Preferred Citation: Fernandez, Renate Lellep. A Simple Matter of Salt: An Ethnography of Nutritional Deficiency in Spain. Berkeley: University of California Press, c1990 1990. http://ark.cdlib.org/ark:/13030/ft2d5nb1b2/
 | A Simple Matter of SaltAn Ethnography of Nutritional Deficiency in SpainRenate Lellep FernandezUNIVERSITY OF CALIFORNIA PRESSBerkeley · Los Angeles · Oxford© 1990 The Regents of the University of California |
To
Enrique Carrasco Cadenas
1934 head of the department of dietary hygiene
National School of Public Health, Spain
Preferred Citation: Fernandez, Renate Lellep. A Simple Matter of Salt: An Ethnography of Nutritional Deficiency in Spain. Berkeley: University of California Press, c1990 1990. http://ark.cdlib.org/ark:/13030/ft2d5nb1b2/
To
Enrique Carrasco Cadenas
1934 head of the department of dietary hygiene
National School of Public Health, Spain
Prologue
This book is the fruit of a project concerned with the effects of delay and denial in human affairs. Anthropology, and the fieldwork that lies at the heart of it, is rarely an easy profession to practice, and a concern with delay and denial brings it more than its share of resistance and frustration. Those who participate, willingly or not, in a system of delay and denial—which has had unfortunate or grievous consequences in the lives of others—are not eager to have this implication of the lives they lead or the professions they practice pointed out to them; yet this is what I have tried to do here in a "simple matter of salt." All the more season, then, to acknowledge the help and support of those who, because of their own possible involvement, and, thus, not easily seeing what I was about, may have felt a natural resistance to the argument. What I advocate, an early preventive use of a simple remedy, and what I document, one country's long delay in getting around to iodizing salt, is worth pondering everywhere, whatever one's possible involvement in whatever system of neglect and denial.
Iodized salt, we should recall, had been introduced to stunning effect on a massive scale in both Switzerland and the United States in the 1920s. E. Carrasco Cadenas, a Spanish public official of the 1930s had advocated, on the basis of his own pilot studies in villages of northern Spain, similar action, but his intelligent and strenuous efforts failed to bring about the desired result in any timely way. This failure in one of Carrasco Cardenas's major projects must have been a great disappointment to him. He died young
at the end of the Spanish Civil War and it is to him and to the memory of his early efforts that this book is dedicated.
Why the simple preventive measures he advocated failed to take root is what this book explores. It is about the social, cultural, and political obstacles that create confusion and disinformation about diseases that—whatever the lifeway of an afflicted community or the belief system of a relatively unafflicted middle class—may be preventable.
Though this book is critical of some aspects of the medical establishment and of some of its narrow definitions, I would like to thank four Spanish physicians for their specific support and for their freedom from "established opinion." First of all, country doctor Manuel García Pérez of Caso, for showing me, as part of a project reminiscent of that of Carrasco Cadenas, schoolchildren he correctly believed were needlessly suffering iodine deficiency, thereby letting me know that my concern was well founded and that the endemic was not limited to a single village. Second, hematologist Joaquín Fernández García of Oviedo, who has a strong concern for the people of Escobines; I am grateful for the privileged "medical rounds" he gave me in that village, removing the doubts—in the face of wide medical denial—I had learned to entertain about the reality of the Asturian endemic. Third, endocrinologist Francisco Díaz Cadórniga, chief of endocrinology at the Hospital de Nuestra Señora de Covadonga de Oviedo, who gave me a historical perspective on preventive efforts in Spain and kept me in touch with new developments. And, last, investigative endocrinologist Francisco Escobar del Rey of Spain's CSIC, who added to that perspective, made important references available to me, and exemplified the citizen-scientist—a scientist active at once in high-technology investigation and in low-technology prevention.
Then I would like to thank the Spanish friends who have repeatedly, despite what must have appeared an obsessive inquiry, made me feel so welcome in Asturias: the family of Luis Días Muñiz in Oviedo and Celina Canteli and Julia Fernández and their respective families in Arriondas. I would especially like to thank Juan Noriega of Cangas de Onis for insisting that he, as a friend, hone my Spanish so as to more effectively take my inquiry beyond the confines of the village.
In the United States, I would like to thank the faculty of Rutgers
University, where the first version of this book appeared as a doctoral dissertation. First of all, I thank endocrinologist Louis Amaroso of New Jersey's School of Medicine. He shared my vision and kindly tutored me through the intricacies of the thyroidology I had to learn in order to link bodily pathology to the concept of a socially constructed disease. I thank Lionel Tiger of the Department of Anthropology who directed the dissertation. I thank the independent scholars of the Princeton Research Forum for the generous feedback they gave me in the spirit of an intelligently critical public. I thank Carole Counihan, a colleague and friend, for having offered me over the years a professional forum in which to explore my ideas, thereby giving my inquiry a badly needed sense of legitimacy. I thank Paula Ardehali, who has enriched our friendship by repeatedly offering wise editorial comment.
And, of course, I thank the villagers of Escobines who, since this is a study of pathology, will be thanked only by their first names (this also conforms to village practice); MariCarmen, Rosa, Carmina, Cheli, Floripes, Ludi, Rosaura, Ramira, Nati, Filomena, Pili, Jacoba, Luisa, Argentina, Chauri, Jesusa, Gene, and Socorro. Nor can I overlook the urban friends whose narratives of their own thyroid disorders have given me important insights: Susi, Milagros, and Celinuca. If the names of men are missing from this list, it is because iodine deficiency disorders, except where the deficiency is very severe, cosmetically affect mostly women. At a more profound level, as this study shows, men and boys are affected by it as well, as, indeed, are entire communities and regions. I thank them for having put up with this intrusive inquiry into the stigmatized condition so endemic in their village and for always receiving me and my family warmly.
Last of all, I thank my family, who have remained with me over the ups and downs of this longitudinal study. My concern with the dwarfed, deformed, and retarded must have seemed like an obsession to them, until they came to realize that it was in the service of better understanding the obstacles to prevention. I thank Andrew for giving me, when he was very young, a very personal reason for resisting denial; and I thank him for later introducing me to my Apple (only with it was it possible to write and rewrite obsessively). I thank Luke for periodically introducing a bit of sinister humor to the project. I thank Lisa for giving me hope, for ex-
terminating passive verbs, and for, several years ago, editing seven very crude chapters into a manuscript that could subsequently be approached by harsher critics. I thank Jim for bringing me to the field and having me espouse anthropology, inseparable from him. We are now jointly at work on the ethnography of this valley of cattle keepers and miners. Under the grants that he was initially able to get, we went to the field as a family, gathered the baseline materials for our diverse studies, and established the relationships that have continued to draw us back to Asturias over a twenty-five-year period. Our joint, and very strong, attachment to Asturias and the friends we have there—in village, town, and city—give an unusual temporal depth to this study. When in the mid-1960s I first came to this beautiful mountain landscape, goiter was everywhere and taken for granted as if it were part of that landscape. Now in the 1980s, major efforts are being made to eradicate it. In a small way, I can claim to have been a part of that change of attitude. This book is about that change in an Asturian mountain valley, set within a far larger problem of delay and denial in the perception and treatment of affliction.
R. L. F.
CANGAS DE ONIS, ASTURIAS, SPAIN
NOVEMBER 14, 1989
Chapter 1
Introduction
Simple Measures and Major Obstacles
A simple, timely action in the 1920s—the iodization of ordinary table salt—would have made the writing of this book unnecessary. But people in iodine-deficient regions of Spain needlessly suffered until the early 1980s, and in many regions of the globe continue to suffer, the chronic and often degenerative consequences of endemic goiter and cretinism. These are the two most well-known manifestations of the set of diseases coming to be known as iodine deficiency disorders, or IDD. A nutrition deficiency disease, IDD is manifested in a wide spectrum of afflictions that iodized salt is effective in preventing.
While the iodization of salt is a simple matter, the reasons for the failure to adopt this measure are complex. It is my task here to contribute to our understanding of health systems and medical care by explaining the complex of reasons that account for such inaction or delay.
The number of victims needlessly afflicted with IDD in Spain over these sixty years is not, even in that country, small. Over this time span, we conservatively estimate at least 10 million Spaniards to have been at risk of IDD; 50,000 have been sufficiently afflicted to have sought treatment.[1]
But inaction and delay have much wider—indeed worldwide—implications. For the failure to take the preventive action here examined is, in respect to IDD and a host of other preventable diseases, repeated over and over again, year after year, in country
after country. According to the most recent United Nations estimate, 800 million people around the globe are at present at risk of IDD (Hetzel 1989). This "simple matter" has very large implications indeed.
We have long known how to prevent the conditions, endemic goiter and cretinism, discussed in this work. Likewise, we have long known how to prevent other nutritional diseases such as pellagra and scurvy, obesity, adult onset diabetes, or the heart disease associated with a high cholesterol diet. More recently, we have learned how to control infant diarrhea with an extraordinarily simple measure also involving salt, but we have managed to propagate that technique to only one-fourth of the world's parents in need of it. We have also long known how smoking is associated with lung disease and how poverty and teenage pregnancy are associated with low infant birth weight, retardation, and other birth defects. But, as in the case of iodine deficiency in Spain, using our knowledge of prevention straightforwardly and to maximum effect has not been easy.
Take the example of our own society. It is our paradoxical tendency to spend very large sums on therapeutic high-technology intervention while neglecting to take preventive action. While the case reported here happens to have taken place in another country, the lessons that can be drawn from it are more widely applicable. The lessons are applicable on a global scale.
Today's newspaper headline, as I write this introduction, offers an instance of these problems:
HOSPITALS OVERWHELMED AS POOR IN NEW YORK CITY SEARCH FOR CARE
At its roots [it is] a crisis of a public-health system that regularly produces advances in medical procedures but cannot adapt itself to meet the most basic health needs of the poorest and weakest. . . . The crisis will not be solved by more beds. Unless there is a concomitant expansion of other services we will simply perpetuate a system in which expensive hospital-based technological interventions are substituted for more appropriate primary-care services.[2]
Here at home in the midst of our greatest city, in a cultural context different from the one reported in this book, is the problem we examine: the misdirection and misapplication of high-technology medical knowledge at the expense of low-technology primary care and prevention. The result of such misapplication of knowledge and resources is needless affliction.
Compared to the dramatic applications and cost of high-technology therapeutics, matters having to do with "primary care" may seem uninspiring. Typically, they involve education, immunization, monitoring and social support, and dietary or behavioral adjustments. It is not the stuff of high drama. Nor are such matters likely to seem the answer when, as in the American case, an infectious, life-threatening disease such as AIDS befalls us. Yet we continue to learn only belatedly, after years of affliction, how crucial preventive measures can be. Indeed, in the case of AIDS, they, for the moment, offer the only hope.
Most often, such low-technology measures are the most effective means of preventing or limiting the spread of chronic, endemic, and nutritional diseases. These, as in the case of iodine deficiency and other kinds of easily preventable disorders, assail hundreds of millions routinely as a part of daily life. Whether for our own sake or for the sake of the vulnerable millions in the less affluent parts of the world, we need to understand better the obstacles to prophylactic thinking and prophylactic action. By analyzing a case history of endemic goiter and cretinism, this work seeks to contribute to that understanding.
The Focus of this Study
In this work, I seek to explain inaction—the sixty-year delay in eradicating endemic goiter and cretinism in the village of Escobines and the parish of El Texu, a set of mountain communities in Asturias, a province of northern Spain. The knowledge gained in these mountain communities is set within the larger Spanish context and ultimately within a global context.
The case examined here illustrates, as I say, the wider phenomenon of inaction—the passive toleration of noninfectious, readily preventable diseases, chronic or endemic, that seem to exempt urban Westerners from their threat. Hence, this study is concerned with two larger issues: the diffusion of prophylactic techniques and knowledge and the generation of political will to employ that knowledge effectively.
There are many other conditions that merit the kind of attention given here to endemic goiter and cretinism, or IDD. Among these conditions are infant malnutrition, smoking, alcohol consumption, and overeating. What we learn of the twentieth century's passive toleration of IDD can help us understand these broader problems.
The iodine prophylaxis that at a mass level is capable of safely and effectively preventing endemic goiter and cretinism became feasible in the early 1920s. Knowledge of it came to the attention of the medical community, heads of state, and the American public during the peak years of the "prophylactic era"—from about 1920 to 1934. It was an era during which prophylactic programs were initiated in Switzerland and the United States and the virtues of iodine prophylaxis were widely discussed in popular literature as well as in professional journals.
Popularly, it was well known that Asturias and many other mountainous provinces of Spain had for many generations been afflicted by endemic goiter and cretinism, but it was during the prophylactic era that knowledge of these endemic disorders in Spain was inserted into the national and international medical record. The breadth and intensity of these endemias was delineated by Gregorio Marañón (1887–1960), Spain's most prestigious twentieth-century clinician. Marañón described their distribution first to his colleagues in the Royal Spanish Academy of Medicine and later to the first International Conference on Goiter and Cretinism (Schweizer Kropfkommission 1928).
The Swiss conveners of the conference offered a forum for presenting the results of pilot iodization programs and sought an international consensus to urge adoption of Vollsalz, "full" or "complete" salt. Marañón, however, rejected iodine prophylaxis for Spain, arguing that it was too specific a remedy for the wide spectrum of affliction he had seen in the endemic areas of his country. Instead of iodization, he favored broad economic development—an approach the Swiss considered a "grand detour" (Ein grosser Umweg ; Hunziker 1924). Regardless of his posture at the conference, at home, Marañón continued to be regarded as the national authority on endemic goiter and cretinism. It was he, after all, who had represented Spain in the international arena and singlehandedly imported endocrinology into Spain (Glick 1976). Since Marañón was also a man of letters and a political statesman who consorted with the king and later with Franco, his stature was such that, had he seen fit, at any point in his career he could have initiated iodine prophylaxis, whether specifically in the several regions of Spain designated by him as endemic or in the nation at large.
Marañón's overriding interest in curative rather than in preventive medicine may explain his failure to endorse iodine prophylaxis, but his medical and social authority, extending well beyond his death in 1960, meant that without his endorsement no prophylactic programs in Spain could get under way on a mass scale. As long as his views dominated Spanish medicine, any attempts at mass iodine prophylaxis faced prohibitive inertia at the national level. Only in 1984, a quarter century after his death, did regional health authorities initiate large-scale iodine prophylaxis in afflicted areas. This is the inaction (it can be seen as a delay only after the initiative gets under way) I seek to explain.
But any adequate and, indeed, useful explanation of inaction in regard to a major problem of public health has to reach beyond a single powerful actor. It must examine the medical, historical, social, economic, and cultural factors—in this case, both in Spain and abroad, both domestic and international—that create the social fabric of ignorance and indifference underlying inaction on any particular frontier of health. In other words, though Marañón was undoubtedly a powerful actor, he was nevertheless acting within a context that both influenced him and supported inaction.
Single individuals and local circumstances, as we shall see here, have created formidable and nationally specific obstacles to prophylaxis. These alone, however, cannot explain the globally widespread delay in implementing iodine prophylaxis. This is no minor matter. While iodine prophylaxis is generally regarded as the most cost-effective, mass-level, public health measure known, its benefits have not yet reached the already mentioned 800 million people around the globe (Hetzel 1989) who are still experiencing the debilitating physical, mental, social, and economic effects of endemic iodine deficiency (Matovinovic 1983:369). In this sense, the close examination of one case can throw light on the general problem of inaction, whether it concerns IDD, other conditions of dietary deficiency or overnutrition, or nondietary but widespread practices, for example, atmospheric pollution and depletion of ozone, affecting the quality of our lives.
Precedents
It is easier to examine events that have happened than those that have not. Nevertheless, some authors have addressed the elusive
subject of inaction. Matthew Crenson (1971) made a start in explaining inaction by examining the widespread hazard of air pollution to large populations and the concentrated interest of a few polluters to do nothing about it. Daniel Koshland (1987), among others, addressing himself to a wide spectrum of scientific, technological, and public concerns, has drawn attention to the need to find ways to weigh the uncertain costs of inaction against the certain costs of intervention. Most recently, And the Band Played On (Shilts 1988) offered a multistranded explanation of the exasperating delay attending the American response to AIDS. A variety of analyses on other fronts have dealt with the failure to withdraw support, for example, for the cultivation of tobacco, for the construction of houses on floodplains, or for the promotion of infant formula in inappropriate contexts. All of these accounts address the problem of inaction. Further studies should identify principles that underlie the reversal of hazardous passivity.
As for goiter and cretinism, I am not the first anthropologist to work in a community where IDD is endemic. Cultural anthropologists, at least traditionally, have been attracted to studying isolated people residing in mountainous areas difficult of access. As will be seen later, geologic factors alone tend to make iodine scarce in such regions, producing disorders in those whose food is exclusively of local origin. The anthropologists who have studied the culture of people residing in regions deficient in iodine have, with few exceptions, remarked on the presence of these endemias; but they have considered the endemias as incidental, as having little bearing on the society and culture they have come to observe. Netting, working in a classically alpine region of IDD, and author of an otherwise exemplary ethnography (1981), illustrates this incidentalist approach.
Other anthropologists, using a contrasting approach, have drawn attention to changes that have introduced goiter and cretinism to peoples previously unafflicted with IDD. Andrew Vayda and Henry Kranzler (1977) have shown how the disruption of traditional trade routes supplanted customary salt (inadvertently rich in iodine) with ordinary uniodized trade salt, imposing IDD on a New Guinea people among whom goiter and cretinism had been unknown. Georgeda Buchbinder (1977) also reported on a recent eruption of endemic goiter in New Guinea which resulted from the
displacement of people from their highland home into a yet higher, previously uninhabited valley. These publications, combined with the alarming visual and quantitative material produced by D. C. Gajdusek (1975), set the stage for the initiation of iodine prophylaxis in New Guinea.
So far, the most comprehensive study of an endemic community is that by Lawrence Greene, a physical anthropologist who in his field study collaborated closely with Rodrigo Fierro-Benitez, an endocrinologist from Ecuador. Greene investigated the psychological and social effects of iodine deficiency on Andean villagers (1973, 1977a , 1977b ). Because his work was comparative both within and across villages, he was able to isolate the effects of endemic IDD from a generalized backdrop of protein-calorie malnutrition. In a medical experiment, he compared the performance of a set of controls—children whose mothers prior to conception had received prophylactic injections of iodine—with the performance of children of the same age and in the same village who had not received this uterine benefit. The latter group's performance on conventional psychological tests and on tests especially devised for this culturally specific situation was, in contrast to that of the iodized group, alarmingly low.
The endocrinologist compared, in a natural experiment, two nearby Indian villages: a village free of IDD (because it had access to nearby unpurified rock salt rich in iodine) with one endemically afflicted (Fierro-Benitez 1968). This study revealed the neurological and behavioral limitation that was an integral part of life in one village—affecting the distribution of employment, migration opportunity, labor assignments, food, comforts, and affection. He went on to show the several effects of widespread behavioral limitation, how it generally lowered the standards and expectations villagers had of each other and created hierarchies in the village, and how the burden of behaviorally limited individuals in the villagers' midst affected, in the larger society, the reputation of all the members of the afflicted community. This collective disrepute, in combination with a long history of exploitative and extractive domination, made the villagers docile and facilitated their exploitation by members of the larger surrounding mestizo society.
Greene did not argue, and on this point he was clearly misunderstood (Vayda 1979), that iodine deficiency caused social and
racial stratification. He and his colleague did, however, argue that widespread behavioral deficit stemming from iodine deficiency served vested interests. For just as IDD produces defects in individuals and, consequently, hierarchies among villagers, it also reinforces social stratification already existing at local, regional, and national levels. In other words, nutritional deficiency works systematically to make all the members of an endemic community—regardless of the degree of affliction in any particular individual—more vulnerable to exploitation.
The pervasive effects of iodine deficiency on a community were also observed by Margaret Mead. Unlike Greene, however, she did not initially set out to inquire into iodine deficiency or into any culture of affliction. Rather, Mead's cultural concerns impelled her to select a particular Balinese village for the observational advantages afforded by unfinished constructions—a village where the walls dividing domestic from public space were left incomplete. Only after having worked in this "unfinished" village for a time did Mead recognize a pervasive underlying iodine deficiency, especially manifest in hypothyroidism. This, she reasoned, was the underlying cause of the lethargy and slowed mentation expressing itself in unfinished construction. Long after completing the fieldwork, she argued (1977) that hypothyroidism's continual sapping of villagers' energies offered her the opportunity of observing the elaborate Balinese culture stripped down to its essential elements.
Neither prophylaxis nor the obstacles to it were Mead's concern. She did, however, notice that those accepting the prophylaxis she offered were outsiders who had married into the village, while those born and raised locally rejected it. Indirectly, this suggested that a lifetime of habituation to pervasive behavioral defect may set up local obstacles to prophylaxis.
Four decades after completing the Balinese fieldwork, Mead recommended, despite perceiving the drag of iodine deficiency on these Balinese villagers, that the proper focus of anthropological investigation should not be the individuals or communities succumbing to environmental or nutritional stress but rather the individuals and communities apparently impervious to it (1977:265). Mead maintained that her opinion spoke for the unexpressed opinion of the majority of anthropologists, presumably those interested in culture.[3] This majority feels itself uncomfortably "racist" drawing
attention to morphological and behavioral limitations it considers itself unable to ameliorate (1977:262). Her admonition seemed for a time to place work such as Buchbinder's and Greene's beyond the pale of "normal" cultural anthropology.
