10. Exorcising the Spirits: The Alternative Therapeutics of Protestantism[1]
I wish to end this study with a discussion of an alternative form of healing offered by an unusual group of vahiny in northwest Madagascar. Protestant exorcists serve as a final option in a locally conceived hierarchy of resort (Romanucci-Ross 1977), especially for problems associated with spirit possession and madness. A wide array of indigenous practitioners (including tromba, kalanoro, moasy, mpisikidy) play key roles in diagnosing and treating the symptoms associated with these categories of experience.[2] However, if their repeated efforts fail to improve the health status of a patient she (usually with her kin) may seek treatment from other healers whose training is derived from nonindigenous (Western and Christian) sources.
Two factors account for this reluctance on the part of Sakalava patients and their kin to consult with Protestant exorcists. First, ethnic factionalism is key. Although exorcists working in northern Madagascar are all Malagasy, they are rarely Sakalava, and many come from the high plateaux. The fact that they are strangers creates an interesting dynamic in the context of therapy. Second, Protestants embrace a competing view of reality and, more specifically, of possession. Since they consider tromba spirits to be evil, few Sakalava are willing to seek out their treatments. In some cases, however, the exorcists’ healing approaches and philosophy offer a welcome escape from the otherwise unavoidable problems that accompany possession.
The therapy offered by Protestants also carries important implications for the study of the ongoing dynamics of identity and power. As shown throughout this work, tromba is a mainstay of social life in Ambanja, yet a minority of women eventually choose to opt out of mediumship. One’s social status is raised by virtue of being a medium and healer, but the possession experience has its problems. As all mediums say, their spirits make them “suffer” (mijaly). From a Sakalava perspective, once a spirit is instated, possession is permanent, and a medium must accept the suffering that accompanies this status as part of her fate. A few, however, find the associated hardships to be intolerable. Exorcists offer these mediums a way to be freed of their spirits. In order to do so, however, a medium must reject Sakalava respect for and beliefs about royal ancestors. Exorcists also expect their clients to convert to Protestantism, thus permanently embracing a worldview contrary to that of their own culture.
| • | • | • |
Sakalava Perceptions of Possession and Madness
In Ambanja, when mediums and other informants describe possession they sometimes compare it to madness (adala, adalan̂a; also, marary saina,very saina/jery, “sick” or “lost mind”). Even though possession and madness are regarded as distinct categories of experience, they overlap somewhat in their causation, symptomatology, and treatment. According to Sakalava informants, possession and madness define a spectrum of symptoms where severity is an important distinction. In this model, tromba possession and madness occupy opposite poles, and possession sickness falls somewhere in between (see figure 10.1). This spectrum of experiences ranges from a good, powerful, and inescapable state to a destructive, dangerous, and frightening illness.
Tromba possession is distinct in that it is an accepted form of behavior and experience, involving periodic changes in personality, dress, and other characteristics as the medium moves in and out of trance. Although tromba spirits periodically may cause harm to a medium—making her sick if they are angry, for example—they are generally regarded as sacred, powerful, and beneficial entities that look after the medium, her kin, and her clients.
Njarinintsy, masoantoko, shay-tuan and bilo are evil, reckless, and uncontrollable spirits. Since they simultaneously are forms of spirit possession and sickness (marary), they occupy a position somewhere between tromba and madness. As described in chapter 9, a njarinintsy, for example, is a generic spirit that has no personal name. Although it possesses and controls the body of its victim, this (as well as other forms of possession sickness) is temporary, and it is regarded as a special form of illness that ceases when the spirit is driven from its victim. During fits of possession a victim may be described as being temporarily mad, suffering from a “sick mind” or “sick spirit” (marary saina) because she periodically and uncontrollably shouts obscenities, attacks people, or wanders aimlessly through the streets. If the harmful spirit(s) is not driven from the victim it may have long-lasting effects, ultimately driving her permanently insane or even killing her.
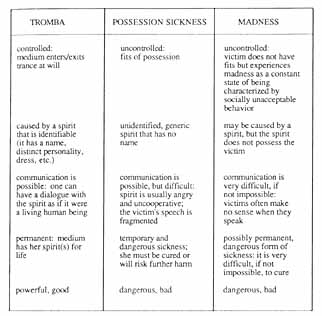
10.1. Characteristics of Possession and Madness (Sakalava interpretations).
Madness is a general illness category defined very broadly by more serious forms of deviant behavior which are fairly constant and long-term. Madness is a frightening problem, for, as an extreme illness category, it is very difficult to cure. It is defined in reference to possession, but it is not the same. Madness may be caused by an angry spirit, brought upon its victim by a tromba because she is resisting possession, or by a malicious spirit, such as a njarinintsy, which has been allowed to stay too long within her. One of the primary problems with madness, however, is it does not necessarily result from a foreign entity that actually resides in the victim. The intangibility of the problem is part of what makes it extremely difficult to treat.
Possession offers other clues for understanding Sakalava conceptions of madness. Whereas tromba is good (tsara) and sacred (masina), madness, like possession sickness, is bad (raty). Communication is also an important factor in distinguishing these categories from one anther. Tromba spirits have full-fledged personalities that enable them to converse and interact with the living. The speech of njarinintsy and similar spirits, on the other hand, is angry and garbled. The mad occupy the other polar extreme: they speak nonsense and this is a constant state for them, unlike the fits that characterize possession sickness.
Although madness may sometimes be confused with possession sickness (especially at onset), it is a distinct category because it is viewed as an extreme and potentially permanent state of being. In Ambanja there were two individuals who were often seen in public places and who were labeled as mad (adala, adalan̂afa). One was an Antandroy man who wore women’s clothing and who carried a stick, which he would swing at passersby. The second was a Comorean woman who, even though she had kin in town, preferred to sleep outside and eat out of garbage heaps. In contrast, the behavior of a victim of possession sickness may be very odd or frightening, but after a fit has ended she appears normal and does not remember what happened. The significance of the breaking of social norms in labeling the mad is evident in the manner in which the diminuitive term adaladala is applied. It is used, in a teasing way, to describe anyone who acts odd or silly. As the following story illustrates, a person must be seriously ill to be called adala or adalan̂a.
The Case of Victoria
One of the more spectacular public displays of njarinintsy violence that I witnessed occurred one afternoon on the main street of Ambanja. As this case illustrates, the application of the label of possession sickness became increasingly problematic, eventually leading those who knew Victoria to relabel her as mad (adalan̂a).
One afternoon I was standing in line in the Peasant’s Bank. Suddenly all three bank tellers ducked behind the counter just as a rush of water flew through the air and hit a crowd of people to my right. I spun around and saw a woman in her thirties standing on the veranda. It was my neighbor Victoria, who often suffered from attacks of njarinintsy. She was soaking wet, holding a bucket in the hand of her limp right arm, and she had a faraway stare. I also noticed that she had one black eye. An older woman started to yell at Victoria, telling her to get away from the bank and leave her alone. Instead, Victoria suddenly made another rush for the interior of the bank, threatening the woman with her empty bucket, waving it in her direction as if to pitch more water on her. Two young men escorted the older woman out, and Victoria, after wandering around the bank for a minute or two longer, departed, walking aimlessly, as if drunk, down the main street and past the post office. The three bank employees, giggling nervously, peered out from under the counter and, then, cautiously, stood up and continued their work. When the older woman was out of sight two customers explained to the rest of us in line that the woman whom Victoria was aiming for was her nasty (masiaka) mother-in-law.
Victoria had been plagued by njarinintsy for over a year; as she told me once, “I suffer too much” (Izaho mijaly loatra). She could often be seen wandering through the streets of Ambanja, wailing and crying, and she argued on a daily basis with her spouse and his kin. Within the last three months her fits of possession happened so frequently that some of my neighbors joked that you could tell the time of day by when Victoria would wander by. Others were disturbed by her behavior: as an old schoolteacher of hers sadly explained, these days it was more common to see Victoria in a possessed state than out of one. He and others stated that njarinintsy should not be like that—generally the victim has fits and then she is fine, but Victoria always seemed to be possessed. One of her friends speculated that perhaps Victoria had been sick for so long from njarinintsy possession that it had started to drive her insane (adalan̂a), that she had started to lose her mind (very jery).
