Part IV
INTERNATIONAL PERSPECTIVES
AIDS Policies in the United Kingdom:
A Preliminary Analysis
Virginia Berridge
Philip Strong
In a paper on the intellectual agenda surrounding the AIDS epidemic, Jeffrey Weeks comments that "AIDS has … provided important insights into the complexities of policy formation in pluralist societies."[1]
Jeffrey Weeks, "AIDS: The Intellectual Agenda," in AIDS: Social Representations, Social Practices, ed. P. Aggleton, G. Hart, and P. Davies (Brighton: Falmer Press, 1988), pp. 1-20.
But, with some notable exceptions,[2]Among recent studies are Daniel M. Fox, Patricia Day, and Rudolf Klein, "The Power of Professionalism: AIDS in Britain, Sweden, and the United States," Daedalus 118 (1989): 93-112; John Street, "British Government Policy on AIDS," Parliamentary Affairs 41 (1988): 490-508; Ewan Ferlie and Andrew Pettigrew, "Coping with Change in the NHS: A Frontline District's Response to AIDS," Journal of Social Policy 19 (1990): 191-220; and Patricia Day and Rudolf Klein, "Interpreting the Unexpected: The Case of AIDS Policy Making in Britain," Journal of Public Policy 9 (1990): 337-53.
most of the burgeoning social science research on AIDS has necessarily focused not on policy formation but on studies of sexual behavior or disease transmission.[3]For the range of British research, see Register of Behavioural Research on AIDS, MRC AIDS Behavioural Research Forum, ed. Mary Boulton (London: Health Education Authority, 1989).
Historians, as social scientists, have been prominent in bringing the historical record into debates on AIDS. But, as Daniel M. Fox and Elizabeth Fee observe, they have played relatively little part in writing and analyzing the "contemporary history" of AIDS.[4]Elizabeth Fee and Daniel M. Fox, "The Contemporary Historiography of AIDS," Journal of Social History 23, no. 2 (1989): 303-14.
In this essay we focus both on AIDS policy development and on "contemporary history." We chronicle the development of AIDS policies in the United Kingdom in the 1980s and focus on three distinct stages of policy development. In particular we show how an initial policy vacuum in the AIDS area gave rise to a new "policy community" and how that community has changed over time. We outline some themes for future policy research and examine the potential role that historians could play in the study of AIDS policies. "Contemporary history," in the United Kingdom at least, has so far focused almost exclusively on "high politics."[5]
See, for example, Anthony Seldon, ed., Contemporary History: Practice and Method (Oxford: Blackwell, 1988).
Indeed, some practitioners have argued that the term contemporary history applies only to conventional political history. We will argue that the study of AIDS policies can provide a model, too, for the way in which the "contemporary history" of health and science policy could develop.[6]Our focus here is primarily historical. Another paper deals with issues from the sociological perspective. See Philip Strong and Virginia Berridge, "No one Knew Anything: Some Issues in British AIDS Policy," in AIDS: Individual, Cultural and Policy Dimensions, ed. P. Aggleton, P. Davies, and G. Hart (Brighton: Falmer Press, 1989).
Another version of this essay, which is reprinted with permission, has been published in Twentieth-Century British History (2 [1991]). The authors are grateful to the Nuffield Provincial Hospitals Trust for financial support for the research on which this essay is based and to Ingrid James for secretarial assistance. Thanks are also due to audiences at the conference on AIDS and the Historian, National Institutes of Health, Bethesda, and at the Wellcome Institute for the History of Medicine in London, where versions of this essay were presented.
This essay is a preliminary analysis based on a survey of the historical material already available: in part published sources, in part a round of initial interviews with participants in the AIDS arena—among them a senior civil servant; gay community activists; those involved in voluntary organizations, both gay and non-gay; clinicians; an actuary; and representatives of a pharmaceutical company. Its purpose is not to convey direct policy advice or to lay down a policy message—much of the social science research on AIDS has necessarily been funded with such an aim—but to identify the nature and determinants of issues, to raise questions about policy rather than to suggest solutions. Nor is its purpose to praise or to assign blame. As Roy Porter commented in a review of Randy Shilts's And the Band Played On , "'Heroes and villains' history only gets you so far. … We need a much more reflective grasp of the dialectics of making decisions. … Shilts typically reduces complex issues to personalities, and neglects the social and structural. By all means let's blame Reagan and media homophobia. But let us also see that the appalling slowness and ineptitude of the U.S. response to AIDS arose out of the mixed blessings of the decentralised state and of City Hall caucus politics."[7]
Roy Porter, "Epidemic of Fear," New Society, March 4, 1988, pp. 24-25.
The focus of this study is, by contrast, British AIDS policies, but the emphasis on the necessity for structural rather than personal levels of analysis is the same.First, the basic epidemiological story of AIDS in the United Kingdom needs to be quickly outlined. The disease was first diagnosed there in 1981, and the first AIDS death in the United Kingdom was reported in 1982. By the end of 1983, there had been 29 cases; there were 106 by 1984, 271 by 1985, and 610 by 1986. By the end of April 1989, there had been 2,228 cases in total, of which 1,190 had resulted in death. London remained the primary center for AIDS cases; the majority of cases came from the Thames regions of the National Health Service. These comprised 70 percent of the total number of cases in the first quarter of 1989. As for the types of people with AIDS, 95 percent were men, and the great majority of these were homosexual or bisexual; 6 percent of these cases were hemophiliacs, and 6 percent were drug users or had acquired the disease through heterosexual intercourse. For HIV-positive persons the percentages were different. Here 14 percent were drug users, nearly half of them women. Drug users are a growing category of the seropositive. Consequently, because of the high proportion of seropositive IV drug users in Scotland, Edinburgh and Dundee in particular, its geographical importance is increasing.[8]
For details of the epidemiological picture, see Department of Health, Press release 89/201, May 8, 1989.
Chronology Of Aids In The United Kingdom
The periodization assigned to the epidemic varies. Jeffrey Weeks, for example, sees 1981–1982 as "the dawning crisis." Then followed (in 1982–1985) a period of "moral panic," when AIDS "became the bearer of a number of political, social and moral anxieties, whose origins lay elsewhere, but which were condensed into a crisis over AIDS." This period was followed by a period of "crisis management," beginning in 1985 and lasting until the present.[9]
Weeks, "AIDS: The Intellectual Agenda."
Weeks uses evidence both from the United States and the United Kingdom to support his case; the death of Rock Hudson in 1985 marked a turning point in public perceptions of AIDS in both countries. Other policy studies have focused on the "crisis management" period—the period when AIDS became a direct and immediate concern for politicians. The emphasis in these studies is on policy as a top-down process; on AIDS as exemplifying the role of the state in sending signals to the public, as well as receiving them; on the consensual nature of policymaking and the handling of AIDS within traditional British policy structures.[10]For examples of these interpretations, see Fox, Day, and Klein, "The Power of Professionalism"; Day and Klein, "Interpreting the Unexpected"; and Street, "British Government Policy on AIDS."
We emphasize different aspects to the AIDS story and specify three distinct policy phases. In the first phase (1981–1986), AIDS slowly became a national policy issue. Policy was essentially, particularly at the beginning, formed in a bottom-up rather than a top-down way. It was initially formed at the local level, both through gay groups and through the construction of clinical and scientific expertise. These groups coalesced to form an initial "policy community" around public health interests in the Department of Health. In the second and briefer phase (1986–1987), a period of "wartime emergency," AIDS came to be viewed as a clear political priority rather than simply a departmental matter, and sections of society were put on almost a wartime footing to meet what was regarded as a national emergency. This phase has been followed (1987–1988 to the present) by a phase of "normalization," where AIDS and the reaction to it are becoming part of the normal policy and institutional processes. The threat of immediate epidemic spread has receded; and the threat of widespread heterosexual infection no longer appears imminent. Changes in therapy and the time scale of disease progression have helped to bring about a model of chronic, rather than acute, disease, which has aided, but not determined, the process of normalization.
1981–1986: Construction Of A Policy Community
In the early 1980s there was little by way of a reaction from central government. In 1981 the Annual Report of the Chief Medical Officer noted that for the first time there had been more than half a million new cases of venereal disease, concentrated particularly in the more recently recognized sexually transmitted diseases.[11]
Annual Report of the Chief Medical Officer of the Department of Health and Social Security for 1981 (London: Her Majesty's Stationery Office [HMSO], 1982), p. 40.
However, at that time this increase was not regarded as so significant that it required political action. Ironically, too, the same report contained the conclusions of an advisory group on the management of patients with spongiform encephalopathy—namely, that "Creutzfeldt-Jakob disease was the only disorder caused by a transmissible slow virus agent which is likely to be encountered in the UK."[12]Ibid.
Initial knowledge of and reactions to AIDS had instead a volunteer ethos; knowledge of the disease was transmitted through existing gay networks and served also to consolidate them. New organizations also began to be founded. How did this gay response develop? Some gay men were in the United States in the early 1980s and began to hear about people dying of strange cancers. A member of a student gay group at Cambridge recalled that the groups's gay helpline began to get calls after a BBC Horizon program, "Killer in the Village," in 1983. The students began to look around for information and to hold weekly meetings on AIDS and health issues. "We were groping in the dark. There was no sense of there being anyone other than us to turn to."[13]
Interview, gay community worker, February 1989.
That television program, like others later in the epidemic, appears to have had a key impact on the gay response. Volunteers at the Gay and Lesbian Switchboard in London arranged to open up a special line after the program, and volunteers were specifically briefed. "For a number of days after, a lot of very worried people were ringing. … The 'Killer in the Village' program was absolutely crucial."[14]Interview, gay community worker, March 1989.
The Gay and Lesbian Switchboard was of central importance in the initial response. In May 1983 more than two hundred attended the country's first public conference on AIDS organized by the Switchboard. Mel Rosen, director of the New York-based Gay Men's Health Crisis, spoke. Some present at the conference remembered his words: "There's a train coming down the track and it's heading at you." A member of the audience recalled: "I was struck by the potential gravity of what was happening and the absolute silence on what was happening. There was very little in the mainstream press."[15]
Interview, gay activist, July 1989.
The Horizon program also led to the refounding (in 1983) of the Terrence Higgins Trust,originally established in 1982 by friends of Terrence Higgins, who had died of AIDS in abject circumstances in a London hospital. When the trust was refounded, many of the Switchboard volunteers—including Tony Whitehead, later chairman of the Steering Committee of the trust—moved over to it. By the end of 1983, the trust was producing its first leaflets on AIDS, and it opened its own AIDS helpline early in 1984. Articles in the gay press—for example, by Julian Meldrum, the trust's press officer and also a Capital Gay correspondent—forced discussion of issues such as safe sex and the role of promiscuity within the gay community. One gay man recalled, "Safe sex really hit London at the end of 1984."[16]
Interview, gay journalist, November 1988.
Also involved in the initial gay response was the Gay Medical Association, which produced a leaflet early on directed at doctors dealing with AIDS. Its response was to stress the potential and actual heterosexual nature of the disease. In April 1983 a letter in the British Medical Journal put this point strongly. In an AIDS review article, A. P. Waterson, a virologist, had compared the syndrome to diseases of overcrowded poultry, relating it, as was common at that time, to the use of nitrites and the high number of sexual contacts among some gay men.[17]
A. P. Waterson, "Acquired Immune Deficiency Syndrome," British Medical Journal 286 (1983): 743-46.
Gay Medical Association representatives commented: "Of course, promiscuity is an important factor in the spread of communicable diseases, but promiscuity is not the prerogative of homosexuals. … The homosexual community has demonstrated its awareness of its own health problems. We are confident that it will respond to health education programmes which are not underwritten by any prejudice or moralising." The correspondents pointed out that this condition could potentially affect the whole of society; already around 25 percent of cases to date had not been in homosexual males.[18]M. R. Farrell et al. (members of Gay Medical Association), "Acquired Immune Deficiency Syndrome," British Medical Journal 286 (1983): 1143.
Many dimensions of the initial gay response remain to be documented. But its voluntaristic, self-helping ethos is clear—with meetings in gay men's houses and flats and in gay pubs. "We formed an ad hoc committee … and I called a public meeting in the upstairs bar of the London Apprentice at Hoxton, a gay pub. It wasn't an education meeting, it was a recruitment meeting."[19]
Interview, gay activist, July 1989.
The "gay freemasonry," the already existing networks of gay men, operated to spread advice and information and to develop reactions to the disease. By 1983 organized sections of the activist gay community had developed specifically around the AIDS issue. (Such phrases are, of course, shorthand. We are wary of monolithic interpretations such as "gay community" or "medical profession," being aware of debates and tensions within these groups.)The policy aims were threefold: to convey the message of the dangers of AIDS to gay men; to develop a more public role (but without thereby sacrificing credibility among says) by raising public and political awareness of the dangers of an AIDS epidemic; and to prevent the danger of an anti-gay backlash by stressing—as the Gay Medical Association had done—the idea of AIDS as potentially and actually a heterosexual disease.
Another policy lobby was also forming at around the same time. Clinical and scientific expertise on AIDS was also in the process of being established. The human immunodeficiency virus was first identified in 1983. Up to and for some time after that date, there was an absence of the kind of scientific knowledge and scientific certainty that had come to be an expected concomitant of any normal fight against disease. Professor Waterson's 1983 summary demonstrated the uncertainty: "The most sinister feature of this acquired immune deficiency is that it appears to be communicable, perhaps principally by intimate physical contact." This scientific vacuum led to explanations couched in terms of morality rather than of science: "The traffic in human material in certain quarters by abnormal routes has reached such a level that, combined with the effects of drug abuse of various kinds, the sheer weight of chemical and microbial insult to the body in general, and to T-lymphocytes in particular, goes beyond the tolerable limit."[20]
Waterson, "Acquired Immune Deficiency Syndrome," pp. 743-46.
The Annual Report of the Chief Medical Officer for 1983 did not moralize but was no less tentative: "Expert opinion suggests that there is no risk of contracting AIDS as a result of casual or social contact with AIDS patients eg. on public transport, in restaurants, or in private dwellings. The spread of AIDS appears to require intimate contact."[21]Annual Report of the Chief Medical Officer of the Department of Health and Social Security for 1983 (London: HMSO, 1984), p. 45.
The explanations being advanced in the scientific and medical press—links with African swine fever; the virus emerging from Africa or Haiti—show that scientific knowledge of the sort normally taken for granted was in the process of being constructed.[22]See, for example, the range of articles in the Lancet or British Medical Journal in 1983 dealing with the origins of AIDS in Haiti and in swine fever.
Expertise also requires experts; and the AIDS experts initially came from a range of areas, such as immunology and virology, and from cancer research, where work on retroviruses had been undertaken for the previous twenty years and where the change from studying chicken viruses to studying human retroviruses had already been made because of new directions in leukemia research. Significantly, too, AIDS brought the area of sexually transmitted diseases and genitourinary medicine in from the cold. One participant commented: "It was a 'Cinderella specialty' with poor facilities and second-rate people working in it. … You
could go into genitourinary medicine without a higher medical qualification. … It was a pretty poor service in terms of the quality of physicians and facilities. … AIDS has helped—it's made genitourinary medicine a primary career option."[23]
Interview, genitourinary medicine consultant, February 1989.
AIDS meant, too, that a specialty not normally close to the center of policy formation in the health arena was drawn directly into a policy advisory role. The early researchers in the AIDS area in Britain came from this mixed type of background. Jonathan Weber and Robin Weiss at the Institute of Cancer Research were viologists; Anthony Pinching at St. Mary's and Richard Tedder at the Middlesex were immunologists; Michael Adler at the Middlesex and Charles Farthing at St. Stephen's were specialists in genitourinary medicine. The Social Services Committee report noted in 1987 the "haphazard recruitment" of expertise to AIDS.[24]
Social Services Committee, Third Report: Problems Associated with AIDS, vol. 1 (London: HMSO, 1987), p. viii.
There were undoubted tensions and differences, as there are in any scientific community; but these new-fledged scientific and medical experts also developed a consistent policy line and a means of airing it. Particularly noticeable was the high media profile they adopted in order to press the case for urgent action on the part of government. Certain of them adopted an overt public lobbying style, which was initially characteristic of the AIDS area. In the absence of the type of established policy consultative machinery that would exist in a well-established area of health policy, the experts resorted to the press and to television. In doing so, they were consolidating existing patterns of health reporting, which rely heavily on the small circle of medical "experts."[25]See, for example, Anne Karpf, Doctoring the Media: The Reporting of Health and Medicine (London: Routledge, 1988), for the role of medical experts in structuring the reporting of health matters. A particular example vis-à-vis hepatitis B is given by William Muraskin, "The Silent Epidemic: The Social, Ethical and Medical Problems Surrounding the Fight against Hepatitis B," Journal of Social History 22 (1988): 277-98.
But they were also joined by gay AIDS activists. The Terrence Higgins Trust in particular was aware of the value of using the media. It became "pretty clued up about news management," as one activist put it.[26]Interview, gay activist, July 1989.
Gay activists and the medical and scientific experts were prepared to be openly critical of lack of action on the part of government or the research councils. Anthony Pinching, for example, in his evidence to the Social Services committee, attacked the Medical Research Council's funding of AIDS research—peer review was in fact "peer refusal."[27]Social Services Committee, Problems Associated with AIDS: Minutes of Evidence, vol. 2 (London: HMSO, 1987), p. 153.
Jonathan Weber criticized its roles as "leading from behind."[28]Ibid., p. 53.
The type of public reaction that would normally lead to exclusion from the "corridors of power" in this case brought admission to them. For the external policy lobbies were complemented by the "public health" reaction to AIDS within the Department of Health. AIDS was initially dealt with through classic public health routines of monitoring and surveillance. From 1982 onward AIDS cases were monitored on a voluntary basis by the Communicable Disease Surveillance Center at Colindale
(part of the Public Health Laboratory Service, whose uncertain future was saved by its role in monitoring AIDS.)[29]
B. H. O'Connor, M. B. McEvoy, and N. S. Galbraith, "Kaposi's Sarcoma/AIDS Surveillance in the UK," Lancet 1, no. 2 (1983): 872.
CDSC doctors early on developed links with gay activists in the Terrence Higgins Trust. Sir Donald Acheson, the chief medical officer, as a public health epidemiologist himself, was also well aware of the disease's potential for spread. His annual reports made conscious references to the role of the great nineteenth-century public health pioneers, such as Sir John Simon, medical officer to the Privy Council Office. AIDS was, in his view, a disease that belonged in this great tradition of the public health fight against disease: "While the scourge of smallpox has gone and diphtheria and poliomyelitis are at present under control, other conditions such as legionellosis and AIDS have emerged. The control of the virus infection (HTLV III) which is the causative agent underlying AIDS is undoubtedly the greatest challenge in the field of communicable disease for many decades."[30]Annual Report of the Chief Medical Officer of the Department of Health and Social Security for 1984 (London: HMSO, 1986), pp. 35-37.
Acheson also spoke of "the need for the control of the spread of infection" as "an issue of prime importance to the future of the nation." Universally hailed for his role in AIDS by members of the policy lobbies ("If any honours are deserved for AIDS, he deserves one"), Acheson had held a meeting in late 1983 with gay activists to register support for the nascent Terrence Higgins Trust and its activities in the gay community. His department also issued a number of warning and advisory circulars: a circular issued by the Advisory Committee on Dangerous Pathogens to laboratory workers in 1984; a leaflet issued by the Health Education Council, Facts about AIDS; and advice for doctors in 1985.[31]
See Annual Report of the Chief Medical Officer of the Department of Health and Social Security for 1985 (London: HMSO, 1986), p. 46.
Also in 1985 the Public Health (Infectious Disease) regulations, made under the Public Health (Control of Diseases) Act of the previous year, were extended to cover AIDS.[32]Public Health (Control of Disease) Act, 1984, chap. 22; Public Health (Infectious Diseases) Regulations, 1985, No. 1546.
AIDS was, significantly, not made a notifiable disease. Acheson was strongly opposed to notification; and the strength of the historical record in the area of sexually transmitted diseases seemed to indicate that a voluntary approach would, for the moment, lead to the best results. But the regulations did allow some draconian precautions, such as the removal and detention in hospital of a person with AIDS (used only once) and restrictions on the removal of bodies from hospitals (for example, a requirement that body bags be used).The department's public health stance was given added impetus by the question of potential and actual heterosexual spread of the disease. This was part of the gay lobby's position; it also arose through the blood tissue, which first developed in 1983. There had previously been
criticism of the government because it had failed to develop self-sufficiency in Factor VIII and other blood products after an outbreak of hepatitis B among children at a special school in Hampshire in 1981. The development of self-sufficiency, critics argued, was being hindered by failure adequately to invest in the expansion of the Blood Products Laboratory at Elstree and by health service cuts that were preventing the regional health authorities from supplying the laboratory with the extra blood it would need.[33]
Andrew Veitch, "Extra £30 Million Could Have Kept Out AIDS," Guardian, May 3, 1983.
Heat-treated Factor VIII, introduced originally because of hepatitis, was available by 1984, but there were technical problems in getting it into mass production. In the spring of 1983, reports of the possibility of the transmission of AIDS through blood first began to appear in the medical press and thereafter in the press in general. In May 1983 a report in the Mail on Sunday on hospitals that were using "killer blood" noted that two men in hospitals in London and Cardiff appeared to be suffering from AIDS after routine transfusions for hemophilia.[34]Susan Douglas, "'Virus' Imported from U.S. Hospitals Using Killer Blood," Mail on Sunday, May 1, 1983.
Exact knowledge of the virus and its transmissibility was limited at this stage; and both the Health Department and the Haemophilia Society, the voluntary organization concerned, gave priority to encouraging hemophiliacs to continue with treatment.[35]Interview, Haemophilia Society worker, June 1989.
A DHSS spokesman was quoted in May 1983 as saying that "the advantage of using imported blood products far outweighs the 'slight possibility' that AIDS could be transmitted to patients through Factor VIII."[36]Quoted in John Hamshire, "Probe on Imports of 'Killer Blood,'" Daily Mail, May 2, 1983.
The department's initial reaction was to issue a leaflet, in August 1983, asking high-risk donors not to give blood. Heat-treated Factor VIII was not available from the United States until the end of 1984. Dr. Charles Rizza, an Oxford hematologist, was reported as saying that, until it was available, "I'm afraid our haemophiliacs are in the lap of the gods."[37]Stephen Cantle, "Haemophilia Alert over AIDS Factor," Doctor, May 12, 1983.
The domestic supply came on stream in the following year. By October 1985, too, a British HIV antibody test had been developed, and all blood donations began to be screened.By late 1984 the policy lobbies were beginning to coalesce into more established policy advisory mechanisms. The Department of Health began to set up administrative and policy advisory machinery focused on the new disease. The Expert Advisory Group on AIDS (EAGA) first met in January 1985 to advise the chief medical officer. Its members came from the clinical and scientific areas of new expertise on AIDS. A "social" group dealing with prevention and health education issues had a mixture of medical and gay activists. There was overlap between the groups. The expert group met seven times in 1985 and set up a number of associated groups: groups on counseling, screening, and resources; a
working group on health education in relation to AIDS; a group on AIDS and drug abuse; a subgroup composed of surgeons, anesthetists, and dentists; and groups on employment, renal units, artificial insemination, and immunoglobulin.[38]
Annual Report of Chief Medical Officer for 1985, p. 46; John Street, "AIDS Policy Advice in the UK" (forthcoming).
In addition to external links, the department developed its own internal policy machinery on AIDS. In 1985 a direct phone line for professional inquiries was linked to a special AIDS unit in the department. By 1985 AIDS had clearly become a departmental policy issue, with its emergent gay/medical/scientific policy community linked to the department. The policy lines that most clearly united the community were a stress on the need for urgent action and for public education to highlight the heterosexual nature of the disease rather than the "gay plague" angle of the popular press.1986–1987: Period Of Wartime Emergency
The governmental reaction until 1986 was primarily at a departmental level. But in 1986 AIDS was recognized as a clear political (in the sense of being a concern for party politicians) priority as well. No longer regarded as a problem for civil servants, volunteers, and medical and scientific experts, AIDS became a political issue—indeed, a national emergency. This reaction was marked in a number of ways, most notably by the formation in October 1986 of an interdepartmental Ministerial Cabinet Committee on AIDS, chaired by William Whitelaw, who was then deputy prime minister. The state of urgency was such that Whitelaw was on the steps of Number 10 Downing Street briefing the press on the (normally secret) meeting before the Cabinet Secretariat had finished typing the minutes.[39]
Peter Hennessy, Whitehall (London: Secker and Warburg, 1989).
The first full-scale debate on AIDS in the Commons was held in November.The health education campaign on AIDS was also enormously upgraded. Until 1985 the Terrence Higgins Trust had been the main source of information and advice on AIDS, but the Department of Health now began to expand its earlier series of leaflets and professional guidance into a public education campaign. In March 1986 a series of full-page advertisements appeared in the national press. These were widely criticized for poor presentation and lack of public impact, but in October, following the creation of the Whitelaw Committee, a public campaign costing twenty million pounds was announced, involving television as well as newspapers and wide distribution of a leaflet to all households in the country. The theme of the campaign—"Don't die of ignorance"—was the potential heterosexual spread of AIDS. This campaign
culminated in an AIDS week in the spring of 1987. There was cooperation, perhaps unparalleled since wartime, between two broadcasting companies, the BBC and ITV. One participant recalled, "If what was known about AIDS was true, then we had to educate the public fast. If it was left, it might be too late." The commitment of the broadcasting companies was wholly exceptional. After the sense of urgency had lessened, however, other considerations became uppermost: "People were beginning to ask, what next? Broadcasters by then had more or less given up editorial rights, were more or less acting as the government's mouthpiece. It made broadcasters reflect on the dangers of giving up editorial freedom and control—not because of AIDS but because of the dangers of being on the slippery slope to government control."[40]
Interview, media worker, January 1989.
In late 1986 the Health Education Council was replaced by a new Health Education Authority, a special health authority under much more direct political control and with specific responsibility for the public education campaign on AIDS. And early in 1987 the Commons Social Services Committee began an extensive series of meetings dealing with problems associated with AIDS. The potential for heterosexual spread of the disease was further underlined by the discovery of the virus among injecting drug users in Edinburgh. In the autumn of 1986 the report of the McClelland Committee on HIV in Scotland declared the prevention of HIV among drug users to be of the highest priority.[41]
HIV infection in Scotland: Report of the Scottish Committee on HIV Infection and Intravenous Drug Misuse (Edinburgh: Scottish Home and Health Department, 1986).
Everywhere, indeed, there was an air of emergency. Norman Fowler, then social services secretary, paid a visit to San Francisco with the chief medical officer early in 1987. Princess Diana's opening of the first purpose-built AIDS ward in the country at the Middlesex received widespread press publicity. The professional guidelines became a flood, and extra funding began to flow. AIDS became a target for increased resources rather than, as previously, a potential drain on existing finance. The £680,000 for AIDS services that had gone to the North East, North West, and South East Thames Regional health Authorities in 1985–86 rose to £2.5 million in 1986–87.[42]
Annual Report of Chief Medical Officer for 1985, p. 46.
The Medical Research Control received a million pounds from the Whitelaw Committee at the end of 1986 for research on AIDS. Early in 1987 a further £17.5 million was approved for AIDS research, £14.5 million of which was to go to a special Directed Programme on AIDS, aimed primarily at developing an AIDS vaccine. In wartime the pharmaceutical industries had collaborated. "It's a war-type coalition where everyone gets their jackets off and mucks in," commented a participant.[43]Interview, MRC research worker, November 1988.
Funding also went to the newly established Global Programme on AIDS, set up by the WorldHealth Organization. In 1987 over £200 million also went from the Overseas Developmental Administration to the European Community's developing program on AIDS.
AIDS was already defined as a problem at the policy community/departmental level before 1986. But how did it become defined as a problem at the political level? How did it become feasible for Conservative politicians to become closely involved in an issue which, in many of its aspects, would appear to have little appeal to the ethos of the Thatcher government? There are a number of possible explanations, none of them mutually exclusive and all warranting further investigation. There is an explanation based on personalities—either the concern of influential public and political figures or the particular involvement of politicians such as Norman Fowler at the DHSS. Fowler was regarded as an astute politician who could use an emergency such as AIDS to attract extra resources to his department. He has also been closely involved in the department's previous continuing activity on drugs, which in some respects—for example, the creation of an interdepartmental Ministerial Cabinet Committee and the development of a mass media campaign—prefigured many of the political responses to AIDS. Lessons from abroad—in particular the danger of heterosexual spread of the disease—also weighed heavily. Dispatches from the British ambassador in Kinshasa had drawn attention to the rapid heterosexual spread in Zaire and the possibility that Britain might share the same fate. The drugs issue in Scotland fueled those concerns. In 1986 the CMO's report pointedly noted that the current sex ratio of the disease in England and Wales was 33:1 (male to female), but in Africa it was 1:1 and in Scotland the ratio was different because of the higher proportion of intravenous drug abusers.[44]
Annual Report of the Chief Medical Officer of the Department of Health and Social Security for 1986 (London: HMSO, 1987), pp. 53-61.
The role of the media was also clearly important. As John Street has remarked, AIDS is perhaps the first "media disease."[45]
Street, "British Government Policy on AIDS." Obviously, other diseases—such as tuberculosis and influenza—have had considerable media salience. In AIDS, however, the political response was unusually (for Britain) determined by the media representations of the nature of the disease. Politicians derived their definitions of the problem directly from television in particular. See V. Berridge, "AIDS and Media Policy in Britain," Social History of Medicine, 3 no. 1 (1990): 144.