If Mead's view ever represented the view of a broad segment of anthropologists, it has now been transcended. Anthropologists have recently shown how society and culture play important roles both in producing and alleviating morphological and behavioral limitations (Scheper-Hughes 1979; Laderman 1984; Kleinman 1980; Kleinman and Good 1985). This case study follows that tradition. It expresses my belief that ignoring stigma and disrepute or treating morphological and intellectual features—such as endemic retardation and bodily deformity that quite possibly have their genesis in conditions that can be ameliorated—as incidental to culture lends support to inaction.
How this Investigation Emerged
I did not choose in advance to investigate the problems of affliction and inaction. Rather, they confronted me in the field after the field site had been chosen, on terrain characteristically that of the social or cultural anthropologist. A broad-scale ethnography was the object of research. The terrain consisted of small mountain communities variably touched by modernization, industrialization, and bureaucracy. In these communities, I, my husband, James W. Fernandez, and our children witnessed, over the course of a longitudinal study, rapid social and cultural change brought about by the shift of agropastoralism to coal mining. This shift got under way during mid-century but increased its tempo during the 1960s, as we were beginning our research. We focused our work on one particular village, Escobines, comparing it to other nearby villages, where the economic shift was proceeding at a different pace. We have presented several facets of that work (J. W. Fernandez 1976, 1977, 1984a, 1984b, 1985, 1986a, 1986b, 1988a, 1988b, 1988c ; R. L. Fernandez 1979, 1980, 1985, 1986, 1987a, 1987b, 1987c, 1988, 1989a, 1989b ; J. W. Fernandez and R. L. Fernandez 1976, 1988).
The documentation and analysis of inaction on the prophylactic front came only gradually to be one part of that larger project.
Early during our series of field visits, I took notice of the goiters much as the incidentalists had done before me. Then I became increasingly aware of the pervasiveness of less obvious disorders. These brought forth my concern for the social aspects of affliction. I speculated that these diffuse afflictions, like goiter, were related to iodine deficiency, but local medical and health personnel denied any connection between goiter (which, they maintained, was not endemic but idiopathic) and these more diffuse afflictions. Moreover, since goiter was said to be "declining of its own accord,"[4] these professionals expressed no interest in my preoccupation. Since I was for a long time unprepared to imagine that physicians could not know about iodine prophylaxis, I interpreted their two-fold denial as expressing political opposition to prophylaxis. Whatever the basis of those denials, their response made it clear that as long as the Franco regime remained in power, an outsider could not hope to investigate political obstacles to prophylaxis.
Franco's death in 1975 put an end to his four-decade regime and inaugurated a period of accelerated political change during which the political obstacles to prophylaxis that I had imagined seemed to recede. Yet, since goiter, though declining, appeared still to be endemic and prophylaxis did not get under way at the close of this era, I was forced to enlarge my tentative political hypothesis and look for others as well. I learned then that the biomedical community abroad attributed this inaction to underdevelopment.
But underdevelopment could hardly explain the IDD and non-prophylaxis before me. Asturias, after all, was a well-developed economic region with roads, tunnels, mines, and harbors; with universal schooling and a high literacy rate; and with low infant mortality.
The extent of development had been revealed to me by our longitudinal study, which in many ways provided a rich backdrop for probing further into the puzzle before me. Unlike Mead's villagers, these Austurian village women were seeking remedies: they were taking vitamins for "thyroid," seeking goiterectomies, and exposing their glands to nuclear medicine, paid for by the state. Yet, and here was the nub, they did not seem to know that they were suffering needlessly. No villager knew of the existence of iodine prophylaxis. And as I inquired further, it became clear that middle-class urbanites and the vast majority of Asturian physicians also did
not know of its existence. I was taken aback by this specific ignorance in the midst of such high-technology medicine. I had thought that in medical circles, iodized salt was universally known as a cost-effective prophylactic.
This revelation of my own unexamined assumption prompted me to inquire into the complex of obstacles that exist in the larger contexts of national and international life, both in Spain and beyond. Pursuing this complex of obstacles, I came to recognize and feel part of an old anthropological tradition that, long in abeyance, was experiencing a revival at the turn of the 1980s. That tradition considers morphology and physiology a legitimate and central part of holistic anthropological inquiry (Konner 1982). Study of the interplay, in the case before me, of geology and chemistry, the human body, medicine, history, economics, and politics, land, and culture might answer questions that discrete biological, cultural, or medical inquiries—narrowly construed—might never answer.
The Diabetes Study Group of the American Anthropological Association, for example, has employed this holistic approach for some time. Why, some of its members have asked, are certain populations like the Papago-Pima especially vulnerable to diabetes, and how can they be protected from it (Knowler et al. 1981, 1983). Other holistically inclined researchers have sought explanations for alcoholism wreaking especially great havoc among people who until recently were hunters and gatherers (Martin 1978) or for the extent to which violence and dietary behavior are integral parts of a single behavior complex (Bolton 1979, Lewellen 1981). Investigators like these and others (Lindenbaum 1979) have drawn our attention to the social factors that foster a disease or perpetuate it unnecessarily.
As a consequence of these efforts, we can view a variety of diseases—a viral disease like kuru, a lowering of immunological defenses like AIDS, and chronic biochemical upset like hypoglycemia—in a new light. We can see them not only as viral or immunological diseases but as social diseases. In the same light, we can view goiter and cretinism as a linked set of social diseases perpetuated by convenient social arrangements. These social diseases require, among other things, active social intervention. If it is to be effective, this intervention must be based on an awareness of
the various resistances within the larger national, international, and scientific contexts.
Collection of Field Data in a Longitudinal Study
The longitudinal study, which I began informally in the summers of 1965 and 1966 by establishing personal relations and mapping our focal village, got formally under way in 1972. The major part of the sixteen-month field trip begun in that year was spent in making a house-to-house census, collecting genealogies, life histories, and narratives. We spent subsequent summers and the year 1977–78 again in Asturias, returning often to the village, enriching and updating our materials. I spent summer 1984 in Spain but largely outside the village, making comparative inquiry in other villages and in other regions, interviewing physicians and other authorities on the obstacles to prophylaxis in urban centers, both in Asturias and in Madrid.
Our house-to-house census of 1972, differing only slightly from the official census of 1970, revealed 783 people distributed over 232 households. I came to be on speaking acquaintance with most of these villagers and to know some quite personally, not through formal inquiry but by participating in their lives as they intersected our lives and the lives of our children.[5] Thus, through focusing my participant-observation, I learned to identify everyone in the upper half of the village by name and to place all the villagers according to where they lived, to whom they were related, how they made a living, and how wealthy, industrious, or reputable they were in relation to others.
I hesitated to openly inquire into goiter, for I was aware that the villagers felt themselves stigmatized by it. Moreover, as already mentioned, I was profoundly aware that authorities felt obliged to deny goiter any significance. Convinced, however, that goiter was prevalent enough to warrant attention, I made a visual inspection of all the villagers and recorded my observations on the census and genealogies. On subsequent visits when updating the survey—keeping track of items like births, deaths, new construction, and resettlement—I took note of changes in the appearance of individuals, recorded goiterectomies when I heard of them or
when women showed me their scars, and added to my archive of personal histories.
The women who gave me these accounts often highlighted matters of health and disease. In this way, I informally came across a wealth of information pertaining to their own or a relative's quest for medical relief from a variety of symptoms. I learned that women received prescriptions for dietary supplements, appetite depressants and stimulants, and thyroid preparations. As these fragments of informal medical histories mounted, I began to trace the many ways in which the afflictions—reported or observed by me—were embedded in the genealogies and in the fabric of village life.
From time to time, middle-class women in the provincial capital and in three Asturian county seats also told me about their quest for relief from thyroid disorders. Hearing isolated tales of affliction narrated by urban, middle-class women, and tying these to the many tales given me by the women of Escobines, I came to discern a characteristic clinical pattern that cut across the urban-rural division. Each woman saw her thyroid problem as a discrete, isolated event; no patient and no physician (with two notable exceptions to be discussed in chap. 7) saw these thyroid cases as possibly the varied but systematic expression of one underlying problem—as symptoms not inconsistent with a diagnosis of IDD. In general, the Asturian physicians who consented to speak with me in the late 1970s refused to entertain this idea.
I concluded then that until Asturians could openly acknowledge endemic IDD in their midst, a formal investigation by a foreigner might only raise professional and political defenses in Asturias and Spain and further delay coming to terms with IDD and the initiation of iodine prophylaxis. The turning point came in 1982 when, for the first time since the days of the Republic (1931–1936), the Socialists were voted into office. On the heels of that election, regional health officials in Asturias, as well as in Galicia, a region on the western boundary of Asturias, announced (the reader may appreciate my feelings of relief and vindication) that IDD was, indeed, endemic and that they would soon be launching a provincial campaign to eradicate goiter and cretinism. National health officials followed that initiative and within a year announced a nationwide campaign to eradicate these disorders.
Direct investigation into the long-standing obstacles to pro-
phylaxis became, therefore, the principal and open focus of my field investigation in 1984, when I returned to Asturias to interview medical researchers, health officials, and clinicians. Their responses, in combination with the field material gathered in the village over previous years, serve as the raw data for my analysis.
Here I need to underscore the end to which I gathered data among two distinct field populations: Asturian villagers and Spanish medical personnel. In the village, I had to establish to my own satisfaction that IDD was endemic and how the people, individually and collectively, responded to their affliction. Once this was done, I needed to ascertain how, if at all, villagers and the conditions of village life posed obstacles to prophylaxis. Only then, after searching exhaustively for local resistance to prophylaxis, did I, a community-oriented anthropologist, search for obstacles posed by the larger social, economic, and political system and by medicine itself.
Field Methods
The materials gathered in the village are different from those out of which a formal epidemiological study is usually made, yet they have crucial value. Observations like mine can be seen as early warnings of endemic disease, enough to either prompt a formal epidemiological investigation or directly take action.
Anthropologists are specialized in two ways that bear on the method of this investigation. First, they gather materials accessible to the naked eye and the unassisted ear. Second, they relate them to genealogies, inheritance patterns, life histories, and narratives. Thus emerges a sense of the prevalence of affliction and its pervasiveness into the social and cultural fabric of a community. In my case, the affliction turned out to be IDD, but the method is broadly applicable to chronic, endemic, and nutritional disease. Tests not within the range of the anthropologist's competence may and often should, of course, provide additional and confirmatory evidence that intervention is in order.
In 1974, the World Health Organization (WHO) defined an area of endemic goiter as follows:
An area is arbitrarily defined as endemic with respect to goiter if more than 10% of its population is found to be goitrous on appropriate survey.
The figure 10% is chosen because a higher prevalence usually implicates an environmental factor, while a prevalence of several percent is common even when all known environmental factors are controlled. (Dunn and Medeiros-Neto 1974:267–268)
This definition set standards that enabled me to ascertain that the level of goitrousness in Escobines was well above the official threshold of endemicity, for the majority of women age forty and over were visibly goitrous, and these accounted for more than 10 percent of the population. In 1979, the WHO definition was adjusted, however, and from my point of view set more stringently, making me doubt that I could ever satisfy any skeptic that goiter was indeed endemic in Escobines. It proposed that endemic goiter be defined "as a prevalence of goitre of at least grade lb of 5% or more in pre- and peri-adolescent individuals or of 30% or more of grade la among adults. At this level, public health intervention seems to be called for" (DeMaeyer, Lowenstein, and Thilly 1979:9).
Visual methods made it difficult if not impossible to distinguish the grade la and lb goiters, which in normal postures are invisible and ascertainable only by palpation. Nor, with the natural attrition of the older bearers of conspicuous goiters, could I hope to demonstrate anything like 30 percent goitrousness in the general village population. By my visual method—observing people in the course of daily living and in normal postures—I could count only the higher grades of goiter: grade 2, thyroid easily visible with the head in a normal position;[6] grade 3, goiter visible at a distance; and grade 4, monstrous goiters (Ibid., 10).
Even so, I inferred from a combination of evidence that goiter was still of endemic proportions. Slightly less than half the women of Escobines age forty and over, 48 percent in this age group, appeared goitrous in 1980. This percentage did not, of course, hold across the rest of the population, for female hormones tie up iodine, making goiter vastly more common in women than in men. But the fact that fifteen women, all of them under forty, had either been goiterectomized, shown me prescribed medications for thyroid, or mentioned their exposure to the nuclear scanner (to measure the uptake of radioactive iodine) gave sufficient reason to infer that grade la and lb goiters were highly prevalent among them.
My count, by ethnographic if not by medical definition "an ap-
propriate survey," satisfied me that the prevalence of overt goiters was such as to justify searching for obstacles to prophylaxis. This private conviction, based on visual observation and confidential information, proved sound enough when the results of the official Asturian survey were finally released in 1986 (Aranda Regules et al. 1986:36, to be discussed in chap. 7.).
Indeed, the regional officials, who carried out their survey only among schoolchildren, in whom goiters are rarely visible with the head in normal position, demonstrated a level of endemicity severe enough to warrant not only the introduction of iodized salt but emergency intervention. The latter meant injecting schoolchildren in the most afflicted zones—including the zone in which Escobines is situated with iodized oil, because iodized salt had not yet become available. This emergency measure, expensive compared to the cost of iodized salt, was followed by an educational campaign and, months later, by the introduction of iodized salt. As a consequence of these measures, the biochemical indicators of IDD (T4 and UIE levels) are approaching normal. Their rise suggests that the incidence of IDD in Asturian youth will soon drop.
My study suggests that when neither clinical not biochemical evidence can be obtained to corroborate the suspicion of IDD, it is appropriate to resort to inference and standard ethnographic methods. However "indirect" the findings these measures yield, they can lend support to the initial suspicion of IDD and help to establish a demand for prophylaxis. To insist on an "appropriate survey" before prophylaxis can be undertaken may quite needlessly, as in Asturias, create an expensive emergency.
The importance of clinical and biochemical tests cannot, however, be denied. Ideally, team research including longitudinal, ethnographic, and genealogical data of the kind presented in this study should be gathered in conjunction with clinical and biochemical tests. But to insist on "appropriate surveys" as the only legitimate method of recognizing an endemia is to strengthen the supports of inaction. Legitimation of only such clinical methods gives reluctant officials the "plausible deniability" they need to continue opposing prophylaxis.
Once appropriate survey techniques, as officially defined, had established the existence of the Asturian endemia, it could no longer be denied. Only then would Spanish physicians and health
personnel help me discern the complex of obstacles to prophylaxis that had for sixty years operated at all levels: regional, national, and beyond the confines of the nation. They cooperated in helping me discern these obstacles only as those obstacles were being dissolved. This irony is worth pondering.
Argument
My central argument holds that failure to implement iodine prophylaxis cannot be explained by "underdevelopment" (Clements 1961, Dunn 1974), for it fails to explain inaction in Asturias or Spain. It must be emphasized that Asturias is a highly industrialized province with one of Spain's highest literacy rates, a province in whose most remote villages primary medical care has been available since at least the 1950s and where immunizations have been routinely offered and accepted since the beginning of this century. Something other than underdevelopment or the resistance of villagers to modern medicine—long an ethnomedical concern but in this case a red herring—must therefore account for prophylactic inaction in Asturias. Elucidation of these other obstacles is what this book is about.
Before these obstacles are addressed, however, it is necessary to discuss iodine—how it moves through the physical world and the organic system, what it does in the body, and what happens when intake is deficient. Chapter 2 offers this discussion. The arguments of subsequent chapters are based on concepts introduced in it, concepts like consanguinity, metabolic error, goitrogens, hypothyroidism, and behavioral and sensory defect.
The next four chapters make up the ethnographic core of the book: the case history of IDD in an Asturian village and parish. Chapter 3, Diet and Image, shows how geology and climate produced a vegetation and—over historical time—an economy and life-style that led to dietary deficiencies. Pathologies resulting from the deficiencies, and a dialect developing out of isolation, long interacted to produce a negative image of the Asturian region, and that image itself until recently predisposed officials and physicians to inaction.
Chapter 4, Kinship and Affliction, considers the extent to which metabolic error and inbreeding played a role in producing the
disorders seen among villagers. Affliction and consanguinity are traced through the genealogies, converting them into the pedigrees of medicine. IDD in Escobines is thereby shown to be not of hereditary but of dietary causation, for the pedigree shows that only after the decline had set in did villagers cease to form consanguineous unions.
Chapter 5, Land and Diet, links poverty to the expression of IDD. As is shown here, relatively landless people resorted more frequently than others to foraging on common land for chestnuts, which are goitrogenous, and experienced IDD more severely. I argue that any complete account of IDD must take into account not only the environmental threshholds of iodine but also the dietary antagonists to which segments of the population may be subject.
Chapter 6, Narrative Accompaniments of Rural Character and Disrepute, asks why no local initiative was undertaken to obtain prophylaxis and finds the answer in part in stories and folklore. Insults, a specialized vocabulary, and denigrating stories suggest the disrepute under which the villagers have long labored, leading them to suspect themselves less capable of progressive initiatives. This chapter concludes the ethnography of affliction.
Chapter 7 moves beyond the confines of the village. Those who hold the village or region in disrepute, fault consanguinity, perpetuate diet differentials, and withhold knowledge about iodine prophylaxis are not villagers but outsiders. It is this kind of opposition to prophylaxis and the manner in which prophylactic knowledge and techniques are disseminated that come under scrutiny in this chapter. Extranational agendas, commerce, publications, and medicine played a part, however unwittingly, in institutionalizing ignorance of prophylaxis in Spain. This institutionalized ignorance is what in Spain ultimately accounts for prophylactic inaction.
Chapter 8, Closing the Gap between Therapy and Prevention, considers whether the explanation of prophylactic inaction as argued in this particular case—observed in an industrialized province of a modern Western nation—stands out as just an exception to the rule of underdevelopment. It points out how we, the outsiders, were we to take into account the contexts in which technical information is disseminated, can offset the ignorance and misinfor-
mation all too often fostered by individuals and institutions within a nation.
Because of the action initiated five years ago, the story told here is moving toward the satisfactory conclusion that might have been achieved many years ago by the simple matter of iodizing salt. Several generations of suffering might have been avoided had the kind of knowledge and awareness we seek to develop here been available and acted on in the 1920s.
Chapter Two
Iodine: An Essential Dietary Element
Introduction
The protagonist here is iodine.[1] It provides the medical background for the remainder of this work. Conventional medical presentations focus on an organ, a physiological system, or a disease, while this presentation focuses on an element. My approach relates the dynamics of iodine's movement through physical, commercial, and organic systems to the theory of trace elements, to iodine's essential role in thyroid function, and to the most common disorders engendered by iodine deficiency.
Western biomedicine recognizes the importance of iodine, but ordinary clinicians often take adequate iodine intake for granted. Spanish physicians did not normally question, or were not normally taught to ask, whether their thyroid patients' iodine intake was sufficient, though many patients came from areas previously identified as iodine deficient. Clinical symptoms were therefore interpreted as idiopathic (stemming from no known external cause) rather than as the result of malnutrition. This is an instance of a tendency widespread in the medical profession to wrongly assume a disease to be idiopathic, and treat it as such, when, in fact, it should be seen as a case of endemic malnutrition that must not only be treated but also prevented in the future.
Knowledge of iodine or of its absence as an essential dietary ele-
ment is crucial to correct diagnosis and action. I seek to give an overview of these matters here. First, I discuss the way iodine normally moves through the environment and within organisms. Following is a discussion of iodine-related pathologies.
Physical and Organic Iodine
Theory of Trace Elements
A trace element's essentiality is difficult to demonstrate, for, in contrast to bulk and macro elements that are ingested and concentrated in living tissue at levels measured in grams and kilos, trace elements are ingested and concentrated in tissue at low concentrations and are measured in milligrams and micrograms. The biological role of only a few of these elements is known at present, but the list is expanding. An early definition of essentiality held that an element is essential if it is required for the maintenance of life and if the organism dies in its absence. The definition was problematic, however, for even in a laboratory experiment it is difficult to eliminate all traces of any particular element and hence to demonstrate that death follows from total deficiency. As a result, a more workable definition of what is essential has been proposed:
An element is essential when a deficient intake consistently results in an impairment of a function from optimal to suboptimal and when supplementation with physiological levels of this element, but not of others, prevents or cures this impairment. (Mertz 1981)
A trace element is now considered essential if on ingestion in suboptimal amounts, it impairs function and on supplementation, restores it. This change in definition is significant for health policy because the presence of apparently unafflicted individuals amid a population believed to be deficient posed, according to the old definition, a problem: their very presence cast doubt on the notion that the element was essential to the maintenance of life. A well-formed, intelligent individual amid a cretinous and goitrous population seemed, in the case of iodine, to call into question the whole idea of essentiality. The new definition disposes of that obstacle to prophylaxis.
The Dose Response Curve
The dose response curve (fig. 1) illustrates the new definition. It facilitates consideration of impaired function and deals with overintake as well as deficiency. Arsenic's toxic effects in large doses are well known, for example, but its deficiency effects are only beginning to be documented. Conversely, effects of molybdenum deficiency were well known before its toxic effects were even surmised.
The shaded area on the left in figure 1 shows impaired function below a certain threshold and adequate function above it. The shaded area on the right indicates the dysfunctional aspects of over-dosage. The intake of iodine at either extreme can produce a hypoor hyperfunctional thyroid gland. Optimal function takes place within a wide range of intake, allowing for daily and seasonal variation. People can take in most of their annual iodine requirement, for example, over the course of a fishing season. The breadth of that safe margin makes it unnecessary for policymakers to spend time pinpointing "locally ideal" levels of supplementation.
A trace element does not act by itself. Its efficacy depends on organification, that is, on its becoming part of a carbon compound within a living organism. It becomes effective only on forming part of larger molecules, such as the pair of thyroid hormones, T3 and T4.
Homeostatic mechanisms buffer the ends of the range of optimal intake. Supraoptimal amounts of a trace element may simply be excreted when intake far exceeds the required level. Suboptimal intake may be buffered, as in the case of iodine, by shifting production of hormone to T3, the generally more potent of the pair, which uses fewer atoms of iodine.