All who knew Victoria agreed that her story was very sad (mampalahelo). Victoria was Sakalava from a nearby village. After completing two years of high school she had met her (common law) husband, who was a truck driver for a northern transport company, and she dropped out of school to accompany him to Diégo where he lived. She had been a gifted student and soon found work at a local business as a bookkeeper. Victoria had always hoped to finish her studies at the private French School there, something that her husband had promised he would help her do if she came to live with him. But ten years later and after having had three children, she was still working long hours. She still dreamed of learning more French and studying Italian. Two years ago her husband had lost his job and he had insisted that they return to Ambanja, a town she hated. There had been much tension (and violence) in her marriage during the last four years. This had increased within the past eighteen months, after her husband had learned that she had secretly had an abortion. As a neighbor explained: “Her husband became very angry with her, and he beat her on and off for several days. The noise was terrible!…Two neighbors had to go to the house to stop him.…Now her mother-in-law is angry at her, because she won’t do anything she is told.”
At this point the attacks of njarinintsy began. Her in-laws took her to two healers, but neither succeeded in driving the spirit(s) from her. They then summoned Victoria’s mother and sister, who lived in a village thirty kilometers from Ambanja. As Victoria’s sister later explained, they took her to a series of expensive healers, but all were unable to encourage a spirit of any kind to speak. Even when a kalanoro made all sorts of promises to leave very expensive items at a sacred spot for the spirit to consume, the only signs that Victoria was troubled by spirits were that she would sob uncontrollably and thrash about on the floor during the healing sessions. Her kin had become increasingly worried, because now they were not sure how to cure (mitaha) Victoria. Her mother and sister went home, leaving her in her husband’s care.
Two nights after the episode in the bank Victoria struck again. She had wandered aimlessly into a bar where her husband was drinking with his brother, some friends, and two women reputed to be prostitutes. As the proprietor later explained in disbelief, Victoria had suddenly rushed behind the bar, grabbing bottles of expensive imported whiskey and rum and smashing them on the floor. Her husband jumped up and grabbed her, dragged her out into the street, and then he began to pound her with his fists. His brother and two other men finally stopped him, and Victoria was escorted home. The next day her in-laws again summoned Victoria’s mother and sister, and told them to take her home to their village. By this time everyone who knew Victoria was certain that she was not sick with possession sickness but was insane. Within the week her sister and mother came from their village and, after spending the night, they took her to the provincial hospital in Diégo. I later learned from her sister that Victoria had spent one month in the asylum and that she was now “quite content [tamana] living by herself in Diégo.…She has not suffered from an attack since we brought her there.”
Victoria’s story reveals how kin, as well as members of the community at large, were actively involved in assessing Victoria’s problem and, ultimately, relabeling it as madness rather than possession sickness. Several factors led to this reassessment of her condition. First, her fits were not short-lived, but instead had begun to dominate her life—to see her out of a possessed state had become an unusual event. The level of violent behavior was typical of njarinintsy, but the frequency of her unusual social misconduct led others to believe that it was more than this. Even the most gifted healers of the region could not drive any spirit from her. Furthermore, if she had a spirit, it was odd that it would never talk, even in fragmented speech. The decision to take Victoria to the asylum was one of last resort, only after the efforts of a series of indigenous healers had failed.
The Limitations of Clinical Medicine
As Victoria’s story illustrates, clinical medicine (and, more specifically, psychiatry) provides one option of last resort for extreme cases of possession and madness. The choice to go to the psychiatrist or the exorcist is a personal matter and the actions of patients and their kin reveal no particular trend of favoring one over the other. More often, however, patients leave the asylum for the exorcists, rather than the other way around.
As I have argued elsewhere (Sharp, in press), the efficacy of psychiatric medicine in northern Madagascar is hampered by a multitude of factors. Problems in part result from a reliance on drug therapy in a country where prescribed medications are often unavailable in local pharmacies (cf. Sachs and Tomson 1992; Vogel and Stephens 1989; for contrast see Lee et al. 1991; Silverman, Lee, and Lydecker, 1986; and Silverman, Lydecker, and Lee, 1990). The practice of isolating patients from kin while they are in the asylum also runs contrary to indigenous therapeutic practices.[3] In turn, as others have argued (Zola 1978; see also Dunk 1989; Lock 1984; Ong 1988; Pappas 1990), the medicalization of disorder often empowers the doctor while silencing the patient. To quote Taussig (1980b: 8), this leads to “the alienation of the patient’s self-understanding and capacity” to articulate the causes of her suffering. In Madagascar, a reliance on Western-derived clinical approaches means that the psychiatrist and patient have radically different perceptions of illness. In essence, they suffer from what I have referred to as “conflicting epistemological realities” that block treatment.[4] Clinical medicine denies the legitimacy of the subjective experience of possession.
Ethnic differences between patients and clinicians are also significant. Malagasy doctors working in the north are generally strangers to the region and rarely see possession (or know that a patient is possessed). Several factors account for this: some informants stated that it is taboo (fady) for njarinintsy victims, for example, to receive injections, and mediums are generally reluctant to mention their spirits to doctors for fear of being ostracized. Also, Sakalava—regardless of whether or not they have spirits—generally avoid clinics because they do not want to come into contact with Merina doctors.
As this chapter will show, exorcism is likewise an extreme choice of therapy, yet a few Sakalava opt for it because it offers powerful alternatives for those who have endured great suffering. Even though exorcisms are painful and frustrating for patients, exorcists are successful healers because they first accept and then transform the patient’s explanations for and experiences of possession and madness. During Protestant healing rituals possession is viewed as an appropriate idiom for describing illness, and madness is redefined as normative, not deviant, behavior. Ultimately this approach carries significant implications for the empowerment of both the patient and the healer and it may lead to a permanent transformation of the patient’s identity.
| • | • | • |
Catholic and Muslim Perspectives on Possession
Ambanja, a large town, is a religious center for Catholics, Muslims, and Protestants. To a large extent the membership of these faiths is defined by the ethnic and geographic divisions that exist in Madagascar. The majority of Sakalava belong to no church (tsy mivavaka; “don’t pray”). Those who do are either Catholic or Muslim (the latter is true especially if they are royalty). Rarely are they Protestant—Sakalava generally define themselves in opposition to those other ethnic groups whose members are. Since it is the Protestants who specialize in exorcism in Madagascar, they will be the primary focus of this chapter. Before discussing their activities, however, I will first provide a brief overview of Catholic and Muslim ideas about possession, many of which overlap. In addition, Catholic and Muslim points of view throw into high relief the relative severity or strictness of the Protestant stance.[5]
Catholic Enculturation and Attitudes toward Possession
As a response to enculturation policies, the Catholic church in Ambanja takes a laissez-faire attitude toward possession. Although it does not openly condone tromba possession, it does not prohibit it either, as do the Protestants. Among Ambanja’s Catholics, Sakalava religion is a subject of intellectual interest. During interviews that I conducted with priests and nuns (who were European as well as Sakalava) their collective approach to possession was generally philosophical or theological in nature. They would return my questions by asking: “What is it—is the spirit real, or is it a delusion that people believe in? How do we explain it? Is it psychological? What is its social and cultural significance?” (cf. Estrade 1979). Several Sakalava clergy have written their theses in France on Sakalava religion, with a special emphasis on tromba (see, for example, Jaovelo-Dzao 1983, 1987). Clergy who show an interest in local culture may be invited periodically by Sakalava parishioners to observe tromba ceremonies. Given these attitudes, it is not surprising that the majority of mediums I interviewed over the course of a year were Catholic, and many sent their children to the local mission school. Just after Easter I visited several mediums in their homes where I found palm frond crosses that they had acquired at mass. In several instances Grandchildren spirits identified themselves as Catholic, as were their mediums (although this news of Catholic spirits shocked church officials). As mentioned earlier, mediums sometimes call on the Christian God, Andriamanitra (“The King of Heaven”), rather than using Zanahary, the collective name for ancestors, when they invoke their tromba spirits.
All priests are trained exorcists, but the Catholic church in Ambanja does not offer this service to its parishioners. Instead, the diocese has an official exorcist who lives in a remote town on the east coast of the island. Whereas Protestants view tromba and other spirits as demons and possession as the work of Satan, the Catholic point of view is more compatible with the Sakalava one. As one Italian priest stated, “It is a matter of faith…if a woman comes to me and says that she is troubled by spirits, I encourage her to pray with me, because this seems to help.” In those cases where a parishioner seeks greater assistance from a priest, she may be told to go to the Protestants to be exorcised and then to return to her own church to pray. This is what happened in the case of a woman named Vivienne (see below).