Particular media stories punctuate the early history of the disease—the death of the chaplain in Chelmsford prison in 1985, for example, and the death of Rock Hudson in the same year. Television programs that followed the pattern of the 1983 Horizon broadcast also appear to have made a particular impact—for example, the Panorama news analysis series devoted an entire program to AIDS in 1985. These programs were reacting on a particularly media-conscious government, with a general preference for mass advertising and market research and a reliance on particular media entrepreneurs. Just before the second mass media campaign was announced, there had been a spate of programs dealing with the AIDSissue, Weekend World among them; and there is evidence that these programs fueled the concern of government ministers.
But the pressure for emergency action also came in traditional bureaucratic ways, from the internal workings of the Department of Health and through the role of both medical and generalistic civil servants. For them, too, as one commented, AIDS just "gradually bubbled up."[46]
Interview, senior civil servant, 1988.
The role of Sir Donald Acheson has already been mentioned. AIDS was, in that context, essentially part of a revival of infectious disease since the 1970s, with outbreaks of salmonella and of hepatitis B as well as the arrival of AIDS. It also was part of the apparent revival of public health medicine, which had been severely downgraded in the postwar period. Acheson was chairing a committee on the public health function within the department at the same time that he was chairing the Expert Advisory Group on AIDS. This committee, which reported in January 1988, placed great emphasis on the role of AIDS in legitimating the revival and extension of public health powers. The legacy of Sir John Simon and the nineteenth-century "heroic phase" of public health was again to the fore; this committee's report, too, was remarkable for its historical consciousness. Acheson also appears to have had the support of the policy and generalist side of the Department of Health and of the civil servants in the Cabinet Office. An interdepartmental committee of officials preceded the Cabinet's interdepartmental political committee. In this sense, the period of national emergency conformed to a fairly classic model of bureaucratic policymaking.But the public context of the political reaction should also be recognized. Governmental activity took place against a background of increasing public fear, which should be distinguished from the "moral panic" and anti-gay feeling to which other writers have drawn attention. This kind of panic undoubtedly existed—in particular in the pages of the popular press, with its talk of "gay plague." But there was also a public fear of contagion. A senior London probation officer recalled, "If we had an HIV-positive person in those days, we'd clear the court."[47]
Interview, senior probation officer, 1988.
In the letter pages of the Guardian and the British Medical Journal in the early months of 1987, the safety of kissing was debated by Dr. John Seale, a Harley Street consultant; Sir Donald Acheson; and Dr. Joe Smith, director of the Public Health Laboratory Service. Although the virus had been discovered and scientific knowledge about transmission was proceeding apace, knowledge was not finally constructed and the boundaries with popular knowledge were undefined. A psychologist recalled: "X , consultant at Y hospital, came to see us at the beginning ofthe epidemic. I asked about transmission through sexual intercourse with women. That was seen as no risk then; now it's high risk. There were the arguments about deep kissing and how you'd need a liter of saliva. … Some doctors in Italy think you can and if it is the case, it's very serious. How do you know? There's sloppy talk—and no acknowledgment of doubts. They're full of certainties, and these change."[48]
Interview, hospital psychologist, February 1989.
Scientific and popular perceptions of the disease appeared to have equal credibility; science itself, early on, was only folklore in relation to AIDS. There was in a sense a popular decline in confidence in the authority of science and of official pronouncements about the disease. How far this decline impinged on the emergency policy reaction remains to be investigated. But certainly the vastly expanded health education campaign appears to have achieved an important, if partial, transformation in public knowledge about the virus and its means of transmission.[49]Department of Health and Social Security, AIDS: Monitoring Responses to the Public Education Campaign (London: HMSO, 1987).
1988 Onward: Normalization Of The Disease
In one sense, the wartime reaction was relatively short-lived. Some of the leading politicians moved on. Norman Fowler left the DHSS in 1988; William Whitelaw relinquished the chairmanship of the Cabinet Committee on his retirement in the same year; Tony Newton, who as minister of health had taken a particular interest in the AIDS issue, also moved on. Some witnesses to the Social Services Committee demanded an expansion of the wartime model of response. A memorandum from the Terrence Higgins Trust urged a national body to control and integrate all services, both voluntary and statutory.[50]
Social Services Committee, Problems Associated with AIDS (Memorandum Submitted by Terrence Higgins Trust), 2:101. The original memorandum, submitted by Michael Adler of the Middlesex Hospital, also argued along these lines, but Adler withdrew this suggestion when he gave evidence to the committee.
But Britain did not appoint a minister for AIDS or an AIDS supremo. The first report of the government's Advisory Council on the Misuse of Drugs—which argued for an extension of the harm-minimization approach to drugs and in particular for the establishment and extension of needle exchange projects—almost missed the emergency boat when it was presented to ministers in the autumn of 1987. It took ministers until March 1988 to decide on the publication of the report because of doubts within the government about the measures proposed.[51]Department of Health and Social Security, AIDS and Drug Misuse, Part 1 (London: HMSO, 1988).
The emergency reaction had become less appropriate.In the new phase, which began around 1988, AIDS gradually came to be perceived more as a "normal" nonepidemic chronic disease, and reactions to it became professionalized and institutionalized. Clearly, however, the high-level reaction has not disappeared. In January 1988, for example, the British government and the World Health Organization
jointly presided over a World Summit of Ministers of Health on programs for AIDS prevention. Delegates from 148 countries, three-quarters of them ministers, attended; 1988 was declared the year of communication and cooperation on AIDS.[52]
Annual Report of the Chief Medical Officer of the Department of Health and Social Security for 1987 (London: HMSO, 1988), p. 8.
But in other ways the period of wartime emergency was over. After the departure of Whitelaw, Fowler, and Newton at the Department of Health, no government minister was quite so publicly associated with the issue. The meetings of the Cabinet Committee were no longer publicized, and the committee itself was disbanded in 1989. Some of the earlier key committees were reconstructed, and some of the early actors became less central in policy development. "EAGA was a force in developing policies very quickly. … Now most are developed in the Department of Health and rubber-stamped," recalled an ex-member.[53]Interview, consultant, February 1989.
The policy community around AIDS was visibly changing to accommodate new experts; it, too, was part of the process of normalization. "The new people represented institutions—but then they all became experts."[54]
Interview, scientific research worker, February 1989.
The volunteer ethos remained important, but it was a rather different type of voluntary sector that became involved in AIDS. The Terrence Higgins Trust continued to expand after some internal changes. But it lost its place in the policy sun and became more marginal to policy development. It was to a degree displaced by a voluntary sector that was partly government funded—as exemplified in the establishment of the National AIDS Trust in 1987. (An earlier U.K. AIDS Foundation had failed to get off the ground in 1986 and had fallen apart amid recriminations.) "It's all become much more mainstream," commented one participant.[55]Interview, voluntary-sector worker, January 1989.
The normalization process was at work in the research arena, too. The Medical Research Council's AIDS Committee was re-formed—"The old-boy network of British science" moved in.[56]
Interview, scientific research worker, February 1989.
The Economic and Social Research Council developed an AIDS program that did something similar for British sociology: established non-AIDS/non-gay networks began to develop research. One early actor took these developments phlegmatically: "We have to learn that AIDS is everybody's business. … No one can be Mr. AIDS. No one can hang on to AIDS as their own. A lot of us find that difficult if we were involved from the very beginning. It's very hard to let other people get in on the turf."[57]Interview, consultant, February 1989.
Normalization and institutionalization were also demonstrated in the way that AIDS became seen as a long-term issue for services and treatment, rather than an emergency issue. In 1988 the Cox report on the short-term prediction of HIV infection revised figures downward:
"Continued exponential growth would lead to about 10,000 new cases diagnosed in 1992. While this cannot be totally excluded, there are a number of reasons for expecting slower growth and predictions in the range of 2,500–5,000 are more likely."[58]
Department of Health/Welsh Office, Short-Term Prediction of HIV Infection and AIDS in England and Wales: Report of a Working Group (London: HMSO, 1988), p. 41.
Once the threat of epidemic heterosexual spread had passed, AIDS became a normal part of the public health administrative machinery established after the Acheson report. In each health district a standing action group accountable to the Health Authority through a nominated community physician was now responsible for coordinating the relevant services.[59]Annual Report of Chief Medical Officer for 1987, p. 125.
AIDS care quickly moved from the specialist to the community care model, with a conference in 1987 on community care followed by the setting up of a Departmental Working Party on the subject. When the British Medical Association AIDS Foundation began to produce videos on the subject aimed at general practitioners, AIDS moved into the primary care arena. The stress on "early treatment"—the use of Zidovudine in asymptomatic disease—made clear that AIDS was regarded as a chronic disease, encompassed within a conventional spectrum of medical reaction. "AIDS will become a chronic disease requiring maintenance doses throughout life, but consequently less debilitating than multiple sclerosis," predicted one observer.[60]Interview, gay journalist, November 1988.
The discourse on AIDS began to emphasize AIDS in the spectrum of chronic rather than infectious or sexually transmitted disease; "a disease like diabetes" was one comment, with AZT as a latter-day insulin. By 1989 AIDS still raised some burning issues—notably the debates, in particular in the gay community, about the ethics of clinical trials and the ethical and practical issues surrounding testing. But other issues—for example, housing and care in the community—were common to many other conditions.[61]On housing see Raynsford and Morris, Housing Is an AIDS Issue (London: National AIDS Trust, 1989).
Some Themes In British Aids Policy
In this section we outline some themes arising from the preliminary research and then propose an agenda for future policy research on AIDS.
Policymaking From Below: The Rise—And Partial Fall—Of A New Policy Community
Fox, Day, and Klein, in their study of AIDS policymaking, emphasize the essential consensual nature of the policy reaction to AIDS and, by implication, the formation of policy in a top-down manner. "Governments," they argue, "have employed their standard procedures for
hearing, acknowledging, and, to a very limited extent, accommodating the dissenters." Like Fox, Day, and Klein, John Street, in his analysis of AIDS policies, emphasizes the medical and clinical input into policymaking and tends to downplay the impact of the gay lobby.[62]
Fox, Day, and Klein, "The Power of Professionalism," pp. 93-112; Street, "British Government Policy on AIDS." Fox, Day, and Klein do comment, however, that the gay lobby may have lacked visibility in Britain because it had fairly easy access to the department.
Both sets of authors focus in particular on the period characterized here as the wartime emergency. In another paper Day and Klein comment on the "normality" of the policy process in relation to AIDS: "Health policies in Britain have generally been developed in a closed arena, where action tends to be limited to professional groups and technical experts … so that in this respect also AIDS falls into a familiar and predictable pattern."[63]Day and Klein, "Interpreting the Unexpected."
But if the initial period of policymaking in 1981–1985 is brought into the picture, then the relative—if temporary—openness of policymaking is more striking. The concept of policy communities, the way in which subsystems in particular government departments develop relationships with outside pressure groups with shared priorities, is of relevance.[64]A. G. Jordan and J. J. Richardson, British Politics and the Policy Process (London: Allen and Unwin, 1987); see also Christopher Ham, Health Policy in Britain: The Politics and Organisation of the NHS, 2nd ed. (London: Macmillan, 1985).
The AIDS story clearly demonstrates how a new policy constituency was formed. There was an initial policy vacuum and a genuine initial openness about what forms of policy might be developed. Groups outside the normal policy arena—the gay lobby and the specialists in sexually transmitted diseases—were admitted to positions of power and policy advice. A three-way alliance, albeit a temporary one, was formed between public health interests in the Health Department and the new scientific and medical experts and the gay lobby. AIDS policy at this early stage perhaps exemplified a genuine pluralistic model, where all groups had potential power in the policy marketplace. But in 1986–1987, with the politicization of policy, power was taken away from that particular policy constituency and given back to more traditional actors and institutions. Thus, the nominal "depoliticization" of AIDS since 1988 has seen a change toward a more conventional model, where established scientific and medical interests play a more central role, as do established voluntary organizations.
Continuity And Change In Policy
Much of this essay has emphasized the essential newness of some aspects of AIDS policymaking. There is no denying the essential novelty that AIDS presented to many in policymaking circles, even at the senior civil servant level. But the element of continuity as well as the newness of policymaking also needs emphasis. How much was new in policy
development and how much was not? Here one can use the analogy of the historical debates on the impact of war on social policy. Historians have, in recent years, tended to downplay the impact of war and the supposed construction of a wartime consensus for social and political reform; instead, they have traced, for example, the roots of the National Health Service in prewar debates and blueprints for health care. The effect of war was to enable change to occur more quickly than might otherwise have been the case.[65]
See Charles Webster, Problems of Health Care: The National Health Service before 1957, vol. 1 of The Health Services since the War (London: HMSO, 1988); also Daniel M. Fox, "The National Health Service and the Second World War: the Elaboration of Consensus," in War and Social Change: British Society in the Second World War, ed. H. L. Smith (Manchester: Manchester University Press, 1986), pp. 32-57.
This analogy can be applied to AIDS. How far has AIDS changed existing policies—and how far has it been a means whereby developments in existing policies have been achieved perhaps more quickly than before? AIDS and drug policy offers one example. Fox, Day, and Klein, in their analysis of AIDS policies, see drugs as the single exception to the general theme of consensus, the one example where existing policy was overthrown. "The only instance of AIDS overriding established policy objectives has been in the field of drugs. … The Government had abandoned its previous stance of augmenting its restrictive and punitive policies on drugs now that AIDS had come to be seen as the greater danger."[66]Fox, Day, and Klein, "The Power of Professionalism."
But AIDS has not overthrown government penal policy; Britain remains part of an international system of legal control; at the European level in particular, the commitment to control is stronger as 1992 approaches. Nor is the harmminimization (or secondary prevention) approach anything new in British drug policy. It had already been enunciated as an official objective of policy—for example, in the 1984 report of the Advisory Council on the Misuse of Drugs.[67]Home Office, Prevention: Report of the Advisory Council on the Misuse of Drugs (London: HMSO, 1984).
Because of AIDS, what was previously an objective of researchers, service workers, and some civil servants has now become politically feasible.[68]For a fuller discussion of these points, see Virginia Berridge, "AIDS and British Drug Policy: History Repeats Itself ...," in Policing and Prescribing, ed. David Whynes and Philip Bean (forthcoming).
Aids And The Renaissance Of "Public Health"
The language of public health has become a commonplace in relation to AIDS. Day and Klein emphasize the definition of AIDS as a public health issue; Gerry Stimson, in a recent commentary on British drug policy, says that AIDS has brought about a redefinition of drugs as a public health matter.[69]
Gerry Stimson, "AIDS and HIV: The Challenge for British Drug Services" (forthcoming in British Journal of Addiction).
AIDS can indeed be seen as part of the pattern whereby the dominance of chronic, noninfectious disease in postwar health planning has been challenged by the rise of communicable disease over the last two decades. AIDS needs to be set in the context of legionnaires' disease and hepatitis B as well as the rise in sexually transmitted diseases. As we have already noted, the Acheson report on publichealth was produced in tandem with the developing AIDS issue in the Department of Health.[70]
Department of Health and Social Security, Public Health in England: The Report of the Committee of Inquiry into the Future Development of the Public Health Function (London: HMSO, 1988).
But "public health" is not an unchanging absolute. Its definition has narrowed in the twentieth century, as the nature of state intervention in social issues has itself shifted.[71]Jane Lewis, What Price Community Medicine? The Philosophy, Practice and Politics of Public Health since 1919 (Brighton: Wheatsheaf, 1986).
In the early twentieth century, concerns for personal hygiene and health education replaced more wide-ranging nineteenth-century concerns for social and environmental reform. The "new public health" of the 1970s and 1980s, with its focus on the individual and on prevention, has revived these earlier social hygienist concerns. AIDS policies—with their emphasis on the voluntary sector, prevention, and epidemiology—have epitomized some key elements of this redefined "public health" and have served to legitimate them.An Agenda For Policy Research
The "social history" of AIDS raises a number of issues that have long been of interest both to social historians of medicine and to medical sociologists. For example, the relationship between doctor and patient has entered a new phase, with debates over clinical trials and the use of alternative remedies publicized through alternative information networks. The "revolt of the patient" has reached a climax through AIDS. The early public reaction to AIDS—the debates on transmission of the new disease, the belief in contagion—is relevant to the way in which scientific knowledge is constructed and the relationship, often symbiotic, between popular and official perceptions of science. But in this section on agenda we will concentrate in particular on some policy issues that merit further research.
Aids And The Character Of Public Policy
Preliminary studies of policymaking and theories of AIDS policy formation need more detailed empirical examination. The rise of a policy community and its change over time have already been discussed. More specifically, we need to look at, for example, the role of expert groups in policy formation. AIDS policymaking has been marked by the use of such groups: the Expert Advisory Group on AIDS, CAPE, the health education advisory committee, the Advisory Committee on Dangerous Pathogens, the Advisory Council on the Misuse of Drugs. The recruitment, membership, activities, and impact of such groups need analysis. But there are other, equally important, elements in the structure of power:
the role of civil servants; relationships within, and between, government departments; and the role of politicians. According to Day and Klein, AIDS has been defined as a technical problem evoking classic public health responses, such as public education campaigns. But how far did these responses also derive from the political agenda of the Thatcher government, which had already laid stress on mass media campaigns in health and other policy areas? The impact of the media and of public opinion on policy also enters into the equation. What has AIDS meant for the new policy lobbies that have developed around it? Dennis Altman, for example, has perceptively commented that the United States gay community, although decimated by AIDS, has achieved greater legitimacy and political acceptability through the disease.[72]
Dennis Altman, "Legitimation through Disaster: AIDS and the Gay Movement," in AIDS: The Burdens of History, ed. Elizabeth Fee and Daniel M. Fox (Berkeley: University of California Press, 1988), pp. 301-15.
What function has AIDS performed for the British gay community and for the medical and scientific experts involved in plicymaking?The Ownership Of Aids
AIDS, as a new disease, has engendered professional tensions over who should have control over treatment and services. The range of differing specialties involved has already been discussed. Within drug clinics AIDS has led to a new emphasis on physical examination and general health, with consequent awakening of medical interest not just among drug specialists but among other areas of clinical expertise as well. There has been a debate on whether there should be separate "AIDS consultants." New occupations have appeared or have been enhanced. Counseling is a prime example—with divisions between the contact tracers re-formed as sexually transmitted disease health advisers and the new professional groups of counselors.[73]
David Silverman, "The AIDS Crisis and Its Impact on Counselling: The Social Organisation of Understanding," paper presented at the third conference on the Social Aspects of AIDS, London, 1989.
Gerald Oppenheimer has noted that the balance of power in U.S. AIDS policies shifted from epidemiology to virology with the discovery of the nature of the disease and the development of testing for it.[74]Gerald M. Oppenheimer, "In the Eye of the Storm: The Epidemiological Construction of AIDS," in AIDS: The Burdens of History, ed. Fee and Fox, pp. 267-300.
The processes at work in the British medical and scientific community likewise need examination.Aids Policy Debate And Resource Allocation
Part of the necessary analysis must concern the allocation of resources to different areas of activity. Some interesting differentials have already emerged—for example, in the much lower allocation of funding for drug services to Scotland despite the overwhelming preponderance
of seropositive drug users in Scottish cities. How far has resource allocation actually reflected the nature of the AIDS debate?
The Role And Professionalization Of The Voluntary Sector
AIDS policies, as this essay has demonstrated, have stressed the role of the voluntary sector. But the role and nature of that sector have changed as AIDS policy has developed. Ben Pimlott has commented, provocatively, that the Conservative government, with its emphasis on voluntarism, has in fact presided over the decline of any real voluntary sector and the rise of a government-funded and -controlled new "voluntary movement."[75]
Ben Pimlott, paper presented at the Institute of Contemporary British History seminar on Ten Years of Thatcherism, London School of Economics, 1989.
How far is this perspective applicable to AIDS?Prevention Policy And The Role Of Health Education
As already noted, AIDS has increased the focus on prevention in health policy and on health education as a means of achieving it. But the "politics of health education" in relation to AIDS needs examination—for example, the replacement of the Health Education Council by the Health Education Authority and the relationships between these bodies and the Departments of Education and of Health; the controversies over the health education "packages," Teaching about AIDS and Learning about AIDS; the debates about the utility and effectiveness of mass media campaigns; and the impact of market research and the relationship between commercial and academic forms of research and evaluation. AIDS provides, in microcosm, a demonstration of some more general prevention policy issues in the 1980s.
Research Policy And Aids
AIDS has had a clear impact on science policy. The Medical Research Council's Directed Programme on AIDS offers an example of an integrated program, from basic science to the clinical level, which scientists had long wanted in other areas. But it also raised other issues, many of which were already inherent in research policy—for example, the relationship of commerce and industry to academic research and a focus on policy-relevant research.
The Local Dimension Of National Policies
This interpretation of AIDS policy has emphasized the initial bottom-up rather than top-down nature of policy formulation. The local dimension must also enter into this approach. In the early years local policies stimulated national attention; for example, the Oxford City Council appointed the country's first AIDS liaison officer. The geographical dimension has also been important in the different nature of the epidemic, and the policy response, in Scotland and in England. Policy is also a question of implementation and impact as well as of formation; here, too, the local dimension is important. How have national policies had an impact at the local level?
The International Dimension Of National Policies
British AIDS policies have also interacted with policy formation at the international level. Among the major issues are the role of the World Health Organization; British participation in European Community AIDS initiatives; and the impact of AIDS in Africa on British policy. It is easy enough to assess British policy in isolation; but cross-national comparisons, as one study has already demonstrated, are fruitful means of exploring different (and similar) time scales of response.[76]
Fox, Day, and Klein, "The Power of Professionalism."
Conclusion: What Role For History?
As we initially noted, historians have been prominent in their initial contribution to AIDS issues. The historical record of epidemics such as cholera, plague, and the Black Death; the area of sexually transmitted disease; and the public health issues of quarantine, screening, and notification entered centrally into the debates.[77]
One paper may stand for many. See Roy Porter, "History Says No to the Policeman's Response to AIDS," British Medical Journal 20, no. 7 (December 1986): 1589-90.
In Britain history was a matter not just for historians but for key policy actors as well. The chief medical officer's reports stressed the voluntaristic tradition in management of sexually transmitted disease; in evidence presented to the Commons Social Services Committee in 1987, the 1916 Royal Commission on Venereal Disease was cited with similar intent.[78]Social Services Committee, Third Report, p. viii.
Public health doctors are in general historically conscious; but the readiness to quote, and to pay attention to, the historical argument also underlines the relative openness of policy at that stage.[79]A point made by David Musto at the conference on AIDS and the Historian, NIH, Bethesda, March 1989. The "openness" of AIDS policy was contrasted with the currently closed nature of drug policy and consequent lack of input from historians.
But history can, as this essay has indicated, make two further contributions:
in outlining the "prehistory" of AIDS and in writing and analyzing the "social history" of AIDS and AIDS policies. We cannot assess the elements of continuity or of change in AIDS policies without some assessment of what has gone before. For example, we need prehistories of virology, of immunology, and of developments in science research policy and drug policy.[80]
For one example of a "prehistory," see Muraskin, "Silent Epidemic."
AIDS has, in fact, highlighted a striking lack of research on the postwar history of medical and clinical specialties and of health and science policy. A "contemporary history" of AIDS itself also needs to be written. The dangers of such approaches are clear—a potential return to the "bad old days" of Whig internal histories of medicine, or a focus on institutional history. But the "combat history" both of AIDS and of postwar and contemporary health policy is a potentially valuable new historical direction.[81]The term combat historians was used by Daniel M. Fox at the conference on AIDS and the Historian.
Foreign Blood and Domestic Politics:
The Issue of AIDS in Japan
James W. Dearing
Japan is, by any measure, a country with a low incidence of acquired immune deficiency syndrome. As of September 1, 1990, the Japanese Ministry of Health and Welfare reported a total of 285 cases out of a population of over 120 million. Estimates by the World Health Organization in Geneva place the number of actual cases in Japan at about 500. Despite the low number of AIDS cases in Japan relative to some other countries, the issue of AIDS took Japan by storm for fourteen months beginning in January 1987. The short-lived yet remarkable salience of the issue of AIDS, juxtaposed with few actual AIDS cases in Japan, offers several insights concerning the Japanese society's reaction to an epidemic and to minority demands.
The issue of AIDS has gone through three distinct phases in Japan. The first phase was dominated by the international problem of AIDS and the policies of the Japanese Ministry of Health and Welfare; the second, by aggressive mass media coverage and public-interest groups that reacted to the threat of AIDS in Japan. In the third and current phase, the issue of AIDS has become routinized in Japan. After telling this three-phase story of AIDS in Japan, I then compare the history of the issue of AIDS in Japan and the United States.
AIDS In Japan
AIDS was first detected in Japan in 1982.[1]
John Roberts, "AIDS in Japan," Japan Journal, November 1987.
Through August 1988 1,048 AIDS carriers were identified by the Ministry of Health and Welfare.Current unofficial estimates by the World Health Organization are higher, but questionable epidemiological extrapolations by the Ministry of Health and Welfare make the number of people in Japan carrying the HIV virus very difficult to determine. Of the 1988 official total, 1,029, or 98 percent, were male. There were 90 identified persons who had developed AIDS, 46 of whom had died. Virus infection in Japan began later than in Africa, the United States, and Europe; although the rate of infection was similar through mid-1987, there is reason to believe that it has grown more slowly in Japan than in other countries since then.[2]
Medical Immunology 14, no. 3 (September 1987). In most countries AIDS has spread primarily through sexual relations. In Japan the majority of people infected with AIDS and carrying the HIV virus contracted the disease through contaminated blood products. Ensuring a safe blood supply is relatively simple compared to the difficult task of convincing people to change their sexual behavior; so the rate of new AIDS cases, especially among hemophiliacs, should be very low in Japan compared to the rate of new cases in other countries.
In Japan the disease has overwhelmingly been contracted through the use of imported blood-clotting coagulant by hemophiliacs. Hemophilia is a genetic disorder, inherited from the mother, of immoderate bleeding even from slight injuries. The disorder is inherited almost exclusively by males. In 1988 over 92 percent of all AIDS carriers in Japan were thought to be hemophiliacs.[3]
Ministry of Health and Welfare, AIDS Surveillance Data Sheet (1988).
Therefore, the vast majority of AIDS carriers in Japan are male. It is the regulation, prescription, importation, and use of blood coagulant which came to define the issue of AIDS in Japan.Throughout the 1980s Japan imported one-third of the world's blood products, 90 percent of which came from the United States. Japan itself has a high rate of blood donation, but until recently donations to the Japanese Red Cross have been used only for whole-blood transfusions, not for making blood products for commercial sale.[4]
"U.S. Blood Blamed for AIDS Spread," Japan Times, June 25, 1988.
Commercial blood products for sale in Japan are manufactured by several large companies in Japan as well as a few firms in the United States and West Germany. Patient prescriptions for blood products are controlled by physicians and hospitals, many of whom maintain their own blood dispensaries; so in Japan the profit in blood products is shared by manufacturers, hospitals, and doctors. The cost of blood coagulant to Japanese hemophiliacs is about four times higher than for hemophiliacs in the United States. Because of the dependence on U.S. manufacturers of blood coagulant, whose blood supply was contaminated with the AIDS virus, the Ministry of Health and Welfare estimates that up to 40 percent of Japan's 5,000 hemophiliacs are carriers of AIDS. Nongovernmental estimates suggest that as many as 60 percent of hemophiliacs are infected.[5]Eric Feldman, "AIDS in Japan," PHP Intersect, November 1987.
In 1988 about 44 percent of hemophiliacs identified by the Ministry as carrying the AIDS virus were twenty years of age or younger;[6]"Total of AIDS Carriers Exceeds 1,000 for First Time," Japan Times, February 21, 1988.
30 percent of them were under fifteen years of age.[7]"Four Become Japan's First Child AIDS Fatalities in 1987," Japan Times, February 14, 1988.
The present essay is based on research carried out in Japan with the support of a grant from the University of California University-Wide Task Force on AIDS, University of California, Berkeley, and was first presented to the 1988 Symposium on Science Communication: Environmental and Health Research, December 15–17, Los Angeles. The author acknowledges the assistance of the following persons: Reimei Okamura, head, International Affairs, Asahi Broadcasting Corporation; Dr. Bin Takeda, Department of Education, Chiba University; Rika Mazaki, news director, Japan Broadcasting Corporation (NHK); Yasushi Saeki, Information Service Department, Databank (NEEDS) Bureau, Nihon Keizai Shimbun; Yoshiaki Takeda and Osamu Murayama, staff writers, Mainichi Shimbun; and Yasuo Nakagawa, news editor, and Tai Kawabata, staff writer, Japan Times . Helpful criticisms on an earlier draft were offered by Dr. Everett M. Rogers, Annenberg School for Communication, University of Southern California; Dr. Youichi Ito, Institute for Communications Research, Keio University; Kiyoshi Nomura, Dentsu Institute for Human Studies; and Dr. Shigehiko Shiramizu, Takachiho Commercial University. The present essay benefited from advice from editors Dr. Elizabeth Fee and Dr. Daniel M. Fox, as well as anonymous reviewers.
The Mass Media Agenda
In modern societies the mass media often determine what issues policymakers and citizens think about, as well as the relative importance they ascribe to those issues.[8]
Everett M. Rogers and James W. Dearing, "Agenda-Setting Research: Where Has It Been, Where Is It Going?" in Communication Yearbook 11, ed. James A. Anderson (Newbury Park, Calif.: Sage, 1988), pp. 555-94). The mass media can also determine how people think about issues and how they evaluate presidential performance. See Shanto Iyengar and Donald R. Kinder, News That Matters (Chicago: University of Chicago Press, 1987). For a study of mass media influence on national policymaking, see Martin Linsky, Impact: How the Press Affects Federal Policymaking (New York: Norton, 1986).