Below, I describe how iodine moves through the environment, the food chain, and the body; how certain factors impede its transformation into hormone; how the body responds to marginal intake; and the disorders in which iodine deficiency plays an important though often poorly appreciated role. This understanding of the cycle, and of iodine physiology and pathology comes from standard biomedical sources (Stanbury 1969, 1978; Matovinovic 1983; Fisher 1983; Utiger 1979; Tepperman, 1980; Petersdorf 1983; Netter 1965; Pitt-Rivers 1961; Thompson and Thompson 1980).[2]
Fig. 1.
Dose Response Curve (based on Mertz 1981:1332)
My purpose in focusing on the element needs to be underscored and explained: conventional medical presentations leave clinicians and health officials without a proper appreciation for the movement of iodine through the physical and organic world, setting the stage for taking the presence and availability of iodine for granted. Prophylaxis may take a back seat to therapeutics when this movement fails to be appreciated.
The Cycle of Iodine in the Environment
Iodine makes up 0.4 percent of the earth's mass but is unevenly distributed. It is present in rock and earth in the form of soluble iodine salts that when taken up by plants, enter the food chain. Iodine's solubility makes it prone to being leached out of soil, especially in areas of heavy precipitation. In this way, it gravitates toward the sea where it becomes concentrated.
Oceanic evaporation permits iodine to become airborne and return to the land by way of atmospheric iodine transport. Climatic forces of glaciation and high precipitation leach iodine out of highlying mountain areas such as the Alps, Himalayas, and Andes, leaving many mountain populations severely iodine deficient.
Leaching is particularly severe where the parental rock is limestone, as in the Cantabrian range of central and eastern Asturias. Limestone lowlands, once glaciated, tend also to be poor in iodine. In such areas, problems of iodine deficiency are compounded, for limestone dissolves as water percolates through it, thus charging groundwater with minerals. As part of drinking water those minerals bind with iodine, making it less available for organification. The "goiter belt" of the United States, stretching from New York State to Minnesota and beyond, exemplifies such a case. As a general rule, the farther the area lies from the sea, the slower it is replenished by atmospheric transport.
Iodide is more abundant in rock and soil than in seawater, but the life forms that thrive in seawater concentrate it, for example, in kelp and fish thyroids. These substances themselves, or the ash derived from them, have long been used in China, the Andes, and Asturias as folk remedies for goiter.[3]
The largest natural storehouse and site of extraction of iodide is the Chilean nitrate bed, which was formed when ancient sea-
beds became mineralized. Until recently, most of the world's iodide production came from this deposit. With the multiplication of industrial uses of iodine in the twentieth century, iodide production has diversified, drawing on both minerals and plants for raw material. Kelp, for example, is harvested on Asturian shores and sent to other Spanish provinces for processing into gums and chemicals. Indeed, more than 99.5 percent of the world's current production of iodide and iodate is destined for industrial ends not related to nutrition. Supplementation of the world's human population with prophylactic iodine would annually take no more than 370 tons. However scarce iodine may be, even in the diets of people harvesting it from the sea for industrial purposes,[4] it cannot be considered a scarce world resource.
Dry salt mined from interior deposits may, before it is purified, be rich in iodide. But contrary to popular belief, solar salt and sea salt made from iodine-rich brine are not themselves rich in iodine, for brine contains impurities drawn off before the salt is harvested. Only artificial applications of iodide during later stages of salt manufacture ensure its iodine content.
Drinking water is frequently used as an indicator of local iodine status, though humans rarely receive more than 10 percent of their dietary iodine from drinking water. It may, however, be an appropriate indicator of intake if one recognizes that water draining the local environment generally reflects the iodine content of the vegetation, thus reflecting the iodine status of people subsisting chiefly on locally grown plant food. It is, however, a poor indicator of iodine status when the diet includes goitrogens (see below) or when the diet includes many foods of animal origin, since terrestrial iodine becomes concentrated at the top of the food chain. This means that people with greater access to milk, eggs, blood, and meat—to foods at the top of the food chain—are less likely to experience pathology than those subsisting almost exclusively on a diet of roots, nuts, and grain. A dual diet within a single zone can thus exempt the richer segment of society from symptoms while producing them in the poorer. Unfortunately, this differential effect props up belief in the innate vulnerability of the poor, while seeming to undermine the environmental hypothesis.
Iodine has been withdrawn or added to diets in unexpected ways. Disturbance of trade routes or a change in salt supply has
brought symptoms of iodine deficiency to populations formerly free of them. In Nepal, for example, newly available solar salt has supplanted the unrefined rock salt formerly transported by animal power over difficult mountain passes (Mumford pers. comm.). In New Guinea, noniodized commercial salt has suppressed traditional salt laboriously extracted from certain rare iodide-concentrating plants (Buchbinder 1977).
Commerce and industry have adventitiously introduced iodine in several ways. Subsistence agropastoralists turning to commercial feeds, for example, have inadvertently introduced iodine from outside the local ecosystem into their own food chain.[5] People have unknowingly absorbed iodine in medications and applied it as a first aid measure to the skin. The expanding food industry has introduced it into food, prompting the National Academy of Sciences to propose that "any additional increases should be viewed with concern. It is recommended that the many adventitious sources of iodine in the American food system, such as iodophores in the dairy industry, alginates, coloring dyes and dough conditioners, be replaced wherever possible by compounds containing less or no iodine" (National Academy of Sciences 1970). A more balanced statement by the academy would have addressed not only national surfeits but also global deficiencies, taking into account as well the dangers at the low end of the dose response curve. The academy thus displayed the unexamined assumption of "iodine affluence" characteristic of much of Western biomedicine. Health workers in the Midwest have recently reported the reappearance of goiter on farms (NYT Sept. 29, 1987:1), calling into question the assumption of iodine affluence even in the United States. In chapter 7, we will see how this assumption has been exported around the globe.
The Physiology of Iodine
Basic Understandings
Marine demonstrated in 1915 the essential role of iodine in thyroid physiology. His findings led to pilot iodization projects in both Switzerland and the United States. Favorable evaluations led to mass prophylactic programs carried out by governmental authorities in Switzerland and essentially by commercial entities in the
United States (Matovinovic 1983). Mass prophylaxis was not, however, extended to most other populations also known to be endemic, such as people residing in the Alps of Austria, Germany, and France or in parts of Scandinavia and Spain. Why this should be so is of course the problem of this book. To begin to answer that question, one must know the basic scientific premises on which the prophylactic programs of the 1920s were launched.
Iodine compounds once ingested are broken down and pass into the blood as inorganic iodine (see fig. 2). The thyroid then captures the circulating iodine, joins it onto proteins, and transforms it into the hormone thyroxine, which is stored in the thyroid and released into the blood stream as needed. Thyroxine is essential for optimum growth and for the metabolic processes taking place in tissue. After the hormone has been used, it is broken down and its iodine component recirculated, part of it passing out of the system by way of the kidneys. Iodine lost through this route is known as urinary iodine excretion (UIE),[6] a rate that measures the iodine status of a population. By WHO standards, a population is iodine deficient when its average UIE falls below 50 micrograms (µ) per day. Mass iodine supplementation averaging 150 micrograms per day gradually raises a population's UIE to normal.
Goiter is an enlargement of the thyroid gland, variably manifest as a bulging growth situated at the front of the neck, a diffuse thickening, or an enlargement behind the sternum. The enlargement permits the gland to trap a higher proportion of circulating iodine. Supplementation diminishes the need for trapping and permits glands not too long established to recede to normal size.
In the early days of prophylaxis in Europe, a set of "anthropological" traits were also taken, apart from goiter, as indicators of iodine deficiency. Corporeally, these indicators were short stature, dwarfism, structural peculiarities of the shoulder, hip and foot defects, and a peculiar walk. Facially, they were a broad nose bridge, droopy eyes, and lack of expression. Prevalence of these signs in combination with a conspicuous number of deaf-mutes was taken as a sign of severe iodine deficiency. Severely impaired individuals were known as cretins.[7] Their pathology was seen as separate from but related to endemic goiter, for scientists and laymen had long observed that endemic cretinism was rarely found where goiter was not also endemic.
Fig. 2.
The Thyroid and Its Feedback System
Public health officials in Switzerland, where cretinism was endemic, therefore targeted the iodine supplement at both conditions, while in the United States, where cretinism was not endemic,[8] goiter alone was targeted for eradication. That difference in targets becomes significant in elucidating the obstacles to prophylaxis, for iodine prophylaxis in the United States came to be
associated exclusively with the prevention of goitrous deformities, not with the prevention of motor and sensory disabilities.
As a result of these differing approaches, the essentiality of iodine came to be widely appreciated: in Switzerland, through official public health channels and in the United States, through commercial advertisements for salt. However vaguely, people consuming iodized salt accepted the theory of iodine deficiency.
Except for the Swiss, however, few Europeans were exposed to the theory of iodine deficiency. Endemic goiter nevertheless gradually declined in most of the Western world as food supplies became increasingly delocalized and as iodine entered increasingly into the diet. In other words, neither supplementation nor public education played a significant role for most Europeans in the decline of endemic goiter and cretinism.
Medical publications reflected this decline: once the overt threat of endemic goiter had receded, so did articles focusing on the once-threatening disease. However vividly the theory of iodine deficiency had once been presented on both sides of the Atlantic,[9] the public and its physicians before long came to take iodine sufficiency for granted.
Current Understandings
Basic knowledge on which prophylaxis was established has, over the intervening sixty years, been elaborated into a refined theory and practice that is a powerful agent in managing thyroid disorders (see, e.g., Stanbury 1978). But these advances concern us here in only a limited way: (1) insofar as they promote dietary intervention or cast doubt on it, and (2) insofar as they prepare us to understand the villagers' symptoms and the treatments to which, as we will see in the ethnography, they have been exposed. Four examples will illustrate these advances.
First, concern about the loss of homeostasis has restrained many physicians from endorsing prophylaxis. These physicians were convinced that the sudden introduction of physiological amounts of iodine into individuals long adjusted to a scarcity of iodine might trigger hyperthyroidism (Plummer 1936). This conviction was propounded with much flair during the prophylactic era, so that persistent fears about sudden iodization lingered even after the
idea was disproved. In Europe, the feared phenomenon came to be known as "Basedowification"—hyperthyroidism renamed for Basedow, a nineteenth-century physician who was a militant opponent of iodine supplementation. In his day, supplements were administered on an empirical basis, in doses now known to have been of pharmacological, rather than physiological, magnitudes. Such doses did perhaps prompt pathology. Fear of Basedowification is now uncalled for, however, because, among other reasons, dietary iodine supplement is available only in physiological doses. Yet at least one diagnostic manual recently republished in Spain still cautions physicians about abusive self-dosification (Marañón y Balcells 1984).
Second, the discovery of thyroid stimulating hormone (TSH) strengthened the view that goiter is an anatomical/physiological adaptation that need not be prevented. The adaptationist view holds that TSH, rising in response to low levels of circulating thyroxine, prompts the proliferation of thyroid cells, implying thereby neither dysfunction nor uncontrolled cellular proliferation. TSH does stimulate the thyroid into work hypertrophy and does enable it to trap a higher proportion of circulating iodide; in this sense, it is indeed adaptive. The view fails to take into account, however, that under conditions of optimal iodine intake, rising TSH warns of dysfunction. The adaptationist view also fails to take into account the higher risk of thyroid cancer.
Third, the uneven distribution of goiter, which tends to affect females more than males, has come to be understood in the following way. Estrogens increase during adolescence, rise during pregnancy, fluctuate during menopause, and are exogenously introduced by way of birth control pills. Estrogens increase the binding of iodine, making it less available for organification. Thus, periods of elevated estrogen production in the female life cycle increase the need for iodine and thyroid hormone. Increased levels of TSH reflect this need and may, during these phases of a woman's life cycle, drive the gland into hypertrophy so as to meet the increased demand. This sex difference—where the severity of endemic iodine deficiency is such that the necks of most males appear normal—allows goiter to be seen as a woman's problem rather than a problem of malnutrition that, however variably,[10] affects both
sexes. Observed solely as a woman's problem, goiter seemed to call for therapeutics rather than for massive dietary intervention to correct the underlying environmental deficiency.
Fourth, thyroxine was in 1953 differentiated into two hormones, T3 and T4, differing in potency and in the number of iodine atoms in the molecule (MIT and DIT).[11] Knowledge of the two hormones seemed for a time to make dietary intervention less urgent, for it was observed that under conditions of iodine deficiency, the T3/T4 ratio shifted in favor of T3, the more potent hormone. Animal experiments later disclosed that while T3 does rise compensatorily in most of the body, it does not rise in the brain tissue, where T4, under conditions of suboptimal dietary intake, is already low. In rats, this constellation of hormone levels was accompanied by suboptimal brain function (Greene 1973, Escobar del Rey et al. 1981b ), which improved measurably after supplementation. These animal experiments led researchers to infer that the brain function of clinically symptomless children might also be improved by supplementation.
Indeed, supplementation has been found to increase the level of circulating thyroid hormones in children whose hormone levels were within the so-called normal range (Connolly, Pharoah, and Hetzel 1979). The rise occurred only in subclinical cases, in children free of symptoms who had, however, low levels of hormone. The rise did not occur in children whose hormone levels were normal and whose iodine intake was optimal. These findings suggest that the apathy and low cerebral function attributable to suboptimal hormone levels tend to escape the clinician's notice. Both measures can be improved, however, as was shown when the children's biochemical levels and school performance both rose on supplementation. One can therefore conclude that the hormonal shift preserves corporeal but not cerebral homeostasis. In other words, it protects the body more than the brain (Lancet 1979:1165–1166, 1983:1121–1122), making dietary intervention more urgent. Denying iodine supplements to a population because it is not blatantly goitrous may then be seen as a means of keeping it apathetic and docile. In other words, goitrouslessness should be no reason to withhold iodine prophylaxis, for subclinical thyroxine levels reduce vigor and intelligence (Delong, Robbins, Condliffe 1989).
Other Factors: Goitrogens and Metabolic Error
Western medicine, during the prophylactic era, understood iodine deficiency as the major cause of endemic goiter and cretinism. Since that era it has given increasing prominence to the role of goitrogens and metabolic error.
Goitrogens are any active forces or substances that induce goiter. They act in at least three ways, by affecting (1) the absorption of iodine into the bloodstream, (2) the chemical coupling of MITs and DITs to tyrosene, and (3) the binding of molecules. Goitrogens play an insignificant role in goiter and cretinism where the diet is varied, but where it is not (as in rural Asturias), they can play an extremely important role. In this chapter, I discuss only the goitrogenic mechanisms. In chapter 5, I will show how poverty induces a high goitrogen intake and how a selectively goitrogenous diet, for the physiological reasons given here, helps to keep segments of the population socially marginated.
Absorption is affected by thiocyanate, a substance produced either in the liver or intestine during the course of digesting foods from three plant families.[12] Cassava is of the Euphorbiaceae (formerly Manihot) family, a starchy root widely consumed in the developing world. Cabbage, cauliflower, broccoli, rape seed, kale, collards, and turnips are of the Brassica family, and radish, cress, and mustard are members of the related Crucifera. Foods from these botanical groups are widely consumed in Europe and the temperate parts of the world, sometimes as garnishes and often as daily fare.
Thiocyanate produced by these goitrogenous foods preempts the sites on fatty acids to which iodine ordinarily binds for its passage through the intestinal membranes. Thiocyanate thus impedes the passage of iodine into the circulation and promotes its loss through feces. This loss is insignificant where iodine is abundant, but where it is scarce, thiocyanate slows down hormone production.
Perchlorate is another goitrogen acting in the same preemptive way in the intestine. While abundant in a variety of nuts, perchlorates are especially abundant in chestnuts (L. castanea sativa ), beechnuts, and acorns.[13] In historical Europe, these nuts were considered "hungry foods," consumed as staples of daily fare only dur-
ing war or when grain crops failed. But as will be seen in chapters 5 and 7, they were regularly consumed where grain was habitually scarce.
Goitrins, another form of goitrogen, interfere with the coupling of MIT and DIT molecules. They too may be derived from cruciferous plants, more from turnips than from cabbage, becoming goitrins only in the presence of certain intestinal parasites that arise locally. They may also, as in one well-known case, be derived from volatile compounds of geologic origin. Where because of the prohibitive cost of fuel, only the richer segment of the population boiled its water, driving off these volatile compounds, only the poor became goitrous (Gait'án 1974). Goitrins like these pique the curiosity but play an insignificant role in the global distribution of endemic goiter and cretinism and contribute little to understanding the obstacles to prophylaxis.
Finally, there are mineral goitrogens that, absorbed through drinking water and passed into the bloodstream, act to bind iodine, thus making it less available for organification. The best-known mineral goitrogens are produced in groundwater flowing over bedrock of limestone, where minerals such as calcium and fluorine dissolve out of the rock, enter the water supply, and are ingested with drinking water. Mineral goitrogens like these are characteristic of the central Asturias and of the historical goiter belt of the American Midwest.
Hereditary metabolic error has come to assume, since midcentury, an increasing role in thyroidology and has become an important consideration in the diagnosis and management of goiter. Metabolic errors may impede iodine metabolism at several sites: they may impede the transport of iodine, the coupling and breakdown of molecules, and the recapture of iodine, leading in these several ways to symptoms like those produced by suboptimal iodine intake. While metabolic errors must be seriously considered in any idiopathic case of goiter or of other thyroid-related diseases, they have rarely been shown to play an important role in goiter and cretinism that is endemic. Even where the stage has been set for the concentration of metabolic error in inbred populations, iodine supplements have dramatically reduced the incidence of IDD. However, since popular interest in inbreeding outweighs popular interest in prevention, it serves the interest of the opponents of
prophylaxis to stir up renewed interest in inbreeding, thus distracting attention from prevention.
Supplementation
Determination of appropriate levels of iodine supplementation has frequently posed what might be considered a spurious problem for health officials deliberating over the institution of mass prophylaxis. This is largely because the breadth of the margin of optimal intake—as we saw in the dose response curve—has not been widely appreciated.
Even when mass prophylaxis was initially being tested, iodine supplementation gave generally satisfactory results. It was seen early on as preventing the appearance of goiter in the young; reducing diffuse, hyperplastic goiters; promoting the gestation and birth of normal offspring; and—once supplementation had been under way for the length of a gestation period—halting the addition of endemic cretins and congenitally deaf to the population. Goiters did not, however, recede in those cases where a stimulus to cell growth had been present over a long period.
In cases where goiter was well established and of long duration, supplementation was counterproductive, making some of the older women's hypertrophied glands tender and painful and threatening the possibility of recurring problems. This response made some physicians hesitate to introduce mass prophylaxis, for they feared inducing toxic goiter, an acute and life-threatening form of hyperthyroidism.[14] As a result of such experience, guidelines were developed suggesting that iodine supplements be withheld from goitrous individuals over age forty. Such individuals could be supported with dessicated thyroid or with the synthetic thyroid hormone that became available after midcentury.
Supplementation posed other problems. Mistakes were made in the early prophylactic programs when very goitrous individuals were wrongly offered hope that their goiters would recede. When the goiters, unresponsive to supplementation, did not recede, their bearers were, on occasion, coerced into having them excised under primitive village conditions.[15] It is understandable that women operated on so peremptorily might become apprehensive and resistant when large-scale prophylactic programs were later
undertaken. Memories of such interventions are passed down by word of mouth and produce psychological obstacles that, on the inauguration of new prophylactic campaigns, require sensitive management.[16]
Prophylactic programs were originally aimed at eradicating only goiter and cretinism, since only these were understood as the acute and measurable manifestations of iodine deficiency. The conditions impeding vigor and cerebral function, surmised in those days but not amenable to quantification, were therefore not targeted for eradication. Medical men working in nonsupplemented areas where the incidence of endemic goiter was nevertheless declining measurably, wrongly came to assume that iodine intake was in the optimal range.[17]
Under these circumstances, goiter and thyroid complaints that were brought to the clinic ceased to be viewed as responses to malnutrition. Instead, they came to be seen as "idiopathic" thyroid. At least in Asturias, therefore, thyroid disorders came to be managed surgically, pharmaceutically, or with radiation.[18] But there is little reason to think these invasive practices were peculiar only to this region or to Spain. There is reason to think that, after the decline of endemic goiter in most of the Western world, enlargements of the thyroid came generally to be seen as idiopathic.[19] The idea that, on a global scale, most thyroid disorders are preventable thus gradually faded away.[20]
Disorders Stemming from Iodine Deficiency
Hypothyroidism
In hypothyroidism, too little hormone is produced for the maintenance of ordinary metabolic processes. A woman who is pregnant and hypothyroid runs the risk of giving birth to a cretin. Symptoms of hypothyroidism are morphological, dermal, neural, and behavioral. Facial expression may be dull, and the voice may become hoarse. Swelling occurs around the eyes, and the eyelids droop. Hair becomes sparse, coarse, and dry. The skin, especially on the shins, becomes scaly and thick. Hypothyroidism impairs memory and intellectual function, and apathy takes over. Some patients become psychotic. Hypothyroidism affects the heart, reflexes, and
menses. Anemia may occur due to prolonged and excessive bleeding, or menses may disappear and lead to precocious aging. In biochemical terms, there is a drop in T4, uncompensated by rising T3.
Hypothyroidism is treated with animal or synthetic thyroxine. Treatment runs the risk of side effects and overreactions that tip the body toward hyperthyroidism.
