of the circulation, showing the lesser circulation above the heart and the greater circulation below the heart.
The central organ of the circulatory system is the heart . It consists of two separate pumps, one for each circuit, simultaneously ejecting an equal quantity of blood into the greater and the lesser circulation. The heart is a muscular organ weighing approximately 300 gm, which contracts rhythmically about 70 times a minute and with each beat expels about 75 cc of blood into each circuit. Each system of blood vessels into which the blood is pumped consists of three parts: the arterial system , the capillary system , and the venous system , as shown in figure 1. The objective of the lesser circulation is to send blood through the vessels of the lungs and there to bring it into close contact with the air, so that oxygen can
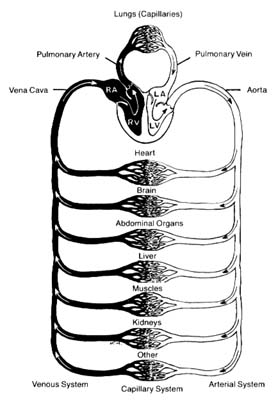
Figure 1. General diagram of the circulation showing the
pulmonary circuit above the heart and the systemic circuit
below the heart. Oxygenated blood is shown in white
and deoxygenated blood in black.
be replenished and carbon dioxide removed; thus the blood in the pulmonary artery (leading to the lungs) has a low oxygen content and high carbon dioxide content, whereas blood returning from the lungs in the pulmonary veins has a high oxygen content and low carbon dioxide content. The objectives of the greater circulation are as follows: to deliver oxygen to the tissues; to pick up and deliver all nourishing substances, vitamins, hormones, and other vital compounds; to carry carbon dioxide, the "exhaust" of the tissues, to the right side of the heart and hence to the lungs for elimination; and to pick up other waste products and deliver them to the points of their excretion or elimination (kidneys, liver, etc.).
Oxygen is the most essential fuel for every tissue of the body. Its utilization is intimately connected with carbon dioxide, the principal waste product of tissues. Thus each cell in the body "breathes" by extracting oxygen from the blood and depositing carbon dioxide in its place. Blood destined for the tissues, fully saturated with oxygen and containing a lower quantity of carbon dioxide, is bright red. It is ordinarily referred to as arterial blood , as it is contained in the arteries of the greater circulation. Blood returning from the tissues has a lower oxygen content and is high in carbon dioxide; such blood, dark red in color, is termed venous blood , as it is contained in the veins of the greater circulation. It shines through the superficial veins under the skin, making them appear blue. It is clear from figure 1 that the terms "arterial blood" (indicated as white in the chart) and "venous blood" (indicated as black) apply only to the greater circulation. In the pulmonary circulation, as I have said, the role of arteries and veins is reversed. Figure 1 emphasizes the fact that the pulmonary circuit consists of a simple system of vessels supplying a single organ; the greater circulation, by contrast, consists of a great number of semiautonomous systems connected parallel to each other. Each organ of the body receives blood from arterial branches, which then divide into capillary branches. The actual exchange of all substances between the blood and tissues occurs within the capillary system.
Structure of the Heart
The heart is a muscular, conical organ located in the center of the chest, slightly more to the left than to the right (fig. 2). It has an apex, directed downward and leftward, and a base at its upper part where major vessels originate. The heart consists of three layers: an inner lining (endocardium ); the heart muscle (myocardium ); and the outer covering (pericardium ). The pericardium itself has two layers: the outer lining of the heart (epicardium ), which is firmly attached to it, giving the surface of the heart a smooth, glistening appearance; and a loose sac (parietal pericardium ), in which the heart is suspended. This parietal pericardium is shown in figure 2, where the front portion of it has been removed in order to display details of the frontal aspect of the heart. Between the two layers of
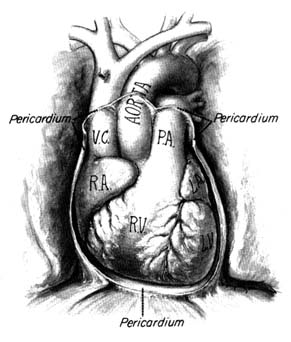
Figure 2. Frontal aspect of the heart with the parietal pericardium
removed. Abbreviations: V.C. = superior vena cava;
R.A. = right atrium; R.V. = right ventricle; P.A. = pulmonary artery.
the pericardium there is a small amount of fluid (pericardial fluid ) which acts as a lubricant, facilitating motion of the heart within the pericardial sac.