The influential newspapers and television networks serve as the forum in which the issues of the day are shaped and debated, much as town squares, country markets, and coffee shops served this public function in preindustrial societies. Thus, an understanding of the "life" of a public issue requires an analysis of mass media coverage. How important has the issue of AIDS been in the mass media's news agenda in Japan? And how have the mass media covered this issue?Our analysis suggests that for several years AIDS was considered strictly a foreign problem. When it was made public in 1983 that the disease had been identified in Japan one year earlier, responsibility for bringing the disease to Japan was attributed to non-Japanese, even though tens of thousands of Japanese businessmen travel abroad every year on organized group "sex tours."[9]
Personal interview with Yasuo Nakagawa, news editor, and Tai Kawabata, staff writer, Japan times, July 19, 1988, Tokyo.
The first newspaper articles on AIDS tended to frame the disease as an international curiosity. Most articles were from international wire services.With the first case of AIDS in Japan, domestic coverage began. NHK, the dominant national (and public) television network, broadcast a fifty-minute informational program in 1983. By 1985 about 30 percent of AIDS stories in the general-interest Asahi Shimbun and about 55 percent of AIDS stories in the four financial Nikkei newspapers (including the Nihon Keizai Shimbun , often referred to as "Japan's Wall Street Journal ") were about AIDS in Japan. As the number of Japanese AIDS patients increased, the percentage of domestic-based articles increased, to over 50 percent for the Asahi Shimbun and over 60 percent for the Nikkei newspapers in the second quarter of 1988. Meanwhile, the percentage of articles about AIDS cases outside of Japan clearly declined. Many of the articles in the Nikkei group of newspapers centered on new product developments and the public stock values of domestic and foreign pharmaceutical companies.
The over-time distribution of the number of articles in these same newspapers is shown in figure 4. As this figure makes clear, early coverage of AIDS tended toward the foreign problem of AIDS, but the issue was of little importance in the print media. The first AIDS story to capture the public's attention occurred in November 1986: A Filipino nightclub prostitute working in the Nagano Prefecture city of Matsumoto
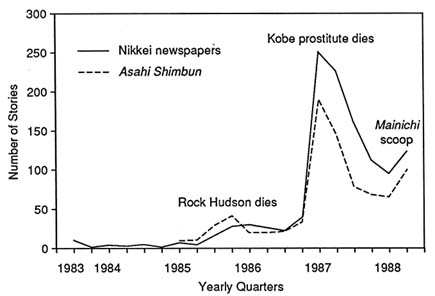
4. Japanese Newspaper Coverage of AIDS
SOURCE : Adapted from data from NIkkei NEEDS data base (an electronic
source owned by the Nikkei Corporation for accessing mass media stories).
was found to have AIDS, and it was suspected that she may have transmitted the disease to men in the area. The prefectural government quickly deported the woman back to the Philippines, declaring her visa expired.[10]
"News of AIDS-Infected Hostess Provokes Fear," Japan Times, November 15, 1986.
With the death of a single woman in January 1987, AIDS became a dominant issue in Japan. The January 1987 story had all the right news angles to propel the issue of AIDS to the top of the news agenda: it was domestic, it was about sex and death, and it implied that approximately one hundred anonymous Japanese men might be transmitting a deadly disease to their wives and other partners (extramarital sex is quite common in Japan).
The January story also involved a Kobe prostitute, but she was Japanese. She, her illness, and the public issue they would give rise to could not just be deported. Nevertheless, the AIDS Surveillance Committee of the Ministry of Health and Welfare did not release news of her illness until two days prior to her death on January 20, 1987, though she had been too sick to work for six months. She was the eighteenth Japanese to die from AIDS, and the first woman. In describing the woman as a
"habitual" prostitute, the Ministry said that she might have had sex with about one hundred men.[11]
"Ministry Reports 1st Diagnosis of Female AIDS Patient Here," Japan Times, January 18, 1987; "First Woman AIDS Victim Dies," Japan Times, January 21, 1987.
This announcement and its aftermath were widely covered by all the mass media in Japan. The most sensational news treatment was in the weekly tabloids, which have a circulation of more than one million. One of these tabloids had been tipped off about the family's funeral arrangements, and it subsequently published a photograph on its front page showing the woman in her coffin. Thus, she did for AIDS in Japan what Rock Hudson and the ostracized schoolboy Ryan White did for AIDS in America. Whereas the five newspapers of study printed a total of 2 stories about AIDS in January of 1985, in March of 1987 the same newspapers ran 189 articles about AIDS (the Asahi Shimbun alone printed 76 of these). The peak in mass media coverage in the first quarter of 1987 (fig. 4) represents this story and its aftershock, which included a sensational story about a pregnant Japanese woman with AIDS who refused to abort her child. These three heavily covered stories domesticized the issue of AIDS in early 1987 and represented the beginning of the second phase of the issue in Japan.How did the Japanese mass media cover the issue of AIDS? The major mass media, with the exception of the Nihon Keizai Shimbun and perhaps NHK, have a reputation for liberalism and sensationalism. According to the present research, early AIDS coverage was dominated by international wire service stories, which stressed homosexual and intravenous drug transmission. When cases first were diagnosed in Japan, staff-written stories and special reports appeared. Yet very few received print space or broadcast time prior to the Ministry of Health and Welfare's announcement that the Kobe prostitute was dying of AIDS. Overnight a maelstrom of AIDS stories dominated the news. For example, on January 19, 1987—one day after the Ministry announcement—NHK began a week of nightly seven-minute informational segments on AIDS on its Today show. Television ratings indicated that 20 percent of the Japanese population saw all or a part of the segments.[12]
Personal interview with Rika Mazaki, news director, Japan Broadcasting Corporation, July 26, 1988, Tokyo.
Certainly a part of the mass media fascination with the Kobe prostitute story centered on the means of transmission, which was heterosexual and thus strikingly different from what reporters and editors had been previously conditioned to think about AIDS transmission. They were forced to interpret AIDS in a new way, framing the issue with a new meaning. The Ministry of Health and Welfare, which served as the primary news source for AIDS information, had steadfastly framed the epidemiology of AIDS transmission in Japan as paralleling the spread of AIDS in the United States.An analysis of the Asahi Shimbun articles on AIDS, in which the articles were coded into twenty-two "subissue" categories, indicates that stories were most often about (1) government spending and policy responses, (2) the epidemic spread of the disease, (3) explanation of the disease and new information reported by medical scientists, (4) tests for AIDS antibodies and the effects of such tests on civil rights and privacy, and (5) means of transmission of the virus, including blood coagulant infection. Table 1 shows that the Asahi Shimbun 's coverage is quite similar to that of four major mass media in the United States.[13]
This coding scheme of twenty-two categories was initially developed for comparing the mass media news coverage of AIDS in the United States with public opinion survey questions about AIDS in the United States. As might be expected, a larger percentage of stories about AIDS from the Japanese mass media fell into the "other" category. Many of these articles dealt with announcements of international AIDS conferences or of joint Japan—foreign country research initiatives. In some of the articles in this category, translations from Japanese to English were insufficient to permit precise codification.
The Pearson's rank-order correlation between the Japanese and American coverage is .86, which is significantly different from zero at the .001 level.Figure 5 compares the distribution of stories by Japanese mass media (the Asahi Shimbun and the four Nikkei newspapers) with the distribution of stories by U.S. mass media (the New York Times , the Washing Post , ABC, and NBC) from January 1985 through June 1987. The distributions are somewhat similar (r = .69, significantly different from zero at the .001 level), although they clearly peak at different times.
Through 1987 Japanese news reporters generally did not question what their sources told them about AIDS. As in the United States, there was little if any investigative reporting about AIDS. But as the disease spread, mass media coverage became more aggressive. Reporters began writing stories about AIDS patients. And Japanese AIDS patients were angry.
On February 5, 1988, the general-circulation Mainichi Shimbun published the first article in a comprehensive series of front-page investigative reports. And these reports changed the direction of influence in the relationship between the Ministry of Health and Welfare and, on the other side, the mass media and public-interest groups. The Mainichi ran a banner-headline interview with a university vice-president, Takeshi Abe, who was also a medical doctor and who had chaired the Ministry's AIDS Surveillance Committee. In the interview Abe stated that clinical testing in Japan of heat-treated blood coagulant (which had been on the market in the United States and in West Germany since late 1983) for use by hemophiliacs had been delayed twenty-eight months (clinical trials had been completed in one month in the United States). Abe, who had been completely in charge of the testing, defended the delay:
When one company is ahead of the others in the research and development of a new drug, the duty of a research council is to coordinate things among
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
the companies to make them even, for the drug inspection by the Ministry of Health and Welfare. At least two or three companies should be bound together. … We needed to give patients the impression that all pharmaceutical companies are reliable to the same degree. … All companies must compete fairly. … It was for the sake of the patients. Those who complain don't understand things.[14]
"Coordination for Clinical Testing Normal: Q & A with Dr. Abe, Vice-President of Teikyo University," Mainichi Shimbun, February 5, 1988.
Apart from what these comments imply about the Japanese coordination of industrial policy, epidemiologists estimate that Abe's delay may have infected over one thousand Japanese hemophiliacs with the AIDs virus. Ministry of Health and Welfare sources anonymously suggested that, although the policy may have led to an increased number
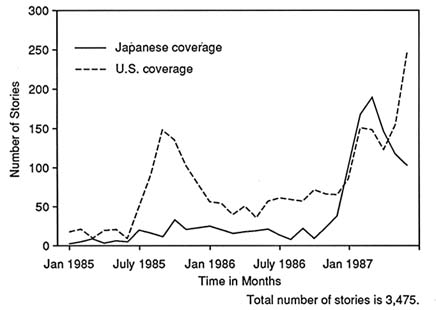
5. Mass Media Coverage of AIDS in Japan and the United States, January 1985–June 1989
of hemophiliacs' contracting the AIDS virus, their experts worried that heat-treated blood coagulant might cause a degeneration of protein. Moreover, they said, AIDS had never been a priority within the Ministry.[15]
"Measures against Hepatitis Contamination Developed in West Germany 7 Years Ago," Mainichi Shimbun, February 5, 1988.
The Mainichi did not stop with Abe's explanation—damning as it was. The newspaper also revealed that the leading Japanese blood company, which had not yet developed the heat-treatment process, had paid Abe $850,000 to set up a nonprofit corporation (the headquarters of which was a two-bedroom apartment that was usually empty) and that Abe had induced two of the foreign firms to pay money to the corporation. The implication was clear: Abe had delayed the clinical testing process to allow a Japanese firm, which had paid him a large amount of money, to develop heat-treatment technology so that the firm would not lose market share to foreign rivals. Meanwhile, the foreign firms were pressured into paying Abe money in order to stay in the race for access to the lucrative Japanese market.[16]
David Swinbanks, "Japanese AIDS Scandal over Trials and Marketing of Coagulants," Nature 331 (February 18, 1988): 552.
The trail of deceit, scandal, and profiteering was lengthened in March 1988, when the Mainichi broke the closely related story that imports of
untreated blood coagulant actually increased during the two years of Abe's delay, while other nations were phasing out untreated blood coagulant for fear of AIDS infection.[17]
"Actual Conditions over Suddenly Increased Import of Untreated Blood Products Made Clear," Mainichi Shimbun, March 12, 1988.
American blood suppliers, seeing that their markets for untreated blood had evaporated in the United States, discounted their prices to rid themselves of untreated coagulant inventories. Japanese hospitals bought the discounted coagulant and resold it to hemophiliac patients for large profits.[18]David Swinbanks, "Pharmaceutical Companies Profit from Japan's Blood Boom," Nature 332 (March 17, 1988): 193.
The Mainichi Shimbun stories fundamentally changed the public issue of AIDS in Japan. Prior to the newspaper's breakthrough, the importance of the issue and the way that it was interpreted were controlled by the Ministry of Health and Welfare. After the Mainichi series the previously vocal but ineffective hemophiliac association became more successful in having its own goals adopted by both the Ministry and the national Diet. Other, more traditionally efficacious, interest groups joined hemophiliacs in denouncing Ministry policy. Legal suits were filed by hemophiliacs. And news coverage of AIDS policy became more critical. A news editor at another Japanese daily newspaper said, "The Mainichi did the best job of any of the media. It was a big scoop and they really pursued it."[19]
Interview with Nakagawa and Kawabata.
The three reporters who worked on the stories received the Mainichi Shimbun Editor-in-Chief's Award for outstanding reporting. By and large, however, while acknowledging the Mainichi scoop, other mass media did not accord the scandal a high position on their news agendas. The Asahi Shimbun , for example, reported on the scandal on page 26, three days after the Mainichi Shimbun broke the story.[20]"Government and Company Compensation Demanded for AIDS Coagulant Disaster," Asahi Shimbun, February 8, 1988.
A news director at NHK was unaware of any particularly outstanding mass media coverage of AIDS, except for NHK's own reports.[21]Interview with Mazaki.
Though hemophiliacs and their supporters have sued corporations and the government, the traditionally slow pace of litigation in Japan has helped to drop the issue of AIDS to what most media observers describe as a "nonissue." Nevertheless, control over the definition and shared interpretation of the issue had been wrested away from the government by the newspaper.[22]See Stephen Hilgartner and Charles L. Bosk, "The Rise and Fall of Social Problems: A Public Arenas Model," American Journal of Sociology 94, no. 1 (1988): 53-78.
The distribution over time of the number of articles about AIDS (fig. 4) in the Japanese mass media shows a positive correlation with the distribution over time of the number of articles about AIDS in the U.S. mass media.[23]
For a detailed qualitative and quantitative analysis of American mass media coverage of AIDS, see Everett M. Rogers, James W. Dearing, and Soonbum Chang, "AIDS in the 1980s: The Agenda-Setting Process for a Public Issue," Journalism Monographs 12B (April 1991): 1-47.
This similarity is perhaps accounted for by the juxtaposition of two variables. First, the United States has approximately 500 times more AIDS carriers and AIDS patients than Japan. Whereas the U.S. mass media underreacted to the issue of AIDS in relation to the large number of patients,[24]Ibid.
it appears that the Japanese mass mediaoverreacted. In January 1987, when media coverage in Japan began to peak, there were fewer than twenty deaths nationwide attributed to AIDS. Theoretically, we would have expected less of a media response (or at least a more moderate one) to the threat of AIDS. But the scarce real-world evidence of AIDS was perhaps little heeded because the Japanese mass media were "primed" for the disease; that is, reporters and editors were aware of what was happening in the United States and in Africa, where the number of AIDS cases was multiplying rapidly. If either of these two conditions (few actual cases but awareness of the U.S. experience with the disease) had occurred separately, such a similarity between the distribution over time of the number of mass media stories about AIDS in each nation would not be expected.
Public Opinion And Public-Interest Groups
Whereas in the United States mass media organizations and public opinion pollsters had asked representative samples of the American adult population over 400 questions about AIDS midway through 1987,[25]
James W. Dearing, "The Polling Agenda for the Issue of AIDS," Public Opinion Quarterly 53 (1989): 309-29.
relatively few surveys of Japanese public opinion about AIDS have been collected. In the present research, therefore, survey results have been supplemented with other indicators of public opinion, such as the public activities of affected interest groups.In August 1983 the National Hemophiliac Society petitioned the Ministry of Health and Welfare to stop the importation of untreated blood coagulant. One month later the society requested the drafting of special legislation to facilitate the quick changeover to heat-treated blood coagulant. Both initiatives ended in vain. Instead, the Ministry required all untreated blood products to be certified not to contain blood from groups of people at high risk of contracting the AIDS virus. In October 1983 about fifty mothers of hemophiliac children banded together and entered a Tokyo factory of Nihon Pharmaceutical, where only domestic blood was used for making coagulant. The mothers pleaded and then screamed for the firm to increase its production of domestic coagulant. Again they were rebuffed.[26]
"Forced to Choose AIDS or Death: Cruel Choice for Patients," Mainichi Shimbun, February 5, 1988.
In October 1984, when the U.S. National Hemophilia Foundation recommended that only heat-treated coagulant be used, the new product had already been on the U.S. market for one year. Almost all Japanese doctors assured their hemophiliac patients and their families that imported untreated blood from the United States was safe. Most Japanese doctors would continue to give such assurances until 1986.[27]
Roberts, "AIDS in Japan."
Evenso, one Tokyo hospital alone tested 1,400 walk-up volunteers for the presence of AIDS antibodies between October 1985 and September 1986.[28]
"Hospital Finds 21 People with AIDS Virus," Japan Times, April 3, 1987.
The death of the Kobe prostitute and its ensuing media storm brought AIDS to the forefront of public concern. Within six days of the Kobe woman's death, more than 10,000 local citizens there approached public health officials to inquire whether they too might have the AIDS virus.[29]
"Over 10,000 People Come to AIDS Counseling Center in Hyogo Prefecture," Asahi Shimbun, January 26, 1987.
This panic was repeated throughout Japan.[30]Interview with Nakagawa and Kawabata.
AIDS discussions drew overflow crowds.[31]"Yokosuka AIDS Talk Draws Crowd," Japan Times, January 21, 1987.
One week after the death of the Kobe woman, a Tokyo metropolitan AIDS hotline had received 170,000 calls.[32]"170,000 Call Tokyo AIDS Information Number," Asahi Shimbun, January 28, 1987.
After their business had declined by more than half, seventy owners of massage parlors in Gifu Prefecture held a lecture on the prevention of AIDS and the testing of employees.[33]"Gifu 'Soapland' Group Sponsors AIDS Talk," Japan Times, February 7, 1987.
Ministry of Health and Welfare officials soon realized that calming the public would be one of their main tasks.Public apprehension led to suspicion of foreigners as AIDS carriers. Public baths and massage parlors posted signs saying "No Westerners admitted." Hostess clubs advertised "Japanese girls only" and "No foreign items work here." In Tokyo's Kabuki-cho red-light district, two previously popular sex nightclubs which featured foreign women closed for lack of business. Newspaper articles mentioned that non-Japanese had lost their jobs because they were suspected of having AIDS. A survey of 390 Japanese high school students in early 1987 found that when asked which ideas they associated with AIDS, the students most often mentioned (1) homosexuality, (2) death, and (3) foreigners.[34]
"Teachers, Students Want to Keep Out Foreigners with AIDS," Japan Times, April 30, 1987.
Government attempts to educate the public about AIDS prevention stressed the danger of sexual intercourse with foreigners, and may have perpetuated the ready association of foreigner with AIDS carrier. According to Feldman, the Kobe city government distributed a comic book to 70,000 high school students which showed "a map of the world with a large finger pointed at Africa, and a boatload of devilish-looking creatures sailing toward Mount Fuji."[35]Feldman, "AIDS in Japan," p. 15.
Public opinion surveys show that awareness of, and personal concern about, contracting AIDS stabilized by at least May 1987.[36]
Prime Minister's Office, "Public Opinion about AIDS," May 1987; Gallup Organization, "AIDS: A Multi-Country Assessment," Public Opinion, May—June 1987.
As in the United States, the distribution over time of data about the means of transmitting the AIDS virus indicates a certain degree of confusion on the part of the public. For example, in a sample of 1,400 blood donors in February 1988 at twenty-one Red Cross donation centers across Japan, 13 percent of the respondents who said they would not donate blood in the future cited the possibility of getting AIDS as their reason.[37]Japanese Red Cross Society, Questionnaire on Blood Donation, February 1987.
The number of blood donors fell by nearly 5 percent in 1987, thesecond consecutive yearly decline.[38]
Jennifer J. Lin, "Attitudes and Awareness on AIDS in Japan," Master's Thesis, School of Medicine, Case Western Reserve University, Cleveland, 1987.
One media analyst suggests that public response to sensational mass media coverage of AIDS has counterbalanced other effects from the mass media; specifically, the fear of contracting AIDS may have reversed a trend toward increased extramarital sex by Japanese women, a trend influenced by exposure to popular television soap operas featuring married women involved in extramarital sex.[39]Shigehiko Shiramizu, personal correspondence, November 11, 1988.
Respondents to a May 1987 survey about AIDS said that they had learned about AIDS from (1) television, (2) daily newspapers, (3) weekly newsmagazines and tabloids, and (4) other people. The weeklies, which carried the most sensationalistic and perhaps inaccurate coverage of AIDS, were cited as an information source about AIDS by 53 percent of respondents aged twenty to twenty-nine, who are most sexually active.[40]
Prime Minister's Office, "Public Opinion about AIDS."
National Aids Policy
After January 1987 Japanese government officials were aware that the government had to play a role in AIDS education and prevention. Official collection of AIDS data was entrusted to the Ministry of Health and Welfare's AIDS Surveillance Committee. This committee served as a coordinating body for linking the efforts of other groups, such as the Ministry's Blood Products Division, its AIDS Patients and Virus Carriers Future Estimate Research Group, the private AIDS Prevention Foundation, the Japan Public Health Association, the Japan Society for AIDS Education, the Tokyo Metropolitan Research Group on AIDS, and prefectural public health departments.
Despite this intra-Ministry coordination, traditional animosity between the Ministry of Health and Welfare and the Ministry of Education has prevented any cooperation regarding AIDS prevention and education. The Ministry of Health and Welfare has jurisdiction over epidemiological research and patient treatment for the disease, and has received supplementary funding from the Ministry of Finance for both tasks. Although the Ministry of Education has supported some educational programs on AIDS awareness and prevention, it has not received supplementary funding for AIDS education from the Ministry of Finance. There is, then, a lack of funding for AIDS education in Japan; there is also virtually no money for educational campaigns about discrimination against individuals perceived by Japanese to be at high risk. Because of the low incidence of sexually transmitted AIDS in Japan,
this task of defusing discrimination among Japanese has been identified as by far the most important aspect of AIDS in Japan by the Japan AIDS Prevention Association.[41]
Personal interview with Bin Takeda, October 27, 1988; AIDS Education I, March 1988, entire issue.
Between 1987 and 1988 the amount of money allocated by the national government for AIDS doubled, from $7.2 million to $15.7 million, but subsequent annual funding has not increased at such a high rate.By late January 1987 the Ministry of Health and Welfare had published 1.5 million copies of two AIDS pamphlets. One was distributed to the general public through local governments, medical institutions, and public health centers; the other pamphlet was for public health center counselors. In early February another pamphlet was produced for the general public.[42]
"Health Ministry Issues AIDS Booklet," Japan Times, February 3, 1987.
By late February the Ministry proposed AIDS legislation that included (1) fines and prison sentences for AIDS carriers who continued to have sex or to donate blood, (2) fines for doctors who failed to report AIDS cases, and (3) the right to refuse entry into Japan to foreigners previously identified as AIDS carriers.[43]"Proposed AIDS Legislation to Be Presented to Diet," Japan Times, February 27, 1987; "Law Would Bar Aliens with AIDS," March 27, 1987.
A watered-down version was soon passed by the Social Affairs Subcommittee of the ruling Liberal Democratic Party. The bill eventually stalled in the Diet.The Ministry of Health and Welfare soon directed local governments to assist in the dissemination of AIDS educational materials, set up AIDS consultation centers for concerned people, and provide special counseling services for AIDS carriers.[44]
"Directive on AIDS Sent to Local Governments," Japan Times, March 19, 1987.
Acupuncturists were ordered to use only disposable needles.[45]"Use Needles Once: AIDS Notice to Acupuncturists," Japan Times, March 25, 1987.
A nationwide public health campaign included the distribution of 340,000 AIDS prevention posters, a toll-free telephone counseling service, and AIDS reference books for physicians.[46]
"Gov't Outlines AIDS Information Campaign," Japan Times, March 28, 1987.
The Japan AIDS Prevention Association distributed videos and sponsored seminars on AIDS.[47]"Know-Your-Enemy AIDS Campaign," Japan Times, April 19, 1987.
The national government also distributed public service announcements, which were aired on television stations.[48]Interview with Mazaki.
Schools were instructed to distribute teaching manuals and videos about AIDS prevention to teachers in March 1988. Apparently, little use was made of these materials. Many teachers refused to talk about a topic that they were unfamiliar with and regarded as offensive. The Ministry reported that the anti-AIDS video was shown at only 3 percent of big-city schools and at less than 1 percent of rural schools. The opposition of school teachers was understandable, since sex education had not previously been a topic discussed in junior or senior high school.After the Mainichi Shimbun exposé in February 1988, hemophiliacs found it easier to influence national health policy. Hemophiliacs successfully defeated national legislation that they considered discriminatory.
They also demanded monetary compensation from the national government and from pharmaceutical companies, as well as a formal apology from the Ministry of Health and Welfare.[49]
"Hemophiliac Association Demands Compensation for Wrongdoing," Mainichi Shimbun, February 9, 1988.
Though the national government has steadfastly refused to accept blame or to apologize, Japanese pharmaceutical companies finally decided to "donate" 200,000 yen per month (about 1,500 U.S. dollars at an exchange rate of 130 yen to the dollar) to each hemophiliac eighteen years of age or over, and 80,000 yen per month to those under eighteen, who have been infected with the AIDS virus through blood coagulant.[50]NHK Television Evening News, "Pharmaceutical Companies Make Offer," October 20, 1988.
Persons in the general public not personally affected by the disease may have sensed that the issue of AIDS in Japan had reached a stage of resolution.Noboru Takeshita, then prime minister, promised that the government would financially assist hemophiliacs by covering the costs of treating asymptomatic patients as well as some inpatient hospital costs.[51]
David Swinbanks, "Relief in Sight for HIV-Carrying Japanese Haemophiliacs," Nature 333 (May 5, 1988): 5.
By September 1988 this promise was specified as paying up to 180,000 yen (about 1,500 U.S. dollars) per month to hemophiliacs with AIDS, payments of about $45,000 to families of hemophiliacs who have died of AIDS, about $1,000 for funeral expenses, and about $80 per month to hemophiliacs who test positive for antibodies to the HIV virus.[52]"Gov't to Compensate Hemophiliacs with AIDS," Mainichi Daily News, September 15, 1988.
So the national government, mostly through the Ministry of Health and Welfare, did take action on AIDS. Yet its public response was not only slow but also, for several years, directed toward the wrong risk groups. Many Ministry statements about AIDS referred to the threat of disease spread by homosexuals and drug users; in effect, the Ministry was echoing the epidemiology of AIDS in the United States and seemingly refusing to acknowledge that the disease was following a completely different epidemiology in Japan. This mistargeting of risk groups led some critics, particularly hemophiliacs and their representatives, to charge that Ministry AIDS policy was deliberately deceitful. Perhaps a more likely explanation is that the Ministry had not conducted epidemiological research about AIDS in Japan prior to 1987, and there were few reported cases of AIDS.
The Ministry of Health and Welfare refused to criticize the activities of its former AIDS Surveillance Committee chairman, Dr. Abe. Somewhat remarkably, Abe has not been the target of official sanction by either the Ministry, the Japanese medical association, or his university.
The Nonissue Of Aids In Japan
The previous three sections suggest that the issue of AIDS has reached a certain "maturity" on the mass media news agenda, in the public
consciousness, and in the minds of policymakers in Japan. If the salience of public issues can appropriately be thought of as cyclically rising and falling,[53]
Anthony Downs, "Up and Down with Ecology: The Issue-Attention Cycle," Public Interest 28 (1972): 38-50.
then the issue of AIDS is clearly ebbing at present in Japan. Because of a unique epidemiology (in that most AIDS cases were transmitted nonsexually), the disease is not as much of a public health threat in Japan as it is in some other countries.The real threat as a result of AIDS in Japan is the generalized perception, demonstrated through public opinion surveys, that anyone other than a "normal" Japanese—meaning foreigners, Japanese hemophiliacs, Japanese homosexuals, and Japanese IV drug users—is likely to have AIDS and should be avoided. In interviews during 1988 Japanese respondents said that they avoided grasping subway handles or using toilets, public telephones, and water fountains after non-Japanese had done so.
Even though it has fallen from importance on the agendas of the mass media, the general public, and policymakers, the issue of AIDS, like the disease itself, has not gone away. The issue has been routinized and institutionalized. Consider the following points:
1. In mass media organizations AIDS is now one of the health problems about which health and science reporters must consider writing. For journalists the issue stands as another example of why reporters must critically appraise the information they receive from authoritative news sources.
2. For the Japanese hemophiliacs who will live through the epidemic, the issue may bring legitimacy to their public identity. The unified response to the disease and to the government has led to far greater efficacy for the National Hemophiliac Society. Though the persons infected by coagulant have yet to receive the full apologies and money that they have demanded, the government and the blood companies have acknowledged some degree of fault. These acknowledgments, which have been reported by the mass media, may suffice as indications to the general viewer and reader that the problem has been handled (and thus that the issue is cognitively routinized).
3. The national government now has a network of offices, counseling centers, and hospitals which deal explicitly with AIDS. Routes for diffusing information about the disease are now established. The Ministry of Health and Welfare has a coordinating AIDS Office. The government has financially contributed (although modestly) to the efforts of the World Health Organization in attempting to curb the worldwide spread of AIDS.
This evidence that the issue of AIDS has been routinized in Japan represents a somewhat typical response to social problems. By this process of institutionalization, issues are legitimized. Legitimization is a goal of issue proponents. In the present case hemophiliacs sought to legitimize the idea that they had been victimized by the government, blood companies, and their doctors. The legitimization process, made visible through institutionalization, transforms an issue into a nonissue. The perception results that "something is being done" and finally that "the problem has been resolved." As early as February 1988, the Japan Times editorialized that "the AIDS problem is being marginalized" and that there is a "growing complacency" about the disease.[54]
"AIDS and Complacency," Japan Times, February 29, 1988.