Hyperthyroidism
An overactive thyroid gland is hyperthyroid. Symptoms are diverse: neural, ocular, cardiac, metabolic, and behavioral. Patients may suffer from nervousness, tremors, and insomnia; pressure behind the eyes, spontaneous tears, and photophobia; heat irritation; abnormal sweating; irregular and rapid heartbeat; changes in appetite and weight loss, hyperactivity, and fatigue. Hyperthyroidism if accompanied by fever can lead to psychosis and coma and is therefore life threatening.
On a global scale, hyperthyroidism tends to be secondary to simple goiter, hypothyroidism, and the treatment of these conditions. American medical researchers have found that most of the hyperthyroidism seen in this country, however, is neither iatrogenic nor secondary to simple goiter but immunologic in origin. These findings apply to urban populations whose iodine status, generally good, is the result of a diversified diet.
Patients are tested for T3 and T4 and for radioactive iodine uptake (RAI). Antithyroid agents[21] are given to impair coupling of MIT and DIT and decrease hormone levels. Arriving at the minimal dose that will produce a euthyroid state is difficult and risky, for antithyroid medications have side effects such as nausea and loss of the taste sense and run the risk of inducing hypothyroidism. Radiation and surgery are other treatments for hyperthyroidism, but these are reserved especially for the treatment of goiters that are large or multinodular. Pharmacologic doses of iodine are administered prior to surgery to reduce the vascularity of the thyroid.[22] Goiterectomized patients in the United States are put onto replacement hormone; elsewhere, as in Spain, the remaining portion of the gland is usually expected to maintain adequate hormone production. Because hyperthyroidism often produces hypothyroidism and raises the probability of thyroid cancer, it is standard prac-
tice in the United States, but not always elsewhere, to monitor excised patients. However adaptive a simple goiter may be, its so briefly described complications make goitrousness a serious health hazard.
Incidence
The incidence of goiter, its sequela, and other thyroid conditions is difficult to know, especially in isolated or impoverished areas or where people are unaccustomed to receiving or demanding modern medical service. Incidence is affected by a number of factors. For example, the incidence of hyperthyroidism in populations long free of endemic goiter is low compared to those until recently endemic. At the same time and at a local level, a high incidence of hyperthyroidism may include cases that elsewhere would be separately classified as autoimmunologic conditions.
Traditional classification systems make it difficult to assess the incidence of thyroid disorders stemming from iodine deficiency. The conventions of international nomenclature have not combined the disorders under a single rubric that signals their common cause. The term iodine deficiency disorders (IDD) has been proposed to fill this need (Lancet 1983:1165), but as of 1988, no medical data system, such as MESH or ICD, had used the term. Hyperthyroidism is tallied on one list, toxic coma on another,[23] and cretinism on yet another. In the absence of a unifying concept, the incidence of IDD as evidenced by these symptoms alone or in combination will—as it was for this investigator in a modern Spanish village—remain difficult to ascertain.
Cretinism: The Transgenerational Effect of Hypothyroidism
Cretinism results from a deficiency of thyroid hormone during gestation. It is caused by an inadequate maternal intake of iodine or an enzymatic defect in the infant. Cretinism becomes apparent during the first year of life and is manifested in stunted growth and intellect. Endemic cretinism occurs in areas of endemic iodine deficiency; when it occurs otherwise—in areas not known to be deficient in iodine—it is attributed to the presence of a defective
enzyme and is called sporadic cretinism. While the causes are different, the outcomes can be so similar as to be viewed under the single concept of congenital hypothyroidism.
Endemic cretinism is the result of a sequence of processes: the levels of estrogen and iodine binding proteins rise rapidly in a woman who has recently conceived, on occasion the demand rising so high as to shift a nongoitrous euthyroid woman into hypothyroidism during the first eleven weeks of gestation. In that event, the gestating fetus is deprived of thyroid hormone, for during this early part of development he is totally dependent on maternal hormone. Since critical development events ordinarily take place during this period, the organism's deprivation of thyroid hormone at this time adversely affects its eventual neurological and intellectual capacity (Fierro-Benitez 1968; Hetzel 1989, chaps. 3 and 6).
The exact sequences and timing of these developmental events are difficult to pinpoint in humans, but the implications of hormone deprivation can be inferred from rats made hypothyroid in the laboratory. The neural tissue and development of the myelin sheath of the offspring of hypothyroid mother rats are poor, so that their nerve impulses are slowed down and the potential complexity of perceptual and behavioral responses is reduced. In rats, these failures and developmental delays cannot be compensated by introducing exogenous hormone after the fourteenth postnatal day.
The developmental agenda for humans is different. After the twelfth week, the human fetus begins to produce its own hormone, but adequate production depends on the availability of unbound iodine in the shared bloodstream of mother and fetus. While the exact timing is unknown, a limit presumably exists for humans also, after which muscular coordination and learning ability are forever impaired.
Natural experiments have suggested what that agenda may be. An iodized oil injection received by a woman before she conceives has been found to protect her offspring from iodine deficiency during his uterine phase, thus protecting him from endemic cretinism. By contrast, the newborn with an uncompensated enzymatic defect who becomes cretinous has obtained the benefits of maternal hormone during the critical period of nerve development. He has lacked it only during the latter phase of gestation, when he is dependent on his own hormone production. Postnatal introduction
of exogenous hormone effectively reverses his enxyme defect and permits recovery from the developmental delay if treatment is begun promptly and sustained for life.[24]
Developmental deficiencies may be compounded by postnatal sociogenic brain damage (Montagu 1972). Since the hypothyroid infant is relatively unresponsive to most stimuli and elicits fewer social interactions, he is predisposed to this additional kind of brain damage.
Paradoxically, then, and contrary to popular belief, the congenital hypothyroidism of the endemic cretin is not genetic, while genetic defect does characterize the sporadic cretin whose heredity the public rarely calls into question. This irony has implications for mass screening and prophylaxis, as will be seen in chapter 7.
It is a mistake to believe that endemic cretinism is hereditary. It is also a mistake to believe that the most common thyroid disorders are idiopathic or autoimmunologic in origin. These mistaken beliefs, operative until very recently in a modern industrialized nation and probably still operative in many parts of the world, pose an obstacle to prophylaxis, for they wrongly classify most of the world's thyroid disorders into categories of disease that have little to gain from dietary intervention.
Conclusion
I began by elucidating the theory of trace elements and describing the iodine cycle. The movement of iodine was traced through the body to show the pathological effects resulting from iodine deficiency and the ingestion of goitrogens. Disorders like hypothyroidism, hyperthyroidism, motor and cerebral defects, and cretinism were traced to underlying iodine deficiency. Attention was drawn to the historical difficulties in recognizing the common denominator of these iodine deficiency disorders and in recognizing that, on a global scale, they represent the greatest proportion of thyroid disease. IDD, like other kinds of deficiency disease, can be dealt with effectively only if it can first be seen to exist in relation to a set of contexts that are historical, social, and political. These will now be examined.
Chapter Three
Diet and Image in Asturias
Introduction
The formation of a particular attitude—especially toward rural people—itself poses an obstacle to prophylaxis. The attitude is grounded in the geology, landscape, and history of the region and in the history of the nation of which that region forms a part. At the center of that attitude is the disrepute of Asturian mountain-dwelling villagers. Disrepute produces defensiveness in these rural Asturians and prejudice in outsiders and contributes to the inaction that is our concern. The logic of that inaction seems to argue that a people who are backward and ill formed and whose speech is peculiar must be essentially inferior. An inferior people, it seems to follow, cannot benefit from dietary intervention. It is difficult to prove such a logic of inaction, but by reviewing the history of Asturias in terms of the interplay of diet and image, the reader will be persuaded, I believe, to consider such logic one of a number of obstacles to prophylaxis. Though the focus here is on mountain-dwelling Asturians, we know that many of these attitudes, toward what Marx called "the idiocy of rural life," are very widespread.
The chapter is divided into four parts. The first gives a historical overview of the community and region in narrative form so that the reader unfamiliar with rural mountain settlements in Asturias may rapidly get a feeling for Escobines, the focal village in which my questions regarding the persistence of endemic goiter and cretinism arose. This part is an overview of the interactive consequences of isolation and sporadic integration into the larger pro-
vincial and national context. The second part describes the physical environment, the region's early history, and the formation of a mountain identity, as that identity interacts with stereotypic images created by outsiders. The third part shows the dietary aspects of stagnation in the countryside, relative to the ascendancy of urbanized and modern Spain. The fourth part reviews Spanish twentieth-century history in terms of events affecting the diet.
Character and Caricature: Isolation and Sporadic Integration
We turn now to the focal village in which, until the 1980s, endemic iodine deficiency disorders were officially ignored. The landscape and lifeway of these villagers resembles that of other communities, similarly afflicted, whose characteristic is a general state of isolation coupled with sporadic contacts with cosmopolitan centers. The isolation of such communities contributes in many ways to a special sense of local character, which the sporadic contact serves to caricature.
On the rainy northern slopes of the Cantabrian range that runs close to and parallels the northern coast of Spain live mountain people who for centuries have tended small stock and small native cattle and cultivated small dispersed plots of land primarily dedicated to spelt wheat. Once New World cultigens found root and acceptance in Spain, these mountain villagers dedicated increasingly larger fractions of land to the cultivation of corn and potatoes. The villagers also foraged for chestnuts, walnuts, and hazelnuts to supplement their diet and for beechnuts as a last resort in very hard times.
Among the higher lying of the mountain villages is Escobines,[1] named for the escoba, yellow flowering broom, that proliferates on steep slopes where soil is too thin for either forest or pasture. Limestone outcroppings serpentine here from slope to slope. Escobinos[2] had at their disposal relatively little cultivable land and therefore dedicated themselves primarily to raising livestock. By contrast, the lowland Asturians, residing on flatter land and closer to the tempering coast, dedicated larger proportions of their land to the cultivation of grain.
People dwelling farther down from the mountain divide,
whether on the north-facing Asturian slopes or on the south-facing ones of Castile, viewed it as a formidable barrier (see fig. 13). But for the villagers residing high on its flanks, the divide was a point of contact. From time to time, ox carts or mule trains moved between the high plains of Castile and the upland villages. Forest and animal products, and a few surplus animals, were traded for things produced more easily on the other side: blankets and ceramics, wine, oil, and grain. This trade, above all, permitted Escobinos to survive when their own cereal crops failed—for very wet, cold years or an occasional drought could wipe out entire harvests. It was then that Escobinos went to Castile to trade for the only affordable supplement, bran, bringing it home on their own or their donkeys' backs. The wealthier villagers, in fact, came to rely on Castilian grain as a regular supplement.
Trade was not the villagers' only contact with the outside world. Their intimate knowledge of the passes brought them into contact with pilgrims and aristocrats. Pilgrims were of such importance to the state that a royal charter of the late Middle Ages decreed that, in exchange for guiding pilgrims and other travelers toward religious shrines and markets in lowland Asturias, the men of this and other high-lying villages adjacent to mountain passes should be exempt from military service. Aristocrats journeyed to the village from time to time to hunt boar, bear, chamois, and fallow deer and to fish for trout and salmon. They employed village men as guides, continuing this practice through the early decades of this century. And when, at the turn of the century, a hunting lodge was built in the village, they employed village women as servants. The villagers were thus not entirely isolated from foreigners or the aristocratic classes. While marriage partners were usually found within the confines of the parish, the exchange of goods and services with outsiders meant that spouses and genes were occasionally introduced from elsewhere.
Snow water, rushing streams, and narrow defiles kept mountain villagers relatively remote, however, from the majority of Asturian country people and their landed overseers. Escobinos who served as guides to foreigners and aristocrats were said to be less deferent than the lowlanders who, as tenant farmers on large but scattered estates, were more subject to the propertied classes. Perhaps it was this lack of obsequiousness that gave Escobinos the reputation for
being rustic and hearty but at the same time foolish. Tinged with a jocular appreciation for this rustic quality, they had about them also an aura of disrepute.
The relative isolation of Escobines broke down in the twentieth century. A road from below was constructed through the village early in the century, increasing contact between lowlanders and highlanders and intensifying occasions for mocking, even disparaging, comparison. By 1930, the road was extended up over the pass connecting central Asturias with Castile. But little traffic moved along it at first, for pedestrians and vehicles were few. The Civil War changed that considerably, however, with the movement of Republican and Nationalist troops as they struggled for control of the pass directly above the village. The Nationalists triumphed locally in 1937 and strung a telephone line to communicate with their superiors. But it was taken down in 1939 when the war was over.
Only in the 1970s was a telephone installed again in Escobines, this time hung on the wall of the most centrally located of the village's thirteen bars.[3] Villagers greeted its installation with relief: "Our abandonment is over!"[4] This sense of abandonment expressed a social feeling more than fact, for since the end of the nineteenth century, schoolteachers assigned by the national government had succeeded in "alphabetizing" most villagers. Moreover, as villagers participated during the nineteenth century and early twentieth century (if not before) in the great labor migrations to America, they were improving on their rudimentary education. Escobinos, when they did not remain abroad permanently (see genealogies, chap. 4), spent years or decades in the New World before returning home. A second wave of migration, to the industrial centers of Europe, took place during the 1960s. Brief as this wave was, it expanded the experiential base of villagers and raised their expectation. Thus, for a century or more, Escobinos have experienced a tension between mountain isolation and sporadic cosmopolitanism.
The governments of the twentieth century also provided villagers with medical personnel: the practicante, trained to make regular rounds, deliver primary care, and give injections,[5] and the médico titular, a state-paid physician officially appointed to serve in particularly remote areas. The practicante made his village rounds twice a week, while villagers called on the physician, usu-
ally residing in a town fifteen winding kilometers downstream, only in times of dire need. When, in the late 1970s, partly under the impetus of newly elected Asturian Socialists, Escobinos formed a neighborhood association, they constructed as their first project a consultation room, believing it would attract the médico titular to hold regular consultations in the village. Similar projects were at that time under way in other villages. These initiatives show how eagerly the mountain people sought the benefits of modern medicine.
Neither the teachers nor medical personnel were ever natives of the parish or of other mountainous parts of Asturias. The parish priest, by contrast, was usually of local or native Asturian mountain stock and resided in the small parish seat, El Texu (pop. 200), a kilometer away from Escobines. The native/nonnative distinctions reflect pervasive spatial-social concerns. Villagers used to exclaim of the priest, "How can such a local one be better than one of us!" And Escobinas deciding whether to undertake a journey to see the doctor would ask, "How can I approach a stranger with such a problem as I've got?" The remarks reveal attitudes of familiarity and foreignness that posed indirect obstacles to prophylaxis.
Today, frequent and regular contact with the urban and industrial world is easing the distinction between insider and outsider. Escobinos began after mid-twentieth century to augment their subsistence incomes with wages earned in the large-scale coal mines downriver. These had opened in the nineteenth century, but until daily transportation between mine and village became available, few Escobinos entered them. Those who did so became mixed workers. Families then allocated their labor resources to diversify income, so that by the 1970s incomes came to be derived from land (subsistence and livestock), wages (mining and construction), small industry (sawmill, fish hatchery, needlework), and tourism.
The latter sector, tourism, expanded when in the 1970s the Spanish middle class, and later also the working class, obtained access to the automobile. In the same decade, several bars and a dance hall, which had been serving the local people for several generations, expanded and multiplied into banquet facilities, hotels, and coffee shops serving wedding parties, tourists, and skiers. In this regard, Escobines is to be distinguished from most other
Asturian mountain villages. Just as its proximity to the pass had for centuries given it a certain access to the world, so proximity to the newly built summer hotels and winter ski area gave Escobines a special worldliness.
Twentieth-century change thus came to Escobines in several ways: the highway, the war and its aftermath, black marketeering, entry into mines, a consolidated school and school buses, television, and—most important for this discussion—a gradual shift from subsistence cropping to dependence on three Spanish staples, wine, bread, and oil, which had to be imported from elsewhere. Pharmaceuticals, whether prescribed or over-the-counter, were found in every home by the 1960s. Likewise, industrially produced foods and supplements, such as industrially formulated mothers' milk substitutes, entered the Escobino diet. A measure of this change is that the larger infants born to today's Escobinas no longer fit into the tiny cribs of traditional times (R. L. Fernandez 1980).
Changes were most apparent within the well-nucleated village. For example, tourist vehicles arrived in such numbers on weekends that in 1984 the parking problem was put on the agenda of the Neighborhood Association.
Continuities were more visible in the fields. On any dry autumn day, the potatoes were still being harvested by family groups, for families remained the primary unit of production and consumption. Pumpkins were still carried in from the fields, for their fiber was still an essential ingredient in the blood sausage made from the family pig. As before, cabbages continued to mark the perimeter of the family's plow land. In other words, people still depended heavily on food grown in their own fields, grown locally on soil long leached of its iodine.
This rural scene describes the landscape of high mountain isolation and the historic context of sporadic outside contact in which goiter and cretinism, IDD, became endemic, persisted, and gradually declined after mid-century. In 1984, prophylaxis was begun, lowering the incidence of IDD (Aranda Regules et al. 1986). But it is still prevalent in the older generations, and goiter and cretinism now embarrass the villagers more than formerly, when they were more isolated and could ignore outsiders' caricatures. Their recent, rapid adoption of pharmaceuticals and industrially produced infant milks demonstrates that it is not, at least since mid-
century, their resistance to modern medicine or costly nutritional supplements that was the obstacle to prophylaxis.
Environment and Identity
Physical Description
We will see how Asturias, the region in which Escobines is located, resembles the terrains where endemic iodine deficiency was typically found. It is a mountain enclave located on the northern coast of the Iberian Peninsula, facing the Bay of Biscay. The enclave's natural obstacles make approach difficult from all sides but particularly from the south, where high mountains divide Asturias from Castile—for many centuries, as now, the dominant administrative center of Spain. Asturias is bounded on the north by seaside cliffs offering few harbors, on the east and west by rapidly descending streams, and on the south by the Cantabrian range. The region's highest peaks, exceeding 2,600 meters, are concentrated in central and eastern Asturias. Visible from the sea, their perennial snowfields prompted ancient mariners, rounding into the Bay of Biscay from the Atlantic, to call them the Peaks of Europe. They were, after all, the first harbingers of Europe beyond. But for Asturias, they were formidable guardians of a region difficult of access.
Both the mountainous topography and the presence of the Castilian plain to the south modify the region's Atlantic climate. Low pressure in the interior creates summer thermal updrafts, sucking the prevailing northwesterly up the mountain slopes where, on cooling, its Atlantic moisture precipitates. Fog and rain occur at all seasons, averaging annually 1,400 millimeters of precipitation. Departures from this central tendency can cause both severe droughts and flooding anywhere in the province, whether in the coastal lands, the central valleys of midprovince, or in the mountainous zone where this study is situated.
Topography varies the rule "higher elevation, higher rainfall": precipitation is greater at relatively low elevations in valleys that are funnel shaped or in the higher reaches of mountain valleys, such as the one in which Escobines lies. Minimal variation in temperature occurs in the coastal zone, rarely falling outside a range
of 10 to 18 degrees Centigrade. Inland, the rising elevation increases the range of temperature.
The geologic factor most frequently associated with endemic iodine deficiency is limestone, which forms the bedrock of the mountainous parts of central and eastern Asturias. Heavy precipitation in combination with carbonic acid—applied by the oceanic atmosphere and compounded by the abundant Asturian vegetation—operate to dissolve the Asturian limestone. This gives rise to exposed karst formations, perforated bedrock, and caves. The latter testify to the intensive leaching process that does not present itself to the eye but is occurring in the soil, loading groundwater with goitrogenous minerals. Leaching was so intensified by glaciation that in high-lying parishes of central Asturias, such as the one in which Escobines is situated, groundwater was as low in iodine (Bootello 1934, 1935; Vivanco et al. 1972) as that of the endemic areas in the Swiss Alps.[6]
Asturias also resembles Switzerland geographically in terms of its vegetation, distribution of population, and industry. Its primeval forest has been replaced by plowed bottomlands and brows of hills, grassy slopes, and scrub where slopes are too steep to sustain meadow. Two Asturian coastal cities (Gijón and Aviles) and inland Oviedo, the capital of the province, form in the central lowlands a heavily urbanized triangle from which heavy industry and its supporting populations stretch up the Caudal, Nalón, and Lena rivers.
Half the Asturian population is still dispersed in hamlets, villages, and small towns, wherever pastoral activity, cultivation, and commerce can be sustained. In 1970, when the total population of the province was 1,045,000 with a density of 99 per square kilometer, the population appeared intensively rural, though only 21 percent of it was even then active in agriculture. Spain's entry into the European Common Market in 1986 has lowered that percentage, for participation in that market diminished Asturians' already modest agricultural incomes.[7]
Defamatory Images: Diet and Stature
No archaeological evidence, skeletal[8] or otherwise,[9] suggests that Paleolithic or Mesolithic inhabitants of Asturias were afflicted with
IDD. These early people were hunters and foragers, consuming an important part of their diet from the top of the food chain where iodine is concentrated. Game diminished and population increased as time went on, driving people increasingly to search out marine resources. Middens dating from the postglacial period demonstrate the importance of iodine-rich seafood in the later prehistoric Asturian diet.[10]
Stone Age inhabitants of Asturias probably never lived in total isolation, in strictly inbred commonities, for Neolithic Asturian peoples had extramountain contacts. Cache shrines found in the high mountain passes indicate that peoples from the central plateau of Spain and this mountain enclave maintained at least occasional contact with each other.
Hints of dietary stress, and a preview of the defamatory images to come, begin to appear when Asturians are first mentioned in history. The Greco-Roman geographer Strabo (63 B.C.–A.D. 24) reports that tribal peoples known as Asturians (Astures) and Cantabrians (Cántabros) lived in the northern Iberian Peninsula where they resided in rustic stone settlements and hunted, fished, and kept small livestock for milk. They consumed—apart from foods of animal origin—acorns, beechnuts, and chestnuts, grinding them in stone mortars and cooking them into porridge.