The heart is a hollow organ comprising four chambers: two atria (the correct term "atrium" is often used interchangeably with the older term "auricle") and two ventricles . The thin-walled atria act as receptacles for the blood returning to the heart; the thick-walled ventricles, consisting of several layers of muscle, constitute the pump proper. The two atria and the two ventricles are separated from each other by partitions called septa (sing. septum ). As mentioned, the heart is a twin pump: the right side (right atrium and right ventricle) handles venous blood, the left side (left atrium and left ventricle) arterial blood. The independent function of the two sides of the heart is often acknowledged by referring to them as the "right heart" and the "left heart." The respective locations of the
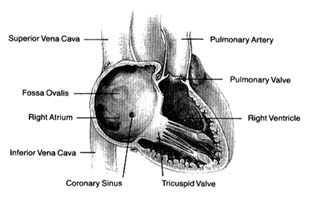
Figure 3. Right side of the heart shown with the front wall removed.
four chambers, as they appear when looking at the front surface of the heart, are shown in figure 2.
Venous blood enters the right atrium through two large veins and a small vein. The large veins, the superior vena cava and the inferior vena cava , channel blood from the upper and lower parts of the body, respectively. The third channel, the coronary sinus , delivers venous blood from the heart itself. The right atrium and its three tributary channels are shown in figure 3. The right atrium is an irregularly shaped chamber connecting, by way of a large opening, with the right ventricle. This orifice is protected by the tricuspid valve . The two large veins enter the atrium at its upper and lower right portions, respectively. The coronary sinus empties into the right atrium at its lower back wall. The mixture of blood derived from the three channels flows into the right ventricle through the tricuspid orifice. The right ventricle is divided into two portions: the lower portion, or inflow tract (behind the tricuspid valve); and the upper portion, or outflow tract, leading to the pulmonary orifice. At the top of the conical outflow tract is the pulmonary artery, separated from the tract by the outflow valve of the right side of the heart—the pulmonary valve (fig. 4). The contents of the right ventricle are ejected into the pulmonary artery, destined for the lungs.
The left side of the heart is almost identical in structure to the right side. The left atrium contains the orifices of four pulmonary veins, two of which drain blood from each lung. This atrium is
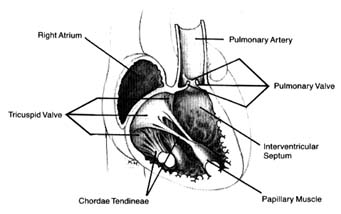
Figure 4. Details of the tricuspid and pulmonary valves.
located on the posterior (back) part of the heart; the pulmonary veins enter on its posterior surface. Its lower part is open, leading into the left ventricle. The connecting opening, the mitral orifice , contains the mitral valve . The left ventricle has a relatively small, conical cavity. The muscle of the left ventricle is three to four times thicker than that of the right ventricle. This relationship is in line with differences in pressure between the two sides of the heart. The upper part of the left ventricle contains both orifices: the inflow (mitral) orifice, to the left and rear, and the outflow (aortic) orifice, in front and to the right. The aorta originates from the left ventricle in a manner similar to that of the pulmonary artery from the right. Its origin contains the aortic valve (fig. 5).
As indicated, the two sides of the heart are separated from each other by partitions, or septa: the atrial septum , and the ventricular septum . The former consists of a thin layer of muscle, with the exception of an oval area where muscle is missing. This feature, the fossa ovalis (fig. 3), is a remnant of a valve, present in the embryo, which protected an orifice between the two atria through which blood could flow from the right atrium into the left atrium before birth (see chap. 11). The ventricular septum consists of a thick muscle continuous with the "free" walls of the left ventricle. It is thinned out in only one small area, underneath the aortic valves, where no muscle is present (membranous septum ). A common
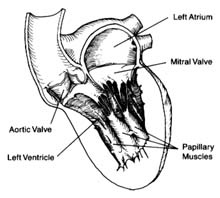
Figure 5. Details of the mitral and aortic valves.
birth defect is for this portion of the septum to be missing, providing a communication between the two ventricles.