A Comparative Conclusion About Society And An Epidemic
The present essay has told the story of AIDS in Japan by focusing on how the mass media, public-interest groups, and government policymakers influence one another in defining and controlling a public issue. When this history is compared with the history of the issue of AIDS in the United States,[55]
See Rogers, Dearing, and Chang, "AIDS in the 1980's."
several comparative conclusions can be drawn about how societies deal with an epidemic.1. Both national governments responded very slowly to the threat of AIDS. In both countries groups assumed to be at high risk for AIDS had been ostracized from society prior to the threat of AIDS; when they were identified as at high risk for AIDS, they were stigmatized even further. A main reason for slow government action was that the disease primarily affected groups outside of mainstream society. In Japan, a relatively homogeneous society, little accommodation by the national government was offered to minority or ostracized societal groups whose members are most affected by AIDS. In the United States, a relatively heterogeneous society, the national government has been far more accommodating of the demands of affected societal groups. The egregious government AIDS scandal in Japan faded from the public consciousness after media coverage subsided, the villain never punished. Competition from other public issues (such as the Recruit Cosmos scandal in which public officials were given large amounts of corporate stock), combined with a lack of new sensational information about AIDS, drove this issue down the agendas of producers, news editors, and reporters. Such a scandal most certainly would have been rectified more in line with the demands of the affected societal groups if it had occurred in the United States.
2. Certain of the mass media in each country provide examples of outstanding investigative journalism centered on government inaction. In each country such media coverage led to changes in national government policy regarding AIDS. In Japan heroic journalism was largely ignored by the other, competing mass media. In the early 1990s AIDS is a nonissue in Japan. In the United States heroic journalism by a few sources eventually put AIDS on the news agenda of virtually all the mass media. The disease has remained on the U.S. news agenda, no doubt influenced by editors' perceptions of issue salience. In comparison with Japan, the United States has a far greater number of people with AIDS, persons carrying the virus, and especially people who know someone with AIDS.
3. In each country the amount of mass media coverage skyrocketed when perceptions spread that AIDS was a threat to the general heterosexual population. In Japan people perceived that the disease was relevant to them when it became known that Japanese prostitutes had AIDS. Extramarital sex is common in Japan. In the United States the illness of Rock Hudson, a movie star who was a stereotype of masculinity, and especially the illness of a teenage schoolboy, Ryan White, gave people the impression that anyone could get AIDS.
4. Policy solutions to AIDS have not satisfied claimants in either country, particularly in Japan. Policy actions in response to mass media coverage of an issue provoke an image of issue resolution to the general public, regardless of whether the issue has really been resolved. In Japan hemophiliacs are still very angry at the government, but the lack of current attention in the mass media means that the government need not respond. In the United States the sheer number of AIDS patients, as well as extrapolations of future patient loads, demands a more proactive government set of policies toward AIDS. Yet, aside from the much greater real-world problem of AIDS in the United States, the present results suggest that in the United States well-organized public-interest groups, such as gay political activists, have been able to affect policy (in contrast, IV drug users are paid little heed by the U.S. government because their interests and needs are not represented by a well-organized political action group), whereas in Japan such groups (even the well-organized National Hemophiliac Society) apparently play a much lesser role in the formation of national policy.
Medical Research on AIDS in Africa:
A Historical Perspective
Randall M. packard
Paul Epstein
The history of Western medical research on AIDS in Africa closely resembles earlier attempts by Western-trained medical researchers to understand the epidemiology of infectious diseases, such as tuberculosis and syphilis, that were known in the West but that appeared to exhibit different epidemiological patterns in Africa. Like research into TB and syphilis, early inquiries into AIDS in Africa attempted to understand why African experience with the disease differed from Western experience. All of these efforts were handicapped by the limited state of Western knowledge about these diseases, an absence of adequate epidemiological data for Africa, and a lack of knowledge about the African societies and cultures within which these diseases occurred. Despite these shortcomings, early medical researchers quickly constructed theories to explain the peculiarities of the African disease experience. These theories were strongly influenced by cultural assumptions about Africa and Africans and tended to focus on the peculiarities of African behavior.[1]
In this regard, of course, Western medical research on AIDS in Africa also resembles the earlier development of medical ideas about diseases in Europe and the United States. Thus, Charles Rosenberg notes in his history of cholera in nineteenth-century America, "A disease is no absolute physical entity but a complex intellectual construct, an amalgam of biological state and social definition" (Charles Rosenberg, The Cholera Years [Chicago: University of Chicago Press, 1962], p. 5). More recently Susan Sontag and Sander Gilman have observed that a number of metaphors have been embedded in the medical construction of AIDS in the West.
Once these theories were constructed, they shaped the course of subsequent research, privileging certain lines of inquiry while largely excluding or marginalizing other potentially important areas of research.In this essay we compare the development of AIDS research in Africa with the history of earlier efforts by Western medical professionals to understand the epidemiology of TB and syphilis. By drawing these parallels, we hope to contribute to a clearer understanding of how Western medical ideas about AIDS in Africa developed and how these ideas have
A different version of this essay is forthcoming in Social Science and Medicine and is reprinted with the editor's permission.
shaped the direction and boundaries of African AIDS research and, ultimately, our understanding of the epidemiology of AIDS in Africa.
Tuberculosis And The "Dressed Native"
Early discussions about the causes of black susceptibility to TB centered on the problem of explaining why Africans had higher rates of morbidity and mortality than Europeans. At the time little was known about the nature of host resistance to the disease or about the role of cofactors in the transmission of infection and in the progression of infection to active disease. Research on TB was in fact in transition from the hereditary arguments of the late nineteenth century to Koch's germ theory. In addition, knowledge of African social and economic life was limited and was infused with racial and cultural stereotypes. Predictably, the explanations of European medical authorities came to reflect the perceptions about Africans that were current in European colonial society.
Central to these perceptions was the image of the "primitive native" making a difficult adjustment to conditions of a "civilized" industrial world. This image, embedded in European discussions of African morality, political participation, and labor skills, came to influence early explanations of TB in Africa. Africans were viewed as more susceptible to TB because they had not adjusted to the conditions of a civilized industrial society; their incomplete adoption of Western clothing and their failure to observe "proper" dietary and sanitary laws symbolized this lack of adjustment.
At the same time, it was argued that Africans who remained in their customary rural environment, working in the open air and wearing traditional attire, were generally healthy. These explanations for African sickness and health, focusing attention on the Africans' maladjustment to civilization, placed responsibility for the adverse living conditions of Africans squarely on the shoulders of Africans themselves and deflected attention from the low wages and inadequate housing policies of employers and government officials. More importantly, these explanations shaped the development of TB control measures, which came to focus naturally on education rather than on social and economic reform. Blacks had to be taught about the dangers of living in overcrowded housing and eating nutritionally inadequate diets, as if they chose to do so out of perversity rather than out of economic necessity.
Later on, discussions about African susceptibility to TB became infused with biological arguments that focused on the Africans' lack of experience with the disease and their consequent lack of physiological resistance to it. Like earlier behavioral arguments, physiological models defined the African as essentially different from the European, as the "other," and at the same time placed responsibility for the disease on the victim.[2]
R. Packard, "Tuberculosis and Industrial Health Policy on the Witwatersrand, 1902-1932," Journal of Southern African Studies 13 (1987): 187-209.
Not until the middle of this century did health officials come to see that the adverse environmental conditions under which Africans lived were not of their own making. Even then, environmental reform efforts continued to be hampered by behavioral explanations that emphasized the Africans' difficult adjustment to the conditions of Western industrial civilization. Typical of this discourse is the following statement by the director of Kenyan medical services in 1963:The African in his rural setting is strictly bound by tribal patterns of behavior, beliefs and customs. He is an integral part of his community and his thinking tends to be communal. … With the transposition to the town he forsakes the communal life for an individualistic life, unsupported by tribal rules and regulations. While forsaking these supports, he is not yet ready to adopt the codes and rules which have brought social stability to western civilizations. Furthermore, he is abandoning ingrained centuries of agricultural and pastoral tradition and learning the technical skills of an industrial world quite strange to him.[3]
N. Fendell, "Public Health and Urbanization in Africa," Public Health Reports 78 (1963): 574.
Even today TB control programs in Africa continue to view TB as a behavioral problem, attributing treatment failures to "patient default" rather than to the government's failure or inability to cope with environmental factors that continue to generate new cases of this disease.
Syphilis And African Sexuality
The recent work of the historian Marc Dawson on the history of syphilis in East Africa provides another example of how earlier Western medical researchers came to construct a behavioral paradigm to explain the peculiarities of African disease experience and how these models shaped medical responses to this experience.[4]
Marc Dawson, "Socio-economic and Epidemiological Change in Kenya: 1880-1925," Ph.D. diss., University of Wisconsin-Madison, 1983, pp. 211-18.
The epidemiology of syphilis, like that of tuberculosis, was not well understood by Western medical researchers during the first decades of this century. Specifically, the epidemiological and pathological differences between yaws, venereal syphilis, and endemic or nonvenereal syphilis had yet to be sorted out. As a result, there was considerable confusion among early medicalpersonnel working in Africa. This confusion led early European observers to regard the African experience with the disease as different from the European and to look for the reasons for this difference. As with TB, early theories about syphilis in Africa focused on behavioral theories that were infused with racial stereotypes.
Early medical researchers in East Africa concluded that between 50 and 90 percent of the African population in parts of Kenya and Uganda were infected with venereal syphilis. Col. F. J. Lambkin, a leading British expert on syphilis, who was seconded to Uganda to study the problem, concluded in 1906: "As things are at present, the entire population is in danger of being exterminated by syphilis in a very few years, or of being left a degenerate race fit for nothing."[5]
Quoted in Dawson, p. 212.
In explaining this extraordinary situation, Lambkin concluded that the major cause of the epidemic was a breakdown of various Ganda social institutions. In this respect he echoed early medical opinions about the spread of TB, as well as later theories about AIDS. Specifically, Lambkin argued that Christianity had broken down customs that restricted the social movement of women. At the same time, sanctions against adultery had been eliminated at the behest of the British colonial government. These changes, he argued, had permitted Ganda women to engage in "promiscuous sexual intercourse and immorality ," resulting from "their natural immoral proclivities " (emphasis added). Lambkin further indicted the Bahima of Ankole as primary disseminators of the disease because of their practice of allowing a man's age-mates and visitors to have sex with his wife.[6]Quoted in Dawson, p. 213.
Similar claims were made by observers in western Kenya. G. L. Gilks, discovering what he believed to be a major epidemic of venereal syphilis in Kavirondo, concluded: "The whole attitude of the native toward sexual matters renders it certain that venereal disease, once introduced, is bound to spread among old and young."[7]
Quoted in Dawson, p. 230.
On the basis of subsequent studies and a careful reexamination of the medical evidence, Dawson suggests that what Lambkin and Gilks were observing was not an epidemic of venereal syphilis but nonvenereal or endemic syphilis, which is caused by the same Treponema pallidum spirochete that causes venereal syphilis. Endemic syphilis, however, spreads through bodily contact in warm climates and in the absence of adequate sanitation. According to Dawson, syphilis was clearly being spread sexually into various parts of East Africa as a result of the development of migrant labor, commercial centers, military movements,
and a growing population of African prostitutes; however, its subsequent spread among large numbers of men, women, and children in rural and urban areas was via bodily contact.
The point of this episode is not simply that the disease was misdiagnosed. After all, the differences between yaws, venereal syphilis, and endemic syphilis were difficult to sort out and in fact were not clearly understood until the 1930s. The importance of this episode lies instead in the way these early medical observers constructed the medical evidence they were observing to fit preexisting assumptions about African sexuality and disease. Seeing a disease, which they assumed to be venereal syphilis, Lambkin, Gilks, and others readily constructed a theory to explain its extraordinary rate of spread. That theory was based on assumptions about the extreme sexuality of Africans—assumptions for which they had virtually no empirical evidence. This is not surprising. As Sander Gilman notes, the association of Africans with sexuality and the tendency to link African sexuality with disease have a long history in Western thought.[8]
Sander Gilman, Difference and Pathology: Stereo Types of Sexuality, Race and Madness (Ithaca, N.Y.: Cornell University Press, 1985); and Disease and Representation: Images of Illness from Madness to AIDS (Ithaca, N.Y.: Cornell University Press, 1988).
By the end of the nineteenth century, when European powers began carving out African colonies, the association could be found in many works of literature and art in continental Europe and held a central position in the constellation of ideas that made up European perceptions about Africans. As a result, early medical authorities, missionaries, and colonial administrators came to Africa with certain strong assumptions about African sexuality. There can be little doubt that these presumptions colored both their epidemiological findings and their control efforts. Following this behavioral explanation, these authorities advocated public health policies that centered largely on the development of measures, often draconian in nature, to control the behavior of prostitutes. At the same time, problems associated with living conditions and sanitation, which were in fact centrally important to the spread of endemic syphilis, were ignored.Aids And The "Sexual Life Of The Natives"
Early discussions of AIDS in Africa developed in an intellectual environment similar to that in which early inquiries into TB and syphilis were conducted. When medical researchers first began studying AIDS in Africa, they quickly realized that the epidemiology of the disease was different from that in the West. The ratio of male to female cases was 13:1 in the West, whereas the ratio in Africa was nearly 1:1. This fact, combined with an apparent absence of known risk groups in the form
of either IV drug users or homosexuals, led early researchers to conclude that AIDS transmission in Africa was different from that in the West. They therefore tried to determine what it was about Africa and Africans that accounted for its peculiar pattern of transmission.
In trying to explain transmission patterns in Africa, AIDS researchers were handicapped by limited knowledge about the etiology of the disease. Thus, when African AIDS cases (or what seemed to be AIDS cases) first began appearing in Belgium in 1983, the infectious agent causing AIDS had not yet been identified. In addition, early discussions of AIDS in Africa occurred, and in fact continue to occur, in the absence of any clear understanding about the role of various cofactors in either the transmission or the progression of HIV infection. Finally, early AIDS researchers had only limited experience or knowledge of the societies and cultures within which AIDS was occurring in Africa.
This lack of social and medical knowledge, combined with the suspicion that the key to understanding AIDS in the West might lie in Africa, contributed to a great deal of speculation about the epidemiology of AIDS in Africa and encouraged researchers to construct hypotheses that often were based on extremely limited data. It is therefore not surprising that stereotypic images of Africa and Africans entered into the discourse on the epidemiology of AIDS in Africa.
Early reports on AIDS in Africa took a somewhat eclectic approach to the question of why African populations exhibited an epidemiological pattern different from that of populations in the West.[9]
See, for example, Peter Piot et al., "AIDS in a Heterosexual Population in Zaire," Lancet 1, no. 8394 (July 14, 1984): 67.
However, a number of influential Western AIDS researchers concluded early on that the apparently equal sex ratio of AIDS cases in Africa was most easily explained by a pattern of heterosexual transmission, a phenomenon relatively rare in the West at that time. This conclusion was supported by early prevalence studies, which seemed to indicate that both cases and HIV seropositivity were most frequent among sexually active adults. But why, then, was HIV occurring through heterosexual transmission in Africa and not to any great degree in Europe or America?This question quickly led to two theories. The first argued that AIDS had existed in Africa for a longer period of time than in the West and therefore had reached a different stage in its epidemiological history. This theory—combined with the virological research of Essex, Gallo, and others on Simian T-Lymphocyte Retrovirus III in African green monkeys—led to arguments that AIDS originated in Africa.[10]
R. C. Gallo, "The AIDS Virus," Scientific American, January 1987, pp. 39-48; P. J. Kanki, J. Avroy, and M. Essex, "Isolation of T-Lymphotropic Retrovirus Related to HTLV-III/LAV from Wild African Green Monkeys," Science 230 (1985): 951-54.
This hypothesis was hotly debated on scientific grounds. More important, it ignited a political firestorm among African political leaders, who regardedthe theory as imperialist scapegoating.[11]
For a fascinating account of this debate from an African perspective, see C. Chirimuuta and J. Chirimuuta, Aids, Africa and Racism (Trenton, N.J.: Africa World Press, 1989).
This produced a political environment in which the cooperation of African governments in further AIDS research appeared to be in jeopardy. As a result, the Western medical research community appears to have put aside the question of African origins as well as investigations into the possibility that HTLVIII may have achieved a different epidemiological stage in Africa.[12]For one notable exception to this pattern, see N. Nzilambi et al., "The Prevalence of Infection with Immunodeficiency Virus over a 10-Year Period in Rural Zaire," New England Journal of Medicine 318 (September 27, 1986): 707-9. This question deserves more research.
The second theory put forth to explain the heterosexual transmission of HIV in Africa focused on African sexual behavior. In brief, it was argued as early as 1985 that the heterosexual transmission of HIV in Africa was the result of higher levels of sexual promiscuity among Africans, or, in the current language of social science research on AIDS, "poly-partner sexual activities." The middle-class businessman or bureaucrat with a string of lovers; the truck driver with sexual contacts all across the African map; and, above all, the pervasive female prostitute, who was said to have literally hundreds of contacts each year—these people were identified as the main vectors of HIV transmission in Africa. Although the association of AIDS in Africa with sexual promiscuity was challenged by both African observers and others with broad knowledge of African societies and cultures, it nonetheless persisted and, like earlier stereotypes concerning black susceptibility to TB and syphilis, became the central focus of medical inquiries into the problem of AIDS.
Why, given all the social and economic factors that distinguish African populations from those in the West, did researchers choose to focus on sexual promiscuity? Officially, the conclusion was said to be based on medical evidence, including studies which indicated that Africans who had multiple sexual partners and other STDs were statistically at higher risk of being infected with HIV than those who did not. Yet evidence for this conclusion, as well as for the association of HIV infection with the years of peak sexual activity, was extremely limited prior to 1986. Therefore, other factors probably contributed to the development of this explanation.
One such factor appears to have been the association of AIDS in the West with the alleged sexual promiscuity of homosexuals. In essence, AIDS was defined as a sexually transmitted disease that was spread in the West within a population defined as sexually promiscuous. Its heterosexual spread in Africa therefore implied similar levels of promiscuity. More than one Western AIDS researcher, in fact, suggested that African heterosexuals had a pattern of promiscuity similar to that of
promiscuous gay men in the United States and Europe (a conclusion that incorporated two discriminatory stereotypes).[13]
Peter Piot et al., "Heterosexual Transmission of HIV," AIDS 1 (1987): 199-206. A similar statement is attributed to N. Clumeck, a Belgian AIDS researcher who was apparently one of the earliest and strongest proponents of the sexual promiscuity theory (Report on the Second International Symposium on AIDS in Africa, reported in Washington Post, October 10, 1987).
More broadly, Western research on AIDS had already defined AIDS as a behavioral problem associated with aberrant life-styles.[14]See Gilman, Disease and Representation, for a discussion of the early construction of AIDS in the West as a disease associated with deviancy.
There was thus a predisposition to look for "deviance" in an African setting.Yet the role of sexual promiscuity in the spread of AIDS in Africa appears to have evolved in part out of prior assumptions about the sexuality of Africans. Thus, at a 1985 conference on AIDS held in the Central African Republic, Dr. Fakhri Assaad of the World Health Organization referred to the widespread pattern of "polygamy without wedding rings" in Africa. According to Assaad, this pattern resulted from the tendency of men to consider it a status symbol to have several wives or mistresses. He noted that, in reference to sexual and other cultural practices that might facilitate the transmission of HIV, that many of the practices had deep religious and traditional significance. In a similar fashion, researchers describing the sexual practices of patients suffering from "Slim Disease" in Uganda in 1985 observed that, although their subjects denied overt promiscuous behavior, they were "by western standards heterosexually promiscuous."[15]
D. Serwadda et al., "Slim Disease: A New Disease in Uganda and Its Association with HTLV-III Infection, "Lancet 2, no. 8460 (October 19, 1985): 849-52.
These researchers based their conclusion on the testimony of ten HIV-positive truck drivers who admitted to engaging in homosexual behavior. Labeling homosexual behavior as promiscuous by Western standards may have been consistent with the dominant view of Western society. Yet surely the issue in this case was not promiscuity but the fact that these subjects engaged in a known risk behavior. Nonetheless, it was not the homosexual behavior per se that was presented as the risk behavior, but the subjects' promiscuity.Yet another example of this tendency to view Africans as sexually promiscuous can be found in a study that compared HIV infection among prostitutes and female controls in Rwanda. Commenting on their sampling procedures, the authors of this study noted, "Matching of the female controls was not extended to marital status since, for the age group studied, celibacy [single status] in women is unusual in Central Africa and commonly associated with prostitution " (emphasis added), a conclusion for which the authors presented not a shred of evidence.[16]
P. Van de Perre et al., "Female Prostitutes: A Risk Group for Infection with Human T-Cell Lymphotropic Virus Type III," Lancet 2 (September 7, 1985): 524.
The parallel between these attitudes and those of early medical personnel faced with an epidemic of syphilis in East Africa, described above, along with the absence of any reliable data supporting these conclusions, forces us to ask whether the attitudes of medical researchers toward
AIDS in Africa did not also have their basis in a deeply imbedded image or trope which continues to shape Western medical and popular thought about African sexuality.
In a similar vein, it has been suggested that other cultural practices—such as scarification, the therapeutic use of razors, and female circumcision—might also play a role in the spread of HIV. Like sexual promiscuity, these risk behaviors were seen as culturally determined.
The Role Of Anthropologists
Having constructed AIDS as a behavioral problem resulting from particular culturally sanctioned practices, AIDS researchers turned to anthropologists for information on these practices. One might expect that social scientists with extensive African experience would have challenged the sexual stereotypes developed by medical researchers. Such challenges did not, however, occur to any great degree. Although recent social science research has questioned some of the behavioral assumptions underlying AIDS research in Africa, the activities of those social scientists who were most closely linked to the AIDS inquiry in its early stages tended to reinforce these assumptions.
Probably the main reason why anthropologists failed to challenge the dominant paradigm in AIDS research had to do with the conditions under which social scientists were brought into the AIDS inquiry. Instead of engaging in an open-ended dialogue with social scientists, assessing available data, and discussing how research methods and agendas might be modified to fit more closely with the contours of African experience, the medical research community expected the social scientist to adhere to the dominant behavioral model. Specifically, they asked anthropologists and other social scientists to provide information about the "risk behaviors" that might facilitate the transmission of AIDS. In other words, what were the practices, customs, or patterns of social intercourse that provided opportunities for HIV transmission? Constructed in this way, the question immediately narrowed the range of sociological data relevant for the discussion. The question became not "What is the social context within which HIV transmission occurs in Africa?" but, rather, "What are the patterns of behavior which are placing Africans at risk of infection?" While the first construction would have allowed for open-ended discussion of a wide range of social, political, and economic conditions that might be affecting health levels in Africa, the latter formulation quickly narrowed discussion to an inquiry
into the "customs of the natives." At the same time, it placed responsibility for transmission on the actors themselves in a not too subtle form of victim blaming.
The result of this emphasis on "risk behaviors" was that anthropologists found themselves being asked to dig through the ethnographic record on African cultures in order to identify possible patterns of behavior that might facilitate HIV transmission. This exercise resulted in conferences, workshops, and seminars in which the medical community was presented with an array of information that was often excised from its social or economic context and presented in much the same way as ethnographic artifacts are presented in natural history museums. Descriptions and pictures of scarification taken among the Nubia in the 1940s and 1950s were displayed as examples of possible "risk behaviors" involving blood transfers. From the broad array of data on African sexual practices imbedded in the ethnographic record of Africa, data revealing a wide range of patterns and extreme variation with regard to sexual permissiveness anthropologists presented only those cases that constituted possible "risk behaviors." Take, for example, the following description of "risk behavior" reported in a survey on "Social Factors in the Transmission and Control of AIDS in Africa" commissioned by the United States Agency for International Development (USAID):
There is a widespread fear of impotence [in Africa]. Our readings mention instances where an older man might ask a younger man to impregnate his wife. The Gwembe Tonga of Zambia use euphemistic invitation in these circumstances—"go and cut wood for me, my friend." … This illuminates our understanding of the perception of sexuality in certain traditional African settings but also indicates another—though limited—instance of a possible route for spreading AIDS through increasing the number of sexual partners.[17]
David Brokensha et al., "Social Factors in the Transmission of AIDS in Africa," report prepared for the Directorate for Health, Bureau for Science and Technology, Agency for International Development, 1987.
The same report contains a lengthy description of ritual sexual intercourse involving the widows of deceased men among the Giriama of Kenya. The authors follow the description with the observation "Clearly if the widow's deceased spouse was an AIDS victim then this custom will contribute to the spread of the disease."
In a similar vein, Daniel Hrdy, who is trained in both medicine and anthropology, wrote in an article on cultural practices relating to HIV transmission in Africa, "Although generalizations are difficult, most traditional African societies are promiscuous by Western standards. Promiscuity occurs both premaritally and postmaritally. For instance, in the Lese of Zaire, there is a period following puberty and before
marriage when sexual relations between young men and a number of women is virtually sanctioned by the society."[18]
Daniel B. Hrdy, "Cultural Practices Contributing to the Transmission of Human Immunodeficiency Virus in Africa," Reviews of Infectious Diseases 9 (November-December 1987): 1109-19, at p. 1112.
This article was circulated in advance to the 300 or so participants who attended a conference on Anthropological Perspectives on AIDS (sponsored by the U.S. Agency for International Development and the National Institute of Allergy and Infectious Diseases), presumably because the organizers viewed it as a model of the types of data they hoped would be presented at the conference.These behaviors may very well occur and may be potential avenues for HIV transmission. Reports of this type—by concentrating on "risk behaviors"—exclude from discussion broader patterns of everyday sexual activity, which in many cases are both less exotic and more monogamous. Moreover, they reinforce, perhaps unintentionally, the impression that sexual promiscuity is culturally determined. For example, Edward Green, in a recent article on the role of behavioral scientists in African AIDS research, noted, "Changes in behavior which promote the spread of AIDS will go against social and cultural norms and values in Africa and against deeply ingrained behavioral patterns." Similarly, Francis Conant, writing in the same volume, concluded, "In dealing with AIDS we are not just dealing with sex; we are dealing with life-ways and complex cultural patterns."[19]
E. Green, "AIDS in Africa: An Agenda for Behavioral Scientists," and Francis Conant, "Evaluating Social Science Data Relating to AIDS," in AIDS in Africa, ed. R. Rockwell and N. Miller (Lewiston, N.Y.: Edwin Mellen Press, 1988) pp. 176, 198.
Some of the contributions by anthropologists have been of such questionable relevance to the issue of HIV transmission as to border on being salacious. Take, for example, Hrdy's extensive account of female circumcision.[20]
Hrdy, "Cultural Practices."
After spending a page describing various patterns of female circumcision in detail, he concludes that there is hardly any correlation between areas in which it is practiced and the distribution of HIV infection, leaving the reader to question the need for the descriptive detail. This pattern of selective reporting only reinforced the popular image of African promiscuity and at the same time strengthened the assumption that the heterosexual epidemic of AIDS in Africa was simply a product of the peculiarities of African behavior.Remarkably, some of these same anthropologists cautioned us not to make generalizations about African sexual behavior and suggested that the problem was not generalized sexual promiscuity but "urbanization": "Away from the social constraints imposed by commitments and obligations to a network of kin, there is the opportunity to engage in behaviors, including poly-partner sexual activities, that would be difficult to undertake in the home village due to social constraints."[21]
Brokensha et al., "Social Factors in the Transmission of AIDS," p. 12.
In a similar fashion, Hrdy concluded: "As people leave rural villages andmigrate to urban areas, the general level of promiscuity usually increases. This increase may be attributable in part to the relaxation of traditional village values but appears to be due primarily to the destitution of poor migrant women, who may become prostitutes, and to the greater mobility and rootlessness of young male migrants and soldiers."[22]
Hrdy, "Cultural Practices," p. 1112.
In short, urban promiscuity was the product of the loss of "traditional restraints." The image of the "detribalized" African, the bane of colonial urban authorities, was a central image in earlier discussions of black susceptibility to TB and syphilis. This image, which was fairly well excised from social science discussions in the 1970s, was being resurrected to explain the frequency of heterosexual transmission of HIV and Africans in the 1980s. This explanation both distinguished Africans from the West and placed responsibility for AIDS on the African. Moreover, given the behavioral thrust of the explanation, the recommended response was finding ways to modify urban sexual behavior. "An understanding of the patterns of population movement will help us to identify high-risk mobile populations and to focus educational resources before the virus is established in those populations."[23]Brokensha et al., "Social Factors in the Transmission of AIDS," p. 11.
While this stress on behavioral modification may not have been as manifestly self-serving as the above-described efforts of medical authorities working with TB to see overcrowding and malnutrition as the result of African ignorance, it shared a similar disregard for the root causes of African sexual patterns within an urban environment.The Political Economy Of African Promiscuity
None of this is to deny that AIDS is transmitted heterosexually or that multiple sexual partners may in fact be a common pattern within the rapidly growing urban centers of Africa. However, explanations that viewed this pattern as either a cultural phenomenon or as a product of declining social constraints ignored the context within which urbanization is occurring in Africa. At the same time, by focusing attention on sexual promiscuity and other cultural behaviors, these explanations have deflected attention from other cofactors that may be as important for the heterosexual transmission of AIDS in Africa as frequency of sexual contacts. In addition, concerns about African sexual behavior limit efforts to explore other avenues of HIV transmission.