We are concerned with the principal carbohydrate of these protohistoric people because, as we know from chapter 2, acorns and other nuts are goitrogenous. Strabo, while mentioning no disease afflicting these Asturians, does contrast the fine fettle of the men, "stocky, well built, and agile," with "the small stature and unattractiveness" of the women.[11] It is, of course, speculative to ask if Strabo's description meant that the women observed by his explorers were hypothyroid and goitrous. Still, as hunters, men tended to range more widely and find themselves at a distance from the mortars and pestles where the vegetal staple was prepared. This would mean that men, more frequently than the women of Asturias, consumed food from the top of the food chain where iodine is concentrated. Women, already more physiologically vulnerable to iodine deficiency, were likely to depend more on what they could gather close to home, consuming fewer foods rich in iodine and also taking in more goitrogens. Under these circumstances, even without cultural rules enforcing different diets
on men and women, the necks of women were likely to be thick and unattractive, sometimes with nodulated goiter. A pathogenic possibility in the division of labor could thus have been the source of Strabo's remark—the vitality of the men, contrasted with the small stature and deformity of the women.
The social image of Asturians that Strabo conveys concerns us here as well. He introduces tribal Asturians to the civilized world as "worse than barbarians."[12] It cannot surprise us that men beginning to be confronted by imperial power—as the Asturians reported on by Strabo were then being confronted by Romans—are portrayed as volatile and fierce and thus as worthy opponents. Their women, in the same imperial vein, are presented as barbarians falling below the observer's disdain and therefore as justifiable objects of colonization. The same contrasting set of observations has frequently enough appeared in colonialist literature pertaining to other peoples.
What underscores Strabo's disdain is the food reported to be habitually consumed by these northerners: porridge. Romans considered the consumption of leavened bread as the defining characteristic of civilized people. Culinary habits and taste, to Roman eyes, condemn these Asturian people. Asturians would only be seen as civilized when they, too—abiding by the "civilized standards" of their observers—were to habitually consume wheaten bread. For many Asturians, as we shall see, this did not become possible until the twentieth century. Hence their food habits acted for the next two millennia as a libel on their image, stereotyping them as "porridge eaters" and haunting them well into the twentieth century.
Recent archaeological excavations corroborate Strabo insofar as handmills for processing acorns and other nuts have been found (Martinez Fernández y J. Manuel Junceda 1969: 119–130), suggesting the central importance of these wild foods and hence the consumption of goitrogens. Given the nature of the lifeway and milieu, this could mean that protohistoric Asturian people were experiencing endemic IDD.
The subsequent image in the literature portrays Asturians as resisting both the Roman invasion and the Roman civilization. The image pits the widely dispersed tribal Asturians against the Romans who sought to concentrate them into urban villas, the ideal
and most local administrative expression of Roman law, hierarchy, and order. The image of that struggle pits peoples whose economy is a combination of foraging, pastoralism, and hoe cultivation against those fully committed to the plow, to grain agriculture, and above all to "civilized" standards of communication.
Defamatory Images: Language
The history of the Latin language, brought by the Romans to Iberia, also has much to do with the disrepute of rural Asturians who speak an uncouth vernacular. While its telling leaps ahead of our chronology, it must be told now. It involves a struggle between the speakers of Romance, the family name for the languages evolved out of Latin. The struggle pits a "disreputable" (Romance) language, Asturiano or Bable, against an ascendant (Romance) language, Castilian.
In northern Spain, and in Asturias in particular, Latin evolved into Astur-Leonés, the language of the Spanish court for several centuries in the early Reconquest period. Until the Middle Ages, Astur-Leonés was also the vernacular on the central plateau, where it was eventually replaced by Castilian. In time, Castilian became the official and academic language of all Spain, but in the mountains of Asturias, the old vernacular, Astur-Leonés, resisted Castilianization (Menéndez Pidal 1950, 1962) and evolved into what is now known as Asturiano. Indeed, Asturiano came to be called Bable (babble), or los bables, because of the difference from valley to valley which had evolved in the orally transmitted language. Roman deprecation thus gave way to Castilian deprecation.
This deprecation became official when schoolteachers in rural areas during the last century, often enough Asturian themselves but oriented toward the Castilian language by training and having few criteria by which to distinguish defect from dialect, came wrongly to associate the two.[13] They simply shamed all youngsters who, for whatever reason, persisted in the use of or regressed to using any form of the vernacular. The children came quite readily to adopt these "learned" attitudes and to see themselves as somehow disabled or thick-headed and their speech as an impediment. This, presumably, was one of the main processes by which rural Asturians came to feel themselves embarrassed or despised for
speaking the lingering old Romance dialect of the countryside, a language, ironically, that was once that of the Spanish court.
Only in the post-Franco years, from 1975 on, is this linguistic deprecation beginning to recede under the stimulus of Asturian intellectuals who, in tracing Bable back through Astur-Leonés to the Latin the Romans had left behind, are setting the linguistic record straight. Along with many speakers of Asturiano, they have rejected the pervasive and harmful view, often perpetuated in educational circles, that Asturiano is only a deformation of Castilian. And they have themselves sought to revitalize the language and encourage its widespread use as a fully expressive vehicle of native intelligence.
In one respect, this achievement is not unlike what is just beginning to happen in the mid-1980s with IDD. What was regarded as a "deformed" language, when traced to its historical antecedents, becomes demystified. Shown to be a fully respectable product of normal language evolution, the oppressive feelings associated with its use are lifted. IDD is likewise becoming demystified; the deformities and defects associated with it are coming to be seen as the natural outcome of a particular ecology and ceasing to be considered expressions of innate inferiority. As in the case of Bable, the onus is thereby taken off the victim.
The Sense of Abandonment
The Roman administration in time withdrew from Iberia, but the Romans remained, affecting administrative structures, law, language, and religion. Thus, when Visigoths from the northeast invaded the peninsula, they were introduced to Christianity, which they embraced. When subsequently, in the eighth century, Moors from North Africa invaded, the Visigoths retreated to the north. There, in the Christian redoubt of Asturias, they regrouped on the northern flanks of the Peaks of Europe in Covadonga and did battle against the Moors. The first victory, against the until then unstoppable troops of Mohammed, occurred in Asturias, in Covadonga, in 718, the date that marks the beginning of the expulsion of the Moors. Covadonga became an important religious shrine and its matrix, Asturias, the seat of the "divine mission"[14] —the Spanish Reconquest—that lasted seven centuries. The role of As-
turians in the expulsion of the Moors is locally celebrated and evokes a sense of glory. Although the Kingdom of Asturias persisted as the center of the Reconquest for several centuries, eventually, as the Moors retreated south, the court shifted over the mountains into León and Castile. This removal evokes a sense of abandonment; it meant that for centuries to come, Asturias lay "isolated behind its mountains, marginated and legendary, playing no significant role in the affairs of Spain" (Ruiz de la Peña 1970:108).
This abandonist view has been promulgated by generations of historians and reflected in official textbooks so that Spaniards in general but especially the mountain-dwelling Asturian villagers have assimilated it—wryly deploring their destiny and reiterating somos abandonados ("we are abandoned").[15] It is an image both of victory over repression and subsequent margination, and that image weighs on Asturians.[16]
The weight of that image can be seen in a curious reversal of meanings. Once they had expelled the Moors from their mountain enclave, most Asturians returned to their small plots of rural land to herd and cultivate, leaving further military action to those who would pursue the Moors beyond the Cantabrian range and receive title to broadly cultivable land regained from them.
These Asturians, rejecting the pursuit of landed estates, came to view themselves as desinteresados, materially disinterested people. Elsewhere, however, and over time, this disinterest was differently interpreted; it came to be seen as a defect, as slow and lacking in enterprise.
Likewise, the honorific Spanish title hidalgo (hijo de algo : son of something) obtained over centuries in Asturias a significantly different connotation from the rest of Spain. On the southern side of the Cantabrian range, the title was reserved for those who, as a reward for heroism in battle, were granted wealth and status. Near the western Pyrenees, the title was, for political reasons, accorded to everyone born in the Basque country (Greenwood 1977).[17] In Asturias, the term was accorded to every man—and his descendant—who had played a part in the initial expulsion of the Moors. In other words, ordinary Asturians for legendary-historical reasons had a claim to the title, and through this generalization, the term in Asturias lost its distinction and even become associated with an impoverished condition. In Asturias, hidalgo could thus come to
mean "landless" and was, among other things, used ironically to designate transhumant herders such as the Vaqueiros of western Asturias who passed over other peoples' properties and common land. Among otherwise sedentary Asturians, they formed an often marginated underclass treated in some valleys as socially inferior.[18] Often enough, and ironically, the creation of stock types by the literati of Madrid helped to visit such prejudicial attitudes upon provincials in general. In this process, Asturians came to be portrayed as boastful, impoverished, and closeminded.[19]
Consonant with historical and geographic realities, Asturias in the fourteenth century, was granted the title of Principality. Arguably a disguise for official neglect and a gesture to the sense of abandonment, the title accorded a certain provincial if not administrative autonomy to the region. This autarchia (autarchy) added to the emphasis on local orientation, jurisdiction, and provisioning. In a roundabout way, it contributed to the sense of abandonment.
Autarchy could never be complete in such a mountainous enclave with such a limited spectrum of cultigens, for vital necessities such as Portuguese solar salt—required in the humid Asturian climate to preserve meat, fish, cheese, and butter—were imported. Salt, along with a few luxuries largely destined for aristocrats, monastics, and the emerging gentry, came by ship into one of the few safe ports on the Asturian coast (González García 1972)[20] or by ox cart and mule train over difficult mountain passes. Scanty amounts of oil, wheat, and wine also came through these points of entry, creating a dual diet that regularly supplemented the diets of the elite but rarely those of ordinary people.
Pilgrims making their way to the holy shrine of Santiago de Compostela near the northwestern Iberian coast also, because of problems of provisioning, left Asturias largely alone. Much as Asturians tried especially to encourage their visitation, the topographic and hydrographic hazards of Asturias, combined with problems of provisioning, made the pilgrimage route from France through Asturias the road less frequently traveled to Santiago, except perhaps in winter when snow and bitter winds blew over the central plateau.
Pilgrims had reason to hesitate before entering the region. For while in the era of mass pilgrimages the diet of most Europeans consisted almost exclusively of grain (Bernard 1975: 40), grain was
known to be scarce in Asturias, and expensive. Hence, since the chartered markets were also few, Asturias was for foreigners a poor and risky land through which to venture.[21]
Si baxas a Ribeira
Lleva pan na faltriqueira
Y si pasas por Merou
Lleva pan de tou
If going by way of Ribeira
Take bread along with you
Take all that's essential
If going by way of Merou.
Land fragmentation, caused not only by highly accidented topography but also by divergent inheritance practices, compounded the impression of Asturian poverty and neglect. These practices favored the accumulation of small, discontiguous parcels of land by crown, church, aristocracy, and a growing number of gentry. Those who cultivated the land and tended livestock were tenants or sharecroppers whose holdings were themselves composed of small dispersed parcels. They paid their rents in grain, the scarce and vital commodity.
The dietary implications of this servitude in grain were severe. The only acceptable grain for payment in kind was escanda (triticum spelta ), a low-yielding spelt wheat suited to the thin soil, heavy rains, cool conditions, and covered sky of Asturias. The grain was laborious to grow, harvest, and mill, having to be planted in the damp cold of late autumn so as to germinate over the winter and be harvested in late summer.[22] It had to be laboriously pulled off the stalk because of the fragile rachis and required burning of the chaff and double milling because of the tight attachment of husk to kernel. It also necessitated storage off the ground in chambers set on top of stilts as protection from rats and pervasive humidity. But even such storage necessitated periodic removal and airing to keep it free of dangerous molds. Escanda was not a dependable foodstuff by which to satisfy the obligations of tenancy, and "payment" of that obligation in such currency threatened the well-being of the Asturian countryman. It certainly did not provide the surplus by which to feed a regular flow of pilgrims.
New Cultigens, a New Dietary Deficiency, and a Negative Image
It is hardly surprising that maize (corn) from the New World found favor in Asturias, taking hold as early as anywhere in Europe.[23] Its proliferation throughout the seventeenth century led to a dietary disease, pellagra, that compounded the already existing negative image of rural Asturians. More important, the decline of pellagra in Asturias and elsewhere holds instructive parallels to the decline of IDD.
The popularity of corn, in comparison to spelt wheat, depended on its yielding far more calories per unit of land, raising the land's carrying capacity. Propertied classes therefore promoted the cultivation of corn by their tenants but continued to accept as payment in kind only the preferred escanda. This intensified the dietary dualism, which did not recede from parts of Asturias until late in the nineteenth century.
That dualization meant wheat and leavened bread for the rich, corn for the poor. Corn was unleavenable and consumed largely as porridge or borona, a heavy loaf.[24] For the poor, this meant the loss of niacin, an essential dietary element that is abundant in wheat and scarce in corn. A niacin-deficient diet, when the rest of the diet is also poor in foods of animal origin (which contain precursors of niacin),[25] results in pellagra, a systemic disease characterized by varied symptoms: diarrhea, dermatitis, dementia, and death (known as the four Ds). Pellagra's symptoms are so varied that for a long time they were not understood as the several aspects of a single disease, in the same way that the many manifestations of IDD are not yet broadly recognized as stemming from a single deficiency (ICD 1979).
People residing in widely dispersed rural pockets of poverty in Europe throughout the eighteenth century came to experience pellagra's four symptoms in ever-increasing number, and Asturians—especially those residing in the most arable, densely settled areas close to the provincial capital—were particularly affected. New symptoms appearing in widely separated parts of Europe brought forth a variety of names, often with negative associations. But it was in Asturias where the disease was first identified.
The dermal condition in Asturias was known primarily as the "sickness of the rose" (mal de la rosa ), or "Casal's necklace," for the color and form taken by its eruptions resembling rosary beads worn around the neck. The proper name refers to Dr. Gaspar Casal, a Spanish (Catalan) physician of the eighteenth century who was practicing in Asturias. He was the first physician to methodically seek the vector suspected of causing pellagra. Though there was no vector to be found,[26] he did demonstrate the heretofore unrelated symptoms to be phased progressions of a single disease. He also drew attention to the dietary connection, pointing out that pellagra was found almost exclusively among the maize-eating poor.
Though unable to find any vector in corn, Casal was able to demonstrate that a diet rich in foods of animal origin, to which only the elite had access, diminished the symptoms. These findings were presented by proxy in 1755 to the Parisian Medical Society, which was then the center of the emerging biomedical community. Their presentation in such a respected setting brought Casal much acclaim (Marañón 1959).[27] Casal's newly discovered disease also came to be known as "the Asturian leprosy," a name suggesting a region rampant with poverty, disease, and dementia and so depicted in a well-known French painting of the period.[28]
This image proved to be so painfully persistent that Roël, an Asturian patriot of the late nineteenth century and also a physician of national prominence, concerned himself less with eradicating the disease than with denying its image:
Asturias is no longer rampant with pellagra. It is no longer a miserable place . . . where people huddle in dark crowded huts. It is no longer the site of the infamous Asturian leprosy where skin boils up and flakes off, and where people wander around demented. (Roël, cited in Fernández-Ruiz 1965:75).[29]
By ignoring pellagra's actual incidence, Roël gave a preview of what was to be the response, decades later, of other Asturian physicians to another disease, IDD.
The image of Asturian "leprosy" might not have been so painful had the dietary implications of the medical breakthrough been more clearly recognized in Spain. Casal had postulated that pellagra was a natural phenomenon—not, as was then widely be-
lieved, a divine affliction[30] —that under similar conditions could occur elsewhere. He went on to demonstrate that pellagra's symptoms developed progressively, usually under specific social and dietary conditions that could be remedied. The recognition he acquired in Spain did not, however, rest on these findings with their very practical implications but on the status accorded him in international medical circles. His prestige did not have practical consequences in Asturias, and the Asturian pellagrin's diet remained unchanged and his affliction unrelieved.
In France, Casal's findings set the stage for the enaction of dietary policies that brought wheat at state-controlled prices to the poor in even the most remote areas, extinguishing pellagra by mid-nineteenth century in the French countryside. In Spain, pellagra declined later and only slowly as a consequence of changes that gradually affected the rural economic order, so that in 1890, notwithstanding Roël's vehement denial, it had still not disappeared.[31]
Plow, Spade, and Livestock
The Spanish Enlightenment of the late eighteenth and early nineteenth centuries inaugurated a period of transition in which Asturias lost its special autonomous status as a principality. In the nineteenth century, the province began to industrialize, to put its landholding practices under critical scrutiny, and came under the command of the centralized government. All these changes affected the Asturian diet.
Transfer of cultivable land in Asturias was traditionally entailed, restricting it to a specified set of heirs, usually within the church or aristocracy. Entailment meant that small cultivators rarely became owners of arable land. Disentailment, desamortización , was therefore enacted to serve the Enlightenment's social and economic, that is, entrepreneurial, goals. Disentailment was expected to turn cultivators into landowners who, at last able to make a profit from the land, would make efforts to increase production so as to have a surplus to bring to market. Regionally produced foodstuffs sold in markets would, in turn, free other men to go into industry. Enlightened thinkers opined that without increasing the volume of foodstuffs grown in Asturias, no industrial development could get under way.
The anticipated benefits were slow to be realized, however. In the disentailment of the 1830s and 1840s, either newly rich Asturians back from the New World or a small minority of local large landholders bought up the disentailed land before small cultivators could borrow enough to make their down payments. The returned emigrants often themselves became absentee landlords, men of status, but received little or no material benefit from the land because it was overpriced for what it could yield.[32] In any event, growth in agricultural production went largely unrealized, and whatever increase did occur simply went into autoconsumption, as the rural population continued to grow.
Under these conditions of economic stagnation, the potato staved off disaster; like maize an arrival from the New World, it found favor in Asturias and was taken up intensively early in the nineteenth century. Unlike escanda or corn, the potato could grow productively even on steep unplowable hillsides, which could be spaded. Upland commons, often held by parishes in central Asturias, were thus broken up to accommodate potato patches, on condition they be returned to the commons after a stipulated number of years. In practice, the broken-up land was rarely reclaimed by the parish, and the cultivator became owner by default. It becomes clear, then, that increasing agricultural production was caused not, as had been envisioned, by disentailment but by extending and intensifying the cultivation of the potato. Ironically, it was also the potato—however small its volume in the market—that did more than the policies of the Enlightenment to alter the structure of landownership.
Whatever the increase in agricultural production in the nineteenth century, it could not support the large numbers of industrial workers recruited from other parts of Spain into the Asturian coal mines at the end of that century and the first two decades of the present. Sustenance for such a work force had to be imported from outside the province, and an infrastructure of railroads, bridges, and tunnels was gradually built to make that possible, at least in the central Asturian triangle close to the coal mining area. An early critical element in that network was laid down in 1884, with the completion of the railroad system connecting Asturias and the central plateau. Farmers on the southern side of the Cantabrian range could henceforth conveniently provision
Asturias with grain, oil, and wine. To urban and industrialized Asturians, this signified the end of the enclave's autarchia.
It was expected, once the requirement for locally produced grain diminished, that Asturian cultivators would quickly move into market-oriented livestock production, for which the region was naturally suited. But Asturians were not able to make that shift quickly, for whenever an animal died, traditional livestock-sharing arrangements (a medias )[33] penalized the cultivator but not the absentee owner. The cultivator was therefore inclined to limit his risk and take on only the minimum number of livestock needed to serve the needs of his family with traction, manure, and milk. The rural economy thus continued to stagnate until close to the turn of the century, when official props for this livestock-sharing arrangement were withdrawn. Rural people, despite the coming of the railroad and the increased importation of grain, thus continued, as they had always done, to eat foods produced locally.
The dietary dimensions of that stagnation are vividly remembered as focusing on milk: "We Escobinos could only afford to consume the buttermilk or whey. The curds and the fat had to be processed for market." The statement must be contextualized, for it does not, after all, sound like impressive deprivation to Americans overloaded with animal fats and proteins. But rural Asturian families rarely consumed animal products other than milk or the pork derived from the annual slaughter of one pig. Beef was eaten only when a sick or injured cow had to be slaughtered. Hunting was the privilege of the elite, and poaching was severely sanctioned. Even milk was not abundant, for the cows had been selected for their hardiness as draft animals[34] rather than as dairy producers. Stagnation meant that animal fat and protein remained in very short supply. Only tardily, well into the twentieth century, did animal production become a major source of income for rural upland Asturians and permit them to gradually accede to the dietary standards of miners, other industrial workers, and urbanites.
The Asturian dietary picture of the early twentieth century, in part a legacy of these preceding centuries, can be discussed in terms of the two elements critical for preventing pellagra and IDD. Niacin, present in bread, was plentiful in the diet of rich Asturians who, at least since Roman times, have had access to spelt wheat
or common wheat imported from Castile. Industrial workers, principally miners, whose bread also derived from grain grown for the most part outside the province, likewise took in optimal amounts of niacin. But it was a different matter for rural Asturians. Their diet depended on the number of livestock, the availability of land, and cash flow. Those who ate both corn and animal products ingested the precursor of niacin through the latter, thereby offsetting the niacin deficiency of the corn-based diet and holding pellagra at bay. Those to whom both cash and commercial outlets were available bought flour or bread, for bread was of highest priority. The availability of bread meant that borona, the stiff Asturian unleavened mass of hearth-baked cornmeal and water, the descendant of acorn porridge, could drop out of the rural diet.[35] Borona's disappearance, a loss that was both symbolically and nutritionally significant,[36] led to the disappearance of pellagra. The disappearance of this food-associated disease passed without notice, however. The accession of rural Asturians to common bread, the primary symbol of civilization, was widely appreciated—though not for its nutritional consequences.