Islam
Muslims in Ambanja are fairly tolerant in their attitudes towards possession. Islamic tolerance is also due, in part, to the fact that in Ambanja men are most active in Islam. Possession is common cross-culturally within the context of Sunni Islam, which recognizes the possibility of possession by jinn (see, for example, Crapanzano 1973, 1977b, 1983; Eikelman 1968; I.M. Lewis 1986, especially chap. 6; I.M. Lewis et al., eds. 1991; Nimtz 1980). Among the Muslims of Ambanja, tromba and other Sakalava spirits are relabeled as such, and are called jiny or devoly (devils, demons).[6] Although all mosques in town have an area or separate building set aside where women may pray, ordinarily no more than ten women attend on a regular basis, and so few members would be mediums. It is not unusual for Muslim men, who are active at themosque, to have spouses who are not Muslim or who are observant only during Ramadan (Ramzan). Some Muslim men have wives who are tromba mediums, and many Muslims consult mediums, moasy, and other indigenous healers when they are ill. Muslims in Ambanja also have their own specialists called badry (so named after the text they use and the ritual they perform), whose healing powers are derived from books written in Arabic.[7] In Ambanja, exorcisms are occasionally held at mosques to drive out spirits from the possessed, but more often adherents see no conflict between possession activities and Islam. The few who seek to have jiny exorcised tend to be men and not women. In such cases it is the priest or fondy (also referred to sometimes as the mwalimo, from the kiSwahili word mwalimu) who performs the exorcism. This generally involves the burning of incense and group prayer at the mosque.
The one exception is a reformist group that I will refer to as Modern Islam. Modern Islam was formed in 1979 by members drawn from an assortment of mosques who found the attitudes of Muslims in town to be too lenient—and syncretic—for their tastes. Members of this group view themselves as more literary and “pure” in their approach to Islam. They stress the necessity of learning how to read and write Arabic (most members of other mosques learn prayer strictly through memorization). Also, more recently, Modern Islam has sought to impose greater restrictions on women by introducing the veil and purdah. So far this has been met with great resistance from local women, so that the female membership of this group lags far behind that of men (there are approximately ten women to sixty or seventy men). Modern Islam also stresses the need to be “scientific.” Its leaders are vehemently opposed to the work of moasy, tromba mediums, and other indigenous healers. If njarinintsy possession is suspected, for example, the afflicted is instructed to go to the hospital first to make sure that her shaking is not caused, perhaps, by malaria. As one member put it, “If it is truly possession, we believe that it is the work of the devil; we are like Christians in this respect.”
Leaders of Modern Islam are able to perform exorcisms, but as of 1987 only one possession case had ever been treated. This involved a tromba medium named Berthine (see Appendix A) who chose to convert because her new husband was a Muslim; it was necessary to rid her of her spirit before she could join. The exorcism involved the following steps. First, she had to break the tromba’s taboos (fady). Second, all of the spirit’s paraphernalia were burned in the mosque. Third, she was asked to pray with others in the mosque. When the tromba spirit cried out, the Koran was placed on her head and the spirit was driven out of her through prayer, as if it were a jiny. Afterward, she was instructed to pray for five days, five times a day. As will be clear from the discussion below, these rituals parallel those that occur during Protestant exorcisms.
| • | • | • |
The Fifohazana or Protestant Exorcists
Nearly all Protestant sects in Madagascar conduct exorcisms. Some have special curing retreats where exorcists work full-time; two of the mostactive groups are the Lutherans and the FJKM.[8] The exorcist movement and its associated specialists are referred to as fifohazana (HP: “awakening,” “revival”; from the verb mifoha, “to wake,” “to arise”); they are also called mpiandry (HP: “shepherds”). Since I am specifically interested in those activities that are related to spirit possession, I will refer to them here as exorcists. Satan (Satany) and devils (devoly) are thought to cause misfortune, and so the exorcist’s goal is to drive spirits out of the bodies of their victims. In general terms, individuals usually fall ill because they have no faith in Jesus (Jesosy).
Exorcists have received special training as healers and they form a special branch of their respectives churches. The majority are Malagasy, and they include pastors, evangelists, and parishioners. They are male and female, and they come from a wide variety of backgrounds, including peasants and educated professionals. Ethnic affiliation reflects the geographical distribution of Protestant missionary activities throughout the island: typically they are Merina and Betsileo from the highlands. There are also Antandroy, Antaisaka, and Antaimoro from the south and southeast and Tsimihety from the west and north. Rarely are they Sakalava or Antakarana. In Ambanja, several churches hold exorcism ceremonies on a regular basis. The FJKM church, which is by far the largest Protestant church in town, is most actively involved in this, and has more than a dozen trained specialists. Others include the Lutheran church and a small Pentecostal group that calls itself the Fifohazana Church, which broke off from the FJKM over a decade ago.
Exorcists gain inspiration and guidance from prophets, and each church has its own. According to FJKM records, the fifohazana movement was started in the 1880s by a Betsileo man from the high plateaux named Rainisoalambo. He was a diviner (mpisikidy) who suffered from severe and incurable skin problems. He had a dream in which he was told to go to the church, and so the next day he threw away his medicines (fanafody-gasy) and went there with his children. Eventually he built his own church in Soatanana, near Fianarantsoa, where he began to heal others. Soatanana is now a major center for fifohazana training and healing activities for numerous churches (Anonymous 1962; Rasamoela 1975; Trexler 1989). Although each church has its own prophets, the Lutherans pride themselves on having the only living prophet, who is named Nenilava (“Tall Mother”). Nenilava is Antaimoro and is the daughter of an herbalist (HP: ombiasy) who converted to Lutheranism when she was young. Her visions and wisdom concerning the teachings of Christ make her a central figure in her church (cf. Trexler 1989).
The style of dress and methods of healing are fairly standard among different Protestant groups. The clothes they wear during exorcism sessions reflect a blending of Calvinist dress of more than a hundred years ago, combined with high plateaux styles (see plate 8 and the last two photos in Estrade 1977). Exorcists always dress in white and keep their bodies well covered. Men generally wear long-sleeved shirts and long pants, and women wear long-sleeved blouses and ankle-length skirts. Both men and women sometimes wear long white robes that have puffy sleeves and dog-eared collars that are tied close to the throat. Some also wear bulky white shawls, reminiscent of the lamba worn by Merina. Many wear a wimple, wrapping a white cloth around their foreheads and then tying it at the back of the head. These clothes may be worn every day like a uniform or only during healing sessions. The quality and elaborateness of clothing often reflect the amount of church treasury funds available for exorcism activities.
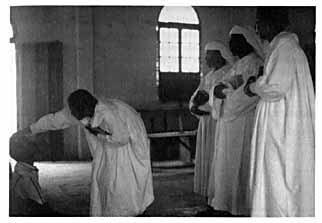
8. Fifohazana exorcist driving spirits out of a patient while others watch and wait their turns. Note that the exorcist has placed her hand on the patient’s head.
The role of an exorcist can be a part- or full-time occupation. Some exorcists assist only during healing sessions that occur on Sundays after regular services, while for others it is a way of life, such as those who live in healing retreats (see below). The majority became exorcists after they or someone close to them was healed. Exorcists treat all forms of illness, including physical ailments such as blindness, headaches, lameness, troubled thoughts, restlessness, madness, and possession. Satan and devils cause illness and suffering, and the exorcist heals by driving them out of their victims through the laying on of hands (HP: fametra-han-tànana) and through prayer (vavaka). The exorcist’s strength and power are derived from the Holy Ghost (ny FanahyMasina) and for this reason Lutherans refer to exorcisms as asa sy fampaheresana (“work and empowerment”). Exorcists prefer to work in groups of three, reflecting the power of the trinity. Groups of other sizes are acceptable, but exorcists avoid working alone. As one put it, “When you work alone you may think that the power is in you, forgetting that it is derived from the Holy Spirit…if you are too proud you might fail in your work.” Exorcisms occur frequently in Ambanja: throughout 1987 I witnessed approximately a dozen, and I heard of more than twenty others. Five of the sessions I witnessed took place at the Lutheran church where I lived, where one of the pastors was trained as an exorcist.