There is every reason to believe that, whatever cultural attitudes shape African sexuality, the tendency to have multiple sexual partners has
been encouraged by the separation of households. This separation has resulted from patterns of labor migration involving rural households, which often must send one or more of their members to seek wage employment in urban or industrial centers, including plantations and other large-scale agricultural projects. Labor migration, in turn, is the result of specific historical patterns of development in many parts of Africa—especially parts of Eastern Zaire, Tanzania, Rwanda, Uganda, Zambia, and Kenya. These areas all have large populations of impoverished rural households without access to land or labor and with few opportunities for acquiring income within the rural economy. As Hrdy rightfully notes, the numbers of men and women seeking employment in urban and industrial centers have increased dramatically since the early 1970s. What he does not indicate is why they have increased. Clearly, a major reason is that declining commodity prices and the increasing cost of agricultural inputs have made small-scale agricultural production unprofitable. The African small holder in many areas of East and Central Africa cannot make a living on the land other than on outgrower schemes, which are often highly exploitive in their treatment of growers. For these impoverished households, survival depends on access to some form of nonagricultural income, primarily wages. Yet employment opportunities are limited, in part because of the capital-intensive nature of many industries in Africa, and wages are often low, a product of lobbying efforts on the part of employers to ensure profits. All this has led to the creation of a class of semiproletarianized men and women, who work in urban and industrial settings but cannot afford to support their families there, and thus to the almost continual separation of rural households. For both men and women this existence fosters the development of "multiple sexual partners": Women who cannot find other employment often must work full or part time as prostitutes in urban and industrial settings; women left alone at home for long periods of time may take on "lovers"; and men may take on second "wives" near their place of employment.
This pattern of multiple sexual partners has undoubtedly also resulted from the political disruption of family life generated by warfare in places such as Mozambique, Angola, Burundi, and Uganda. Not only are families torn apart by these experiences, but the rape of rural women by marauding guerrilla armies must represent a particularly brutal form of "sexual poly-partnerism," which has little to do with cultural norms. Again, as with the impoverishment and disruption of rural households described above, it is important to understand the forces that have generateed
these wars, including the foreign governments that continue to support one side or the other to serve their own political ends.
It is important to understand that the pattern of multiple sexual partners is shaped by strong social, economic, and political pressures, and not simply by cultural norms. The presence of such forces will limit the success of efforts to control the spread of HIV through sex education, just as these factors have limited efforts to control population growth in Africa.
The parallel between AIDS prevention and birth control is in fact highly relevant. One of the principal obstacles to the success of population control programs in Africa and elsewhere in the developing world has been the economic pressures on parents to produce large families. These pressures, like those leading to the separation of households, have resulted from particular patterns of development that have created high demands for family labor. As long as this demand continues, unprotected sexual activity is going to occur with considerable frequency. For sexual activity is not simply about pleasure. It is also about social reproduction. If efforts to control the spread of HIV infection do not include policies that deal with the underlying causes of both family separation and the high demand for family labor, we may be fighting an uphill battle in trying to reduce the heterosexual transmission of AIDS in Africa through behavioral modification and condom use.
The Impact Of Medical Paradigms On Aids Research In Africa
The early contributions of social scientists to our understanding of the epidemiology of AIDS in Africa, therefore, were not very helpful. Instead of providing information that might have encouraged medical researchers to develop a broader perspective on the social and economic factors shaping the AIDS epidemic, social scientists contributed to a narrowing of research and to the development of a medical model centered on the problem of African sexuality. This paradigm has prevented researchers from exploring factors that may be of equal or greater importance in the transmission and progression of AIDS but which are not suggested by the paradigm. This, we believe, has resulted in a premature closure of African AIDS research. Two of these understudied areas are the role of high levels of background infection and malnutrition, and unsterilized needle use in the transmission and progression of HIV.
The Role Of Background Infections And Malnutrition In Aids
A number of studies have indicated a positive correlation between HIV seropositivity and the presence of other immunosuppressant conditions, such as malnutrition, tuberculosis, malaria, or trypanosomiasis.[24]
J. M. Mann et al., "Human Immunodeficiency Virus Seroprevalence in Pediatric Patients 2 to 14 Months of Age at Mama Yemo Hospital, Kinshasa, Zaire," Pediatrics 78 (1987): 673-77; J. L. Lesbordes et al., "Malnutrition and HIV Infection in Children in the Central African Republic" [letter], Lancet 2, no. 8502 (August 9, 1986): 337-38. For a review of data on the relationship between nutrition, immunity, and infection, see R. K. Chandra, "Nutrition, Immunity and Infection: Present Knowledge and Future Directions," Lancet 1, no. 8325 (March 26, 1983): 688-91; J. Mann et al., "Association between HTLV-III/LAV Infection and Tuberculosis in Zaire," Journal of the American Medical Association 256 (July, 18, 1986): 346; William Legg et al., "Association of Tuberculosis and HIV Infection in Zimbabwe," paper presented at the Fifth International Conference on AIDS, Montreal, June 8, 1989.
Most of these studies assumed that these other conditions have followed on immune suppression caused by HIV infection. Yet a few studies suggest that these immune-suppressant conditions may have preceded HIV infection and facilitated its transmission. Lamoureaux and his colleagues, for example, noted the high incidence of TB in association with HIV infection among Haitians and Africans and evidence that in many cases infection with Micobacterium tuberculosis appears to have preceded HIV infection. They concluded:We feel that the prevalence and persistence of M. tuberculosis infection in Africans and Haitians, along with the concomitant increase, due to the infection, in CD4+ lymphocytes and macrophages, which are the target cells of HIV, as well as the frequent provocation of an immunosuppressed state in such TB-bacillus-infected individuals, probably represents a common factor predisposing these two populations to infection with HIV when exposed to the virus.[25]
G. Lamoureaux et al., "Is Prior Mycobacterial Infection a Common Predisposing Factor to AIDS in Haitians and Africans?" Annales Institut Pasteur/Immunologie 138 (1987): 521-29.
Similarly, Thomas Quinn and his colleagues reported that "the immune systems of African heterosexuals, similar to those of US homosexual men, are in a chronically activated state associated with chronic viral and parasitic antigenic exposure, which may cause them to be particularly susceptible to HIV infection or disease progression " (emphasis added). The authors noted in addition:
Our serological studies, as well as others, demonstrate that Africans are frequently exposed, due to hygienic conditions and other factors, to a wide variety of viruses, including CMV, EBV, hepatitis B virus and HSV, all of which are known to modulate the immune system. … Furthermore Africans in the present study are at additional risk for immunological alterations since they are frequently afflicted with a wide variety of diseases, such as malaria, trypanosomiasis, and filariasis, that are known to have a major effect on the immune system. The frequent exposure to these multiple microbial agents could act collectively or individually to result in immunological modulations rendering a host more susceptible to HIV infection or by influencing disease progression by increased viral replication and cytolysis of T4-positive cells.[26]
T. C. Quinn et al., "Serologic and Immunologic Studies in Patients with AIDS in North America and Africa: The Potential Role of Infectious Agents as Co-factors in Human Immunodeficiency Virus Infection," Journal of the American Medical Association 257 (1987): 2617-21.
Quinn and his associates concluded: "Prospective studies are warranted in different population groups to examine the specific impact of these viral, bacterial, and parasitic infections and other antigenic stimuli on the susceptibility and development of HIV disease."
Unfortunately, such studies are extremely difficult to conduct, and to date none have been reported, although in NIAID's new International Collaboration in AIDS Research program, such studies will be encouraged.
Other studies have suggested that the infectivity of HIV-infected individuals may increase with disease progression. If declining immune function is in turn accelerated by the presence of concurrent infections or malnutrition, then the risk of transmitting infection, through heterosexual contact or otherwise, may be higher in Africans infected with HIV than in other HIV-infected persons who are not subject to the same levels of background infection.[27]
Linda Jackson, "Bioanthropological Perspectives on Endemic Virus versus Epidemic HIV-Infections and AIDS in Tropical Africa," unpublished paper. Jackson suggests that the progression of HIV infections may also be facilitated by the widespread use in an unsupervised setting of antibiotics, antimalarials (especially quinine compounds), and antihelminiths, which can increase levels of chemical immunosuppression and thereby magnify the clinical response to HIV exposure.
The one predisposing medical condition that has been examined in considerable detail is the role of genital ulcer diseases (GUDs), which are seen as disrupting genital epitheliums and thereby facilitating the sexual transmission of HIV.[28]
Robert Ryder et al., "Extramarital Prostitute Sex and Genital Ulcer Disease (GUD) Are Important HIV Risk Factors in 7068 Male Kinshasa Factory Workers and Their 4548 Wives," and Marie Lana et al., "High Prevalence and Incidence of HIV and Other Sexually Transmitted Diseases (STD) among 801 Kinshasa Prostitutes," papers presented at the Fifth International Conference on AIDS, Montreal, June 5, 1989.
Unfortunately, these studies have not controlled for the possibility that HIV is being transmitted by infected needles in the STD clinics where men and women with GUD go for treatment, rather than directly through sexual intercourse. Thus, the relationship between HIV transmission and genital ulcers remains clouded (see below for further discussion of the problem of needle transmission). We should note here that the high degree of attention given to GUDs, in contrast to the relative lack of attention to other infections diseases that might facilitate HIV transmission, is consistent with our argument that AIDS research in Africa has been narrowly focused on the problem of sexual behavior. In this regard it is interesting to note a recent New York Times article reporting the conclusions of AIDS researchers about the spread of AIDS. These researchers have concluded that there is considerable variation in the risk of HIV infection as the result of heterosexual contact. This risk does not appear to be related to frequency of unguarded contacts. Instead, it is evidently related to one of a number of possible cofactors. With the exception of levels of HIV infection, all the cofactors being considered are directly related to sexual contact.[29]Elizabeth Rosenthal, "The Spread of AIDS: The Mystery Unravels," New York Times, August 28, 1990, p. C1.
Presumably no attention is being given to nonsexual factors such as those suggested here.In short, the susceptibility of Africans to HIV and the facility with
which it is transmitted heterosexually may be a direct result of the high background levels of infection and malnutrition and other immunosuppressant conditions that exist in most African countries, and not simply a question of frequent sexual contacts or other "cultural practices."
If background infections do facilitate the transmission of HIV, then it seems likely that the population at greatest risk is not the urban middle class, who appear frequently in AIDS statistics, but the urban poor, who possess higher background levels of infection and malnutrition as a result of their impoverishment and lack of access to adequate medical care. Unfortunately, few studies have accounted for class, and those that have are inconclusive.[30]
For example, Biggar's research in eastern Zaire suggested that there may be a socioeconomic gradient for HIV seropositivity, with seropositivity rates being highest among the poorest agricultural workers he surveyed (R. J. Biggar et al., "Seroepidemiology of HTLV-III Antibodies in a Remote Population in Zaire," British Medical Journal 290 (1985): 810). Joan Kreiss and her colleagues, in their study of Nairobi prostitutes, noted that seropositivity was significantly lower in upper-class (33 percent positive) than in lower-class prostitutes (66 percent seropositive) (J. K. Kreiss et al., "Aids Virus Infection in Nairobi Prostitutes," New England Journal of Medicine 314, no. 7 (February 13, 1986): 414-418). The authors, however, make little effort to explore the constellation of factors that might be associated with "low status," limiting their research instead to the presence or absence of risk behaviors or exposures, such as scarification, transfusions, the presence of STDs, and, most important, the frequency of sexual contacts. Factors such as malnutrition and the presence of other immunosuppressant diseases, which may facilitate the transmission of HIV, were not explored. The study did measure immune levels (T-cell helper/suppressor ratios) and compared those of the seropositives against those of the seronegatives. They did not, however, measure, or at least did not report, the comparative immune levels of high- versus low-class prostitutes. On the other hand, M. Melbye and his colleagues found a positive correlation between high education and occupational levels and HIV seropositivity (M. Melbye et al., "Evidence for Heterosexual Transmission and Clinical Manifestations of HIV Infection and Related Conditions in Lusaka, Zambia," Lancet 2, no. 8516 (November 15, 1986): 1113-15). Clearly, more studies that control for social class are needed.
If it is found that malnutrition and concurrent diseases that suppress the immune system predispose Africans to AIDS infection, and if HIV is transmitted through heterosexual contact, then the potential risk group may be very large indeed, and certainly is not limited to prostitutes, truck drivers, and bureaucrats. The risk group surely will include the rural families from which infected urban workers come and to which they eventually return. In this regard, one would expect to find high prevalence rates in the areas that have traditionally served as labor reserves for the cities which are currently centers for AIDS infection—for example, the Songea area of Tanzania; the Kwango region of Zaire; and areas of northeast Zambia that serve as labor reserves for the copper belt. These areas experience high rates of migration and are thus more likely to be exposed to AIDS infection emanating in the cities than other regions. They are also by definition impoverished regions and thus contain a population that may be particularly vulnerable to AIDS transmission.
Northeast Zambia is an interesting case. For it is not only a labor reserve area but also part of the so-called matrilineal belt of Africa. Hrdy, Brokensha, and Good have suggested that the rising incidence of AIDS in this area may be related to patterns of sexual promiscuity associated with matrilineal descent.[31]
Hrdy, "Cultural Practices," p. 1112; Brokensha et al., "Social Factors in the Transmission of AIDS"; Charles Good, presentation at the Conference on Anthropological Perspectives on AIDS in Africa, January 7, 1988.
For example, Hrdy notes that "in the so-called 'matrilineal belt' centered in south-central Africa, there is an especially high degree of adolescent promiscuity and uncertainty about paternity." He goes on to describe inheritance patterns and concludes that "matrilineal inheritance … may reduce societal pressure to prevent promiscuity; matrilineal societies are often promiscuous societies." Whether or not this assertion is correct, linking matrilineality with HIV transmission represents a clear case of decontextualization, which ignores the wider social and economic conditions associated with participationin a labor reserve economy. It is thus another example of how, in their quest for "risk behaviors," certain anthropologists have contributed to the decontextualization of African lives and to the narrowing of AIDS research. Clearly, the two explanations call for very different responses. Knowing which one is correct is therefore of considerable importance.
Needle Use: An Alternative Model
The second area of inquiry that appears to have been obscured as a result of the medical research community's fixation on African sexuality is the role of injections and transfusions in the spread of HIV. High levels of background infection are associated in Africa with high levels of needle use in a range of therapeutic settings, which may or may not observe adequate sterilization procedures. Where sterilization is not employed, there is a risk of HIV transmission. Although this area of risk has been recognized, it has been given inadequate attention.
In two control studies of infants and children in Kinshasa, Mann and his colleagues correlated HIV seropositivity with a history of frequent previous injections: "The greater number of injections previously received by seropositive children of seronegative mothers than by seropositive children of seropositive mothers (who presumably have similar HIV burdens) strengthens the argument that these injections represent an important route of exposure to HIV, rather than reflecting medical needs for HIV-associated illness."[32]
J. M. Mann et al., "Risk Factors for Human Immunodeficiency Virus Seropositivity among Children 1-24 Months Old in Kinshasa, Zaire," Lancet no. 8508 (1986): 676.
The authors noted that all children and infants in Kinshasa are commonly given intramuscular injections and that there was a high expectation among mothers that injections are an essential part of any cure. "Injections are often administered in dispensaries which reuse needles and syringes yet may not adequately sterilize injection equipment. Furthermore injections are frequently given by untrained personnel or traditional healers." The seropositive infants and children in these studies also had a history of transfusions, which are commonly given to children who suffer from anemia due to malaria.Children and infants are not the only segments of the African population who are at risk of transmission through injections and transfusions. The view that injections represent the most effective form of medical therapy is clearly widespread in Africa. And adults are just as vulnerable to this means of transmission as children. Of 500 cases studied by Quinn and his colleagues in Kinshasa, 80 percent had a history of prior injections. This was in fact the greatest risk associated with
AIDS in the study, though the authors noted that it was impossible to assess the significance of risk activities without information on control populations. Similarly, in a study of over 2,000 hospital workers, the only identifiable risk factors were hospitalization during the previous ten years, transfusion within the last ten years, and medical injection within the last three years.[33]
T. Quinn et al., "AIDS in Africa: An Epidemiological Paradigm," Science 234 (1986): 955-63.
In this context it is worth noting that STD clinic attendees, who are reported to have high rates of HIV infection, also have higher than normal histories of injections. The number of such injections may in fact be remarkably high. It has been calculated that among prostitutes in Nairobi the mean time to reinfection after treatment was only twelve days.[34]
L. J. D'Costa et al., "Prostitutes Are a Major Reservoir of Sexually Transmitted Diseases in Nairobi, Kenya," Sexually Transmitted Diseases 12 (1985): 64-67.
Prostitutes and their customers may thus be repeatedly exposed to needles.Melbye and his colleagues rejected the hypothesis that needles accounted for the high rates of HIV infection among the STD clinic attendees they studied in Lusaka, arguing that in the University Teaching Hospital's STD clinic, where they carried out their studies, "clinic needles are not commonly reused" (emphasis added).[35]
Melbye et al., "Evidence for Heterosexual Transmission," p. 1115.
In addition, they noted that the prevalence figures were as high for those STD clinic attendees who received injections as for those who did not. These arguments are not very convincing, in part because the researchers made no attempt to elicit information about treatment that these patients may have received from other clinics as well as from various indigenous healers, who may have been somewhat less careful about needle reuse. One might also imagine that clinic staff would have been more careful about sterilization in the presence of the AIDS researchers.The association of hepatitis B infection with STD attendance also points toward a connection between injections and HIV transmission. Thus, Van de Perre and his associates, in a study of prostitutes drawn from an STD clinic in Butare, Rwanda, found that twenty-nine of thirty-three prostitutes were seropositive for HIV, as compared to four of thirty-three female controls; thirty-one of the prostitutes also had hepatitis B virus markers, as compared to only eighteen of the controls; and thirty-one of the subjects and thirteen of the controls tested positive for Chlamydia trachoma . While high prevalences of hepatitis B have also been reported among homosexual populations in the United States, its transmission among heterosexual populations has been more frequently associated with unsterilized needle use. This finding suggests that the subject population in this study may have been exposed to unsterilized needles more frequently than the controls and that this exposure may have accounted
for their higher rates of HIV infection. Therefore, it is impossible to state with any certainty whether frequent sexual activity results directly in HIV transmission or only puts one at risk of exposure to other STDs and thereby at risk of being infected with HIV through exposure to unsterilized needles. The authors of the study, in fact, concluded: "This study suggests that HTLV-III has to be considered as an infectious agent transmitted among promiscuous Central African heterosexuals by sexual contact and/or parenteral contact with unsterile needles used for STD treatments " (emphasis added).[36]
P. van de Perre, "Seroepidemiological Study of Sexually Transmitted Diseases and Hepatitis B in African Promiscuous Heterosexuals in Relation to HTLV-III Infections," European Journal of Epidemiology 3, no. 1 (1987): 4-8, at p. 8.
The possible role of needle transmission among adults in STD clinic settings provides an alternative explanation for the commonly reported correlation between frequent prostitute contacts and HIV infection among African men, as well as the association between genital ulcers and HIV seropositivity. The studies that have shown a correlation between prostitute contact, genital ulcers, and HIV seropositivity in Africa have drawn their subject population from STD clinics and their control populations from among blood donors or medical staff populations.[37]
Ryder and colleagues ("Extramarital Prostitute Sex and Genital Ulcer Disease") drew their sample population from outside clinic settings. However, they did not control for the possibility of needle transmission.
As noted above, these studies have not controlled for the possibility that the chain of causation may involve contact with prostitutes, leading to STDs and genital ulcers, leading to clinic treatment and HIV infection through exposure to unclean needles. Prostitutes may be a major risk group for AIDS, but they need not be the primary vectors for HIV transmission that they are frequently made out to be. They may simply be a source for the transmission of STDs, which are a risk factor for HIV transmission through unsterile needle use or genital ulcers.[38]J. A. De Hovitz, "A Perspective on the Heterosexual Transmission of the Acquired Immunodeficiency Syndrome," New York State Journal of Medicine 86 (1986): 117-18.
Clearly, studies need to be done which control for the possibility that needles may be a primary route of transmission.If needle use is a significant means of HIV transmission, we need to examine why sterilization does not occur. Clearly, one of the reasons is that injections are performed by indigenous therapists who are unaware of the risks involved in reusing needles without sterilization. Yet lack of sterilization also occurs in government-run clinics. We should not conclude that the failure to sterilize needles is necessarily a product of laziness or ignorance on the part of African medical personnel, lest we construct another cultural stereotype to explain the spread of AIDS in Africa. Given limited medical budgets (averaging five dollars per capita) and shortages in foreign exchange in most African countries (a product of the declining value of African exports on world commodity markets and currency devaluations instigated by the International Monetary Fund), disposable needles, sterilizers, and even the chemicals needed for
sterilization are often in short supply. The energy costs involved in running sterilizers, even where they exist, may also limit the sterilization of needles.
Warfare is also contributing to the reuse of needles in many countries, such as Mozambique, Uganda, and Angola, by disrupting electrical power supplies and urban and rural health services. In Mozambique, for example, Renamo "terrorists" frequently destroy power lines to the city of Beira. Until the recent acquisition of generators by the city, these actions disrupted needle sterilization within the city hospital. The destruction of rural clinics and medical equipment also increases pressure to reuse needles.
In short, as the World Health Organization has advocated, we need to examine the political economy of health care, and not simply the incidence of improper needle use.[39]
World Health Organization, Special Programme on Africa, Strategies and Structure: Project Needs, vol. 2 (Geneva: WHO, 1987), pp. 3-4.
In a similar vein, the role of transfusions in transmitting HIV needs to be viewed within the context of a lack of financial resources to properly screen donated blood and an extremely high incidence of trauma injuries requiring blood transfusions associated with warfare and automobile accidents.Age Distribution Studies: A Critique
Data on the age distribution of both AIDS cases and seropositivity have been used to support the argument that injections do not contribute materially to the transmission of HIV in Africa. Evidence collected on the distribution of 500 AIDS cases in Kinshasa is presented in figures 6 and 7.
Commenting on this distribution, Quinn and his associates conclude, "The sex and age distribution of 500 AIDS cases reflect patterns seen in other sexually transmitted diseases both in developed and developing countries in which incidence and morbidity rates are higher among younger women."[40]
Quinn et al., "AIDS in Africa," p. 957.
On the last point, Peter Piot recently suggested at an AIDS conference in Washington that older men may be having sex with younger women.These statements imply that the age-sex distribution of AIDS cases supports the assumption that AIDS is being transmitted through heterosexual contact. Yet if one looks at the age-sex distribution of tuberculosis, one sees a similar pattern. Surely no one would argue that TB is a sexually transmitted disease. As is now recognized, women in their childbearing years have a higher risk of contracting TB because of a generalized lowered resistance.[41]
This susceptibility suggests that we need to be careful in extrapolating general levels of HIV infection from prevalence surveys using pregnant women.
Conversely, children in the age range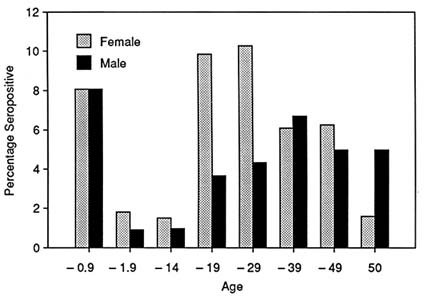
6. HIV Seropositive Rates, Kinshasa, 1984–1985
SOURCE : T. Quinn et al., "AIDS in Africa: An Epidemiological Paradigm,"
Science 234 (1984): 955–63.
from four to fourteen, for reasons that are not altogether clear, have a higher level of resistance to a number of diseases, including TB. This phenomenon may in fact occur in AIDS. Thus, several studies recently reported in the New York Times noted that children in their teens infected with HIV show fewer signs of a declining immune system than similarly infected adults. Dr. James Goedert of the National Cancer Institute followed up eighty-nine patients from a hemophilia center, all of whom were infected with HIV. After seven years 35 percent of the adults had symptoms of AIDS, whereas only 10 percent of those infected as children and teenagers had AIDS symptoms. Two other studies reported similar findings. Dr. Goedert concluded that "AIDS could resemble chicken pox, measles or other diseases that are more severe in adults than in children and adolescents."[42]
Gina Kolata, "AIDS Symptoms Found Slowed in Teen-Agers," New York Times, April 3, 1988, p. 25. Dr. Goedert reported at the International AIDS Conference in Stockholm in 1988 that children between the ages of two and eighteen had a 12 percent risk of developing AIDS eight years after infection, whereas adults eighteen to thirty-four had a 26 percent chance of doing so (G. Kolata, "Studies Link Age to AIDS Development," New York Times, May 21, 1989, p. 34).
If this is the case, then the low incidence of AIDS in the four-to-fourteen age range may reflect resistance to viral replication and AIDS rather than an absence of infection. In other words, the age distribution of AIDS cases in Africa need not support the hypothesis that AIDS is transmitted primarily through heterosexual contacts. Why, then, did Quinn and his associates choose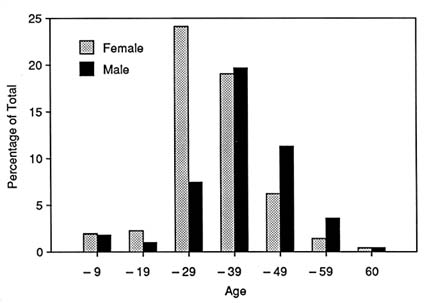
7. Distribution of 500 AIDS Cases, Kinshasa, August 1985—December 1985
SOURCE : T. Quinn et al., "AIDS in Africa: An Epidemiological Paradigm," Science 234 (1984): 955–63.
"other sexually transmitted diseases," rather than other infectious diseases, as their comparison?
The possibility that young children are resistant to HIV progression raises an additional issue. That is, in many parts of Africa, all children under five are vaccinated at the same time—often with unsterilized needles that are reused. Since this practice is widely recognized as a potential avenue for the transmission of HIV, one would expect to find more AIDS cases in young children. But few such cases have been found. This lack of cases may, as suggested above, be related to the children's resistance to disease progression rather than to an absence of infection. As a result, the cases acquired through this route would show up in the young-adult population.
Medical researchers will immediately object to this explanation on the ground that seropositivity data appear to reveal the same pattern of age and sex distribution. In other words, it is not just that fewer cases appear among children in the four-to-fourteen age range; they also appear to be infected less. This finding appears to support the heterosexual contact model and to call into question the importance of other
forms of transmission, and particularly injections. Thus, Robert Biggar in a recent review of epidemiological data on AIDS concludes: "The results of serosurveys using accurate tests have shown that HIV infection in central Africa is largely heterosexually transmitted. Evidence supporting this includes … the great concentration of HIV-infected persons in the years of greatest sexual activity (15–65 years old) with the peak age-specific prevalence being during the years of peak sexual activity (25–29 years for women; 30–34 years old for men)."[43]
R. J. Biggar, "Overview: Africa, AIDS and Epidemiology," in AIDS in Africa, ed. Rockwell and Miller, p. 3.
How reasonable is this interpretation? First of all, it must be noted that there is little reliable cross-sectional data on the age-sex distribution of HIV seropositivity or AIDS cases in Africa. In fact, until recently statements about the age distribution of seropositivity were based on a small number of prevalence studies conducted in hospital or clinic settings involving the use of what have often been questionable sampling methods. The first study to present age-specific seroprevalence data using reliable screening methods, and the one that is cited by Biggar and others, was conducted by Melbye and his associates at the University Teaching Hospital in Lusaka, Zambia, in August 1985.[44]
Melbye et al, "Evidence for Heterosexual Transmission," p. 1115.
The 1,078 subjects in the study included inpatients and outpatients, blood donors, and medical staff. The study found that high levels of HIV seropositivity occurred in women and men between twenty and sixty years of age, with none of subjects under fifteen or over seventy being seropositive. The investigators concluded: "Our findings strongly suggest that heterosexual transmission is an important route of HIV infection in Africa. Seropositivity was restricted to subjects who were in their sexually most active years of life."[45]Ibid.
Yet even a cursory examination of the data used in this study quickly reveals a significant problem in the sampling method employed. While the total sample consisted of 1,078 subjects, the "under fifteen years" subgroup included only 12 subjects, all of whom were surgery patients between ten and fifteen years of age. The "over sixty" group consisted of 47 subjects, and only 21 subjects were over seventy years of age. In effect, 97 percent of the sample fell between fifteen and seventy years of age; 94 percent, between fifteen and sixty. Similarly, if one looks just at the blood donors and hospital staff, 94 percent of the sample fell between fifteen and fifty years of age. The small sample size for the populations on either side of this age group, and particularly in the "under fifteen" age group, makes any conclusions about the distribution of seropositivity among the wider population from which this sample was drawn meaningless—especially when one realizes that more than 50
percent of the populations of most African countries are under fifteen years of age! In other words, the sample was not representative of the population from which it was drawn.
There is the additional problem created by the use of a hospital population who may have a range of risk factors, including injection and transfusion histories. Without knowing how these risk factors are distributed through the different age groups, one cannot know whether age or the frequency of particular risk factors is being reflected in the age distribution pattern.
It is unclear whether the same problems apply to later sources of prevalence data that are said to support the sexual transmission paradigm. A study of over 5,000 "healthy persons" living in Kinshasa who were tested between 1984 and 1985 revealed a similar distribution of HIV infection. The results were reported by Quinn and his associates in 1986.[46]
Quinn et al., "AIDS in Africa," p. 958.
The report, however, provided no details on how the sample was collected and made no reference to earlier reports that describe the methods involved. A more recent study, conducted in the Central African Republic and employing random sampling, reported an absence of antibodies to HIV in children four to fifteen years of age. The investigators warned, however, that more surveys were needed to confirm this finding because the sample for this age group was nonrepresentative.[47]M. Merlin et al., "Epidemiology of HIV1 Infection among Randomized Representative Central African Populations," Annales Institut Pasteur/Virologie 138 (1987): 503-10.