Iodine was a different matter, and its lack was not so definitively overcome. The rural population, whose food was almost entirely of local origin, ingested much less iodine than the urban population regularly provisioned with extraregional foodstuffs. Asturian mountaineers residing in isolated pockets beyond the reach of trading networks remained the most iodine deficient. However much they troubled themselves to obtain flour, their consumption of bread remained occasional and hardly supplied them with optimal levels of iodine. The fact that goiter and cretinism persisted in such areas even after common bread had become a staple—after the "blessing" that is bread became available throughout the central uplands[37] —may have strengthened the popular view that goitrous and cretinous people were hereditarily defective and that the defect was independent of dietary habits.[38]
Politics and the Asturian Diet
"Fat Cows" and Autarchy
The years during and just after World War I were lived in Spain under a failing monarchy and the dictatorship of Primo de Rivera.
During this period, efforts were made to raise both the standard of living and of education in remote areas. For rural Asturians, these were the years of the "fat cows," vacas gordas , when demand for livestock in wartorn Europe raised prices.
This was followed by falling prices, the world depression, the return of villagers to autarchia, and the closing of doors to New World immigration. Asturians who had been abroad for years or even decades returned home or were repatriated, and young men who had expected to go off to find their fortune remained at home, severely stretching the absorptive capacity of villages.[39] People responded to this unprecedented increase by extending cultivation into meadowland.[40] Villagers eager to emphasize this point claim to remember that even steep, shady meadows were planted in potatoes or corn. These bad times meant that the food supply was "relocalized."[41]
In 1931, the Republic was voted in, though it soon became clear that the expectations with which it was proclaimed could not be met. Disappointment brought on social and political unrest, to which the government overreacted at least twice. Rural uprisings such as Casas Viejas in Andalusia (Mintz 1982) polarized the nation. The Asturian uprising of October 1934—considered the only authentic workers' uprising in the history of modern Europe (Jackson 1984, Elorza 1984)—drew harsh reprisals from the government. Forces called in to lead the suppression were led by the future caudillo, General Franco, whose decisive response exacerbated tensions even further.
The Spanish Civil War erupted in 1936, inaugurating a period of autarchia for the nation. The Nationalists—opposing the Republicans or Loyalists, the government party—received military help in the form of aircraft from Germany and won the Civil War in 1939 just as World War II was breaking out in Europe. Whether or not Germany's help affected the outcome decisively, the collaboration served historically to ostracize Spain from postwar Europe and exclude it from participation in international associations and economic exchange. Franco, who had become head of state and was to remain in that position until 1975, thus established his grim personal style in the years of autarchia of the 1940s when wardevastated Spain tried to pull itself up by its bootstraps. It was for most Spaniards a decade of great scarcity, if not of famine (Grande Covián 1940, 1943; Calderín 1942) and also of tension. Censorship
was decreed, publications closely monitored, unions outlawed, and mass meetings prohibited, damping, for example, the flow of information on dietary supplements (see chap. 7). Elsewhere in the Western world, such information is considered of broad public interest.
In Asturias, the return to autarchia was doubly harsh, for Nationalists cut off trade between it and the central plateau. This punishing restriction weighed heavily on Asturian urbanites, who had become accustomed to basic imports from Castile. Women from high-lying mountain villages then began to black-marketeer across the passes,[42] resuming the delocalization of their own food supply that was begun decades earlier.
Niacin had meanwhile, during the Civil War, been synthesized in a U.S. laboratory, and Americans, hearing of an outbreak of pellagra on the front, sent it as a gift to the beleaguered Loyalists (Shapiro 1982). This meant that the communications breakdown during and after the war did not prevent Spanish health officials from learning in a timely manner of this scientific breakthrough, a breakthrough Casals had anticipated but had not had the means to achieve. Indeed, soon after the war, the national journal of public health reported that state clinics were using the "anti-pelagra factor"—the Spanish name for niacin—to treat an outbreak of pellagra (Peraita 1940, Grande Covián and Jiménez García 1941). There is no mention in the Spanish literature, then or later, of niacin being used preventively.
Since neither ignorance nor oversight can explain the use of niacin for exclusively therapeutic ends,[43] one can infer that the Franco government, fearing prohibitive expense and loss of foreign exchange, hesitated to use niacin as a nutritional supplement. Indeed, Spain's national journal of public health in 1942 published a detailed code of censorship regarding matters of public health, medicine, and pharmaceuticals (Comisión Central de Censura Sanitaria 1942)—a code that suggests the governments's tight control over health information and spending.[44]
Rationing controlled the production, milling, and distribution of grain during postwar autarchia. Shortages were such that a dark "official bread" was put out, presumably intended to stave off caloric and nutritional deficiencies, whose ingredients included bran and grain of an inferior quality imported from Argentina,
Spain's principal trading partner during the 1940s. Rural and urban people alike maintain that this official bread contained serrín , sawdust. So despised was it, and so intensely loaded with negative associations, that until the 1980s, dark bread of any kind in Spain was generally considered unfit for human consumption. The remark may seem anecdotal until one considers how, throughout Spanish history, wheat and leavened bread have been esteemed while other more lowly staples have been denigrated.
External Influence and Outreach
Autarchia gave way to the austerity of the 1950s, a time during which the West cautiously began to open up trade with Spain. Spain agreed then to lease out military bases to the United States, buying from it in return certain agreed upon American agricultural products: feeds and livestock selected specifically for either meat or milk production. The cows imported into Asturias were Carolina holstein, which, unlike the hardy native casina stock, required stabling, gentle terrain, and feed supplements that also had to be imported. The new livestock forced Asturians to become increasingly dependent on the world market and vulnerable to its fluctuations, but it also enabled Asturias to respond to a rising demand for dairy products, becoming, in a later decade, Spain's number one dairy producer (García Dory, Miguel Angel, and Silvio Martínez Vicente 1988).
This obligatory exchange with the United States marks the beginning of a dietary revolution that has radically increased the proportion of animal fat and protein in the Spanish diet and for the first time in Spanish history, has depressed the consumption of bread. In other words, the United States proved capable of exercising great influence on the Spanish economy and diet. But as we shall see (chap. 7), the United States refrained from exercising such influence in matters of health.
Spanish domestic policy, even under 1950s austerity, guaranteed shoes, bread, and wine for everyone, "to keep Asturians like us from becoming too restless." The policy was so successful that the regional beverage sidra , a mildly alcoholic apple cider, was replaced by wine.[45] In the wake of this relative affluence, Asturian alcoholism rates soared to one of the highest in the nation.[46]
When it chose to act decisively, the Spanish government could wield a very significant influence on Spanish health and consumer behavior.
Despite the provisioning of these Spanish basics, restlessness increased, however, and culminated in the late 1950s in illegal strikes, at the forefront of which were Asturian miners. Uneasy, the government was pushed to further set aside its policy of austerity and isolation and took measures to support the integration of Spaniards, largely as guest workers, into an industrialized Europe. An outflow of young villagers thus responded to the European opportunity. This was offset by an inflow of government-sponsored mass tourism, primarily to Spain's Mediterranean beaches. Foreign exchange from tourism, combined with worker remittances from Europe, primed the capital pump and allowed Spain to become, by 1969, the world's tenth most industrial nation (Anuario Estadístico Oficial 1970).
Invisible Deficiencies amid Abundance
By the early 1970s, in the waning years of Francoism, Spain had become a consumer society. Significant among the imports in 1970 were infant formula, pharmaceuticals, and pharmaceutical patent purchases (R. L. Fernandez 1979, 1980). By 1980, the Asturian lactic industry was producing infant formula of a quality that competed with Swiss imports. Spaniards had become Europe's largest per-capita consumers of pharmaceuticals (El País 1981b , Dec. 16), yet no domestic or imported iodized salt had by then come onto the market.
In summer 1983, Grande Covián, the Asturian physician and internationally distinguished research physiologist and national health adviser, declared himself surprised to learn, at Madrid's International Thyroid Conference, that iodine deficiency was still a national problem.[47] Author of a postwar article on pellagra, he was then about to launch a nationwide educational health campaign aimed at reducing cholesterol consumption and preventing heart disease, diseases brought on, at least in part, by overnutrition (Grande Covián 1975, 1988). His surprise at learning only in 1983 of the continued persistence of IDD in Spain and especially in Asturias, his home province, suggests that (for reasons discussed
in the chapters following this ethnography) chronic, endemic, nutritional diseases can remain invisible to medical experts. Indeed, diseases and disorders of nutrition to which one is habitually conditioned can remain invisible even to the internationally renowned nutritionist/physiologist who is himself a native of an afflicted region.
A brief nutritional ethnography drawn over time, such as has been presented here, shows us historic processes by which ethnic character and caricature are established. Such processes serve in significant ways either to screen and make invisible or to view as hereditary defects those pathological conditions that are in fact chronic or endemic, of nutritional or environmental origin. As long as these conditions are screened or made invisible in this way—by a process of ethnocentric and prejudicial image creation—effective management is either prevented or truncated. But much more is to be said about this process of neglect, benign or otherwise, than can be culled from ethnographic history.
Chapter Four
Kinship and Affliction
Introduction
Dilemmas of Explanation
Metabolic error can lead to symptoms that resemble those of IDD. This similarity seems to call into question the utility of giving supplementary iodine to people known to be inbred, likely to have concentrated over the generations whatever metabolic error was in their midst. We know that such doubts are poorly founded, that iodine deficiency rather than heredity is the principal cause of endemic goiter and cretinism, and that notions of hereditary causation tend to be fostered by opponents of iodine prophylaxis.
Hereditary versus dietary or environmental causation is not, of course, a dilemma of explanation confined to IDD. It is a dilemma considered and reconsidered in clinics and courts, for example, in treating alcoholism or in pressing suit against those whose nuclear devices are seen as having raised the incidence of leukemia above normal background levels.[1] The genealogical method developed to deal with that dilemma in the case at hand may well be employed to sort out other conditions and diseases whose behavioral, hereditary, and dietary components remain to be clarified.
When, as in the case of endemic goiter and cretinism, the idea of hereditary causation continues to linger as if it had never been thoroughly refuted, it seems appropriate to closely examine a field situation in which that dilemma is present to see what else might be learned from it.
Here I examine the idea of hereditary causation in the field, observing the extent to which (1) marital unions have actually been made among consanguines, (2) higher consanguinity coincides with a higher level of affliction, and (3) decline of symptoms is a function of dietary improvement. I present genealogies, to a depth of five and six generations, from which the local pattern of kinship is extrapolated. Despite the fact that only the youngest of the generations in that genealogical matrix is not deeply inbred, IDD is seen to be declining. This confirms the established view that modernization and delocalization of the food supply induce a decline of IDD. But this hardly yields insight into the obstacles to prophylaxis. Other things are to be learned from a case study.
The Narration of Affliction
When recounting genealogies, villagers remind themselves of local-historical situations, the people who took part in them, and their symptoms or afflictions. Many of these symptoms, it turns out, are not inconsistent with a diagnosis of IDD,[2] making it possible to transform the genealogies into pedigrees and chart the decline of IDD. Affliction is often the primary psychological or dramatic element in these stories: the docility of the retardate, for example, whose aging parents count on his plodding labor to survive comfortably, or the lethargy of the obese woman courted only for the land she will bring into a union. These and other protagonists, tellers as much as those told about, are grounded in genealogy.
Neither in the literature of IDD nor that of anthropology is it customary to bring local narratives to bear on pedigrees or kinship models. Here these narrative materials are included because they are valuable, suggesting subtle aspects of affliction not disclosed by highly focused biochemical or clinical tests. These stories suggest, moreover, the interplay of affliction and social environment: how affliction affects a family or a community and, in turn, how these create a social environment accepting of affliction and possibly inhospitable to dietary intervention.
The chapter is divided into two parts. First, I relate inbreeding to the ideal kinship pattern, present the social and demographic background, describe the interest and emotion that over time have
pressed on those with marital or reproductive decisions before them, and offer the key to the genealogical charts. Second, I present the narratives, whose meaning is clear only when seen in light of the underlying social structure.
Ideal Kinship
You'd find that most of us, if you went back far enough, are related. But you can't deal with everyone as if they were family. You can't invite them all to the wedding. Therefore most of us remember only who is cousin to our parents, and some of us remember who was cousin to our grandparents, and a few oldsters remind us of who was cousin to their grandparents. But we don't consider the offspring of these far-back cousins to be family, they're offspring of cousins we never knew. It's too much.
— Araceli González, 1915–1980[3]
Kinship as Compromise: The Negotiation of Contrary Material and Ecclesiastical Imperatives
The epigraph above suggests the pervasiveness of kin relations in Escobines and the limitations, whether temporal or material, on explicitly recognizing those relationships. This complicates the task for the genealogist, since Escobinos who do not recognize themselves as kin may be consanguinally related.
The very basis of social and economic existence in Escobines is kinship and propinquity. Rural work and leisure are shared by kin and neighbor, categories that here overlap a great deal. Property is inherited equally by members of both sexes in a system known as partible inheritance. This system has been practiced for many generations in central Asturias and has created a problem of recurrent fragmentation of property in an ecology where land is limited.
Facing this problem, those contemplating marriage give serious consideration to the properties they are likely to inherit, especially to fragments that may be rejoined through matrimony, giving a firmer basis to the prospective household economy. Where parti-
ble inheritance is the norm, it is therefore materially advantageous for cousins to marry.
Escobinos ultimately feel themselves constrained, however, by the Catholic church, which they believe prohibits marriage between hijos de hermanos —offspring of siblings, that is, first cousins—who have not paid for "a papal dispensation." Since they understand ecclesiastical rules as requiring them to marry "out," while economic realities urge them to marry "in," they find themselves under contradictory social and economic pressures, which they resolve by sibling exchange. This exchange strategically manipulates the system to satisfy both ecclesiastical and material imperatives.
Figure 3a depicts the essential first elements in that strategy: sets of siblings are "exchanged" in marriage. That is, two brothers marry two sisters (each pair monogamously), or a sister and brother marry another sister and brother, as in figure 3b. The offspring of these unions, because they are primos,[4] first cousins, do not marry (fig. 3c). Primos who are not the offspring of sibling exchange unions do occasionally marry "by the pope,"[5] but offspring of the unions of sibling exchange, sometimes known as primos hermanos, sibling-cousins, have (in the village) neither been known to apply for such dispensation nor form unions. Their offspring, however, are considered ideal partners in marriage (fig. 3d). As offspring of first cousins, they would, by Western reckoning, seem to be second cousins and therefore eligible to marry each other. Yet, on close inspection, comparing figures 3a and 3d, it can be seen that these "second cousins" are in fact as closely related as first cousins, having one set of grandparents in common. This matrimonial exchange of sets of siblings is the first step in the strategic manipulation of contradictory imperatives. Escobinos call this kind of marriage atrueque, exchange of valuables (i.e., partners), implying transfer of neither wealth nor cash.[6]
Escobinos do not recognize atrueque as an ideal or as a recurrent pattern in their kinship system but only as a means to accomplish their ends. It is an "ideal" in the sense of a logical abstraction; it is extrapolated from a thematic interest appearing in the villagers' actual conversations, behaviors, and genealogies. The older women who brought atrueque to my attention usually spoke of such unions with satisfaction, even smugness, as if in the presence
Fig. 3.
Preliminary Elements in Doing Atrueque
of an ideal strategy. Younger Escobinas have learned, however, to feel embarrassed about such unions, as if they were somehow the stuff of very humble folk—not quite sanctioned socially, officially, or ecclesiastically.
Rarely in real life, of course, were the number of siblings, their ages and sexes, not to mention their inclinations, distributed in such a way as to realize atrueque consistently over the generations. But it is important to grasp that ideal as a logical possibility toward which, over many generations, actual behavior tended.
The second step in approaching this ideal is depicted in figure 4. Sibling exchange marriages can logically recur no more frequently than in alternating generations because of the restriction on the joining of primos hermanos in matrimony. In the intervening generation, partners must be drawn from "outside." Marital partners selected to marry these primos hermanos may themselves, in these intervening generations, also be related, as, for example, the "outside" partners who, it can be seen by the bar connecting them, are siblings.
Other ways to marry "in" while appearing to marry "out," as will be seen in the genealogies below, are not hard to find in real life. However, the ideal pattern if worked out most parsimoniously over four generations with only two offspring per union, would be very simple, as in figure 5.
The pattern, one can observe in figure 5a, could go on indefinitely, giving the misleading impression of producing closed lineages, which is not how the problem is solved in practice. What is important to observe in this pattern is how the spouses drawn in as outsiders are drawn from relatives inextricably linked over the generations. The degree of cousinship in such a system—whether worked out as in the model or more variously in real life—is difficult to calculate. In fact, villagers do not calculate it and never speak of "second cousins" or "third cousins once removed" as some people do in the urban West. While the degree of relationship remains unspecified, possibly for reasons of strategy, it will be seen in the genealogies that spouses in all generations except the present one of young adults are almost never unrelated.
Ego is the offspring of the youngest generation, the product of what may be called monogenetic monogamy, in contrast to the presumed heterogenetic monogamy of the West.[7] Ego, as can be seen
Fig. 4.
Partners drawn from outside may themselves be siblings.
in figure 5a, has only eight great-great-grandparents, while a similar ego in a system of perfect heterogenetic monogamy, as in figure 5b, has sixteen. This reduced number of ancestors in the monogenetic system means that under ideal conditions, an Escobino's ancestors stop doubling after only three generations. Marriage practices in Escobines actually fell short of that ideal. Nevertheless, the practice impeded fragmentation of landed wealth and also—and this is the crucial point—produced an unusual degree of genetic concentration.
Reconciling Health, Wealth, and Love
Escobinos no longer feel a need to marry "in." This is not surprising, as diversification of the economy and improvement in transportation in this century expanded trade relations, diversified income, and reduced Escobinos' reliance on locally grown food-stuffs. These same forces also expanded Escobinos' network of human relations and the pool from which spouses could be drawn.
The ideal was not a prescriptive rule, after all, but only a guide. Offspring abiding by it, marrying close relatives, had a better chance of obtaining the means for making a living locally. Those who did not abide by it either emigrated, stayed single, or put love before wealth—reversing the refrain Salud, dinero y amor (Health, wealth and love).
Mucho siento que te arrimes
A la corteza de un roble
Que olvides un amor firme
Porque te dicen que es pobre.
Fig. 5.
Two Models of Monogamy
Observe the expanding number of grandparents in (b) .
I feel injured that now you lean
Against the bark of an oak tree
And forget a firmer love
Simply because she's said to live
in poverty.
This and many other verses[8] attest to parents urging offspring to marry wealth, that is, landed security. Usually, this meant marrying consanguinally, but not always, for it might involve marrying off a young Escobina to an old widower, or a young Escobino to an Escobina five, ten, or even fifteen years older, causing notable differentials in marital age.[9] These differentials, observable on the genealogical charts, are another expression of the promotion of material well-being and the making of marriages of convenience at the expense of youthful sexual attraction or amorous inclination.
The parental interest in marriages of convenience, casar por interés, is understandable. Elders hoped thereby to improve the chances of their descendants residing locally. It made it more likely that grandchildren would serve as affectionate caretakers in the elders' declining years. Offspring impoverished by land fragmentation either produced fewer surviving grandchildren or emigrated, leaving the elders to a lonely and poorly attended old age. Parental pressure on young Escobinos was therefore intense, and in the past, many young Escobinos resolved the tension—between personal inclination, social pressure, and material prospects—by marrying consanguinally.
The Restricted Reproductive Pool: Demography and Consanguinity
Consanguinity must be appreciated against a demographic backdrop (fig. 6). According to our 1972 census, there were 783 Escobinos distributed over 232 households.[10] One hundred ninety-eight of these households represented marital unions formed around living couples or by the remaining widowed spouse.[11] These couples, grouped by age, manifested decreasing consanguinity with decreasing age. My criteria of consanguinity were twofold:
Fig. 6.
Age Pyramid of Escobines, 1972
(1) that the couple or widowed individual recognize the "blood" relationship, saying, for example, somos algo de familia (we are somewhat related), and (2) that the relationship be traceable.
As already discussed, there are problems in quantifying IDD where much of the population has not been treated, where IDD is not a reportable disease, where goiter is a stigma, and where the gradations of defect and deformity in the population cannot be clinically assessed. Nevertheless, by visual inspection alone, it was clear that the majority, 56 percent, of married women and widows age forty and older were goitrous (i.e., had goiters of grade 2, 3, or 4), as were a noticeable number of younger women, perhaps 20 percent.[12] A number of younger women, goitrous or not, sought medical attention for a variety of symptoms, receiving treatment directed at the thyroid. Six people were congenitally deaf: five were men, and one was a woman. Clinical and biochemical tests run by health authorities on this population showed low enough levels of T3 and T4 to warrant emergency intervention (see chap. 7).
As can be seen in figure 7, 50 percent of the couples age forty or above were consanguinous, as were 44 percent of those in their thirties and only 12.5 percent of those in their twenties.[13] The majority of Escobines marriages concluded since 1972 have drawn spouses from outside the parish, and none have been concluded, as formerly, to favor the reunification of property. Young Escobinas refuse to marry men exclusively dedicated to cultivation and herding; hence, no young couples now make their living exclusively from the land. In Escobines, the trend away from consanguinous unions has probably been more precipitous than in other nearby villages where modernization arrived more gradually, for a very successful village dance hall known as La Pista, the "dancing field," has, since the late 1960s, been drawing increasing numbers of young people from far downriver. Young Escobinos, even those who are university students, now tend to meet at La Pista the outsiders they eventually marry.[14]
It is now important to point out that more than "convenience" and lack of appropriate unrelated partners account for the high consanguinity of the recent past. Emigration, going on for well over a century, introduced villagers to a wide field of possible partners abroad. Yet only two of those men who emigrated be-
Fig. 7.