The four heart valves consist of two sets almost identical in structure and function. The two inflow valves separate the atria from the ventricles (atrioventricular valves ). The two outflow valves separate the ventricles from the two main arterial trunks (semilunar valves ). The inflow valves prevent blood from backing into the atria during ventricular contraction. The purpose of the semilunar valves is to prevent the sucking back of blood from the aorta and the pulmonary artery during ventricular relaxation.
The atrioventricular valves are attached to rings that form the two orifices between atria and ventricles. These rings are made of dense fibrous tissue (annulus fibrosus ), and the valves themselves are moderately thick, curtainlike structures. The right-sided atrioventricular valve, the tricuspid valve (fig. 4), has three leaflets; the left-sided valve, the mitral valve, has two leaflets (fig. 5). Free edges of each leaflet are connected through a series of delicate strings or cords (chordae tendineae ) with muscular outgrowths, pillarlike structures, in the lower part of the ventricular cavity (papillary muscles ). Each ventricle has two such papillary muscles, connected through the chordae tendineae with free edges of the valve leaflets. These chordae fan out like a parachute to the edge of the valve curtains. The papillary muscle and chordae tendineae stabilize the valves and prevent their flapping back into the atrium when they close in response to the high pressure in the ventricle.
The semilunar valves derive their name from their crescent-shaped leaflets. Each valve consists of three delicate leaflets, forced apart by high pressure during the ejection of blood into the aorta and the pulmonary artery. These leaflets, or cusps, stay close to the wall of the two arterial trunks, permitting free flow of blood. During the beginning of ventricular relaxation the cusps are sucked back with the blood and completely close the orifice separating the vessels from the ventricles during that portion of the heart cycle.
Structure of the Blood Vessels
The greater circulation consists of the aorta, the arteries, the arterioles, the capillary network, and the veins. The aorta, after arising from the left ventricle, sends off two coronary arteries and then runs upward (as the ascending aorta ), arches to the left (aortic arch ), and turns downward (descending aorta), in front of the spinal column, until it reaches the lower abdomen, where it divides into two principal branches. (The aorta and its more important branches are shown in figure 6.) The coronary arteries supply the heart itself; the aorta supplies blood to the head and upper extremities by means of four major arteries: two carotid arteries and two subclavian arteries . On the right side the carotid and subclavian originate as a joint, short trunk (innominate artery ); on the left side they arise directly from the aorta. The aorta sends off no major branches until it passes below the diaphragm, where three major arteries originate from its frontal wall, and two from its side wall, supplying all abdominal organs. The branches of the coeliac artery supply the stomach, liver, spleen, and pancreas. The renal artery supplies the kidneys, and the iliac artery carries blood to the lower trunk and the legs. The mesentric artery supplies the intestines.
The coronary arteries provide the blood supply for the heart itself (fig. 7). The left coronary artery runs a very short course and then divides into two large branches, the anterior descending coronary artery and the left circumflex coronary artery . The former supplies the front of the heart, particularly the left ventricle; the latter supplies the lower left portion, the back of the left ventricle, and the left atrium. The right coronary artery runs a moderately long course before dividing into branches; it supplies the right side of the heart and the lower back portion of the left ventricle. Even
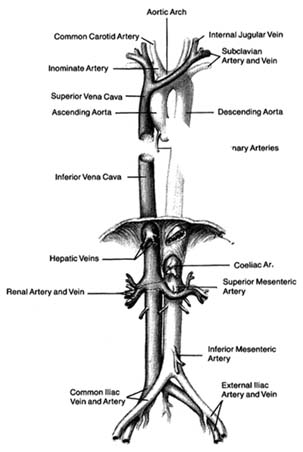
Figure 6. The principal arteries and veins. The heart has been removed from the illustration. Only initial portions of smaller vessels are shown.
though only two arteries originate from the aorta, the two branches of the left coronary artery are counted as major vessels; thus the clinician is used to thinking in terms of three, rather than two, sources of arterial blood supply to the heart.