The purpose of these healing sessions is to cure specific ills as well as to ensure general well-being in the congregation. Some churches schedule sessions on a regular basis, such as on the first Sunday of each month. Private, intensive sessions can be arranged for those who suffer from serious problems. Exorcists may apply their powers at home as well, treating themselves and members of their households, or they may be called into a patient’s home to work. Some patients come on their own, but most often they are accompanied by kin. The majority of patients are adolescent girls who are plagued by njarinintsy and other forms of possession sickness; older women (thirty or older) who wish to rid themselves of tromba spirits; and those whom kin label as mentally ill (adala). Serious problems can not be cured in one session but require a number of visits to ensure that the spirit(s) has left permanently. If the patient is not a Protestant she or he is also expected to convert and become a regular member of the church.
Exorcism as Therapy
Exorcism sessions are electrifying events that are exhausting for both exorcist and patient, and they can be frightening for young children and for the uninitiated. During these sessions a patient’s kin may also be present, as may parishioners, who have been encouraged to attend so that they may assist by praying and singing. Parishioner participation is necessary for several reasons. First, prayers and hymns are imbued with the power of the Word of God. Second, spirits enjoy music and so hymns help to draw them out of their victims. Third, by participating in these sessions parishioners are witnesses of God’s work.
Exorcisms have several stages. If the exorcists are not in their robes, they will don the proper attire before they begin (often this is done with great ceremony at the front of the church). All church services open with the singing of hymns, and this is also true for exorcisms. The session then proceeds with readings from the Bible and most often these include the following passages:[9]
Then he said to them: ‘Go forth to every part of the world, and proclaim the Good News to the whole creation. Those who believe it and receive baptism will find salvation; those who do not believe will be condemned. Faith will bring with it these miracles: believers will cast out devils in my name and speak in strange tongues; if they handle snakes or drink any deadly poison, they will come to no harm; and the sick on whom they lay their hands will recover.’
[10][Ary hoy Izy taminy: Mandehana any amin’izao tontolo izao hianareo, ka mitoria ny filazantsara amin’ny olombelona rehetra. Izay mino sy atao batisa no hovonjena; fa izay tsy mety mino no hohelohina. Ary izao famantarana izao no hanaraka izay mino: hamoaka demonia amin’ny anarako izy; hiteny amin’ny fiteny izay tsy mbola hainy izy; handray menarana izy; ary na dia misotro zava-mahafaty aza izy, dia tsy hampaninona azy izany; hametra-tànana amin’ny marary izy, dia ho sitrana ireny.]
Jesus repeated, ‘Peace be with you!’, and said, ‘As the Father sent me, so I send you.’ Then he breathed on them, saying, ‘Receive the Holy Spirit! If you forgive any man’s sins, they stand forgiven; if you pronounce them unforgiven, unforgiven they remain’
[Ary hoy indray Jesosy taminy: Fiadanana ho anareo; tahaka ny nanirahan’ny Ray Ahy no anirahako anareo kosa. Ary rehefa nilaza izany Izy, dia nanisy fofonaina, ka hoy Izy taminy: Raiso ny Fanahy Masina; na helok’iza na helok’iza no avelanareo, dia voavela izany; ary na an’iza na an’iza kosa no tsy avelanareo, dia tsy voavela izany.]
In addition to these passages, which speak of the laying on of hands and the healing powers of God, exorcists may read others that refer specifically to the problems of those who have come to be cured. These people are asked to form small groups at the front of the church and sit on the ground on a mat. Amid the singing, the exorcists lay their hands upon the heads of these people and pray quietly for their health and well-being. Patients with more serious problems are then called before the congregation and are healed separately.
The tenor of sessions directed at helping more serious cases is very different, especially when possession is the cause of the problem. During sessions for tromba possession, for example, the spirit is first reidentified as a demon or as Satan. The spirit must be encouraged to come forth so that it may then be driven from the body of its victim. These actions echo and draw from those of a tromba ceremony, where the spirit arrives by possessing the medium, announces its name, and converses with the audience. An exorcism, however, it not a joyful event but a frightening and volatile one because the spirit is quickly angered when confronted by the exorcists. If there are several exorcists present, they divide into groups (preferably into threes) and they work together with each patient; periodically they change places, rotating from one patient to another. In this way the intensity of the healing power directed at each person is great and is varied. As parishioners sing, the exorcists shout at the spirits in the imperative voice, a form that in most cases is used in Malagasy only to address naughty children, animals,[11] and demons: “Voka!” (“Get out!”), “Mivoka amin’ny ianarana Jesosy!” (“Get out in the name of Jesus!”).
As the exorcism progresses, the language becomes more powerful and the volume increases as exorcists shout their orders and parishioners sing louder and more intensely. This is usually when the spirit arrives. If it is a tromba, curses may suddenly issue forth from the mouth of the patient; if it is a njarinintsy, the victim will start to wail loudly, scream, and sob. Possessed patients usually collapse periodically on the ground, at which point the exorcist orders them to “get up!”(mifoha!). The exorcist speaks directly to the spirit, encouraging it to engage in a dialogue. He asks, “Who are you!? Why have you possessed this person!? What do you want?” and, in hearing the answers, he shouts back again, “Get out! get out you devil!” (Voka! Voka devoly!) or “Go back to the desert from whence you came!” (Handeha amin’ny tany karakaina!). These sessions can be violent, not only because the patient may fall or thrash about but because the exorcist, in wrestling with the spirit, may push at or tug on the patient’s body. Sometimes an exorcist repeatedly pushes a patient to the ground and then orders the patient to “get up! Rise up in the name of Jesus!”[12]
Eventually, the wailing will stop and the patient will regain consciousness, feeling exhausted. The hymns become quieter, and the session will end with a prayer to bless all who are present. This session will be followed by at least one more session, generally later that week, to ensure that the spirit has departed permanently. One unusual case that I witnessed involved three members of an Antandroy family (mother, father, and thirteen-year-old son). It was the mother who originally requested to have a tromba exorcised, but soon it was clear that the father, too, had a bilo spirit. Each time the father’s spirit was driven from him it would then move into the body of his wife or son, so that each person in turn had to have this spirit exorcised. This required several weeks of intensive work, involving six exorcists who worked with the patients two or three times each week.
Following these healing sessions, the exorcists, pastor, or congregation members visit patients in their homes to make sure they are well. If a patient had a tromba spirit, she will be instructed to bring all of the spirit’s paraphernalia to the church, so that it can be burned or otherwise destroyed. Patients are also expected to return to the church for Bible study and prayer and they are encouraged to join the church as permanent members.
Being an exorcist is difficult and involves great dedication. As one confided:
One of the problems in being an [exorcist] is that people here [in Ambanja] think I’m like a moasy [herbalist]—they want to be able to come just once, be cured, and leave. Maybe they think I am more powerful than most moasy but, still, I am the same to them. If they ask me to come to their house to help them, I always ask them if they use fanafody…that is our [the fifohazana’s] way. They may say no, but sometimes I think they are hiding that they do use it, because they are afraid to say yes. For us, we are not like the moasy, because we expect the person to become a member of the church,to choose to be Christian. It is no good if I come and exorcise them and then I don’t see them again.…I think some people think, “he is an exorcist, so why don’t we have him come and see what happens?”…One time a well-known woman here in town…had me come to her house.…I think her husband had a tromba [spirit], or maybe he is a little crazy [adala]?—but I am not sure. His wife had me come exorcise him—and I gave him a book to study, but they didn’t come to the church.…Being an exorcist is difficult—people will come to you at any time—sometimes in the middle of the night—because they are afraid and they ask if they can sleep here in our house. We take them in, we share their problems.…I am not as strong as they think I am, I have my faults, I sin, too, sometimes. But this is why I have chosen to be an [exorcist].
The Protestant Toby (Camps) or Curing Retreats
Several Protestant churches have centers for faith healing which are called toby (HP, lit. “camp”) and which I will refer to as “curing retreats.” The Lutherans are most famous for this, having established a large retreat in the high plateaux near Fianarantsoa. The mother church, which is located in a suburb of Antananarivo, also hosts regular healing sessions. In 1987 a new retreat was being built in the outskirts of this city so that there would be a second hospital that was more centrally located on the island. Many patients come to the Lutherans seeking the guidance of the Prophet Nenilava, who moves back and forth between the two centers. Smaller, usually rural retreats, can be found throughout the island.
Exorcists and their patients live full-time at these curing retreats. Primary curing activities involve the laying on of hands and intensive prayer sessions. Sometimes the kin of seriously ill patients will come and request that the exorcists accompany them home. A group of them (preferably three) will join the household temporarily to watch over and heal the sick person, and room and board is provided as payment for their services. Because the bonds that develop between the exorcists and the patient’s kin can be strong, sometimes an exorcist later marries someone from the patient’s household.