Even assuming that the distribution of HIV infection in the sample population in these studies accurately reflects its distribution in the underlying population, what does this finding indicate? Or, put another way, could the high prevalence of HIV among sexually active subjects and the relatively low prevalence among children reflect the presence of factors other than levels of sexual activity? For example, if the transmission of HIV is facilitated by the presence of preexisting immunosuppresant infections, and if children between the ages of four and fifteen are more resistant to such infections than either infants or adults, the four-to-fifteen age group would have a lower prevalence of HIV than other age groups regardless of how the infection is transmitted. Alternatively, their increased resistance to other infectious diseases may reduce their exposure to risk of infection through needles and/or transfusions. In short, age distribution data, even if correct, need not indicate that sex is the only avenue of HIV transmission in Africa.
These possibilities are admittedly speculative. Moreover, they run counter to the often-quoted instruction given to all medical students: "When you hear hoofbeats, think of horses, not zebras." AIDS, however, is a relatively new disease, about which there is a great deal more
to be learned. Thinking of horses, while reasonable in a diagnostic setting, may prevent medical researchers in Africa from seeing the entire range of factors at play in the epidemiology of AIDS in Africa. In any case, in Africa one can just as easily come across a zebra as a horse.
Conclusion
The point in all this is that assumptions about the importance of sexual promiscuity in the transmission of HIV in Africa were initially based on limited, and in some cases methodologically questionable, data. These assumptions, nonetheless, shaped both the questions that AIDS researchers asked and the way that they interpreted data. This narrowing of research, in turn, discouraged serious consideration of the role of alternative avenues of transmission, such as injections, or of the role of possible cofactors, such as high background levels of infection and malnutrition and associated problems of poverty and maldevelopment, which may be as important in the heterosexual transmission of HIV as the frequency of sexual contacts.
We are, in fact, much further from understanding the epidemiology of AIDS in Africa than some medical researchers, development officers, and social scientists would have us believe. It is clear that heterosexual transmission of HIV occurs in Africa, but how or why it occurs has not been demonstrated. AIDS, like Burkett's lymphoma, may yet prove to have a complex etiology involving a combination of political and economic forces associated with underdevelopment in Africa. These forces have brought together particularly susceptible populations—populations subject to high background levels of viral, parasitic, and bacterial infections—in a social setting marked by high levels of familial separation and multiple sexual partners. These conditions, in turn, have contributed to the spread of other STDs, which in turn have created a high risk of exposure to HIV via genital ulcers and/or infected needles.
The medical research community and the social science community working with it must develop research agendas that will illuminate these complex interactions, instead of obscuring them through a precipitous move to find quick answers that can be easily translated into AIDS containment programs. The early history of Western research on TB and syphilis should serve as a warning that, if we continue to look for easy solutions, those solutions may have a limited impact and, at the same time, our understanding of the wider epidemiology of AIDS may be
diminished. Before we spend millions on the type of behavior modification model of intervention now being developed, we must have a higher degree of certainty about how HIV is being transmitted and what the real risk factors are, as well as knowledge of the social and economic context within which risk behaviors are set. If primary risk factors are poverty and unemployment, our proposed interventions must address the causes of these conditions. We must not allow AIDS to become one more symptom for which the West finds a cure without addressing the underlying causes of this and many other health problems. At the very least, studies that explore other cofactors and avenues of transmission need to parallel efforts to understand and prevent the sexual transmission of HIV.
Any attempt to initiate a more comprehensive approach to AIDS research in Africa requires that medical researchers and social scientists develop a more productive working relationship. Such a relationship will necessitate adjustments on both sides. Social scientists need to resist attempts to limit their input to collecting and presenting cultural artifacts; they need to be critical of colleagues who continue to accept this limited role. If the conferences and workshops at which social scientists and medical researchers are brought together are to be productive, their agendas must be expanded to address broader issues of African social and economic life and not simply the "sexual life of the natives" and other forms of risk behaviors. At the same time, any attempt to open up the agenda must be sensitive to the medical research community's need for questions and hypotheses that take account of the existing epidemiological data and that can be empirically tested.
For their part, medical researchers need to take a more open view of how the social science community can contribute to epidemiological research on AIDS in Africa. They need to recognize that AIDS research in Africa can be illuminated by a more fundamental knowledge and understanding of the contours of African social and economic life, which involves more than a cataloging of risk behaviors. Medical researchers, like social scientists, also need to be more openly critical of their own colleagues. Research based on unrepresentative samples or faulty sampling methods need to be challenged. Peer review procedures need to be uniform, so that conclusions presented on AIDS in Lusaka are viewed as critically as conclusions made about AIDS in New York City. The medical community also needs to be more forthright and open about the limits of our present knowledge about the epidemiology of AIDS in Africa. Too many studies have taken an authoritatitve tone that is not
warranted by the data available and, in doing so, have encouraged premature closure of African AIDS research.
AIDS and HIV Infection in the Third World:
A First World Chronicle
Paula A. Treichler
Understanding the AIDS epidemic as a medical phenomenon involves understanding it as a cultural phenomenon. Yet excessively positivist or commonsensical notions of "culture" may limit our ability to recognize that AIDS is also a complex and contradictory construction of culture. This is particularly true of AIDS in developing countries. AIDS in the developed world (the "First World" and, to a lesser extent, the "Second World") is now routinely characterized as a social as well as a medical epidemic, as a challenge to conflicting values, and as an unprecedentedly complex cultural phenomenon; in contrast, AIDS in the developing world—the "Third World"—is believed to lead a much simpler life.[1]
For an excellent discussion of the vexing terms First World, Third World, and Second World, see Carl E. Pletsch, "The Three Worlds, or the Division of Social Scientific Labor, circa 1950 to 1975," Comparative Studies in Society and History 23, no. 4 (1981): 565-90. Pletsch argues that the notion of the Third World is bogus; indeed, he writes that, except for the political categories of left and right, "the scheme of three worlds is perhaps the most primitive system of classification in our social scientific discourse" (p. 566). I agree with Pletsch that as a framework for investigation this classification system yields studies in which non-Western civilizations—that is, the Second and Third Worlds—are "almost pure fantasies" (p. 566). Because it is these "fantasies" I am attempting to chronicle, I deliberately use the First World/Third World terminology in this essay, along with such alternative signifiers as colonial, postcolonial, industrialized, developing, and poor. See also my "AIDS, Homophobia, and Biomedical Discourse: An Epidemic of Signification," in AIDS: Cultural Analysis/Cultural Activism, ed. Douglas Crimp (Cambridge, Mass.: MIT Press, 1988), pp. 31-70.
Even when these cultures themselves are seen as mysterious, AIDS is seen as a scientifically understood infectious disease that, without our help, will devastate whole countries, whose passive citizens struggle against it in vain.This vision is well intentioned and perhaps even necessary to marshal external resources. But it obscures the fact that diverse interests are articulated around AIDS in the developing world in ways that are socially and culturally localized and specific. Deeply entrenched institutional agendas and cultural precedents in the First World prevent us from hearing the story of AIDS in the Third World as a complex narrative. One consequence of this inadvertent cultural imperialism is that very simple generalizations about the epidemic may be accepted as "the truth about AIDS," with few efforts made to unravel their diverse and often contradictory claims.
A different version of this essay was published in Remaking History , ed. Phil Mariani and Barbara Kruger (New York: Dia Art Foundation, 1989), pp. 31–86, and is reprinted with permission. Research for this project has been supported in part by grants from the National Council of Teachers of English and the University of Illinois at Urbana-Champaign Graduate College Research Board and by a fellowship at the Society for the Humanities, Cornell University. For comments, suggestions, and resources, I would like to thank K. Anthony Appiah, Awour Ayodo, Stacie Colwell, Paul Farmer, Elizabeth Fee, Daniel M. Fox, Gertrude Fraser, Colin Garrett, Ibulaimu Kakoma, Cary Nelson, Elisabeth Santos, and Simon Watney, as well as University of Illinois librarians John Littlewood (Documents) and Yvette Scheven (Africana).
The term AIDS in this essay refers to the AIDS epidemic as a broad social and cultural crisis; the terms HIV disease and AIDS and HIV infection are used interchangeably to mean the broad clinical spectrum of HIV-related conditions from symptomatic infection to the specific diseases presently used to define "AIDS" (I use AIDS to mean the inclusive medical spectrum only if this sense is clear in context).
This essay does not seek to determine "the truth about AIDS." Rather, I look closely at how selected First and Third World publications attempt to chronicle and conceptualize the epidemic. I begin with a discussion of AIDS in Haiti, to show a typical discursive construction of "Third World AIDS." I then contrast the familiar statistical chronicle of the global epidemic with other accounts, suggesting how differing conceptualizations, different "truths," work to promote differing material consequences. Contradictory accounts of the epidemic in Kenya, for example, suggest the value of listening carefully to contradictions; selecting too readily a given account as the definitive truth short-circuits efforts to better understand how truth is situated—and how it is produced, legitimated, sustained, and interpreted. I conclude that understanding the discursive production of the AIDS crisis—the production, that is, of these differing narratives—is a necessary if not sufficient part of addressing its conceptual and material complexity. In turn, such understanding provides crucial grounding for genuine cooperation between the developed and the developing worlds.
A U.S. Doctor Unmasks Truth In Haiti: Third World Aids In First World Media
We had come near the end of a long line of anthropologists working in these remote villages. … Coming at the end gave us certain advantages. … But as time passed we became aware that we had also inherited serious problems. The !Kung had been observing anthropologists for almost six years and had learned quite a bit about them. Precedents had been set that the !Kung expected us to follow.
Shostak, Nisa[2]Marjorie Shostak, Nisa: The Life and Words of a !Kung Woman (New York: Vintage, 1983), p. 26.
The very activity of ethnographic writing —seen as inscription or textualization—enacts a redemptive Western allegory.
Clifford, "Allegory"[3]James Clifford, "On Ethnographic Allegory," in Writing Culture, ed. James Clifford and George E. Marcus (Berkeley: University of California Press, 1986), p. 99.
All accounts of the AIDS epidemic in the Third World, whether they are medical reports, patient testimony, media observations, investigative journalism, World Health Organization news bulletins, or government reports, are at some level linguistic constructions. These diverse
representations of AIDS in the Third World draw their authority from many sources, including the credentials and persuasive powers of individual authors, consistency with accepted beliefs and knowledge about AIDS and about the Third World, compatibility with our own social and political perspectives, and resonance with familiar traditions of discourse. Though often covert, the influence of discourse is powerful and pervasive in establishing and legitimating a given representation.
Discourse about AIDS, for example, draws on widely accepted narratives of past epidemics. Though these histories may be employed to supply a variety of arguments and moral conclusions about today's epidemic, they share the premise that any infectious disease is a knowable biological phenomenon whose strange and seemingly contradictory aspects are ultimately illusory: decoded by experts, its mysteries will one by one become controllable material realities. Discourse about AIDS in the Third World shares but exaggerates this premise, first equating the Third World (especially Africa, "the dark continent") with the savage, the alien, or the incomprehensible, then asserting the importance and achievability of reason and control. Though these two features may initially seem to be in conflict, they exist in fact in a relationship of discursive symbiosis: the metaphors of mystery and otherness produce the desire for control, which is in turn fulfilled and justified by the metaphors of otherness and mystery.[4]
See Homi Bhabha, "The Other Question—the Stereotype and Colonial Discourse," Screen 24, no. 6 (November-December 1983): 18-36; and Chandra Talpade Mohanty, "Under Western Eyes: Feminist Scholarship and Colonial Discourses," Boundary 2 12, no. 3 and 13, no. 1 (Spring and Fall 1984): 333-58.
A highly visible story, for example, was written for Life magazine by the physician-author Richard Selzer, who visited Haiti in the mid-1980s in an effort to learn the truth about AIDS behind the government's apparent attempts to downplay its prevalence.[5]
Richard Selzer, "A Mask on the Face of Death: As AIDS Ravages Haiti, a U.S. Doctor Finds a Taboo against Truth," Life 10 (August 1987): 58-64. Hereafter documented internally by page number.
The metaphor of the article's title, "A Mask on the Face of Death," invokes the government's denials in the language of exotic tropical rituals such as carnival and voodoo. The subtitle is "As AIDS Ravages Haiti, a U.S. Doctor Finds a Taboo against Truth"; although these probably are not Selzer's words, they suggest to the reader not only that official denials mask the brutality of the epidemic but also that Selzer, the expert medical observer, can perceive the reality beneath the mask. Selzer's article is in the tradition of the privileged First World informant of conventional anthropological, ethnographic, and travel literature—the stranger in a strange land, whose representation of AIDS in the Third World is legitimated by its claim to be an objective, scientific account of phenomena observed or experienced firsthand. As Mary Louise Pratt has observed, travel writing has provided ethnographic description with a discursive legacy, despite the ethnographer's desire to repudiate it; both, in turn,permeate representations in other genres.[6]
Mary Louise Pratt, "Fieldwork in Common Places," in Writing Culture, ed. Clifford and Marcuse, pp. 27-50; see pp. 35-45 for discussion of arrival scenes. The Clifford and Marcus collection offers an extended reflection on relationships between anthropology, ethnography, and travel writing.
Thus, Selzer's article opens with the conventional arrival scene of this dual legacy: "It is 10 o'clock at night as we drive up to the Copacabana, a dilapidated brothel on the rue Dessalines in the red-light district of Port-au-Prince" (p. 59). Outside the bar Selzer is importuned by men and women offering a variety of sexual pleasures; inside, he interviews three female prostitutes from the Dominican Republic who describe AIDS as an economic problem for them, not a health problem. The direct interrogation of the native informant is another staple of privileged observer accounts; in AIDS narratives it is often prostitutes who are interviewed, and they always seem to be wearing red.[7]Photograph of "Mercedes" by J. B. Diederich for Life 10 (August 1987): 60; story on Mombasa by Tom Masland, "AIDS Threat Turns Shore Leave into Naval Exercise in Caution," Chicago Tribune, March 17, 1988, sec. 1, p. 13; Newsweek photo of prostitute, p. 46 in Rod Nordland, with Ray Wilkinson and Ruth Marshall, "Africa in the Plague Years," Newsweek, November 24, 1986, pp. 44-47.
The following day, Selzer talks with physicians and examines a large number of patients with apparent HIV-related illnesses for whom little in the way of treatment is available.Selzer is carefully nonjudgmental with respect to street life and indeed speculates that the virus may have entered Haiti as an accidental feature of First World exploitation: "Could it have come from the American and Canadian homosexual tourists, and, yes, even some U.S. diplomats who have traveled to the island to have sex with impoverished Haitian men all too willing to sell themselves to feed their families? Throughout the international gay community Haiti was known as a good place to go for sex" (p. 64). Selzer pursues this characterization of Haiti as sexual victim ravaged by Western capitalists. Acting on "a private tip from an official at the Ministry of Tourism," Selzer and guide drive to a once luxurious hotel fifty miles from Port-au-Prince that was a prime vacation spot for gay men. Because the two Frenchmen who own the hotel are out of the country, Selzer and his guide are shown around by a staff member, a man about thirty who clearly
is desperately ill. Tottering, short of breath, he shows us about the empty hotel. The furnishings are opulent and extreme—tiger skins on the wall, a live leopard in the garden, a bedroom containing a giant bathtub with gold faucets. Is it the heat of the day or the heat of my imagination that makes these walls echo with the painful cries of pederasty? (p. 64)
Ill at ease among the tiger skins of a hotel in Haiti, the Western travel writer goes to work on "Third World AIDS." Ultimately, for Selzer, AIDS in Haiti is an unambiguous mor(t)ality tale about the evils of sexual excess: as northern homosexual men ravaged Haitian boys, so does AIDS ravage Haiti. Nostalgia for the observed culture's original innocence gives way to regret at its exploitation by decadent foreigners and speculation about the deadly effects of exotic customs and sexual
practices. Selzer's account therefore tells us something about his concrete daily activities, his heated imagination, and his strategies for transforming selected experiences into prose, but his desire to bring the country's plight to world attention is as much about language as about AIDS in Haiti.
The status of Selzer's article as a firsthand report of observed phenomena does not rest on our firsthand knowledge about AIDS, the Third World, or Haiti. In certain concrete ways, just as cinematic convention represents scenes viewed through binoculars as two intersecting circles, Western AIDS discourse transforms a culture so that it ceases to recognize itself but paradoxically becomes recognizable in the West. What is needed is to sort out the multiple voices, texts, and subtexts of the AIDS epidemic—which has in part evolved, as Jan Zita Grover puts it, as a "creature of language."[8]
Jan Zita Grover, "A Matter of Life and Death," Women's Review of Books 5, no. 6 (March 1988): 3. See also Simon Watney, "Missionary Positions: AIDS, 'Africa,' and Race," Differences: A Journal of Feminist Cultural Studies 1, no. 1 (1989): 83-100.
Several elements of Selzer's account of AIDS in Haiti are now virtually obligatory in First World chronicles of Third World AIDS. First, the opening arrival scene, as I have noted, situates the First World observer in relation to the Third World culture—a culture that, in AIDS chronicles, almost always belongs to the fallen world of postcolonial development. Indeed, the term Third World grew out of the perceived confrontation between capitalist and communist interests and hence presupposes an analysis dependent on such concepts as colonialism, industrialization, modernity, and development. Second, the statistics provided by Haitian physicians function in at least two ways: to anchor in objective fact Selzer's more personal observations about the prevalence of AIDS, and to demonstrate the specialized knowledge of expert native informants whose on-the-scene experience equips them to reveal the truth behind the official mask. (In Selzer's story the inside informants assert that AIDS is more widespread than officials admit; but in other AIDS stories insiders also function to accuse the government and the media of exaggerating the AIDS crisis for political gains.) Another element is provided by "the reigning American pastor," a nonnative informant whose unreliability as a cultural informant is demonstrated by his moralistic condemnation of voodoo—a system of practices believed by some to facilitate the spread of HIV. Voodoo, he tells Selzer, is "a demonic religion, a cancer on Haiti" that is "worse than AIDS" (p. 62). In positioning himself against his fellow American, "a tall, handsome Midwesterner with an ecclesiastical smile," Selzer secures his own reliability, much as ethnographers quote descriptions of a given culture by earlier travel writers to repudiate the bias of such unscientific observations.
Selzer's visits to health care settings constitute another element, revealing a devastated health care system—part of the economic fallen world that parallels his image elsewhere of Haiti as the victim of First World sexual exploitation. A further familiar feature of AIDS stories is "the view from the street," represented by Selzer's talk with the three healthy Dominican prostitutes. Their remarks seem designed to underscore the ignorance and dangerous false security engendered by the government's official silence. One of them, Carmen, scoffs at Selzer's suggestion that prostitutes as a population are sick with AIDS:
"AIDS!" Her lips curl about the syllable. "There is no such thing. It is a false disease invented by the American government to take advantage of the poor countries. The American President hates poor people, so now he makes up AIDS to take away the little we have." The others nod vehemently. (p. 60)
The notion that AIDS is an American invention is, like so-called conspiracy theories, a recurrent element of the international AIDS story. It is one not easily incorporated within a Western positivist frame—in part, perhaps, because it often reveals an underlying narrative about colonialism in a postcolonial world. The West accordingly attributes such theories to ignorance, state propaganda, or psychological denial; or it interprets them as some new global version of an urban legend, like alligators in the New York City sewer system.[9]
Conspiracy theories of AIDS are reviewed by Robert Lederer, "Origin and Spread of AIDS," CovertAction, no. 29 (1988): 52-67, and are reported regularly in the New York Native, a gay New York City weekly periodical. The function of conspiracy theories in postcolonial settings is discussed by Paul Farmer, "Sending Sickness: Sorcery, Politics, and Changing Concepts of AIDS in Rural Haiti," Medical Anthropology Quarterly 4, no. 1 (1990): 6-27; and Alma Gottleib, "Hot Blood, Vengeful Blood: AIDS and Blood Symbolism in Africa," paper presented at the conference on the Impact of AIDS on Maternal-Child Health Care Delivery in Africa, University of Illinois at Urbana, May 5, 1990.
But Carmen's theory of AIDS invokes two further narratives that reinforce the notion of a global economy changing in ways the West cannot fully control. One is a tale of postmodern scholarship about the difficulty of finding good native informants these days. As Shostak's introduction to her ethnographic study Nisa makes clear, native informants are quite likely to be already wise in the ways of Western inquisitors. Discussing Nisa , Pratt convincingly argues that Shostak is nevertheless able ultimately to transcend the "degraded" ethnographic culture of too-knowing informants and achieve a redemptive resolution for her story. Selzer's framing of Carmen accomplishes something similar, together with a second narrative, to which I have already alluded, concerning the construction of the subject in a fallen world. Pratt suggests that ethnographic characterizations of the !Kung changed in the course of foreign colonization. Precolonial ethnographers rendered them as sly, bloodthirsty, untrustworthy, appetitive, manipulative; after colonization they came to be represented as helpful, friendly, innocent, good, and vulnerable. Carmen's speech takes place at a pivotal moment in the global AIDS drama, and this context encourages us to hear her emphatic
denial of AIDS as a prelude to tragedy—perhaps as we would hear Violetta in the first act of La Traviata .[10]
A parallel shift in the course of the AIDS epidemic in the United States is clearly evident in representations of gay men, as illness and death transform a threatening and alien community into a vulnerable one. Pratt (in "Fieldwork in Common Places," pp. 44-50) discusses redemptive endings. Working against them is the ethnographic paradox that the Other becomes worldly-wise through contact with "modern civilization"—often in the guise of ethnographers themselves. In Selzer's encounter, the fact that he pays the prostitutes to talk to him parallels the further irony of ethnographic research in which the privileged investigator enters into a commodity exchange with the native informant—anexchange which, as Pratt puts it, turns the "anthropologist preserver-of-the-culture" into an "interventionist corrupter-of-the-culture."
Selzer finally sums up: "This evening I leave Haiti. For two weeks I have fastened myself to this lovely fragile land like an ear pressed to the ground. It is a country to break a traveler's heart. … Perhaps one day the plague will be rendered in poetry, music, painting. But not now, not now" (p. 64). Here the stance of physician as ethnographer is clearer, the physician's ear pressed to the body of Haiti as he might press it to the body of a patient. But though the diagnosis is grim, the language is utopian: the First World AIDS narrative successfully repels the various threats of postmodern disruption to deliver a message of transcendent, universal humanism.
What are we to make of this? I am not suggesting that Selzer's account is not "true," or that we should exonerate the government of Haiti on its AIDS policies. I wish rather to point out how narrative conventions establish and sustain our sense of what is true. Visual representations reinforce the illusion of truth, in part because they reproduce familiar representations of the Third World and reinforce what we think we already know about AIDS in those regions. Thus, the color photographs in Selzer's Life story show us frail, wasting bodies in gloomy clinics; small children in rickety cribs; the prostitutes in red. One of the Dominican prostitutes, for example, is glamorously photographed, the full skirt of her red dress fanned out across a bed. Similarly, an April 1988 news account of the fear of AIDS in Mombasa, Kenya, reports an exchange between a U.S. sailor and a prostitute, a "23-year-old Ugandan woman in red shorts"; and a Newsweek photograph of a woman in red leggings and a skirt is captioned: "'Avoid promiscuity': Prostitute with men in Zaire." Photographs in a 1986 Newsweek story on AIDS in Africa depict the "Third Worldness" of its health care system: in Tanzania a man with AIDS lies hospitalized on a plain cot with none of the high-tech paraphernalia of U.S. representations; a widely reprinted photograph shows six "emaciated patients in a Uganda AIDS ward," two in cots, four on mats on the the floor; rarely are physicians shown. A story on Brazil carries similar low-tech images. In contrast, publications originating in these countries do not omit technical images: African publications often show African scientists and physicians, and among the photographs in a 1987 story on AIDS in Veja, the Brazilian equivalent of Newsweek, are an enormous fully equipped modern hospital and masked and gowned physicians and nurses.[11]
See photographs in Nordland et al., "Africa in the Plague Years," and Kenneth M. Pierce, "Nowhere to Run, Nowhere to Hide," Time, September 1, 1986, p. 36. Images of AIDS in Brazilian magazines like Veja, first brought to my attention by Elisabeth Santos, are further analyzed in Haydée Seijo-Maldonado and Christine A. Horak, "AIDS in Latin American Newsmagazines: A Contest for Meaning," unpublished manuscript, 1991. Odd linkages among photographs, captions, and text do not only occur in Third World contexts, of course. A story on AIDS in the Canadian journal Macleans, for example, includes a photograph of pedestrians on a crowded Toronto city street; shot from behind so that the pedestrians are moving away from the camera, the photo appears to illustrate the caption: "Toronto sidewalk traffic: Growing fear on AIDS virus spreads to general public" (Macleans, August 24, 1987, p. 31).
A different problem occurs in a 1988 National Geographic story called "Uganda: Land beyond Sorrow." The story's portrait of unrelieved despair is oddly challenged by the magazine's characteristically stunning photographs. A young woman with AIDS in a long, flowing dress, for example, stands supported by her mother, who is wearing vivid pink; the caption tells us that the woman, Jane Namirimu, is pregnant and already too weak to stand alone. Yet the beauty of the composition, even the adjacent photograph of her grave taken when the photographer returned three months later, transforms the text's bleak assertions into an almost utopian narrative of elegiac fatefulness in which aesthetic universality redeems individual suffering.[12]
Robert Caputo, "Uganda: Land beyond Sorrow," National Geographic 173, no. 4 (April 1988): 468-74; the Caputo photo of Jane Namirimu and her mother is on p. 470. Pratt (in "Fieldwork in Common Places," p. 40 and p. 45) discusses respectively the fallen postcolonial world of ethnographic writing and the trope of utopian universality.
A final problem is the literal appropriation of images. J. B. Diederich's photographs for the Selzer story were at least original for Life; but some AIDS photographs are familiar not simply because they invoke a familiar tradition but because precisely the same images circulate among diverse publications. In one of Diederich's photographs, a large, striking study in brown and white, an emaciated Haitian woman in a white dress sits gracefully on a wooden bench and looks out at the camera. The caption reads, "Tuberculosis is but one of the wasting infections of what Haitians call maladi-a ." Selzer's article does not define maladi-a or tell us whether tuberculosis is counted in Haiti as a disease that signals AIDS or is, like AIDS, simply one of many wasting diseases; nor is it clear that the woman in the photograph has actually been diagnosed with AIDS. But reproduced months later in the Canadian newsmagazine Macleans, the identical photo, no longer ambiguous, is captioned "Haitian AIDS victim: a former playground for holidayers."[13]
Selzer, "Mask on the Face of Death," p. 63. The Diederich photograph is reprinted in Macleans, August 31, 1987, p. 37. To take another example, the Newsweek photographs accompanying Nordland, "Africa in the Plague Years," have been widely reprinted. One (p. 44) shows an emaciated woman framed in the doorway of her home, holding a small thin baby in her lap. The Newsweek print is captioned "Two victims: Uganda barmaid and son," and is credited to Ed Hooper—Picture Search. Appearing on the cover of the May 24, 1988, issue of the Washington Post's weekly journal Health (vol. 4, no. 21) is a photograph of the identical woman shot at a slightly different angle; accompanying Philip J. Hilts's featured story "Out of Africa" (pp. 12-17), the photograph is now captioned as follows: "In the Ugandan village of Kinyiga, Florence Masaka, 22, and her 2-month-old daughter have both tested positive for the AIDS virus." The byline accompanying the story incorrectly credits the photos to "Al Hooper." Hilts's article and the photographs were reprinted in Africa Report, November-December 1988, pp. 26-31, to accompany "Dispelling Myths about AIDS in Africa"; the photos were captioned only with text from the story. The Hooper photographs also accompanied Catharine Watson's "Africa's AIDS Time Bomb: Region Scrambles to Fight Epidemic," The Guardian, June 17, 1987, pp. 10-11; and the Weekly Review (Nairobi), June 24, 1988, p. 18, reprinted the mother and child photograph with the caption "Ugandan AIDS victims" and no picture credit. Most recently it appears in Hooper's book Slim: A Reporter's Own Story of AIDS in East Africa (London: The Bodley Head, 1990), where the caption reads: "Florence and Ssengabi, sitting outside their hut in Gwanda. Florence died one month after this picture was taken; her baby, Ssengabi, died four months later." (Picture follows p. 170.)
Hence, our understanding of the situation in Haiti is based on a series of filtering devices, a layering of representational elements, narrative voices, and replicating images. These mediating processes are not, of course, a simple function of high-tech Western representation. Firsthand experience is not unmediated either, so one cannot get off a plane in Port-au-Prince or Nairobi, look around, and determine who is correct. Within these countries there are also differing constructions: there are people who agree with the Western media's account that AIDS is devastating the whole region; there are people like Carmen, who believe the disease is largely imaginary, the latest Western trick to reduce the Third World's population in the wake of failed birth control strategies in the past; there are others, including scientific investigators, who believe the disease exists but is a "white man's disease"; and there are still others who point to serious flaws in most existing data about the prevalence,
incidence, epidemiology, chronology, and social history of AIDS and HIV infection in the Third World.[14]
Sabatier quotes a Nigerian prostitute named Juliet as follows: "Although white clients generally pay better than their African counterparts, I will never go to bed with a white man unless he wears a condom. As far as I am concerned, AIDS is a white man's disease" (René Sabatier, Blaming Others: Prejudice, Race, and Worldwide AIDS [Washington, D.C.: Panos Institute; Philadelphia: New Society Publishers, 1988], p. 96). Similarly, a letter to the editor of the Weekly Review in Nairobi even inverted the Western argument for gender-neutral transmission to argue that AIDS in Africa could not really be affecting men and women equally because why should a disease that is homosexual in one country be heterosexual in another?