The arteries in the body divide and subdivide into smaller segments. The smallest arterial branches, at the borderline of visibility, are called arterioles , beyond which the blood enters a myriad of
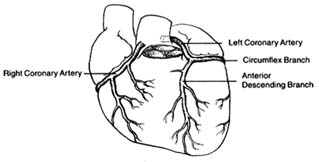
Figure 7. The coronary arterial circulation.
microscopic channels with very thin walls, the capillaries . These minute blood vessels are located within the tissues and organs of the body; they are integral parts of the various organ structures. The capillaries join together into very small veins, or venules , which in turn join together into increasingly large veins, eventually forming the two major veins, the superior and inferior vena cava. Larger veins usually accompany corresponding arteries and carry the same names, as indicated in figure 6. The inferior vena cava, the principal lower vein, is located alongside the aorta, deriving tributary veins similar to branches of the aorta. It drains blood from the abdomen and the lower part of the body into the right atrium. The large upper vein, the superior vena cava, drains blood from the head and upper extremities through four tributary veins analogous to the four corresponding arterial branches. It runs a short course in the chest, entering the upper portion of the right atrium.
The pulmonary circulation is presented in figure 8. Venous (dark) blood collected in the right atrium is pumped by the right ventricle into the pulmonary artery, which, after a short course upward, divides into two principal branches, each supplying one lung. The right and left branches of the pulmonary artery are large vessels, frequently referred to as the "right pulmonary artery" and "left pulmonary artery," in which case the pulmonary artery is called the "pulmonary trunk." Each artery divides into as many branches as there are lobes of the lungs (three on the right side and two on the left). These branches subdivide further into smaller and smaller branches, forming pulmonary arterioles and then pulmonary capillaries. The capillaries collect into venules and veins,
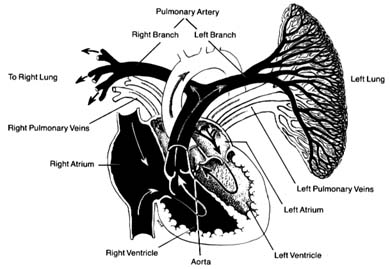
Figure 8. The pulmonary circulation. The right lung has been removed
from the drawing. Oxygenated blood is shown in
white and deoxygenated blood in black.
through which fully oxygenated blood returns to the left side of the heart. Four large veins, two from each lung, carry the blood to the left atrium.
The blood vessels show important structural differences, related to their various functions. The aorta and the largest of the arteries act as collectors and receptacles of blood; hence they are thick-walled and elastic. Smaller arteries participate in regulating blood flow and may require contraction and relaxation under certain conditions; hence their tissues are less elastic and more muscular. The arterioles have a particularly well-developed musculature; its contraction and relaxation is the principal factor in regulating blood pressure, as will be discussed later (chap. 3). The walls of the pulmonary artery are thinner than those of the aorta, as it is exposed to considerably lower pressure. Smaller pulmonary arteries and arterioles have poorly developed musculature, although in certain diseases this muscular tissue develops. The veins of the systemic and the pulmonary circuits are thin-walled, collapsible vessels in which blood flows under low pressure. Larger systemic veins have valves (similar to the semilunar valves of the heart) that prevent backflow
of blood, particularly in parts of the body where blood flows against gravity.
The lymphatic system is an auxiliary system of blood vessels carrying a white tissue fluid (lymph ) resembling blood plasma that participates in the nutritional process of organs. Most tissues of the body contain lymphatic capillaries, which collect certain elements of tissue fluid and carry it through a fine network into larger vessels and then into a large duct (thoracic duct ) that runs upward along the thoracic spine and empties itself into a tributary of the superior vena cava. The lymph thus mixes with blood and becomes part of the blood plasma. Smaller lymphatic vessels are connected with lymph nodes, which act as important filters, extracting undesirable components of tissue fluid and preventing them from entering the bloodstream.