In northwest Madagascar, near Ambanja, there are three FJKM curing retreats. The closest was established in 1986 and lies eight kilometers from the town (and one kilometer off the main road). The work of these Protestant exorcists tends to be ecumenical in nature, reflected by the fact that although all those living at the retreat are members of the FJKM church, the deacon (HP: iraka), who moves between the threeretreats, is Anglican, as is the Antaimoro planter who donated the land. The FJKM church also has sought to combine efforts with other churches in order to establish an additional center in Ambanja.
The retreat near Ambanja occupies one-third of a small village, which has a total population of approximately two hundred people. It consists of a large open area about the size of a soccer field, surrounded by numerous structures, including an outdoor kitchen and shaded eating space; an unfinished (roofless) church; a long rectangular building that has four apartments in which the exorcists live; and three small, two-room houses that are for patients and their kin. The church is constructed of concrete. All other buildings are modest structures made from traveler’s palm.
Eight adult exorcists (four men and four women, including two married couples), and about a dozen children are the retreat’s full-time residents. At any given time there are three to five patients living there who are usually accompanied by one or two of their kin (such as parents, spouses, or siblings). The exorcists are Tsimehety, Betsileo, and Antaimoro, whereas the majority of the villagers are Sakalava as well as Antaimoro settlers. Patients are of diverse backgrounds and include fairly equal proportions of tera-tany and vahiny: when I visited in April 1987, they were Sakalava, Antakarana, and Tsimehety from the north; Comorean; and Antaimoro migrants from the south. Flanking the settlement on one side are fields, where the exorcists grow manioc, rice, maize, and greens. On the other are the villagers’ dwellings, a Catholic church, a schoolhouse, and a playing field.
Like the majority of their patients, exorcists are poor, yet therapy itself is free and thus practical, since they rely on the power of the Holy Spirit to heal. Exorcists live solely off donations and the bit of food they can eke out of the land. As is true for hospital care throughout Madagascar (and elsewhere in the Third World) patients are expected to cover all of their own expenses, so kin accompany them to make sure they have clean clothing and food to eat. The cost of a long-term stay at the retreat can create serious hardships. Such was the case for an elderly Antakarana couple who had been living at the retreat for six months so that their son could be treated for madness. As the father explained:
Here it is very hard for us, we have five other children…two, who live nearby, come to visit and bring us rice when they can. Here rice is very expensive, half again as much as it is in the market in Ambanja. I must work in other people’s coffee and cocoa fields for money, and my wife helps othersin their houses. We always need money to buy rice and other food, nivaquine [for malaria] and aspirin. Since there is no car that goes to Ambanja, it is very hard for us to travel to and from this village. We are not sure how much longer we can stay.
Most patients who come to this retreat are adults. They suffer from an assortment of problems. The majority (male and female) are mentally ill. The second largest group consists of single women who are suffering from tromba and other forms of possession. There are also those who are crippled (kalemy) and, finally, those with more general ailments, the most common being skin problems. When I visited the retreat outside Ambanja in April 1987, there were five patients there: two Sakalava women who suffered from tromba possession; a young Antaimoro boy, about age ten, who appeared to be mentally handicapped (as one exorcist said, “When he first came here he didn’t even know how to use silverware”); a Comorean man in his late thirties who was diagnosed as mentally ill (marary saina), who sat and talked to himself; and the young Antakarana man whose father is quoted above and who was also said to be mad. The majority of patients who come here have previously sought help from indigenous healers but found no cure. Some patients may stay for months, while others have remained for years.
Each exorcist is responsible for several patients, who in turn have three exorcists assigned to them. The treatments they administer take several forms. First, everyone is expected to pray (mivavaka) three times a day, since prayer weakens Satan. Second, laying on of hands (fametrahan-tànana) occurs twice a week. The notion of community is constantly stressed, and thus fictive kinship is a key defining principle for social relations among exorcists and patients. The pastor and deacon are referred to as “father” (papa or baba), and exorcists refer to each other as siblings, expecting patients and their kin to address them in this manner as well.[13] There is also a strong emphasis placed on the importance of work, and so patients labor in the kitchen, fields, and elsewhere according to their individual abilities and strengths. When one Sakalava villager was asked to describe the exorcists, she said “they work very, very hard” (miasa mafibe izy).
Three times a year the FJKM fifohazana exorcists hold reunions, and the location rotates between the three curing retreats in the northwest. One of my assistants went to observe a reunion during Pentecost, which lasted for two days. Much time was spent praying and singing hymns or working in the compound, and a communal feast was held wheremeat was served. This meal was a great luxury that the exorcists at this retreat could ill afford: since they receive little if any money from the mother church, their daily diet generally consists of a meager dish of boiled manioc and bananas, often with no rice. In all, 695 people attended. This official head count included the ten patients and their kin. The patients consisted of the five currently in residence at this retreat, plus five others who came from the two other retreats. These patients included three women who were suffering from tromba possession (see accounts of Vivienne, below, and Mona, who appears later in this chapter; also Appendix A); two men who were mentally ill (marary saina); and a woman with a child who had a severe case of diarrhea. The other participants consisted of seventy exorcists, other novices training to be exorcists, and congregation members, including those who had come for first communion.
Throughout the night the exorcists healed through the laying on of hands. Participants were split into two groups, so that the majority stayed outside while the ten patients were taken to be healed separately inside one of the houses. As one exorcist explained to my assistant, this was done because healing sessions can be upsetting to watch, since sometimes Satan can make patients act violently.
Seeking Cures for Possession: Three Case Studies
The stories that appear below all concern extreme cases. The first involves a woman who, like Victoria, suffered from problems that shifted between possession sickness and madness. The other two are women who refused to accept tromba mediumship as a permanent manifestation of their lives. Although all three of these patients are Sakalava, they each took a radical step in the therapeutic process, seeking assistance from non-Sakalava Protestants for their problems. Two of these women have chosen to convert, thus abandoning Sakalava culture for a new religious system.
Vivienne
Vivienne is from a family where many of the women are tromba mediums. Her older classificatory sister is an established medium who receives many clients in her home and who was one of my key informants (see Alice in Appendix A). Another classificatory sister is Berthine … (see above) who had her spirit exorcised by members of Modern Islam.
Vivienne is the daughter of a Sakalava mother and Tsimihety father. She is fifteen years old and she attends junior high school to the north in Ambilobe. She was raised by her mother, who was Catholic and who died when Vivienne was twelve. Her father lives in Diégo. Following her mother’s death he arranged for Vivienne to live with his brother and his brother’s wife, who are both members of the FJKM church. Throughout the summer Vivienne has been living with her aunt (MoSi) in Ambanja. Although her aunt is not Christian, she decided to bring Vivienne to the Pentecostal retreat that my assistant attended.
For one year Vivienne has been very sick, troubled by a njarinintsy spirit. As her aunt explained: “Sometime she is crazy [adala izy é]!…If I ask her to set the table, she puts spoons under the tablecloth; at other times she cooks with hair!…She swears [vetaveta] and she has tried to hit her uncle! Now she lives with me.…Sometimes she cries and laughs suddenly—this even happened when she was at school! I took her to the Catholic priest and he told me to take her to the Lutherans [around the corner]. We went there one Sunday, but nothing happened. So then I took her to the FJKM church. Her father’s relatives want her to come and stay here [at the retreat], but Vivienne refuses, saying that she is Catholic and that she has no intention of changing her religion.”
Vivienne and her aunt later returned to the retreat, where they lived for four weeks. Here Vivienne took part in healing and prayer sessions several times each day. After two weeks she felt stronger (hery) (and, as her aunt and the exorcists noted, she had also become more cooperative) and she started to work in the fields. Three months later she returned to school. Vivienne occasionally attends Sunday services at the FJKM church. When her Sakalava friends tease her about this, she states flatly that she goes for her health and she insists that she has not converted.
I later asked one of the Lutheran exorcists about Vivienne, who stressed that, in his opinion, she was not possessed, but was mad (marary saina):
She doesn’t look at you when you talk, but she gazes around and talks to herself. That is not like someone with njarinintsy. I remember I asked her if there was anything troubling her and she said yes, that there was a boy who had tried to harm her with fanafody—he pretended that he loved her and sweet talked her, but she later realized he didn’t care about her at all. This is so common!…With these young girls it is always a problem with a boy. I told her to forget about it, that there were better ones out there. I tried to heal her and to help her, stressing that she must come back with her family—I am not a doctor, I can not cure someone in just one session! But she never came back. I think that she must have gone to the FJKM church because she has relatives who pray there. This is better, because her kin will be there with her and, besides, their work is the same as mine. They know how to heal the same way as I do.