Discrepancies between doomsday predictions by the Western media and official denials by Third World governments introduce another complicating factor: every state has a "social imaginary," something it dreams itself to be, and its explicit declarations and official statistics are likely to be pervaded by this implicit social dream.[15]
Ann S. Anagnost, "Magical Practice, Birth Policy, and Women's Health in PostMao China," paper presented at the Unit for Criticism and Interpretive Theory Colloquium, University of Illinois at Urbana, December 7, 1988.
The dream of controlling the AIDS epidemic—whether controlling the blood supply, statistical and epidemiological knowledge, media coverage, biotechnology, or moral and sexual behavior—may well declare itself in a Western tongue. The photograph of the Brazilian hospital may accurately document the existence in Brazil of sophisticated medical capabilities. But as a representation of "the AIDS epidemic," it may be as bogus as the "Haitian AIDS victim." Symbiosis is self-perpetuating: while Third World representations function as elegiac icons that can be seamlessly decontextualized and appropriated by the First World narrative voice, the Third World media, dependent in varying degrees on First World sources and technology, recontextualize these images as their own. As Edward Said argues, modern representation in the decolonized world depends increasingly on a concentration of media power in metropolitan centers; this contributes to the monolithic nature of Third World representations, which are in turn a major source of information about Third World populations not only for the "outside world" but also for those populations themselves.[16]Edward Said, "In the Shadow of the West," Wedge 7-8 (Winter-Spring 1985): 4-11, at p. 5.
There is, however, another way of confronting the epidemic. If we relinquish the compulsion to separate true representations of AIDS from false ones and concentrate instead on representation and discursive production, we can begin to sort out how particular versions of truth are produced and sustained, and what cultural work they do in given contexts. Such an approach illuminates the construction of AIDS as a complex narrative and raises questions not so much about truth as about power and representation. Richard Selzer's essay on AIDS in Haiti provides useful information—not necessarily about the true nature of AIDS in the Third World but about the power of individual authors and Western mass print media to produce and transmit particular representations of AIDS according to certain conventions and, in doing so, to sustain their acceptance as true.[17]
Jean William Pape, a leading AIDS researcher in Haiti and one of the physicians Selzer consulted, expresses disenchantment with the Western press for consistently ignoring "the efforts of the Haitian people to fight, with almost no resources, the most devastating disease of this century." He told the Panos Institute: "I have given over 60 interviews to American and other reporters about AIDS in Haiti. It is very time-consuming and exhausting, and takes energy I would like to put into my work. Of all those interviews there are only one or two that recorded what I said, and the context in which I said it, accurately. The others often painted a picture of AIDS in Haiti that was unrecognizable to me" (quoted in Sabatier, Blaming Others, p. 90). (Selzer also consulted Pape, but I have no evidence that Pape found his report objectionable.) But negative reactions to Western media reports do not necessarily disrupt the cycle of representation. Some African governments, for example, angry at what they believed to be inflations of their statistics or simply wishing to deflect focus on the AIDS problem, prohibited AIDS researchers and physicians from giving interviews to the Western press. "One result of such attempts at control," said James Brooke, West Africa correspondent for the New York Times, in an interview with the Panos Institute in November 1987, "has been to force foreign reports to rely more heavily on foreign researchers working in those countries, making it more difficult than before to convey an authentically African point of view" (quoted in Sabatier, Blaming Others, p. 95). See also James Kinsella, Covering the Plague: AIDS and the American Media (New Brunswick, N.J.: Rutgers University Press, 1989). A series in the New York Times entitled "A Continent's Agony" ran from September 16 to 19, 1990 (see note 30 for a listing of lead articles). I discuss this series in "AIDS, Africa, and Cultural Theory," in Transition 51 (1991): 86-103.
This is what Michel Foucault refers to as a regime of truth.[18]"Regime of truth" is Michael Foucault's term. See "The Political Function of the Intellectual," Radical Philosophy, no. 17 (1977): 13-14. See also Treichler, "AIDS, Homophobia, and Biomedical Discourse."
Other forms of representation, drawing on different conventions, different rules, may make claims to truth in different ways.The Country And The City: Dreams Of Third World AIDS
It is not impossible that in the future, as in the past, effective steps in the prevention of disease will be motivated by an emotional revolt against some of the inadequacies of the modern world. … Knowledge and power may arise from dreams as well as from facts and logic.
Dubos, Mirage of Health[ 19]René Dubos, Mirage of Health: Utopias, Progress, and Biological Change (New Brunswick, N.J.: Rutgers University Press, 1987), pp. 218, 219. Originally published 1959.
A regime of truth is that circular relation which truth has to the systems of power that produce and sustain it, and to the effects of power which it induces and which redirect it.
Tagg, Burden of Representation[ 20]John Tagg, using Foucault to analyze the function of photographs in representing "the true," in The Burden of Representation (Amherst: University of Massachusetts Press, 1988), p. 94.
You'd be surprised: They're all individual countries.
Ronald Reagan[21]Ronald Reagan, press conference after returning from a Latin American trip, December 15, 1987.
"The statistical mode of analysis," argued Raymond Williams in The Country and the City, was "devised in response to the impossibility of understanding contemporary society from experience." Characterizing preindustrial English society as knowable through experience (if only partially so), Williams contrasted this "knowable community" with the "new sense of the darkly unknowable" produced by urbanization and industrialization. The metaphor of darkness was routinely invoked in discussions of the rise of cities: the East End, for instance, was called "Darkest London." Statistical analysis was one of the new forms of knowledge "devised to penetrate what was rightly perceived to be to a large extent obscure."[22]
Raymond Williams, Keywords: A Vocabulary of Culture and Society, rev. ed. (New York: Oxford University Press, 1985); in discussing the word experience in Keywords, pp. 126-29, Williams refers to his earlier analysis in The Country and the City of experience and statistical analysis as different ways of producing knowledge (London: Chatto and Windus, 1973), especially pp. 215-32.
Given this historical mission, it is not surprising that statistical analysis is widely seen as a powerful way to understand the latest incarnation of the "darkly unknowable": AIDS in the Third World. Statistical data, at the least, are seen as the necessary foundation for other knowledge. The ability to produce statistical information is used to measure a nation's degree of development, predict its ability to cope with the AIDS crisis, and in some cases determine its eligibility for external aid.[23]
See, for example, the testimony of Bradshaw Langmaid, Bureau of Science and Technology, USAID, on funding criteria for AIDS aid to African countries, in AIDS and the Third World: The Impact on Development, Hearing before the Select Committee on Hunger, U.S. House of Representatives, 100th Cong., 2d sess., June 30, 1988, Serial No. 100-29 (Washington, D.C.: U.S. Government Printing Office, 1988), pp. 33-34.
Even if a country cannot produce its own statistics internally, it can demonstrate its ability to cope by cooperating with external studies.[24]Most studies depend on some degree of cooperation between the First and the Third World and are thus influenced by the scientific and political commitments of given agencies and their ability to find common grounds of inquiry as well as resources. Scarce resources have created wide variation in scientific research in Africa; yet much more research goes on than stereotypes about Africa would suggest. Needless to say, views on cooperation with Western scientists are also highly variable, reflecting in some respects the ideological commitments of the state as a whole. See Sabatier, Blaming Others, pp. 108-9, on the distinction between the many long-term collaborative projects that predate AIDS and what African commentators call "parachute research" or "tourist research," in which foreign researchers drop in "to collect blood samples, data or clinical observations, and just quickly [take] off again, to write up their findings for a (Western) scientific journal."
But more obviously, the international discourse on AIDS and HIV infection in theThird World is shaped on a day-to-day basis by statistical findings and projections. Once numbers are generated and publicized, they take on a life of their own. Because they may generate calls for action (and therefore time, money, and organization), AIDS estimates may be initially resisted. But though specific numbers may be questioned and even denounced in given instances, the use of numbers as a fundamental measure of the reality of AIDS is not.
Data with regard to AIDS/HIV in Third World countries are regularly generated by several sources, including the U.S. Public Health Service Centers for Disease Control (CDC) and the World Health Organization's (WHO) Global AIDS Program (GPA); the GPA's AIDS Surveillance Unit is widely regarded as a legitimate producer, synthesizer, and interpreter of international numbers. By January 31, 1989, the number of countries reporting to the GPA was 177, of which 144 had reported one or more cases of AIDS (up from 175 and 138 in three months): a total of 139,886 cases worldwide had been reported to WHO, though WHO considers a more realistic total to be 250,000 to 500,000; WHO estimates that 5 million are infected worldwide, with a million or more infected in Africa alone. These totals mean that at least one new case of AIDS is being reported somewhere in the world every minute, or 60 new cases every hour and 1,440 each day. Projections about the worldwide distribution and future prospects of AIDS and HIV infection led Jonathan Mann, then director of the GPA, to conclude that "the global situation will get much worse before it can be brought under control."[25]
Jonathan M. Mann et al., "The International Epidemiology of AIDS," Scientific American, October 1988, pp. 82-89, at p. 82. See also Peter Piot et al., "AIDS: An International Perspective," Science 239 (1988): 573-79. Monthly statistical updates are available from the Pan-American Health Organization in Washington, D.C., WHO's regional health office for the Americas. Though the worldwide estimate of HIV infection is often given in the press as five to ten million, official estimates are somewhat lower: six to eight million was the estimate given at the Sixth International Conference on AIDS in San Francisco by Dr. Michael Merson, Mann's replacement as head of WHO's Global AIDS Program (Roland De Wolk, "Parley Opens with a Bleak Prognosis," Oakland Tribune, June 21, 1990, pp. A1, A4).
WHO did not officially acknowledge AIDS as a global health problem until late 1986—some five years into the epidemic for some countries. By the end of 1987, however, WHO's surveillance reports and seroprevalence data were sufficient to suggest three broad global patterns of AIDS:[26]
Mann et al., "International Epidemiology of AIDS," p. 84; Piot et al., "AIDS: An International Perspective," p. 576.
Pattern I, typical of industrialized countries with large numbers of reported cases (the "First World," roughly, including the United States, Canada, Western Europe, Australia, and New Zealand), is characterized by the initial appearance of HIV infection in the late 1970s; rapid spread primarily among gay men, bisexual men, and IV drug users in urban coastal centers; and recipients of blood products. HIV infection and illness are at present slowly increasing in the heterosexual population but at highly variable rates, with perinatal transmission (from mother to infant) likewise increasing but not uniformly widespread; infection in the overall population is estimated to be less than 1 percent. In Pattern II countries (typically in sub-Saharan centralAfrica, the Caribbean, and Latin America), HIV infection may have appeared in the late 1970s but was not widely identified as AIDS-related until 1983; heterosexual transmission is the norm, with males and females often equally infected and perinatal transmission therefore common; transmission via gay sexual contact or IV drug use is believed to be low or absent. A Pattern III profile is attributed to the Second World countries of the Soviet bloc as well as to much of North Africa, the Middle East, Asia, and the Pacific (excluding Australia and New Zealand): HIV is judged to have appeared in the early to mid-1980s, and only a small numbers of cases have been identified, primarily in people who have traveled to and engaged in some form of high-risk involvement with infected persons in Pattern I or II areas.[27]
Mann et al., "International Epidemiology of AIDS," p. 84. The Soviet Union did not report its first official "indigenous" death from AIDS until September 1988—a pregnant Leningrad prostitute named Olga Gaeevskaya; "Epidemiologists were incensed that the woman's doctors failed to diagnose AIDS before she died" (Edmonton Journal, October 11, 1988, p. A2). Another "outbreak" of HIV infection (the headline says "AIDS") occurred among twenty-seven babies and five of their mothers in a hospital in Elista, capital of a region along the Caspian Sea. Some authorities blame unsterilized needles for the babies' infection and suggest that the mothers' infection was contracted while they were breast-feeding the infected babies (John F. Burns, "Outbreak of AIDS Triples Testing in a Soviet City," New York Times, February 5, 1989, p. 29).
What will be the material effects of the global epidemic? Again we can identify a widely accepted set of predictions. In developed countries such as the United States, where 13 percent of the gross national product is spent on health care, AIDS and HIV-related illnesses are already straining the health care system; in many developing countries, where annual expenditures on health care are often less than five dollars per person and inadequate even for current needs, future prospects are grim. The epidemic will almost certainly jeopardize the World Health Organization's ambitious global goal of Health for All by the Year 2000. Further, despite the widespread stereotype of people with AIDS as the disadvantaged of society, the twenty-to-forty age group is the most vulnerable worldwide—the age group most central to the labor force, to childbearing, to caring for the dependent young and old, and, ironically, to marshaling and managing the resources for addressing the AIDS epidemic.[28]
For assessments of the impact of AIDS on the Third World, see testimony in AIDS and the Third World: The Impact on Development; AIDS Prevention and Control: Invited Presentations and Papers from the World Summit of Ministers of Health on Programs for AIDS Prevention (Geneva: World Health Organization; Oxford: Pergamon Press, 1988) [Jointly organized UK government and WHO; held at Queen elizabeth II Conference Centre, Westminster, London, on January 26-28, 1988]; Panos Institute, AIDS and the Third World (London: Panos, in assoc. with Norwegian Red Cross, 1989; Philadelphia: New Society Publishers, 1989 [trade edition of nontrade dossier published 1986, 1987]; Sabatier, Blaming Others; Cindy Patton, Sex and Germs: The Politics of AIDS (Boston: South End Press, 1985); Norman Miller and Richard C. Rockwell, eds., AIDS in Africa: The Social and Policy Impact (Lewiston, N.Y.: Edwin Mellen Press, 1988); R. M. Anderson, R. M. May, and A. R. McLean, "Possible Demographic Consequences of AIDS in Developing Countries," Nature 332 (1988): 228-34; Robert J. Biggar, "Overview: Africa, AIDS, and Epidemiology," in AIDS in Africa, ed. Miller and Rockwell, pp. 1-8; Raymond W. Copson, AIDS in Africa: Background/Issues for U.S. Policy (Washington, D.C.: Congressional Research Service, Library of Congress, 1987 [17 pp.]); Christine Hawkins, "AIDS Expected to Slow Population Growth," New Africa 251 (August 1988): 25; Charles Hunt, "Africa and AIDS," Monthly Review 39, no. 9 (February 1988): 10-22; Institute of Medicine and National Academy of Sciences, Confronting AIDS: Update 1988 (Washington, D.C.: National Academy Press, 1988); Nancy Krieger, "The Epidemiology of AIDS in Africa," Science for the People, January-February 1987, pp. 18-21; M. Over et al., "The Direct and Indirect Costs of HIV Infection in Developing Countries: The Cases of Zaire and Tanzania," paper presented at the International Conference on the Global Impact of AIDS, London, March 8-10, 1988; Kenneth Prewitt, "AIDS in Africa: The Triple Disaster," in AIDS in Africa, ed. Miller and Rockwell, pp. ix-xv; Jane Perlez, "Africans Weigh Threat of AIDS to Economies," New York Times, September 22, 1988, p. 16; Al J. Venter, "AIDS: Its Strategic Consequences in Black Africa," International Defense Review 21 (April 1988): 357-59; Gloria Waite, "The Politics of Disease: The AIDS Virus and Africa," in AIDS in Africa, ed. Miller and Rockwell, pp. 145-64; Catharine Watson, "Africa's AIDS Time Bomb: Region Scrambles to Fight Epidemic," The Guardian, June 17, 1987, pp. 10-11.
Synthesizing many studies on AIDS in Africa, Miller and Rockwell spell out in further detail the demographic, economic, and medical consequences of the epidemic. Education and prevention, they point out, still the best resources for controlling the spread of the virus, are difficult enough in media-rich Western countries; the task of communicating complex health messages to the diverse populations and geographical sites of Third World countries is formidable.[29]Miller and Rockwell, "Introduction," in AIDS in Africa, pp. xxiv-xiv.
These predictions have combined to bring about widespread international agreement about the significance of the epidemic; and as experience increasingly documents the futility of closing boundaries to the virus, so also are global leaders coming to agree with the WHO doctrine that "AIDS cannot be stopped in any country until it is stopped in all countries."[30]Quoted in Marilyn Chase, "Rich Nations Urged to Help Poor Lands Fight AIDS by Backing WHO Program," Wall Street Journal, June 17, 1988, p. 4. On the evolution of the epidemic in Third World countries, see Lawrence K. Altman, "New Support from Africa as WHO Plans Effort on AIDS," New York Times, December 22, 1985, p. 11; Erik Eckholm, "AIDS, an Unknown Disease before 1981, Grows into a Worldwide Scourge," New York Times, March 16, 1987, p. 11; Thomas W. Netter, "AIDS Spurs Countries to Act as Cases Rise around World," New York Times, March 22, 1987, p. 18; Steven V. Roberts, "Politicians Awaken to the Threat of a Global Epidemic," New York Times, June 7, 1987, sec. 4, p. 1; "AIDS Now Is a Global Public Health Crisis, Harvard MD Stresses," American Medical News, June 12, 1987, p. 19. On international cooperation see Simon Watney, "Our Rights and Our Dignity," Gay Times, March 1988, pp. 32-34; Sabatier, Blaming Others; Amadou Traore, "Meeting Point: Dr. Gottlieb Monekosso, WHO Regional Director for Africa," The Courier [Africa-Caribbean-Pacific-European Community] 105 (September-October 1987): 2-5. A cooperative international policy is outlined in the document Concerning a Common European Public Health Policy to Fight the Acquired Immunodeficiency Syndrome (AIDS), Council of Europe Committee of Ministers Recommendation No. R (87) 25; adopted at the 81st session, November 26, 1987. Jonathan Mann, former director of the Global AIDS Program, advocates aggressive, activist strategies to achieve global cooperation; in an "AIDS Monitor" column on the January 1988 global summit (New Scientist, February 4, 1988, p. 32), Mann states that the international declaration reached at the summit represents "an extraordinary consensus." The impact of the epidemic at decade's end is assessed in a four-part series in the New York Times which ran from September 16 to 19, 1990: Erik Eckholm with John Tierney, "AIDS in Africa: A Killer Rages On," September 16, pp. A1, A11; John Tierney, "AIDS Tears Lives of the African Family," September 17, pp. A1, A6; John Tierney, "With 'Social Marketing,' Condoms Combat AIDS," September 18, pp. A1, A6; Erik Eckholm, "Confronting the Cruel Reality of Africa's AIDS Epidemic," September 19, pp. A1, A14.
The power and centrality of numbers to these constructions of AIDS are obvious. Without the sophistication and authority of statistical
methods, the epidemic as a global issue could not have been articulated at all. Yet while this First World numerical chronicle of global AIDS may appear to be unfolding smoothly as our knowledge grows, in fact it is problematic. Consider the following judgments about Africa, all published in 1988:
1. "The continent hardest hit by the AIDS pandemic is Africa where all three infection patterns can be found." (WHO)
2. "Medical experts consider the epidemic an accelerating catastrophe that, in the words of one, 'will make the Ethiopian famine look like a picnic.'" (Congressional Research Service)
3. In many of the urban centers of Congo, Rwanda, Tanzania, Uganda, Zaire, and Zambia, "from 5 to 20 percent of the sexually active age-group has already been infected with HIV. Rates of infection among some prostitute groups range from 27 percent in Kinshasa, Zaire, to 66 percent in Nairobi, Kenya, and 88 percent in Butare, Rwanda. Close to half of all patients in the medical wards of hospitals in those cities are currently infected with HIV. By the early 1990s the total adult mortality rate in these urban areas will have been doubled or tripled by AIDS." (WHO)
4. "A Newsweek cover story claimed one Rakai village [in Uganda] had seven discos and 'sex orgies.' In reality it has 20 mud huts, a handful of fishing boats, and no electricity." (The Guardian )
5. "The tale of AIDS in Africa is not one of widespread devastation and the collapse of nations. There are 53 countries in Africa and AIDS exists substantially in only a few of them." (Washington Post )
6. "Like the tenacious theories put forward as explanations for the heterosexual spread of HIV in Africa, the whole AIDS pandemic is shrouded in mystery and uncertainty. There is no reliable information on AIDS and by the time one message has percolated its way down to the general population, it is out of date and a new one is already on its way to replace it." (West Africa )[31]
(1) Mann et al., "International Epidemiology of AIDS," p. 84; (2) Copson, AIDS in Africa, p. 9; (3) Mann et al., "International Epidemiology of AIDS," p. 84; (4) Watson, "Africa's AIDS Time Bomb," p. 10; (5) Hilts, "Out of Africa," p. 12; (6) Mary Harper, "AIDS in Africa—Plague or Propaganda?" West Africa, November 7-13, 1988, pp. 2072-73, at p. 2072.
Given the statistics cited above, how can it be that the most fundamental meaning of the narrative remains contested?
Several sources of confusion and contradiction can be identified. Estimates of infection and actual cases of AIDS for entire populations may be derived from inadequate data: too few studies, studies of too small a sample size, nonrepresentative samples, and so on. Rates estimated for all Africans are often based on small studies in urban areas; studies of "prostitutes" may in fact classify all sexually active single women as
prostitutes. Chronological claims (about when AIDS first appeared) are primarily based on flawed blood-testing procedures and other problems of diagnostic method. In Africa "underreporting" is taken for granted and estimates corrected upward; at the same time, the number of positive cases actually diagnosed may be too high or too low, depending on the procedure used. Research cited as evidence may be unpublished, based on conference papers unavailable for detailed scrutiny, or sloppily interpreted; and many published papers do not report important data. Moreover, interpretations of the epidemic may be based on divergent and not mutually understood paradigms and forms of evidence. Testing blood samples in a laboratory involves different practical operations and generates knowledge different from that produced by a clinician examining patients or a journalist interviewing people on the street. Experienced medical experts in Africa, who tend to make lower estimates of cases, claim that their knowledge is discounted as clinical and experiential by Western and European academic scientists.[32]
For an overview of problems associated with diagnosis and testing, see Albert E. Gunn et al., AIDS in Africa (Washington, D.C.: Foundation for America's Future, 1988); R. Sher, "Seroepidemiology of HIV in Africa from 1970-1974," New England Journal of Medicine 317, no. 7 (August 13, 1987): 450-51; I. Wendler, "Seroepidemiology of HIV in Africa," British Journal of Medicine 293 (September 27, 1986): 782-85; World Health Organization and Centers for Discase Control, "HIV Not Related to Monkeys," WHO-CDC AIDS Weekly Report, July 25, 1988, p. 8. See also Dieter Koch-Weser and Hannelove Vanderschmidt, eds., The Heterosexual Transmission of AIDS in Africa (Cambridge, Mass.: Abt Books, 1988), especially Felix I. D. Konotey-Ahulu, "AIDS in Africa: Misinformation and Disinformation," pp. 24-25.
Rumor and fantasy play their part as well. Cultural practices are taken out of context, exaggerated, distorted, or invented. Voodoo continues to animate accounts of HIV in Haiti, with grizzly descriptions of Voodoo sorcerers biting off the heads of infected chickens and sucking the bloody stumps. African tales often involve the notorious African green monkey, whose photograph keeps circulating long after his role in AIDS has been discounted. Africans are said to have sexual contact with these monkeys, or eat them, or eat other animals they have infected (Haitian chickens?), or give their children dead monkeys as toys. Purporting to explain why HIV transmission is heterosexual in Africa, reports hypothesize radical differences between African and Western bodies based on physiological, behavioral, cultural, moral, and/or biological factors. As Sander Gilman has comprehensively documented, these rumors are tirelessly fueled by historically entrenched myths of the exotic.[33]
Sander I. Gilman, Disease and Representation: Images of Illness from Madness to AIDS (Ithaca, N.Y.: Cornell University Press, 1988). An influential anthropological source for rumors about exotic behaviors has been Daniel B. Hrdy, "Cultural Practices Contributing to the Transmission of HIV in Africa," Reviews of Infectious Diseases 9, no. 6 (November-December 1987): 1109-19. The rumors preserve bits and pieces of such anthropological research without its larger cultural context. The first major study of prostitutes is Joan K. Kreiss et al., "AIDS Virus Infection in Nairobi Prostitutes: Spread of the Epidemic to East Africa," New England Journal of Medicine 314, no. 7 (February 13, 1986): 414-18. A detailed critique of many studies can be found in Richard C. Chirimuuta and Roaslind J. Chirimuuta, AIDS, Africa, and Racism (London: Free Association Books, 1989), who also suggest that "underreporting" is no more a problem than "overdiagnosing." See also Cynthia Haq, "Data on AIDS in Africa: An Assessment," and Barbara Boyle Torrey, Peter O. Way, and Patricia Rowe. "Epidemiology of HIV and AIDS in Africa: Emerging Issues and Social Implications," both in AIDS in Africa, ed. Miller and Rockwell, pp. 9-19 and 31-54. A general critique of studies on AIDS in Africa is provided by Margaret Cerullo and Evelynn Hammonds, "AIDS in Africa: The Western Imagination and the Dark Continent," Radical America 21, nos. 2-3 (March-April 1987): 17-23, and Krieger, "Epidemiology of AIDS in Africa." An attempt to place AIDS statistics within a broader political and economic perspective is presented in Carol Barker and Meredeth Turshen, "Briefings: AIDS in Africa," Review of African Political Economy 27, no 105 (January-March 1986): 51-54. An elaborate web of speculation about Haiti can be found in Alexander Moore and Ronald LeBaron, "The Case for a Haitian Origin of the AIDS Epidemic," in The Social Dimensions of AIDS, ed. Douglas Feldman and Thomas Johnson (New York: Praeger, 1986), pp. 77-93. The historical debate over "the Haitian origin of syphilis," of course, goes back centuries, a debate noted in his critique of Moore and LeBaron by Paul Farmer, "The Exotic and the Mundane: Human Immunodeficiency Virus in Haiti," Human Nature 1, no 4 (1990): 415-45.
While increased international scientific dialogue has answered some questions about global AIDS and HIV, it has confirmed the difficulty of answering others and has underscored the need for thick description—complex, multileveled, multilayered research. Jay A. Levy's 1988 state-of-the-art collection on AIDS, for example, includes detailed review chapters on AIDS in Haiti and in Africa. Both demonstrate the diverse and very different clinical manifestations of HIV infection in those settings and emphasize the need for revised diagnostic and reporting systems. Treated at length in the Haiti chapter are the complex interaction
of HIV infection with tuberculosis (alluded to by Selzer), while the Africa chapter reviews controversial origin questions as well as various explanations for the high rate of heterosexual transmission; both chapters emphasize remaining questions and the need for continuing investigation.[34]
Nathan Clumeck, "AIDS in Africa," in AIDS: Pathogenesis and Treatment, ed. Jay A. Levy (New York: Marcel Dekker, 1989), pp. 37-63. Existing studies are summarized by Clumeck; by Hilts, in "Out of Africa"; and by Torrey et al., in "Epidemiology of HIV and AIDS in Africa." On the clinical manifestations of AIDS in Haiti, see Warren D. Johnson, Jr., and Jean W. Pape, "AIDS In Haiti," in AIDS: Pathogenesis and Treatment, ed. Levy, pp. 65-78; interactions of AIDS with tuberculosis are discussed on pp. 72-77.
The overwhelming difficulty of even characterizing the diversity of the epidemic, let alone containing it, suggests that statistical measures—numbers—may once again be functioning as Williams says they did in the late nineteenth century: to offer us the illusion of control. As these numbers are taken up and deployed for various urgent purposes, however, they may take on a life of their own and reinforce a view of HIV disease as an unmediated epidemiological phenomenon in which cultural differences (such as differences in sexual practices) can simply be factored into a universal equation. But the local interacts with the global, AIDS continually escapes the boundaries placed on it by positivist medical science, and its meanings mutate on a parallel with the virus itself. Added to the medical, epidemiological, social, economic, and educational challenges of the AIDS crisis is its inevitably political subtext. AIDS is not a precious national resource; it is something nobody wants. Wherever it appears, AIDS discourse quickly becomes political as it is articulated to preexisting local concerns. To begin to identify these concerns, it may be useful to retreat from the power of numbers and see what other forms of knowledge tell us.
In Africa analysis of AIDS must inevitably confront questions of decolonization, urbanization, modernization, poverty, endemic disease, and development: in Uganda, for example, the legacy of civil war is significant in assessing the AIDS situation, as is the influence of the church in discussions of health education; in Kenya, for the independent press at any rate, AIDS is used as an ongoing test of the central government's ability to acknowledge and resolve conflict.[35]
See, for example, Caputo, "Uganda: Land beyond Sorrow"; Lloyd Timberlake, Africa in Crisis: The Causes, the Cures of Environmental Bankruptcy, ed. Jon Tinker (Philadelphia: New Society Publishers, 1986); and ongoing coverage in the Nairobi Weekly Review.
In France Jamie Feldman found in interviews that for French AIDS researchers the AIDS epidemic "reveals the impact that France's colonial past and present African immigration have on French life."[36]Jamie Feldman, "Identity, Illness, and the Process of Giving Meaning: French Medical Discourse on AIDS," unpublished manuscript, University of Illinois at Urbana-Champaign, July 1988. See also Michael Pollack, Les homosexuels et le SIDA: Sociologie d'une épidémie (Paris: Éditions A. M. Metailie, 1988).
In his ethnographic study of AIDS in urban Brazil, Richard Parker suggests that the epidemic needs to be linked to "the social and cultural construction of sexual ideology," or what he calls the "cultural grammar" of the Brazilian sexual universe.[37]Richard Parker, "Acquired Immunodeficiency Syndrome in Brazil," Medical Anthropology Quarterly 1, no. 2 (1987): 155-75, at pp. 158, 159.