Declining Incidence of Consanguineous Unions
tween the turn of the century and the Civil War brought home a spouse from elsewhere.[15] The other returnees drew spouses from the small pool of cousins, fellow villagers, and parishioners. A few drew spouses from outside the parish, from villages at nearby higher elevations (see fig. 8), where people were exposed to the same environmental hazards and economic conditions as in Escobines. Escobinos also found spouses at lower elevations; close examination revealed, however, that these were nearly exclusively drawn from villages popularly known as afflicted with goiter.
Figure 8 shows that not every settlement[16] at a convenient distance forms part of that pool. Towns were not part of the pool, nor, with two exceptions, were the villages situated close to the downriver industrial centers long served by commerce. These two exceptional villages, perhaps because they were caught in an intricate fold of mountains whose topography made transport difficult or whose geology made for a particularly high load of goitrogens,
Fig. 8.
The Larger Pool from which Escobines Spouses Were Drawn
stand out in a turn-of-the-century record as having an uncommonly high, 90 percent, prevalence of goiter (Fernández-Ruiz 1965).
The people in this reproductive pool numbered about 3,000. They shared common characteristics of elevation, lifeway, and diet—factors shared by many other Asturian villages in the higher reaches of this watershed, populated in 1970 by about 25,000 (GEA s.v. Aller). This larger number did not, however, form part of the restricted reproductive pool, a fact that asks us to consider what additional common denominator distinguished the villages in the pool but not the other nearby villages.
The widely quoted refrain, "No goiter, not beautiful," might at face value suggest a special preference for the goitrous or those likely to become goitrous. But any preference for goitrous partners is ruled out when we notice that goitrousness is feared and, when possible, avoided or remedied. Endogamy and endemic villages may be better explained by exclusion: prevalence of severe endemic goiter excludes villagers from the general reproductive pool of the vicinity and channels courtship into similarly afflicted villages.
Genealogies and Genealogical Stories
Preliminaries
The genealogical charts presented below, along with what is normally encoded in genealogies, register social and pathological information. Marital unions and their offspring, sibling groups, are of course the dominant elements. Also registered are temporal facts pertaining to birth, death, life span, and generation and social facts encoding place of residence, emigration, family names, and nicknames (which may also be "passed down"). The individuals whose stories appear in the text are designated on the charts by number. Sensory, motor, and behavioral aspects are encoded as in the pedigrees drawn up by thyroidologists. The criteria employed, already discussed in chapter 1, combine visual observations with the villagers' judgments of intelligence and performance.
The tree diagrams of anthropological convention represent the ethnographic reality only in part. Escobinas, when they speak
about kinship, emphasize cousin groups rather than lineage. They do this beginning with ego (whether herself, a descendant, or a neighbor) and work out broadly in a single time frame (horizontally on the charts) to siblings, cousins, and their in-laws. Only with prodding do Escobinas move up from this "messy genealogical gossip"[17] pertaining to these current relationships to the common ascendant, where they once again begin to talk about cousins. All the while they recount lively details about these personages. These stories are mnemonic devices and signposts and help them instruct offspring (or the anthropologist) in these relationships.[18]
The Imagery of Relationships
Escobinas find their way through these "messy" relationships without visual aids, but yarns and the interweaving of a fabric—metaphors appropriate to women—make up a goodly part of their verbal imagery.[19] The anthropologist, basing herself on these verbal images, takes the liberty of compressing them into one graphic image, however impoverished, suggesting a three-dimensional, more or less circular, social fabric (fig. 9). Chains of stitches (each stitch an individual) form groups (siblings) and rings (generations and contemporaries). Rings corresponding to other generations are suspended above (older) and below (younger) this first ring. Yarns connect the rings or generations, vertical ones descending to offspring, slanted ones to less immediate relationships. Yarns also radiate beyond the rings, as if spinning out to villages from which partners have been drawn. Yarns are also stretched out to more distant places such as Madrid, Brussels, Havana, and New York, connecting Escobinos to the larger society in which relatives have settled down and from which many return.
"Intermingled blood"[20] is another popular image, a dead metaphor, perhaps, for urban Westerners whose technical appreciation of consanguinity is grounded in modern genetics, not in blood but in DNA. But if we think of how blood flows and property is conveyed down the generations, and how affection, cariño, develops out of frequent contact, especially with one's cousins, then we can better appreciate the imagery of these fabric-working, warmblooded Escobinas. They relate cariño to carne, flesh. "Isn't flesh the substance through which blood flows? Isn't flesh what we rub
Fig. 9.
Kinship Imagined
up against? Isn't it our constant rub up against each other that produces affection [relationships] among us?"
Key to Genealogies
Social and Temporal Aspects . Conventional signs as well as other signs devised to encode social and temporal matters are listed here.
Additional social and temporal signs in the charts are explained as follows. The approximate time span of a generation may be indicated in Arabic numerals. The numbers in the rectangle refer to the investigators' set of archives. Last names, always pseudonyms, are printed on the line connecting a set of siblings; nicknames may appear there also. In a population of some 700 people described by only thirty-seven last names, nicknames aid identification. And since in practice they are also sometimes inherited, they can aid in tracing genealogies. Some nicknames are derived from place of origin and may be used in a person's presence, but most nicknames do not obtain such usage, least of all those with any element of disrepute.
The diagram (p. 84) shows that the husband's grandmother (1) was her grandfather's (2) niece, while her grandmother (3) and his great-grandmother (4) were siblings. The designation of "higher consanguinity" is here applied to those who speak of themselves as being algo de familia, somewhat related or something of family. Examination of a sample of unions describing themselves with this phrase showed that the individuals in question were indeed multiply and demonstrably related.
Symptoms, Defects, and Renown . A set of signs indicate symptoms and defects; they have been adapted from medical conventions. In addition, I have devised signs to indicate local renown and disrepute, for like Mead, I believe we must try to understand the ways in which talents and aptitudes arise under difficult circumstances. What is more, it is useful to have a device for readily
Fig. 10.
Codes for Consanguineous Unions
Fig. 11.
Disparity in Marital Age
identifying talented individuals who may be recruited into health campaigns arising out of studies like this one.
Individuals I have either known, observed, or been specifically told about are the only ones whose symptoms or defects are registered on the charts. In figure 12, I have divided the circle or square into quadrants to signal different aspects of symptoms not inconsistent with IDD. The upper right quadrant indicates thyroid pathology and morphology; the upper left quadrant, sensory and motor problems; the lower quadrant, behavior. In practice, these distinctions overlap.
Theoretically, the symptoms presented can appear in either sex but are drawn here in the sign of the sex with which, in Escobines, they are usually associated:
Fig. 12.
Coding by Quadrant
The rays around the penultimate sign are assigned to those who have a special aptitude, such as proficiency in evaluating land values, managing a business, public speaking, or writing articles, poems, and formal documents. The last sign is social, referring to a couple who have been "thrown together" in a particular kind of union of convenience known as achoramar . The attribution of worthlessness is a social way of speaking about pathology or symptoms disabling a person mentally or physically. Usually, the attribution is given to a couple whose several symptoms are not inconsistent with a diagnosis of IDD. The language in which Escobinos discuss these matters of aptitude and affliction is presented in chapter 6.
Method by which Escobinos were Registered
Earlier, I discussed the method of focused participant observation by which I initially gathered my observational and genealogical data. The data base became richer as I repeated my visits to the field site for, once I recognized individuals and knew where they lived and worked, to whom they were related, and the nature of their preoccupations, they spontaneously revealed additional material related to the afflictions they or their family members and neighbors had experienced. In this way, in addition to updating my visual observations, I amplified my original data with material that direct questioning on these stigmatized conditions could not have elicited. The symptoms and defects noted on the genealogical
charts reflect, then, my own observations combined with those the villagers have themselves noted.
Some readers, never having done anthropological fieldwork or practiced focused participant observation, may have no idea how data like this is gathered. I gathered and coded my data as follows.
I could see the necks of young women thicken early in pregnancy; most often, these thickenings declined in the postpartum period. The former I marked as goitrous,




The upper left quadrant registered men and women who, in comparison to Escobinos in general, spoke thickly, and others whose speech (over the years of my observation) had become slurred, and I marked them accordingly,






The villagers' terms and characteristic narratives (described in
chap. 6) undoubtedly recall the buffoons and idiots described in literature and known to villagers around the world, even in zones not known to be afflicted with iodine deficiency. This similarity does not mean that such terms for the anthropologist or public health worker lack all utility in identifying affected individuals in any particular community but rather that the villagers, lacking specific terminology, invent terms to fit their own needs, and these terms can call the outsider's attention to conditions that need to be examined in detail to determine if they can be remedied or prevented in the future.
A point made earlier should be reiterated here: symptoms not inconsistent with a diagnosis of IDD may or may not be the consequence of IDD. I am not, and indeed most physicians are not, in a position to definitively trace symptoms to a single cause, symptoms such as dwarfishness, deafness, poorly coordinated gait, low intelligence, puffy facies, and edematous and scaly limbs. When I or any villager was able to attribute such symptoms or defects to trauma or to a disease process distinct from IDD, for example, to protracted lethargy and depression following the untimely loss of a loved one or, more simply, to a limp resulting from an accident, then I did not record the symptom or defect on the charts. This does not mean that all the charted defects and symptoms stem from IDD. It means only that neither the villagers nor I have a better explanation than IDD for the appearance of that symptom or defect.
It will be seen that the genealogies that follow provide evidence for the pervasiveness of pathology and defect, its apparently familial aspect, and its apparent decline in the younger generations, which, though inbred, have experienced a more diversified diet.
A familial-type defect not yet apparent may show up, however, after a long delay and after the reproductive period is over. If it shows up only after such a delay, this in itself signals departure from an earlier pattern in which such symptoms showed up in youth, usually early in the reproductive period (see photographs). It also suggests that whatever the cause of these familial traits—widely presumed in Spain and elsewhere to have been brought forth by inbreeding—diet may either defer or entirely suppress their expression. In other words, expression of the genotype is subject to environmental thresholds.
Genealogies and Their Associated Narratives
Genealogy 1: Sibling Exchange, Atrueque, and Its Decline
Pirico El Tabernero [1], "The Innkeeper," heads what looks like a lineage, figuring as the only remembered ancestor in the generation that came into maturity before the middle of the nineteenth century. His nickname, attesting to his entrepreneurship, offers the clue to such depth of memory, for he opened the first licensed establishment in Escobines where spirituous liquors and medical remedies could be sold. His nickname was therefore transmitted through the most enterprising of the offspring in the descendant generations down to Flor La Tabernera[2], who in her old age worked out this genealogy with me.
Pirico's grandchildren, Ramona[4] and Francisco[5], who are siblings, then marry the siblings Francisco[7] and Ramona[6].[21] This double union brings forth eleven offspring, primos hermanos, some of whose joint offspring, primos, one would in turn expect to practice matrimonial exchange. But they do not realize the ideal. Why?
One sibling set is called los del tío Pedro, "Uncle Peter's people" (the written translation does not convey the denigrating oral intonation). Uncle Peter's nickname was Zapatero (Cobbler). Escobinos saw cobbling as a lowly occupation practiced only by those too unfit physically to work the land. Peter's crippled son Eladio [8] inherited the nickname but failed at cobbling. He remained single and got so peculiar that villagers said, "He's a vestige of the past, takes a stand against anything new and makes a practice of defecating every night at the base of the telephone pole."
By the time this sibling group came to my attention, all the aging sisters had nodulated goiters. Virtudes[10] and Guillerma[11] were singled out as objects of mockery.[22] Soon after marriage, Rosa died of cancer; the husband of Trinidad[13] either committed suicide or was killed in the aftermath of the Civil War and left her childless, so that there were no offspring either to exchange in marriage with primos or to care for "Uncle Peter's people." They allowed Gerardo[9], their nephew, to mow for them but refused to turn over their land to him legally. Trusting no one, they lived
Genealogy 1.
meagerly, climbed slowly up to their meadows, and, in slow, pained motions, turned the hay over themselves. Relatives more distant than Gerardo would gladly have taken care of them in return for the land, but custom restrained them, allowing them only to watch the spectacle on which they and other villagers commented, "serves Uncle Peter's people right."
The nickname Tabernera, which generically could have attached itself to all the cousins, devolved only on Flor[2]. She ran off secretly to marry Jesús[15], related to her not as primo but in multistranded fashion. Their impromptu city wedding involved neither parental negotiations nor banquet. This elopement was a risky departure from convention which—like the initiative of Flor's great-grandfather—took gumption.
One of Flor La Tabernera's sisters was distinctly retarded[16]; another emigrated with "the son of my mother's cousin" to the New World. One brother also emigrated [17], married a Mexican woman, and "nothing more was heard from him"; another [18] married Amalia Piquero Polés[19], related to him on both the maternal and grand-paternal side.[23]
One might expect to see renewed sibling exchange in the generation of young adults of the 1970s. But here there is only one candidate, Gerardo[9], conceivably "destined" for either cousin Azucena[23] or Angustias[22], who, having married before his coming of age,[24] were no longer available so that he marries Margarita[24]. Gerardo's sister Irene[26] had a congenital limp. She, in a union of convenience, was matched to Salvador[27], substantially younger and a descendant of her grandfather.[25]
Flor's last son, Chusín[28], precocious and full of initiative, skillfully managed to avoid marrying Irene, courting instead Natividad Avello[29], niece of El Mecánico, "the one with technical talent."[26] Chusín was thus able to tap the technical talent in his wife's family, building up a construction company that has proven to be so successful that he instead of his sisters has taken responsibility for his brother Paco, El Ay[30], born retarded.[27]
The cousins who are Flor's grandchildren have all married outsiders with the exception of Jesusa[31], who married Ignacio[32], related to both her parents.[28] Difficulty in sorting out family property deferred this couple's wedding at least twice. Their parents punctuated the courtship period with tempestuous outbursts and
reconciliations, culminating in an unheard of event, the two families getting together ceremoniously to jointly butcher a pig. The couple's wedding, followed by a banquet for 200 people, represents in Escobines the last of the intentional, property-oriented, consanguineous unions. Two years passed before Jesusa carried a pregnancy to term. Said Jesusa's sister Celina[33], "Good riddance, unions like that. Me, I'm marrying for love."
La Tabernera's account of the family tree goes back farther than most genealogies, probably because a formidable entrepreneur's string of descendants have shown memorable and spirited intelligence. For all her wit, Flor was very short, had scaly skin, a hoarse voice, and the most nodulated, second-largest goiter in the village (WHO grade 4).[29] These characteristics suggest that from early on she had been getting along on low levels of thyroxine. Whatever subclinical hypothyroidism she suffered did not, however, undermine her humor, memory, vitality, or empathy, did not stop her from reading (she named both daughters after protagonists in novels), and did not curtail her joy in making up spontaneous verses about her neighbors. Undoubtedly, she was a victim of IDD and probably also of metabolic error, inferable from her pedigree. What is remarkable is how she managed to rise above the defects of her environment and the deleterious genes apparently concentrated within her genotype—the result of generations of inbreeding. I am pleased to bear witness to this formidable woman.
Genealogy 2: The Burden of Dependency
This genealogy centers on Los Mocos, the collective nickname of a sibling group which draws attention to their unwiped noses. Villagers, in the idiom of the 1970s, consider almost all the siblings as subnormal, retarded.[30] Their nickname goes back at least to their mother Rosa La Mocona [33],[31] only one of whose daughters, Rosario, ever gave birth. The baby was baptized Anabel and became known as La del Quempu [34]. El Quempu is a small, well-defined neighborhood where the baby was raised by two women, both named Virtudes. One of these women was her mother's sister[36], the only one of Los Mocos considered "more or less normal"; the other was Anabel's grandmother's sister-in-law[37], also long known as La del Quempu. Indeed, the devolution of the
Genealogy 2.
nickname on Anabel testifies to the two women's multistranded relationship.
Anabel, attractive and good-natured, demonstrated a capacity for hard work and organization and assumed responsibility for the Mocos's household well before she was grown. But her chances of a good marriage were poor because she carried with her a burden not only of "bad blood" but of several adult dependents. Bound to accompany Anabel into the household of her marriage would be her aunt, Virtudes, her retarded mother, and at least one uncle. A young, eligible Escobino bachelor admired Anabel and wished to marry her, but his parents pressured him to avoid mingling Anabel's legacy of blood with his own. Ovidio[39], by contrast, the grandson of Virtudes La del Quempu, accepted the burden of Anabel's dependents gladly. For one thing, the retardates were already related to him; his father Pachín[40] was, after all, first cousin of Los Mocos. For another, had he not chosen to marry Anabel, Los Mocos would have been split up among a number of households that, in compensation for their custodial services, would have received a fraction of the land any single Moco was due to inherit. In other words, the advantage for him was significant, for by marrying Anabel, he and she together would receive all the inheritance accompanying Los Mocos. The property was substantial, for it was common knowledge that Anabel's grandfather[41] had married La Mocona only for the lands accompanying her into marriage, and people, remarking on the retarded siblings, often said, "Look what he got for all his greed."
The tíos, aunts and uncles, as the couple called their older dependents, make the couple's rather large mixed-farming enterprise viable, based as it is on the tíos' plodding contribution: they attend flocks and stock on upland commons too steep and remote for other herding families. Escobinos say that the absence in those remote uplands of humans and, above all, of human voices, is tolerated by Los Mocos—limited as they are to only monosyllables. Villagers believe that ordinary Escobinos cannot tolerate such isolation. The tíos' labor input thus permits the couple's native livestock to remain productively dispersed. When not in the upland commons, the animals are cycled through meadows and small stables, taking maximum advantage of natural graze and thereby avoiding winter purchases of agricultural inputs. Ovidio was thus released from
the tedious labor of driving the animals over many mountainous kilometers and could instead accept temporary low-paying road construction jobs, an occupational choice he justified by saying, "How could anyone expect me to go into better paying mine work? What would happen to all my dependents if I were to die in a mine accident?" Ovidio is a loving man who treats the tíos kindly and accepts their limitations as his own. It falls to Anabel, meanwhile, to administer the household, manage the money, and assign the household's available labor wherever it is needed. Under this family economy, the tíos have fared unusually well. Villagers remark that only one tía died before reaching old age.
Anabel is wearing out before her time, however. The goiter, which through most of her reproductive years gave her no trouble, "flared up," making her so nervous "the cup danced in my hand." The médico titular, the county physician, remarking on this nervousness, recommended that she see a private psychiatrist. The latter took her money but in the long run proved unable to alleviate her condition. Eventually, a young and better trained physician[32] paved the way for her to see a state endocrinologist who diagnosed her with radioactive iodine, found her hyperthyroid, and had her partially thyroidectomized, leaving her with a fraction of the thyroid but without any prescription for supplemental thyroid hormone. Her nervousness is now a matter of the past, and she complacently accepts the memory loss, obesity, and lassitude that getting rid of nervousness seems to have cost her. Members of the family remark that the eldest of her four offspring, Viti[42], is already a promising family administrator and, living in the apartment building Anabel and Ovidio built next door for their offspring, is able to take over the administration of Anabel's extended family.
In comparison, the cousins of Los Mocos were seen only as plodding and poor. The reversal of their last names—Avello Vígaro and Vígaro Avello—suggests a previous atrueque union. Lola[43], the firstborn, was in fact very beautiful and perhaps not so plodding, for Francisco Sidora [44], the attractive offspring of "outsiders," married her. El Sidora was one of five offspring born to La Sidora [45], an enterprising commercial woman from a goitrous village in the lowlands. La Sidora, with a husband also from the same village, came to trade in cloth and hams but settled eventually in
Escobines to organize a wooden shoe industry among the landless and illiterate poor. She bid on trees in the public forest, advanced staples on credit to her carvers, and made profits in the classical style of a company store.
Apart from Lola, the cousins of Los Mocos who married at all, married humbly. Two were unmarriageable; but Jose[47] married Luisa[48], the daughter of his father's cousin;[33] and Francisco[53] married Isabel[54], to be discussed in a moment. Jose's son Pepín[49] married Perla[50] from the other goitrous village down-river, a woman whose mother, as a child, had lived in the house adjacent to Pepín's own. In all probability, this makes theirs a consanguineous union.[34] Both of Pepíin's sisters, María Lola[51] and Rosita[52], married into Sumonte, a high-lying village two kilometers up off the main highway. This village is considered by Escobinas a situation of remote hardship for a young woman. It is there, as will be seen in chapter 6, that Rosita's own hardship story unfolds.
Francisco, who married Isabel, was hardly able to make a living but relied on Isabel's income, earned by milling chicken feed at the small mill she had inherited. Their daughters, Maripe[55] and Sabel[55], both married outsiders, miners from downriver. During adolescence, these girls—inspired by the monstrous goiter of their mother's maternal aunt[57][35] —were preoccupied by fears their necks would enlarge. These fears augmented in each sister as she felt her neck thicken during her first pregnancy. Months later these swellings receded, however, as the swellings of their older female relatives and their cousins in the hardship post did not.
The comfortable, physically well-endowed offspring of aunt Lola and Francisco Sidora were, of course, Maripe and Sabel's cousins. These became urbanites before Maripe and Sabel were born. The third, Robusto[59], studied fishing regulations, obtained a local appointment as river guard, earned himself a good salary, married Victoria[60],[36] and became part of an emerging village elite, a local but worldly family. The social distance that separated Maripe and Sabel from their much older cousin and his family thus felt immense and increased when all three of Robusto's offspring were sent off, each in turn, to boarding school, two of them permanently removing themselves from the life of the village. Lolita[61], how-
ever, returned from boarding school. One could see then that she had inherited both brains and beauty, for she was as stunningly beautiful as her grandmother was reputed to have been in her youth. To top these incredible gifts, Lolita also seemed destined to marry for love.