Elisabeth
Elisabeth is forty-two years old and the daughter of Sakalava parents. She was raised in a small village northwest of Ambanja. When she was very young (five years old) she had already begun to show signs of tromba possession, and by the age of seven her parents had held a ceremony to instate a fairly powerful Child spirit within her. Neighbors were skeptical of this development, finding it difficult to believe that a girl so young could have a tromba spirit; nevertheless, she soon had clients who came from other villages and towns seeking her spirit’s advice. By the age of fifteen she had two other spirits, a Child and a Zafin’i’fotsy Grandparent.[14] As Elisabeth put it, mediumship was a very difficult (sarotra be) experience. For much of her childhood she fell sick periodically, suffering from chronic weakness, dizziness and fainting spells, terrible headaches, and frequent nightmares.
At age seventeen Elisabeth convinced her parents to let her go live with her sister in Ambanja. She had previously visited the town on many occasions, preferring it to the sleepy village in which she grew up. In Ambanja she took her first lover who eventually became a common-law spouse. This relationship lasted for three years. She later met her husband, Claude, with whom she lived on and off for twelve years. Eventually she grew tired of this relationship. As she put it, all Claude wanted was the money she earned as a medium. As in her childhood, she frequently fell ill and sometimes was unable to get out of bed for weeks at a time. This made it extremely difficult for her to carry water, go to market, or care for her two children, especially when her husband was not with her. Twice spirit mediums had diagnosed her tromba spirits as the cause, and by the age of thirty-five she had held the appropriate ceremonies to have two additional spirits instated. Each time her health only improved temporarily. She also spent much time and money seeking help from other local healers and doctors, all to no avail. Repeatedly she was told by friends and kin that her spirits were responsible for her bouts of illness, and she had become frustrated nearly to the point of panic. Unable to earn enough money to host additional ceremonies to appease her spirits, her health only worsened.
In 1984, Elisabeth’s sister took her on the ferry to the nearby island of Nosy Be, where they sought out the Protestant exorcists at the FJKM church there. After several weeks of intense healing sessions (three times a week for four weeks), Elisabeth was finally freed from her spirits. Like the majority of mediums, she did not recall what took place during these interactions between her spirits and the exorcists, but she described the process as frightening and exhausting (mavozo aho,kajobe aho), followed by a sense of elation after each session. She has since converted to this church, and is now among their most highly respected exorcists. She lives in Nosy Be, two blocks from the pastor’s house. She has not, however, visited with her kin since this time. Only her sister comes to see her, since others, especially her parents, are ashamed that Elisabeth keeps the company of Merina Protestants.
Zaloky
Zaloky is approximately fifty years old (although, as described in chapter 2, she is easily mistaken for a woman who is much older). Zaloky’s life as a medium is fairly typical for older Sakalava tera-tany women. She wasmarried at age sixteen and, at age thirty-two, after the births of three of her four children, she became possessed by the transitional Child spirit Zaman’i’Bao(see chapter 5). Within two years she had become a respected healer in the area and she had a steady flow of clients. At age thirty-five her husband died. She describes the next five years as difficult and bitter ones because of struggles with her children over land rights (again, see her story in chapter 2). She eventually married (by common law) her second husband Marcel, a Tsimihety migrant laborer who had been a regular client of hers when seeking guidance from Zaman’i’Bao for problems related to work or physical ailments.
Zaloky describes her past activities as a medium as very difficult: “Zaman’i’Bao is a very powerful spirit, and his mediums must be strong [mahery]. It was a difficult life: I had many [clients]! too many! [bemaro! beloatra!]…they would come whenever they wanted, it didn’t matter how I was feeling.…You know, Zaman’i’Bao, he is hard on his mediums, he spits up blood.…Some days I would not be able to get up after a session [with a client]…my back and neck would be so sore; one day I saw black spots for three days! It was terrible…when a tromba spirit gets angry, he makes you sick.…I didn’t have the money to host a ceremony to make him happy, and this really frightened me. I wondered, is he going to kill me?…Marcel, who had gone to the FJKM church as a child, told me to go there to have the spirit driven out, but I didn’t want to. I was so afraid! [mavozo é!]. We live near the newly built Lutheran church, and my spirit didn’t like that either. They would start to sing and I could hear them in my house. I’d get scared, because sometimes Zaman’i’Bao would arrive suddenly and be very angry, especially when they sang the hymn “Jesosy Tomponay” [“Jesus our Master”].…Then one day I just wandered into the church, [possessed by] the tromba [spirit]! Can you imagine! I don’t remember what happened, but Marcel and the pastor say they stopped the service right there and drove out the spirit.…that was ten years ago.…Now Marcel and I pray there every week.…They take care of me; they are my family [HP: fianakaviana].” Zaloky is now a respected elder in the church. She and Marcel have fallen into economic hardship within the last few years and they continue to be troubled by land disputes with her children. The Lutherans give them food and she in turn has decided to will her land to this church (unless a disco next door overruns her homestead first).
Vivienne, Elisabeth, and Zaloky have each suffered from a form of possession which is fairly typical for Sakalava women their respective ages. Vivienne is an adolescent troubled by problems of love and romance, and she suffers from njarinintsy possession. Elisabeth and Zaloky were established mediums for Child and Grandparent spirits that commonly appear among women of their backgrounds and ages. All three are also unusual, however, and even marginal, in other ways. Vivienne’s problems with possession are extreme, now bordering on madness. Elisabeth’s career as a medium began at an exceptionally early age. Rather than accepting her fate, she has suffered terribly throughout her life, unable to cope with her status as a spirit medium. Regardless of her actions, she continued to be plagued by illnesses caused by her tromba spirits. For Zaloky, an older woman, the more mundane forms of suffering associated with mediumship eventually were intolerable. Although she had many clients, trance exhausted her and she found demands of visitors to her house to be too great. This was compounded by the terrible conflicts with her children over land rights.
These three women present extreme cases for yet another reason: although they are tera-tany, they eventually sought solutions through a nonindigenous institution dominated by peoples from the high plateaux. In the case of Vivienne, the Protestant exorcists may be able to help her through a serious illness—whether it is possession sickness or madness—coaxing it to leave and then giving her continued support. Elisabeth and Zaloky, on the other hand, are women who have rejected the role of tromba medium, choosing instead to be freed permanently from possession. They have come to the exorcists hoping to have their spirits driven from them because they find the suffering they experience as mediums unbearable. This is a pattern that has emerged in the Lutheran church, where, in addition to Zaloky, two other Sakalava have joined for reasons associated with tromba. The first is an old man (in his sixties) who, like Zaloky, had a tromba spirit exorcised and who later joined the congregation. He and Zaloky felt their ties to the local community were fragmented: Zaloky was embroiled in a bitter quarrel with her children over land inheritance, and this older man was unmarried and had no children. Another Sakalava convert was a twenty-year-old man who joined because he was deeply distressed by the suffering that he saw his mother and ex-wife endure as tromba mediums.
Seeking the assistance of the exorcists reflects a deliberate choice to opt out of and thus be free from the institution of spirit possession, which in many ways epitomizes what it means to be Sakalava. This involves embracing, at least in part, Protestantism as a new faith, either by drawing on the power of the exorcists for convenience’s sake to drive out unwanted tromba spirits, or through the more permanent act of conversion. In choosing this route, however, one becomes, in a sense, less Sakalava, not only because one rejects tromba, but also because Sakalava look disfavorably upon Protestant vahiny. As the stories of these three women show, this choice may also mark a shift away from kin and Sakalava identity: two of these former mediums have chosen to become members of new Christian communities that in many ways are like newly found kin.
| • | • | • |
The Power of Protestant Healing
Exorcists’ clients are drawn from a variety of backgrounds; one thing that they all share in common is that they are desperate. Other healers—indigenous and clinical—have failed to relieve their suffering. Their distress may be compounded by their marginality within the local Sakalava community. Pertinent factors here include understanding the following: the manner in which practitioners of this alternative healing system cope with a competing epistemological reality derived from Sakalava culture, the significance of power in the therapeutic context, the relevance of structural shifts in identity, and the meaning of community.