In both the United States and Great Britain, AIDS intensifies stress on health care systems already in crisis. In South Africa apartheid is seen to reproduce itself in the government's public health campaign: a post-campaign survey of black attitudes in the Johannesburg area found thatmany believed there were "two totally different kinds of AIDS. The one that only affected blacks was acquired through sexual and ritual contact with baboons in central Africa. The other was acquired by sexual contact with homosexuals—white AIDS."[38]
David Seftel, "AIDS and Apartheid: Double Trouble," Africa Report (November-December 1988): 17-22, at p. 21.
In Cuba mandatory HIV testing of the general population has identified a small number of infected people, who have been placed under indefinite quarantine. Placed in AIDS sanitoria, they receive air conditioning, color television, regular health checkups, and other amenities not generally available to the population at large. This treatment is variously interpreted by Western commentators as a manifestation of Cuba's progressive health care policies (one can certainly argue that Cuba is providing more support and resources for its infected citizens than many other countries) or as totalitarian and homophobic repression in a police state.[39]See Elizabeth Fee, "Sex Education in Cuba: An Interview with Dr. Celestino Alvarez Lajonchere," International Journal of Health Services 18, no. 2 (1988): 343-56; Nicholas Wade, "Cuba's Quarantine for AIDS: A Police State's Health Experiment," New York Times editorial, February 6, 1989; p. A14; Richard Goldstein, "AIDS Arrest: The Cuban Solution," Village Voice, February 14, 1989, p. 18.
These examples and others suggest that the reproduction in AIDS discourse of existing social divisions appears to be virtually universal, whether it is white or black AIDS, gay or straight AIDS, European or African AIDS, wet or hot AIDS, East or West German AIDS, central African or western African AIDS, foreign or native AIDS, guilty or innocent AIDS.[40]
Though these dichotomies are primarily social, the differentiation among types of AIDS and strains of HIV is also a scientific and clinical question. See, for example, Clumeck, "AIDS in Africa."
A First World/Third World dichotomy manifests itself in diverse ways. In Africa people with AIDS are sometimes described by those in their own countries as having sexual practices as strange as those of gay white men in San Francisco.[41]Hilts (in "Out of Africa," p. 12) notes the incredulity that greeted the appearance of AIDS in Africa. He quotes a pulmonary specialist in Uganda who first saw AIDS there in 1983: "It looked like the new American disease. But none of us could believe it." But before too long, AIDS began to be blamed on the loose morals of African people—always those in other countries, classes, or ethnic groups. Thus, an editorial in the Kenya Times (Nairobi), May 26, 1987, blamed Uganda for lax sexual behavior, noting that "nature has its own law of retribution." See discussion in Sabatier, Blaming Others, p. 105. In contrast, see Frank Browning, "AIDS: The Mythology of Plague," Tikkun 3, no. 2 (March-April 1988): 69-71. Browning says that most descriptions of U.S. subcultures involved in AIDS make them sound "as strange as those of Bantu twig gatherers" (p. 70).
In Japan officials believed initially that transfusion-related HIV infection among Japanese would not be a threat thanks to procedures for sequestering the national blood supply; while this Japanese/foreign division remains an animating feature of AIDS discussion and policy, statistics make clear that it can no longer be considered a safeguard.[42]Clyde Haberman, "Japan Plans to Deny Visas over AIDS," New York Times, April 1, 1987, p. A18. According to a report in the Independent (London), February 14, 1987, when the death of a Japanese prostitute in Kobe was attributed to AIDS, the immediate conclusion was that she had been infected by sexual contact with a foreigner; as one Japanese newspaper put it, "Her death was the result of an infatuation with Europe." Sabatier (in Blaming Others, p. 114) notes that "in the red light district of Tokyo warning signs suddenly appeared: 'Gaijin [foreigners] off limits.'" For a more extended discussion, see James W. Dearing, "Foreign Blood and Domestic Politics: The Issue of AIDS in Japan," in this volume.
Richard Parker identifies a similar dichotomy in the Brazilian medical community's transition from conceptualizing AIDS as a "foreign import" to accepting it (from 1985 on) as a disease that has "taken root."[43]Parker, "Acquired Immunodeficiency Syndrome in Brazil," p. 157; and Alan Riding, "AIDS in Brazil: Taboo of Silence Ends," New York Times, October 28, 1987, p. 8.
Great Britain's announcement that HIV-positive applications for visas from high-risk countries would be denied entry provoked accusations of racial imperialism when central African countries were classified as "high risk" but the United States was not.[44]Sabatier, Blaming Others, pp. 106-7. See also Robert Pear, "U.S. Seeks to Bar Aliens with AIDS," New York Times, March 27, 1987, p. A18; and Serge Schmemann, "Calls of 'Hi Sailor' Get the Heave-Ho," New York Times, May 14, 1988, p. 4.
These divisions are, at least in part, produced by what Dubos calls the inadequacies of the modern world—that is, by a set of historically produced social arrangements. When AIDS in Africa or Brazil is termed "a disease of development," it is precisely the intractable social topography of recent history that is invoked, the problematic contours of development—environmental devastation, malnutrition, war, social
upheaval, poverty, debt, endemic disease—now unavoidably illuminated and scrutinized in the international light of the AIDS crisis. As Rudolph Virchow wrote in 1948, "Epidemics correspond to large signs of warning which tell the true statesman that a disturbance has occurred in the development of his people which even a policy of unconcern can no longer overlook."[45]
Dubos, Mirage of Health, p. 218; many researchers characterize AIDS as a "disease of development," among them Marc H. Dawson, "AIDS in Africa: Historical Roots," in AIDS in Africa, ed. Miller and Rockwell, pp. 58-69. Virchow is cited in Paul Epstein and Randall Packard, "Ecology and Immunology," Science for the People (January-February 1987): 10-17, who also discuss AIDS and development.
Even the seemingly simple message to "use a condom" is actually a complicated drama that must incorporate competing scripts, play to hostile audiences, and ultimately raise as many questions as it answers. Already it has returned to the world stage such stock characters as the Ugly American who, in the guise of the U.S. Agency for International Development, distributed in central Africa condoms that were too small and inelastic.[46]
Brooke Grundfest Schoepf et al., "AIDS and Society in Central Africa: A View from Zaire," in AIDS in Africa, ed. Miller and Rockwell, pp. 211-35, at p. 218.
But the larger point is that, as Brooke Grundfest Schoepf and her colleagues argue, the adoption of condoms involves "much more than a simple transfer of material culture."[47]Ibid., p. 228; the authors observed (as USAID, apparently, did not) that condoms "which hurt their wearer or break during normal use may limit the effectiveness of AIDS prevention efforts." See also Hooper, Slim
Describing their experience with Project CONAISSIDA (an AIDS education and research program in Zaire), these researchers identify myriad ways that the condom question puts stress on the entire fabric of social relations. They point out, too, that the AIDS crisis is embedded in a continuing economic crisis that affects men and women differently: married women in plural households may take up prostitution as a means of economic existence when their husbands can under current conditions no longer support the traditional plural households. Women's groups with whom CONAISSIDA has contact express interest in information about AIDS, and about condoms; but they also articulate resistance to the view that information and condoms offer a total solution, emphasizing the role of deepening poverty and the need for income-generating activities for women to provide alternatives to multiple-partner sex.A different sort of complication is raised in Africa by the important role of nongovernmental organizations (NGOs). While these organizations may be reluctant to shift their agendas for AIDS or to ally their already fragile causes with a yet more stigmatized one, they nevertheless often have excellent international and community networks. The International Family Planning Agency has prepared and distributed a well-received manual on AIDS for local as well as national use; such efforts are likely to bring about increased U.S. aid for family planning.[48]
Gill Gordon and Tony Klouda, Preventing a Crisis (London: International Planned Parenthood Federation, 1988). Reviewed by Harper, "AIDS in Africa—Plague or Propaganda?"
But as Schoepf and her colleagues point out,Ideological issues also need to be addressed. In Zaire nationalist sentiment currently links contraception and condom use to western population control strategies, which are viewed as a form of imperialism. Some husbands also
view contraception as an encouragement for wives' extramarital sexual relations. … These considerations suggest that it may be preferable to separate AIDS prevention from birth control efforts, rather than to place responsibility for AIDS interventions within family planning programs.[49]
Schoepf et al., p. 219. Few alternatives to the condom exist. At the Fifth International Conference on AIDS in Montreal, there was for the first time discussion of a female condom and of the use of spermicides without the use of condoms; but at the Sixth International Conference in San Francisco, some data suggested that for some women the use of spermicides might increase the risk of HIV transmission by causing inflammation and breakdown of the vaginal mucosa.
But fruitful acknowledgment of division is not accomplished by formula. To take one final example, the system of sexual classification that dominates discussions of AIDS internationally—heterosexual, homosexual, bisexual—is not universal. Criticisms of this system applied to AIDS discourse in Western industrialized countries are all the more valid in other cultures; for not only is sexuality complicated for individuals, with no fixed correspondence among the components of sexual desire, actual practice, self-perceived identity, and official definition; it is culturally complicated as well. Richard Parker argues that the hetero/homo/bi classification is seriously, conceptually, at odds with "the fluidity of sexual desire" in contemporary Brazil.[50]
Parker, "Acquired Immunodeficiency Syndrome in Brazil," p. 161.
While the medical model's distinctions clearly exist in Brazilian society and are increasingly familiar as a result of media dissemination, they remain largely part of an elite discourse introduced to Brazil in the mid-twentieth century. The traditional classification relates sexual practices to gender roles , with both gender and sex constructed by a fundamental division between a masculine atividade (activity) and feminine passividade (passivity). Two males engaged in anal intercourse would be distinguished by who was the active masculine penetrator, who the passive feminine penetrated. Neither would necessarily perceive his behavior as "homosexual," nor would everyday language readily furnish him with the lexicon to do so. As Parker suggests, this different perception of same-sex behavior has obvious and dismaying implications for conventional notions of "risk group" identification and "safer sex" education.[51]Ibid., pp. 160-63. I have greatly oversimplified Parker's intricate representation of Brazilian sexuality, which, as he emphasizes, is not the mere overlay of a Western ethnographer but permeates language, slang, informal discussion, and ongoing open debate about sexuality as an essential aspect of cultural identity and "Brazilianness." But the penetrator/recipient and other distinctions that construct masculinity/femininity between same-sex partners occur elsewhere, including the United States. See Charles F. Turner, Heather G. Miller, and Lincoln E. Moses, eds., AIDS: Sexual Behavior and Intravenous Drug Use (Washington, D.C.: National Academy Press, 1989), pp. 73-185, for an illuminating review of recent research on "same-gender sexual behaviors" in several cultural settings. See also Ralph Bolton, "A Selected Bibliography on AIDS and Anthropology" (forthcoming in Journal of Sex Research). For an analysis of sexuality from a different perspective, but one potentially helpful in articulating women's concerns, see the conclusions and recommendations "adopted by the group of experts" at a UNESCO conference in Madrid, March 12-21, 1986 ("UNESCO: On Prostitution and Strategies against Promiscuity and Sexual Exploitation of Women," Echo [Newsletter of the Association of African Women for Research and Development] 1, nos. 2-3 (1986): 16-17).
Parker's work, like other projects noted here, demonstrates the contributions of interpretive cultural analysis. The provisional nature of science is very difficult for policy and funding agencies to live with. Rather, there is pressure to produce a coherent narrative in which qualifications and ambiguities, if they must be mentioned, become simply routinized features of the story, to be quickly forgotten; problems of data are perceived to be mere temporary impediments to a refined and comprehensive analysis. Western medical science is conceived as a transhistorical, transcultural model of reality; when cultural differences among human communities are taken into account, they tend to be enlisted in the service of this reality, but their status remains utilitarian. This utilization may effectively accomplish specific goals: it is reported
that some native practitioners (e.g., of voodoo) have successfully overcome men's traditional resistance to the use of condoms by describing AIDS as the work of an evil spirit who uses sexual desire and the virus as secret weapons; condoms provide a means to trick the spirit and escape its lethal designs.[52]
Sabatier, Blaming Others, p. 134.
One can certainly support a global anti-AIDS strategy that mobilizes the scientific model of AIDS in culturally specific ways, yet acknowledge imperialist aspects of a strategy that valorizes itself as universal rather than culturally produced. As the foregoing examples suggest, ethnography and other forms of interpretive research are neither better nor less mediated than statistical approaches or other "objective" ways of knowing a culture, but they are different and produce unique insights. Nor are they incompatible with theoretical sophistication.
Research of this kind is not, however, the currency of the First World/Third World transaction. Expert advising is now a major Third World industry: more than half of the $7–8 billion spent yearly on aid to Africa goes to European and North American professionals trained to provide expertise to the Third World.[53]
Timberlake, Africa in Crisis, p. 8.
Gathering information, reporting facts, and advising the Third World are also mediated activities, permeated by history and convention. In Blaming Others , the Panos Institute's immensely useful 1988 sequel to and self-critique of its indispensable 1986 dossier AIDS and the Third World , Renée Sabatier observes how ironic it is that in the information age, information should be such an elusive resource.[54]Sabatier, Blaming Others, p. 4.
But a second irony explains the first. It is not, precisely, a question of obtaining and disseminating "information" but, rather, of acknowledging what information entails: acknowledging how language works in culture, how stories contradict one another, how narratives perform as well as inform, how information constructs reality. Cultural analysts in many fields are acknowledging the inevitability and indeed even the necessity of such multiple and contradictory stories. Yet, having recognized the theoretical complexity of communication, we are pressing communication into a purely pragmatic role that subordinates complication and contradiction to unequivocal assertion and scientific harmony.Different accounts of truth produce differing material consequences. Tracing the historical relationship between the "country" and the "city" and their evolution in English literature and social thought, Raymond Williams argues that in the course of nineteenth-century imperialism these two ideas became a model for the world, dividing not only the rural from the urban within a single state but the undeveloped world
from the developed one. Underlying this model is the notion of universal industrialization, underdeveloped countries always on their way toward becoming developed, just as the poor man is always assumed to be striving to become rich. "All the 'country' will become 'city': that is the logic of its development."[55]
Williams, The Country and the City, p. 284.
Though this linear progression is largely a myth of late capitalism, that does not impede its deployment as an agenda item for the Third World.For the new possibilities arising out of the AIDS epidemic, the "country" is a very fertile field. As of 1986, according to a reference work called Emerging AIDS Markets , 1,119 companies and other organizations are involved in AIDS-related activities: only 20 to 30 of them are based in Third World countries, but at least 200 of them are engaged in research on AIDS in Africa and other projects likely to entail the use of Third World populations as trial subjects in the development of diagnostic products and vaccines.[56]
Emerging AIDS Markets: A Worldwide Study of Drugs, Vaccines, and Diagnostics (New Haven, Conn.: Technology Management Group, August 1986). See also Vicki Glaser, "AIDS Crisis Spurs Hunt for New Tests," High Technology Business 8, no. 1 (January 1988); and Manny Ratafia and Frederick I. Scott, Jr., "AIDS: A Glimpse of Its Impact," American Clinical Products Review (May 1987): 26-29; this article also makes clear the size and diversity of the "AIDS market" for the development of clinical products.
Recent reports about vaccine trials make explicit the need for test populations that are "pharmacologically virgin" and, further, are still becoming infected at high rates. Gay men and IV drug users in the First World do not fulfill these criteria, not only because infection is leveling off in the first group and pharmacological virginity is not characteristic of the second, but also because any First World population is too educated, too exposed to the media, and too likely to take steps (including alternative treatments) to avoid infection or reduce clinical illness. In the mind of the city, only the country can furnish the unspoiled virgin material that the market needs, the naive informant still too ignorant to contradict instructions.[57]See Gina Kolata, "Africa Is Favored for AIDS Testing," New York Times, February 19, 1988, p. 7; the "AIDS Monitor" column in the New Scientist, February 18, 1988, p. 36; and Jane Perlez, "Scientists from Western Countries Pressing for AIDS Studies in Africa," New York Times, September 18, 1988, p. B5. Perlez, reporting vaccine discussions at a conference in Tanzania on AIDS and Africa, writes: "In Africa, unlike the United States, the virus is most commonly spread through heterosexual contact. Officials believe that, despite warnings to use condoms and avoid multiple partners, further spread of the virus is inevitable. ... Because of behavioral changes brought about by extensive education about AIDS, the spread of the infection among gay men in the United States has slowed. Thus, there would be few new infections in a study group, whether or not its members took the vaccine, the scientists said. The scientists said they regarded intravenous drug users, a group that continues to have a high incidence of AIDS in the United States, as unreliable for the necessary follow-up that is needed for a study group." A WHO committee developing ethical guidelines for vaccine testing said the decision to go ahead should be made by three groups: scientists developing the vaccine, scientists knowledgeable about vaccine development but with no academic or commercial stakes in it, and "government officials and their scientific advisers from the population where the vaccine is to be tried." No representatives of the population to be tested are mentioned.
First And Third World Chronicles
History is a legend, an invention of the present.
Mudimbe, Invention of Africa[ 58]V. Y. Mudimbe, The Invention of Africa: Gnosis, Philosophy, and the Order of Knowledge (Bloomington: Indiana University Press, 1988), p. 195.
The ethnographer's trials in working to know another people now become the reader's trials in making sense of the text.
Pratt, "Fieldwork in Common Places"[59]Pratt, "Fieldwork in Common Places."
But there is always another story, and a continuing one in the AIDS epidemic involves the untrustworthiness of other stories—their sources, motives, data, presuppositions, methodology, and conclusions. In January 1985, for example, the Nairobi Standard publicly reported the
presence of AIDS in Kenya for the first time in stories headlined "Killer disease in Kenya" and "Horror sex disease in Kakamenga."[60]
Nairobi Standard, January 15 and 18, 1985. For the development of research on AIDS in Africa, see Ruth Kulstad, ed., AIDS: Papers from Science, 1982-1985 (Washington, D.C.: American Association for the Advancement of Science, 1986); and Koch-Weser and Vanderschmidt, The Heterosexual Transmission of AIDS in Africa.
Subsequent accounts in state-owned newspapers repudiated the report, claiming that the deaths were from skin cancer rather than AIDS, but Western press accounts speculated increasingly on the frightening implications of the presence of AIDS in central Africa. Then in November 1985 Lawrence K. Altman's multipart series on AIDS in Africa in the New York Times reported not only that the epidemic was spreading rapidly in Africa but also that prominent U.S. researchers were convinced the disease started there. Altman's opening sentence dramatically presented the thesis that was to become most controversial: "Tantalizing but sketchy clues pointing to Africa as the origin of AIDS have unleashed one of the bitterest disputes in the recent annals of medicine."[61]Lawrence K. Altman, "Linking AIDS to Africa Provokes Bitter Debate," New York Times, November 21, 1985, p. 1.
Altman went on to say that these "sketchy clues," including blood samples, "have led to what has now emerged as the prevailing thesis in American and European medical circles that the worldwide spread of acquired immune deficiency syndrome began in Central Africa, the home of several other recently recognized diseases."But, as Altman conceded, not everyone accepts this designation of the virus's homeland: "The Africans vigorously disagree, and there is some criticism of the validity of the studies on which the theories are predicated. Indeed, controversial new results point both to and against AIDS originating in Africa, a fact that is fueling the international furor."[62]
Altman, "Linking AIDS," p. 1. On the "international furor" see especially Chirimuuta and Chirimuuta, AIDS, Africa, and Racism; and Richard C. Chirimuuta, Rosalind Harrison, and Davis Gazi, "AIDS: The Spread of Racism," West Africa, February 9, 1987, pp. 261-62.
Two effects in the West of the Times series were to establish AIDS in Africa as an important scientific question and to place Africa firmly on the national agenda for AIDS media coverage, culminating in the journalistic frenzy of late 1986, which represented Africa as "devastated" by AIDS and AIDS-related illnesses. In Africa the effect was different. When Altman's series began to run in the International Herald Tribune in November 1985, for example, outraged Kenyan officials confiscated the entire shipment. The African offensive against the "African origin" theory was launched with an editorial in Medicus , the official publication of the Kenya Medical Association, which hypothesized that tourists from around the world had introduced AIDS into Africa.[63]
In the Western media AIDS in the Third World is used to draw conclusions about the West. Thus, Selzer's view that Haiti is "devastated" is intended to serve as a cautionary lesson about gay excess. Stories about Africa may likewise serve to warn Western readers about themselves. "FUTURE SHOCK," proclaimed the cover of Newsweek in December 1986, citing new worrisome projections of AIDS increases in the United States; a related cover headline was titled "AFRICA: THE FUTURE IS NOW." On AIDS and the media in general, see James Dearing and Everett M. Rogers, "The Agenda-Setting Process for the Issue of AIDS," paper presented at the International Communication Association, May 28-June 2, 1988; and Kinsella, Covering the Plague.
At this point the Kenyan newsmagazine Weekly Review , published and edited in Nairobi by Hilary Ng'weno and widely considered one of the best newsmagazines in Africa, took on the responsibility of keeping the public informed about AIDS reports in the African and international press. In the face of increasingly vocal controversy and government
silence, the magazine took the general position that developing adequate public health measures was more important than countering Western propaganda. Thus, the Weekly Review began providing summaries and analyses of scientific and press reports printed in the West, citing the numbers of AIDS patients reported in Zaire, Rwanda, Uganda, and Kenya. Although itself often critical of the Kenyan government's mode of responding to the AIDS epidemic, the Weekly Review has also been critical of Western reporting. What Africa needs, Ng'weno told the Panos Institute, is concrete assistance, not "a never ending siren recounting a litany of disasters about to engulf the continent."[64]
Quoted in Sabatier, Blaming Others, p. 97.
An insightful analysis of the AIDS situation in Kenya is provided by the political scientist Alfred J. Fortin. Although Fortin criticizes the actions of the African government, he is primarily critical of what he has elsewhere called the "aggressive bureaucratic and careerist politics" of the "development establishment"; unless development agencies remain under fire, he argues, the AIDS epidemic will allow them to reproduce the power relations of dominance and dependency already in place. In "The Politics of AIDS in Kenya," Fortin argues further that the dominance-dependency relationship of development guarantees English as the international language of AIDS discourse, a language that is necessarily "blind to the African world of meaning." He concludes that, despite Kenya's "comparatively well-developed medical infrastructure and working coterie of Western scientists, its efforts have fallen short of even the minimum requirements suggested by its statistics."[65]
Alfred J. Fortin, "The Politics of AIDS in Kenya," Third World Quarterly 9, no. 3 (July 1987): 906-19, at p. 907. See also Alfred J. Fortin, "AIDS and the Third World: the Politics of International Discourse," paper prepared for the 14th World Congress of the International Political Science Association, Washington, D.C., August 28-September 1, 1988.
However much the Weekly Review may itself be skeptical of "the development establishment" as well as Kenya's response to the AIDS epidemic, it does not buy Fortin's position either. Calling his paper "a hard-hitting and indictive, if lopsided, criticism of the Kenyan government, the ministry of health and the local press," the editor goes on to contest a number of points of Fortin's analysis—for example, Fortin's point about language:
[Fortin's] paper questions the language of discourse at discussions on AIDS in Africa. It argues that Africans have chosen to use the Western language when talking about the disease and since the language is transplanted, Africa is dependent on the West for its meaning and its continued development. Since the language is not indigenous to Africa, Fortin says, hence it is "blind to the African world of meaning."
Students of African history have long argued that most of the diseases prevalent in Africa today were first witnessed with the advent of the foreigner on the continent and most of the terminology used by the medical practitioners in Africa [is] also borrowed from the developed world.
African government and researchers have also been emphatic that the AIDS virus was first diagnosed in the United States and, therefore, it would follow automatically that the language used in reference to the disease should be that developed by those who diagnosed it first.[66]
Hilary Ng'weno, "The Politics of AIDS in Kenya," Weekly Review, September 4, 1987, pp. 11-13.
As I understand it, Fortin's argument about discourse was intended to challenge—as Parker's is with regard to Brazil—the entire discursive formation of international AIDS discussions applied unthinkingly and hence in some sense imperialistically to diverse cultures; it is a position most discourse analysts would share. Ng'weno, however, rejects the corollary implication of this view: that English is somehow "foreign" to Kenya and Kenyan leaders. Though English is indeed a colonial legacy, it plays many roles in Kenyan activities today. Hence, Zairean philosopher V. Y. Mudimbe argues that Western discourse has contributed to but not monopolized what he calls "the invention of Africa"; rather, the objects of that discourse are also subjects who have produced an intricate interweaving of European and African commentary, rendering the notion of a "purely African discourse" an impossible dream.[67]
Mudimbe, The Invention of Africa.
At the same time, Ng'weno makes the political point that language marks nationality and origin: to use English with regard to AIDS helps sustain its identity as a Western disease. Ng'weno's position acknowledges the power of linguistic constructions of reality, and demands the right of Africans to participate in that construction process. This resistance to adopting AIDS, to giving it—in the words of the Altman story—a home, is reflected elsewhere in the Weekly Review , where supposedly indigenous African terms for AIDS and AIDS-related terms (like "slim disease" and "AIDS belt") are placed in quotation marks and often explicitly rejected; the term magada , cited by Fortin as the name for AIDS in Swahili, is never used in the Review .[68]The naming of AIDS internationally is addressed by Sabatier, Blaming Others; Hooper, Slim; and Farmer, "The Exotic and the Mundane."
The juxtaposition of these two complex and interlocking analyses makes clear that the chronicle of AIDS in the Third World cannot be understood monolithically. It must be understood not only in terms of the "rich history and complex political chemistry" of each affected country but also as a heteroglossic series of conflicted, shifting, and contradictory positions.[69]
Miller and Rockwell, AIDS in Africa, p. xxiii.
Even "AIDS" and "the AIDS epidemic" and "HIV disease" must be understood this way. We are talking, after all, about an epidemic disease with more than forty distinct clinical manifestations, some of which consist of the absence of manifestation, some of which are unique to particular regions of the world, and some of which apparently have nothing to do with a deficiency of the immune system. When we talk about the Third World, we are talking about more thanone hundred countries of the world. In Africa alone, we are talking about a continent four times as large as the United States, which has more than 50 countries, 900 ethnic groups, and 300 language families (Zambia alone has 74 languages). As Miller and Rockwell argue, it is absurd to talk about "the AIDS problem in Africa" except for specific and well-defined purposes.[70]
Ibid., p. xxiii.
The international AIDS narrative is hence neither complete nor fully accessible. The present invents the past, but the present itself has not yet been invented; accordingly, this is a narrative necessarily in process, which we must read with all our critical faculties at work. A crisis serves as a point of articulation for multiple voices and interests, and the AIDS crisis in the Third World is no different. My goal has been to demonstrate that, as in the First World, (1) diverse interests are articulated around AIDS in ways that are socially and culturally localized and specific; (2) institutional forces and cultural precedents in the First World prevent us from hearing the story of AIDS in the Third World as a complex narrative; (3) understanding this complexity is a necessary if not sufficient condition for identifying the material and conceptual nature of the epidemic; and (4) such an identification is necessary to effectively mobilize resources and programs in a given country or region.
In the course of this essay, I have identified several analytic strategies through which we may explore these questions and tried to suggest areas of discourse where better understandings may be particularly valuable: the conventions of mass media stories; the discursive traditions and modes of representation that figure in the AIDS narrative of the sciences and social sciences (including tropes, stereotypes, linguistic structures, and pervasive metaphors); the emergence of a dominant international AIDS narrative and its role in the linguistic and professional management of the epidemic; the processes through which AIDS is conceptualized within given institutions for everyday use; and the very terms through which we identify what chronicle we think we are telling. The checks and balances provided by the warring voices at each of these multiple discursive points render it impossible to refuse contradiction—that is, to argue that any single unchallenged account of AIDS exists in the Third World, any more than it does in the First World.
To hear the story "AIDS in the Third World," we must confront familiar problems in the human sciences: How do we know what we know? What cultural work will we ask that knowledge to perform? What are our own stakes in the success or failure of that performance? How do we document history as it unfolds? In concrete terms, we certainly
need to forsake, at least part of the time, the coherent AIDS narrative of the Western professional and technological agencies and listen instead to multiple sources about and within the Third World.[71]
Nancy Schmidt, "African Press Reports on the Social Impact of AIDS on Women and Children in Africa," paper presented at conference on the Impact of AIDS on Maternal-Child Health Care Delivery in Africa, University of Illinois, Urbana-Champaign, May 6, 1990.
When we do so, we may find it less instructive to determine whether a given account is true or false than to identify the diverse rules and conventions that govern whether and where a particular account is received as true or false, by whom, and with what material consequences.The performative work that such narrative structures do can be identified, challenged, recuperated, reassigned; it cannot be eradicated. Language about AIDS, illness, and epidemics is already informed with metaphor (influenza got its name because illnesses were believed to be under the influence of the stars; infect means "to contaminate," "to communicate," and "to stain or dye," a connotative web even the most vigilant housekeeping cannot sweep away). To believe that information and communication about AIDS will separate fact from fiction and reality from metaphor is to suppress the linguistic complexity of everyday life. Further, to inform is also to perform; to communicate is also to construct and interpret. Information does not simply exist; it issues from and in turn sustains a way of looking at and behaving toward the world; it shapes programmatic agendas and even guides capital investments.
Diverse voices, then, represent not diverse accounts of reality but significant points of articulation for ongoing social and cultural struggles. Further, once we adopt the view that reality is inevitably mediated, we become ourselves participants in the mediation process; such voices may then provide important models for challenging existing regimes of truth and disrupting their effects—in the Third World, as in the First.