Redefining the Symbolic Order through an Alternative Epistemological System
As I have argued elsewhere (Sharp, in press), understanding the therapeutic efficacy of Malagasy exorcists is a difficult task. Csordas, in his work with charismatic Christians in the United States, stresses that efficacy and outcome hinges on an assessment of procedures (such as rituals) used by therapists as well as the process (or experiences) undergone by patients. Anthropologists need to have a clearer understanding of patients’ subjective experiences of “encounters with the sacred, episodes of insight, or changes in thought, emotion, attitude, meaning, behavior” (1988: 121). An analysis of exorcists in Madagascar reveals the relevance of their approaches and epistemological model to therapeutics. A key aspect here is that exorcists use invasive conversionary tactics that require the active participation of the patient and, if possible, her kin. Through this process the meaning of suffering is transformed and often, in turn, the patient’s definition of self is also altered.
Patient and healer may have radically different perceptions of illness and personal disorder. As Taussig (1980b) has argued, medical care may serve as a method to silence the patient rather than one through which to communicate with and comprehend her perceptions of her illness. In northwest Madagascar, ultimately therapeutic success or failure hinges on the healer’s ability to comprehend the patient’s epistemological reality. To rely on the knowledge of indigenous healers to solve problems associated with possession and madness means to embrace the logic of the cultural system from which they originate. For example, established mediums typically specialize in tromba possession because they grasp the deep-rooted internal cultural logic that shapes the significance of royal ancestors and the nature of their needs and whims (cf. Lévi-Strauss 1963a). For the exorcist, on the other hand, an oppositional stance to this internal logic is central, since conversion is the ultimate goal. Paradoxically, to achieve this goal, the sharing of ideas must be part of the process. The exorcist helps the patient by redefining her conception of reality (and, ultimately, her identity). The patient, in turn, must embrace the Protestant belief system to be fully healed.
This is a dialogic process, one that is clearly evident in cases involving possession. Ironically, exorcists do not deny the existence of spirits; rather, they refuse to distinguish between different categories, relabeling all spirits (tromba, kalanoro, njarinintsy, and so forth) as demons (devoly). As Greenfield (1992) illustrates, the strength of a group of Spiritist healers in southern Brazil lies in the syncretic nature of their healing practices. They rely on an assortment of models of illness causation, including the teachings of the spiritist Allan Kardec, modern physics, and Candomblé, Umbanda, and other Afro-Brazilian religions. Their work attracts clients because their ideas make sense to people of diverse origins who populate the polycultural, urban world of Brazil. Protestant exorcists in Madagascar are not nearly so liberal (or eclectic) in their approaches. Nevertheless, within the therapeutic context there is still a sharing and overlapping of information between Sakalava and Christian systems. Exorcists would never, for example, draw on the power of a tromba spirit to heal, yet they do rely on a form of possession involving the Holy Spirit to achieve a similar end. In addition, the exorcist’s approach is participatory, designed to engage the patient in a continuous dialogue about her life and the meaning of spirits for her. Prayers, hymns, and sermons serve as didactic tools to transform the patient’s way of perceiving her illness as well as the world more generally.
In contrast to the tolerance of Catholic enculturation policies, Protestant churches in Madagascar have always made conscious and deliberate attempts to define their doctrines in reference—and opposition—to indigenous beliefs (fomba-gasy) (Gow 1979; Mutibwa 1974; Trexler 1989; see also entries authored by Sibree, Pearse, Dahle, Haile, Davidson, and others in the journal of the London Missionary Society [LMS] 1881–1900). As zealous evangelists, the ultimate goal of these exorcists is to undermine a patient’s beliefs by simultaneously acknowledging their legitimacy. In reference specifically to tromba possession, they accept the pervasiveness of these spirits’ taboos (fady), and then, in turn, they declare that “tromba [itself] is taboo” (fady tromba), an expression that operates like other fady in Madagascar to mark difference, distinguishing ethnic groups from one another.
The power of communication is central to the act of exorcism, especially when exorcists engage the spirits themselves. Just as an accordionist or valiha player entices tromba spirits to arrive in their mediums, Protestant healers use their own music to encourage the spirits to possess patients. Their style of interaction with these spirits parallels that of tromba mediums, or other indigenous healers, who seek to placate or cajole a spirit into staying (in the case of a tromba) or departing peacefully (as with a njarinintsy). Exorcists, however, take this one step further: they taunt, scold, and lecture spirits and then they drive them, with force, from their victims. Exorcists fully comprehend the meaning of possession in the lives of their patients, and they seek to alter their ways of perceiving their experiences. Thus, on the one hand, exorcists successfully integrate two seemingly divergent or conflicting epistemologies. On the other, through conversionary tactics, they undermine indigenous cultural logic.
Work, Independence, and Empowerment
Protestants draw on the indigenous symbolic order in other ways to heal as well as transform the patient’s sense of the world. For example, they supply new meanings for the concept of work (asa). As described in previous chapters, ideas surrounding work are highly charged for the Sakalava, whose lives are shaped by the plantation economy of the Sambirano. Preferably, work should be framed by economic independence involving such activities as caring for one’s own fields. If one works to serve another, this should only be done for Sakalava royalty, and not in the sense that characterizes the enterprises, where work means alienated wage labor.
In the healing retreats of the northwest, a new Protestant work ethic has emerged (cf. Weber 1991 [1930]; see also Comaroff and Comaroff 1991: 140ff). When patients have the strength, they are expected to assist with daily chores, cooking in the kitchen, cleaning the church and other structures, and assisting in the fields. Such participation serves to integrate them into daily community life. It also stresses the duty that one has to serve God, the master of us all, a concept aptly expressed in the hymn mentioned by Zaloky, “Jesosy Tomponay,” or “Jesus our Master.” Women who have abandoned mediumship continue to perform sacred work, but for a Christian deity rather than for royal ancestors.
The significance of work carries over into other exorcist activities, where themes of power and dominance are important. For example, healing sessions are referred to as “work and empowerment” (asa sy fampaheresana). The exorcist’s conversionary tactics are invasive, requiring the patient to submit to God’s power. Exorcism also may be empowering for the patient, however, since she is required to become actively involved in the therapeutic process (cf. Taussig 1980b). Elisabeth, in choosing to be trained as an exorcist, has taken the final step. Her “work” is what will shape her new identity as a Sakalava convert and as an active Protestant.
Structural Shifts and Redefining Identity
As noted above, those who opted for exorcism were already marginalized for a variety of reasons, including madness, alienation from kin, or cultural dislocation resulting from migration. A final factor contributing to their marginality is especially notable. Even though all mediums I interviewed considered tromba possession to be a difficult experience, the majority accepted it as their lifelong fate. During the course of this research, however, I met five women who had opted for exorcism. Vivienne, Elisabeth, and Zaloky sought respite from tromba mediumship, possession sickness, or madness. A fourth woman was Mona, who attended the Pentecostal retreat. She was thirty-four and had three tromba spirits. Mona had suffered immensely during the previous six years from a host of problems for which no indigenous healer could find a cure, and she hoped that if her spirits were driven from her, her health would return. Finally, Berthine chose another route: she had a tromba spirit exorcised as part of her conversion to Islam. The afflicted may already be marginal even before becoming a Christian. Vivienne shared many of the problems of school migrants (chapter 9); in addition, she suffered from the complex problems associated with madness. Others already felt somewhat alienated from Sakalava kin or friends, as was true for Elisabeth and Zaloky (and the two men who converted to Lutheranism; see above). Thus, in at least three of these cases, it is not spirit possession that marks a Sakalava woman’s marginal status (I.M. Lewis 1966, 1971, 1991, and essays in I.M. Lewis et al., eds., 1991) but her inability to cope with it.
The exoricist’s power plays a pivotal role in the process of redefining such a woman’s identity. This is evident in the style of social interaction that occurs during healing sessions, where the exorcist and patient assume dominant and submissive positions. While an exorcist stands, the patient kneels before him or her. Exorcists will often touch the head of the patient, either with their hands or the Bible (see plate 8). This is a highly charged, symbolic gesture, that violates Malagasy rules of status etiquette. As noted in the story of Marie (chapter 8), the head is sacred and should not be touched. This is especially important if the patient is a tromba medium (and, even more so, if she is in the process of entering trance), since these royal spirits are said to sit (mipetraka) in her head. Only elders and royalty can raise their heads about others. Thus, the patient, in accepting the exorcist’s mode of treatment, submits to Protestant authority. Only once the patient embraces Christianity through conversion is the relationship between patient and exorcist defined as an equal one.
Thus, the power of the exorcist to transform a patient’s identity is rooted in the manipulation of the indigenous symbolic order. Structural shifts in identity may be partial or complete. Nevertheless, they define a central aspect of this therapeutic process, since a Sakalava patient must embrace beliefs that run contrary to her own culture if the therapy is to work. A medium must deny the existence of royal ancestors and be willing to relabel them as demons. She also must accept that the Holy Ghost is more powerful than tromba and that a Christian God is her savior and guardian. Finally, she must submit to the power and authority of a community peopled by non-Sakalava vahiny. Should she convert, her identity no longer hinges on her ethnicity; rather, she is relabeled as a Christian. If she is trained to be an exorcist, like Elisabeth, her new work (asa) as a shepherd (mpiandry) (rather than a tromba medium) defines who she is.
Joining a Community of Strangers
The concept of community is generally assumed to be central to religious experience (Durkheim 1965 [1915], especially Bk. 1; V. Turner 1969: chaps. 3 and 4), and, more specifically, in charismatic Christian communities, where the collective provides a supportive environment for those who otherwise feel socially, culturally, politically, or economically disenfranchised (see, for example, Comaroff 1985; Finkler 1985; Jules-Rosette 1975; Kehoe 1989; La Barre 1992 [1962]; Lawless 1988; McGuire 1982; for a fictional account from Africa see also Achebe 1959). An important dimension of the healing methods used by Malagasy exorcists is that, in severe cases, the patient must live apart from her original community and within the confines of the curing retreat. Thus, the concept of the Protestant community itself is viewed as therapeutic. Here patients are accompanied by kin and they are under the constant, watchful eye of exorcists. This practice is rooted in Malagasy culture, regardless of ethnic origin: throughout Madagascar, the room where a sick person convalesces can quickly become overrun by a constant stream of kin and other visitors. Similarly, patients at Protestant curing retreats are never left alone.
On a grander scale, the retreat is also simultaneously a model Sakalava village and an alternative Christian community. The retreat near Ambanja, for example, has been built in the middle of an already existing village, and the dwellings of other inhabitants are indistinguishable from those of the exorcists. Only the Protestant church and an outdoor communal kitchen stand out. Patients are expected to become active members of this community, taking part in the prayer sessions that occur several times a day and, as mentioned above, assisting in the work that keeps the retreat operating.
In the retreat, the notion of “cure” is relative and is subjectively defined, the concept of community playing a key role. Although (ex-)patients may continue to be troubled by their illnesses, they find that their eccentricities are usually better tolerated by others if they join a Protestant congregation or if they continue to live at the curing retreat. For example, the symptoms of madness that originally were viewed as extreme forms of social deviancy are redefined as the normative behavior of individuals who have been blessed. The assessment of therapeutic success also hinges on the healer’s subjective point of view, for in this context the cure is conditional, based on conversion to a new faith. It is, however, highly unusual for Sakalava to convert to Protestantism. Although such a choice is viewed as a major triumph for the exorcists, among Sakalava, converts such as Elisabeth are anomalies and even pariahs. Since they risk being abandoned by kin, mediums who choose to convert will stay close to the Protestant community. In so doing, they gain, as Zaloky said, new “family.”
Just as fictive kinship was pivotal in the context of tromba, it is also operational in these new Christian communities. Those who embrace Christianity are defined as “brothers” and “sisters” of one another, and all are children before God, the Father. Through exorcism rituals, patients break from Sakalava structural relationships and adopt new, Christian ones. In addition, a subtle shift in ethnic affiliation occurs: since the majority of Protestants are from the high plateaux, the kin terms used are not those of Sakalava village or town networks, but others derived from highland dialects. This shift is reflected in Zaloky’s choice of language, since she uses a high plateaux term (fianakaviana) when she says that the Lutheran church is her new “family.”
Even though the final step of conversion may relieve the suffering of these Sakalava women, it nevertheless raises other questions about the future of tera-tany identity in the Sambirano. Karp, for example, reports that within a year’s absence from Tesoland in Kenya, all of the mediums he knew had converted to Christianity and no longer practiced possession (personal communication; see also Karp 1987, 1989). In Ambanja, however, I do not anticipate that Protestantism will make major inroads into the community of Sakalava tera-tany, because for them this faith is too strongly associated with French colonial and Merina enemies. At present, conversion is rare and is a last resort, for the price one pays is very high. Elisabeth and Zaloky are extreme cases that involve women who desperately sought relief and found it only by joining this isolated community of strangers.
Notes
1. Portions of this chapter appear in a discussion of therapeutic efficacy in another article (see Sharp, in press): these include the overview of fifohazana healing, the case studies of Elisabeth and Vivienne, and figure 10.1.
2. There is an extensive literature in anthropology which addresses the efficacy of indigenous healers in treating mental illness, as well as other forms of affliction (see Fabrega 1970; Janzen 1978; Kiev, ed. 1964; Kiev 1972; Lebra 1982; Lévi-Strauss 1963a, 1963b; Prince 1964; Sow 1980; Taussig 1987, 1989; Torrey 1986; V. Turner 1964).
3. Bloch (1971: 59–60) for example, gives a brief description of a visit to an asylum in the high plateaux. He reports that patients lived in great fear of witchcraft from “heart thieves” (mpaka-fo) because they were surrounded by strangers. In essence, the asylum is oftentimes little more than a prison (see also Sharp, in press).
4. A discussion of the applicability of psychiatric diagnoses cross-culturally is beyond the scope of this chapter. Several authors identify psychiatry as being most effective when applied to Western, middle-class whites (see, for example, Marsella and White, eds. 1982; Meltzer 1978; Pande 1968; Pederson 1982). Kleinman (1978, 1980) suggests that psychiatry can be applied effectively cross-culturally if the psychiatrist comprehends the patient’s “explanatory model” of illness. Kleinman’s stance has its limitations, however, since it overlooks the depth of the patient’s subjective experience. He assumes that mainstream psychiatric practices can be effective as long as the psychiatrist has a grasp of the patient’s cultural background. Also, as Pappas (1990) argues, Kleinman’s model does not include an assessment of power within the therapeutic context. Thus I prefer to speak of competing epistemologies (Sharp, in press) since this emphasizes the complexity of the cross-cultural therapeutic encounter.
5. Spirit possession has long been a focus of interest for theologians; for other perspectives see, for example, Eikelman, Pazder, Peaston, and Salman in Prince, ed. (1968).
6. My informants did not describe spirits as occupying a second world apart from that of the living, as explained elsewhere in the literature (see Boddy 1989: 3ff, 269ff; Lambek 1981: 26; P. Stoller 1989, especially 48–49).
7. For an account of similar practitioners elsewhere in Madagascar see Mack (1986: 65) on the katibo, specialists who use sacred books called sorabe.
8. Until recently the Anglican church had no exorcists. This changed in 1987 when the Anglican bishop, who was a missionary from the United Kingdom, was trained as an exorcist by the Lutherans. He chose to do so not so much because he felt the need to drive out demons, but so that he could learn how to converse with and thus more effectively assist parishioners who believed that they were possessed.
9. These passages are central to defining the work of Pentecostal groups worldwide. For additional references see Goodman (1988); Jules-Rosette (1975); La Barre (1992 [1962]); and Sundkler (1961).
10. English text is taken from The New English Bible (Oxford and Cambridge University Presses, 1970); the Malagasy is taken from the Protestant Bible produced by Fikambanana Mampiely Baiboly Malagasy (1986).
11. For an analysis of the use of the active voice with animals see Bloch (1972).
12. Trexler (1989: 12) reports that a decade ago Lutheran exorcists would hit their patients with such force that in three cases they died; recently they have become more restrained in their actions. I never saw an exorcist strike anyone.
13. As was explained earlier, Malalgasy kin terms and terms of address are determined by the sex of the speaker and the person to whom they are referring. Since the majority of exorcists come from the high plateaux and the south, they tend to use Merina and related terms, thus: pirahadahy “brothers,” pirahavavy “sisters”; rahavavy “sister” for male speaker, anabavy “sister” for female speaker, and so forth. As with Sakalava, alternative terms of address are determined by relative age: zoky for “older sibling” and zandry for “younger sibling.”
14. Elisabeth was reluctant to give the names of her exorcised spirits.