Maripe and Sabel watched Lolita, home on school vacations, being courted by an engineer employed in the capital city. Observed in their watchfulness the girls felt themselves admonished.
My mother told us, "Never entertain such dreams for yourselves. Families like us do best by resigning ourselves to our lot and following our own destiny." (Sabel Avello González, June 1966)
As an adolescent, Sabel's mother Isabel had aspired to a better partner than she got with plodding Francisco, cousin of Los Mocos. But the monstrous goiter of her aunt had made people speculate about a possible defect in her family line, dashing those hopes. The mother's embittered admonition, more in tone than in word, thus sunk into her daughters. Nevertheless, they basked in Lolita's splendor while worrying they might not be invited to the wedding, which took place in the parish chapel late in summer 1966.
The occasion was a splendid affair followed by a banquet and dance, which—to compress years into a sentence—set the stage for tourism in Escobines and, in the long run, laid the groundwork for village renewal. Now, almost twenty years since Lolita's wedding, selective emigration does not drain away from the village all the most promising young people.
One of the brightest of those who have decided to stay is Viti[42], Anabel's eldest daughter, the descendant of a series of consanguineous unions. Of the kin one can have in Escobines, Viti has most immediately the most humble and more remotely the most splendid. Villagers see Viti's vindication of her family line as giving hope for their own eventual comeuppance.
In 1981, it was Viti, then a university student, who was chosen by the youth of Escobines to give the keynote address at the annual fiesta of Carmen. Hundreds, if not thousands, came to the fiesta where Viti acquitted herself with intelligence and verve, even if she did upset the elders who did not welcome her invitation to "dialogue" about the problems the village "ought to be facing."
Later, she married an outsider of some promise from far downriver, a miner picked for advanced training in the industry, settling down with him next door to her parents' home.
Viti, after having enjoyed a pregnancy marked by astonishing good health, recently gave birth to a son[62]. The course of Viti's pregnancy astonished Escobinas who themselves had become puffy and goitrous and routinely expected to lose one or two teeth during pregnancy. Viti and her husband have given this son a name never before used in the village and perhaps not even in the central mountain zone, Pelayo, the legendary hero of the first days of the Reconquest. The significance of this name—the source of revitalization of a nation—did not escape Viti, direct descendant of Los Mocos.
Selected Individuals: Some Medical and Dietary Observations . At this point the biographical-genealogical narrative must be joined to medical and dietary observations at the individual level. The women now in their thirties, the middle reproductive years, who as adolescents were anxious about their appearance, their ominous heritage, and uncertain about their future, passed early in marriage through periods of puffiness, irritability, increasing despondency, and disarray. Conditions like these were seen by their husbands as normal, as normal as becoming a parent. But from the biomedical point of view, the symptoms probably stemmed from hypothyroidism, for the irritability and puffiness tended to disappear after each of the couples set up as a household separate from the parents and bought food at the Economato, the miner's purchasing cooperative. But the symptoms did not disappear in all these women. Sabel and her sister Maripe, each one having brought into the world the number of children each had desired, are both now on birth control pills and continue to be somewhat thick of neck and complain of loss of memory. Maríia Lola, their cousin, became goitrous during adolescence, married late (at age 32), away from the mainstream, and is barren; and Rosita, her sister, well into her thirties, only got married after obtaining a goiterectomy. The menstrual changes and mild depression that followed her excision have been extensively commented on by her female relatives. They expect her to bear no offspring, and in this they are probably
right. Very likely, she has become hypothyroid as a consequence of the excision.
Presenting a contrast to these women in their middle reproductive years are the women on the threshold of reproduction, now in their twenties, who in their greatest well-being are represented by Viti. Their pregnancies and early years of marriage are less troubled than were those of the women just a few years older. Nevertheless, even among them, vestiges of IDD can be seen. Viti's sister Monchi[66], according to her mother, "always a finicky eater" throughout her childhood ate only a narrow range of foods and altogether avoided the marine fish Anabel regularly set down before her on the family table. Monchi—failing to obtain the benefit of the diversified range of foods that have become available to Escobinos only in this generation and probably endowed with errors of iodine metabolism that, as we have seen on the genealogical chart, have shown up familially—is probably subclinically hypothyroid. My impression was corroborated by the visiting physician who knows this family well. Monchi's poor schoolwork, a certain lethargy, and slightly puffy face indicated to him that she was hypothyroid.
Monchi seems, in this regard, similar to her friend Paquita, also finicky and lethargic. Paquita's hypothyroidism was accentuated by pregnancy, however. When her hoarseness and small incipient goiter persisted well beyond the offspring's infancy, she was sent to see a specialist who, in 1987, excised her goiter. This occurred when her offspring, born and raised out of wedlock, turned two. I saw Paquita while she was recuperating in the hospital, where she maintained that she did not expect to be on any kind of supplemental hormone, "because the doctor, el de las manos doritas ("he of the golden surgical hands") thinks I'll be fine with the part still remaining inside me."
The experience of Monchi and Paquita, on the one hand, and Viti, on the other, suggests that the effects of such inbreeding as did occur in Escobines need not be devastating when dietary iodine is optimal, as it appears to be in Viti. The effects of environmental iodine deficiency can be devastating, however, when dietary iodine is suboptimal, as it was before mid-century for Los Mocos and everyone in Escobines. It is quite possible, of course,
that the tíos and their mother, La Mocona, all had low native intelligence, independent of any limitation imposed by iodine deficiency or goitrogens (see chap. 5). But whatever intelligence may have been inherently lacking, it was undoubtedly limited even more by iodine deficiency.
The goiters in the tías, and the dwarfism and retardation in all the tíos, traits that have not shown up debilitatingly in the next generation, suggest that iodine deficiency in Los Mocos was permissive—permitting the genotype to manifest itself in the phenotype. Optimal intake of iodine might have compensated their metabolic error. In the same way, it is likely that both Viti and Monchi, given the consanguinity and symptoms manifest in both parental lines, have metabolic errors that remain unexpressed. The error appears to have expressed itself only in Monchi, who routinely passes up the one rich source of dietary iodine available to her. Fortunately, Paquita's two-year-old son, once he enters school, will ingest optimal levels of iodine, for those only slightly older than he have already been injected with iodine (see chap. 7) and in school are served lunches seasoned with iodized salt.
Genealogy 3: "Those Who Paid the Pope"
The offspring of half -siblings complexly intertwine in this genealogy, in which property is concentrated not only by unions of convenience but by deceit. When the treatment received by the retarded in this genealogy is compared with the treatment received by Los Mocos, one notices how varied such treatment can be.
We begin here with Fernando Rabín González[67] marrying María Rabín[68], his father's cousin's daughter, who dies after bearing him two sons, Leo[69] and Manuel[70]. The widowed man marries again and is again widowed, twice inheriting the land left to him by his spouses, then marrying another María[71] who bears him six offspring. Descendants of his first and third wife subsequently manipulate property to the disadvantage of other possible inheritors.
The dramatic scene of manipulation—as reported by Flor La Tabernera, the principal actor's widow—is the deathbed of Joserón, "Swaggering Joe,"[72], the grandchild of Fernando and his first
wife, María. To an astonishing degree, Joserón resembles, both in appearance and age, his half-uncle Jesús[15] (from Genealogy 1), the son of Fernando and his third wife, María, her last born. Taking advantage of this remarkable likeness,
[Jesús] jumps into Joserón's deathbed, and pretending to be the man who's just died, and in front of duly planted witnesses, revises the dead man's testament to benefit only Leandro, the firstborn of Joserón's two offspring, thus disinheriting Leandro's half-sister Rosa. (Flor La Tabernera)
This story was felt to be so amusing it was repeated even by those who had no financial interest in the outcome.
Joserón's two offspring were born to him by two successive wives, Virtudes[75] and María[76], who were sisters. The latter had vowed to remain a virgin and had to be subjugated to consummate the marriage, giving birth to a daughter, Rosa[77], when her dead sister's son Leandro was seven. The half-siblings were raised, however unhappily, in the maternal grandparents' house, considered in those times a fine house built out of the way of the occasional floodwaters that periodically inundated the lower village. After mid-century, when the floodwaters had been brought under control, prestigious taller houses were built below this fine house, pushing it, as it seemed, against the cliff, "showing only their backsides to it," so that it came to be dubbed Tras Casas, House behind Houses. The name of location became Rosa's nickname, Rosa Tras Casas[77]. And as she herself was a little "backwards," Tras Casas acquired a pejorative connotation, ceased to refer to place at all, and became only a mocking insult.
Customary practice would have split the inheritance between the half-siblings because neither of the parents—neither Joserón nor the sisters he serially espoused—had any other offspring. Indeed since the half-siblings had identical grandparents and the "same blood," there was no reason not to share equally in a very substantial landed inheritance. But because of the melodramatic deathbed scene, Rosa was disinherited and left to reside alone with her mother, María, goitrous, obese, and tetchy. Rosa herself was goitrous, obese, and tetchy but had strong legs, a nice face, and a superb voice for singing asturianadas, the traditional mellifluous songs, songs she could project across deeply clefted valleys. Mem-
Genealogy 3a .
Genealogy 3b .
bers of her extended family, confident that the young Rosa had strength and art enough to piece together a subsistence with a similarly tetchy middle-aged man, married her off to her cousin[78] in a union of convenience.[37] One may speculate that the members of the extended family did this to get bothersome semidependents off their hands, either by "greasing the palm of the local priest" or actually "paying the pope."
The motivating force behind Jesús's substitution of himself for the dead man is worth speculating about, because it involves retardation. Jesús had a long-standing resentment of his only sister, Virtudes[79], who—before she became aware that two of her own offspring [78 and 80] were defective—had not treated Jesús's congenitally retarded son Paco[30] kindly. Thus, her harshness may have invited Jesús's long-deliberated retaliation. However, Jesús may simply have been motivated by the prospects of a kickback from the favored inheritor, Leandro[74]. In any event, it is clear that important sums were at stake, for Leandro soon invested his ill-gotten inheritance in transforming the vacant and ostentatious house of an indiano, a wealthy returned immigrant, into a profitable hostelry. Purchase of that white elephant eventually benefited not only himself and his four offspring but many villagers, giving them an important point of contact with the outside world.[38] Yet it must be remembered that capital for the investment was gotten together by exploiting a retarded relative.
Endemic Disease, Opportunity Costs, and Modern Memory
The narratives given here, hanging as they do on the scaffolding of genealogy, illustrate the importance of affliction and its vivid place in memory. They show also how its distribution among sets of cousins, combined with other assets and defects, sets the stage for the particular unions out of which future generations are produced. This is the social and biological fabric out of which the present young adults of Escobines have emerged. We have been able to see that unlike their ancestors, their choice of mate is not wholly determined by the property they are about to inherit or the metabolic errors inherited already. Villagers surmised that something about these afflictions was heritable, and until recently,
this understanding, however vague, constrained their choice of partner as well as the size of the pool—through the mechanism of social exclusion—from which partners could ordinarily be drawn. The opportunity costs of this affliction were very great, and its costs resonate in many ways in the genealogical narratives.
These genealogies were offered in the form of pedigrees that graphically represent family histories in which IDD, when observed or inferred, was charted. The pedigrees suggest that IDD in Escobines may have been intensified by the formation of recurrent consanguineous unions. Selective out-migration—which under circumstances of an underlying environmental iodine deficiency tends to subtract the most fit from the population pool, leaving the least fit at home—may have compounded any metabolic error. Whatever this error, dietary iodine deficiency compounded its effects. But what this study of a breeding isolate and its very recent breakdown makes dramatically clear is that gradual dietary improvement alone is capable of greatly reducing IDD, even in inbred populations.
By no means, however, are the young adult Escobinas of today entirely free of those thyroid disorders that are difficult, if not impossible, to distinguish from IDD. We do not know from this natural experiment, and cannot learn from this method of focused participant observation, whether their varied symptoms stem from hereditary or dietary causes, since whatever dietary protection they received was casual and unlikely to have been optimal.
Whether optimal iodine intake can offset most errors of iodine metabolism cannot, however, be resolved when this upcoming generation is exposed to the physiological demand of the reproductive period. For this upcoming generation of Escobinos is the first to have descended from heterogenetic unions and also to have received, since 1984 (see chap. 7), what is believed to be an optimal iodine intake. We will never be able to learn from this upcoming Escobines generation, therefore, whether prophylaxis alone can stem the expression of minor errors of iodine metabolism. But the forfeiture of such knowledge seems a small price to pay for having spared much of this generation the debilitating effects of malnutrition.
Chapter Five Land and Diet
Introduction: Landed Resources and Life Chances
Chapter 4 evaluated by means of genealogical narratives the extent to which endemic goiter and cretinism in Escobines were exacerbated by the high level of inbreeding. That analysis showed that consanguinity appeared to account for the heightened vulnerability of some, but by no means all, Escobinos to iodine deficiency. Here I examine the role of other factors in iodine deficiency disorders, namely, land, poverty, and diet. I describe a situation where plowland is scarce, but communal forest products are available to everyone. Then, taking a materialist perspective, I consider how landed resources relate to life chances.
Diet, under subsistence conditions, is closely related to what the nearby land provides. That relationship becomes looser as income and, in turn, food come to be derived increasingly from elsewhere. This chapter examines the land, its produce, and the varying access to it that Escobinos have enjoyed in terms of rights over its fruits and how these, in turn, have affected the diet and the expression of IDD among Escobinos. We will find a mild but interesting correlation between access to landed resources and affliction. This is a correlation denied by villagers, however, in part because of an egalitarian ethic and in part because there are many more factors than landed resources which correlate with vulnerability. Last, it suggests how in a feedback relationship, IDD accentuates social divisions. These in the larger society are themselves already an expression of differential property rights.
The Land: Unequal Access to Its Fruits
The territory to which Escobinos have primary access, and on which most of them made their living until village men entered the mines, covers an irregular area of about fifty square kilometers at the southeastern tip of its municipio , or county (fig. 13).[1] The headwaters of the river El Escobón drain this area, to which Escobinos have for centuries had privileged access. At the lowest, most northern extremity of this area, El Escobón passes through the village of densely packed houses, through the flatland that lies between it and the parish seat, and passes altogether out of the township.
Escobinos conceive of this land primarily in terms of its economic use, and it is therefore appropriate to begin by laying out the villagers' land typology. For them and for us, as we shall see, the variations in that typology signify variations in diet.
The contrasting categories of vega and monte encompass almost all the subtypes of land. Vega is land that is cultivable, desirable, accessible, or relatively flat, denoting valley bottoms if they are wide or any flat to rolling land of high quality. It is a relative term, denoting in eastern Asturias, where some villages lack flatland altogether, the cultivable though not necessarily arable land that by terracing has been wrested from steep slopes. But situated in central Asturias, Escobinos have at their disposal a relatively wide valley and subsidiary hanging valleys above it. Thus, vega in Escobines refers to the valley bottom stretching from El Texu up to Abejas, all of which was once under the plow. But in its larger sense, vega encompassed also the land that individual families cultivated in subsidiary valleys like Nogales. In its most restricted sense, it encompassed, however, only the set of plowstrips communally enclosed which formed part of the two-field system: the Vega de Arriba , the upper vega just above the village, and the Vega de Abajo , just below it, between Escobines and the parish seat. Escobinos, not prone to quantifying, agree that less than 1 percent of the township territory is vega.[2]
Escobinos use the term vega also in a larger, social sense. For example, when they speak of los de la vega, "the people of the vega," context determines whether they are speaking of people residing beyond the mountains on the high plateau of Castile, on the
Fig. 13.
Escobines Township
relatively flat coastal areas of Asturias, or in the señorial dwellings of the nearby parish seat. Monte is, by contrast, land that is less desirable: sloped, unplowable, marshy, stony, forested, or inaccessible. People of the monte are by implication poor, hard-laboring, and humble.
Like vega, monte is part of a deeply felt dichotomy. Land in its "natural" state is monte, referring to the land that remains after
vega has been defined. Hence scrub, fern, broom, exposed rock, and mixed forest—uncultivated land—is monte. It also refers indirectly to human behavior, for a meadow that fails to be groomed periodically becomes monte, and a plowfield in the enclosed vega can become monte if it is not cared for properly.
By extension, monte is transformed into the adjective montés : unkempt, rustic, feral, wild. Escobinos who cultivate the land and seek out each other's company consider themselves sociable and civilized, contrasting themselves with others who spend most of their time with the animals in the wildlands and speak monosyllables or merely grunt. But Escobinos regretfully know themselves to be montés in comparison to "those of the vega" and to city people. In other words, the dichotomy of land types parallels the dichotomy of social types, and both, as we shall see, are related to local affliction.
The important economic categories within the local domain are as follows: tierra, plowland; huerta , garden; prado, meadow; pasto, open pasture; and puerta, open pasture in the uplands (see fig. 14). Bosque is forest in general, of which there is castañéu, chestnut; hayedo, beechwood; and robléu, oak. The fruits of these lands have been listed here as Escobinos view it, in terms of declining edibility: most valued are milk and grain, less valued are nuts, least valued are beechnuts, and acorns are reserved for pigs. In this way, the terms for land are dietarily significant.
Escobines households traditionally had access to all these categories of land (García Álvarez 1964; Tuero Bertrand 1974; Tuero Bertrand and Gonzalo Anes 1978), but by the twentieth century, with the economic shifts discussed in chapter 3, there were vecinos, neighbors, who, though residing in the village, did not have plowland at their disposal.[3] Their livestock, however, had access to grub, browse, and communal graze. Thus, it was possible even without access to plowland to fatten a pig on acorns or keep a few goats for milk. In addition, everyone could gather firewood and other useful materials in monte, and everyone could gather chestnuts on private property of "mixed ownership" (García Álvarez 1964:81) during a designated part of the day and season. Similar but more complicated provisions were made for access to hazelnuts and walnuts, the more esteemed nut crops.
Gleaning rights in the communally administered vega were un-
Fig. 14.
Vertical Profile of Land Types
derwritten by customary code and religion. Land-poor Escobinos who did not live off charity could scrape together a living by keeping a limited number of minor livestock, spading a potato patch, and foraging. As we know, these foraged tree fruits are goitrogenous. Thus, much of the plant material available as dietary staple for landless Escobinos and as a dietary supplement for landed Escobinos was goitrogenous. Landless families could live somewhat better, if still but poorly, combining herding and foraging with other activities. They could keep bees, carve wooden shoes, make baskets or charcoal, smoke hams for other villagers, or perform day labor as jornaleros, receiving their pay in meals, grain and tubers, milk, or cash. Nuts, potatoes, grain, occasional cabbage or turnips, and a little milk made up the very poor family's daily fare.
A symbolic reminder of this diet is an implement, a small brass or copper bowl attached to an arm-length iron handle. Mended by rivets in several places and polished, it hangs on the entry wall as a silent reminder of the milk and chestnut soup cooked in it—the mainstay of households where there was little else to eat in the winter. This implement signals a diet dependent on monte. Few Escobinos admit to ever having experienced such a diet.
Differentials in Landholding
Land, and the improvements on it, can best be appreciated visually, hence the township's territory will here be described from the
perspective of an Escobino standing on Peñascu (2,005 m), a peak at the upper, southern tip of Escobines territory. From it, one looks out on chain after chain of "unimproved" mountains. Puerto, the emerald green summer pasture over which one is perched, actually makes up only a small fraction of the mountain landscape. This perception comes as a surprise, for the importance of the concept of puerto to mountain villagers engaged in raising livestock seems, at first, quite out of proportion to its actual extent. It is the place where livestock, after a winter season of short rations, fattens "for free." And, in contrast to life in the village, puerto is a place of relative freedom where courtship tends to flower. It is, moreover, in puerto that whole milk was a regular part of the diet, rather than the skim milk or whey customarily taken in the village. It is thus a place, a condition, and also an evocative period in the Escobino life cycle—one of relative freedom and plenty—and it comes as a surprise that actually so little of the uplands reflects that verdant vision.
Surrounding puerto is monte, exposed rock and scrub; and on the slopes falling away toward the north is forest. The small fraction of land that has been improved in this territory—tierra and prado—is visible only several kilometers away where the land drops down toward the northwest. At its distant center lies the vega at about 600 meters, a narrow strip of valley floor through which El Escobón flows, flanked by the highway.
The last villages of the upper watershed of El Escobón, the three that make up its uppermost parish, cluster along at the edge of that valley floor, sparing the best parts of the vega for cultivation. Tierra thus makes up about 1 percent of the township territory, prado 35 percent, and pasto, monte, and rock the remainder. This distribution of land categories is plausible really only from a perch such as Peñascu, for the land that one sees as a cultivator, or from a passing vehicle, appears to be much more productive.
From Piquín (1,500 m), a vantage point closer to the village, improved land dominates the view, and property divisions become visible. Piquín towers over the village and casts a shadow over it on a December noon. From this peak, looking across the vega to the northeast, one sees several sets of meadows: those on the broad slopes bordering on the vega, those on the steep slopes set above the tributaries of El Escobón, and those in the bowls of the hanging
valleys. Multitudinous meadows, between 800 and 2,000 of them, are distributed over these territories.[4] Figure 14 gives a profile of the land types as seen between Escobines and Piquín.
Most prominent are the individual meadows, delineated by stone walls and hedgerows. Small-scale topographic features affecting their value can be distinguished on them, for example, the thin black lines of irrigation ditches that divide some meadows into horizontal segments, enhancing hay production. The history of a number of properties can be read from their shape and vegetation. For example, the recent creation and yet more recent subdivision of a large oval wrested from monte can be known from the age of the hawthorne planted on its boundaries and from the newly planted "living fences" of hazelnut quartering that oval. Meadows vary in size by a factor of one to twenty, but the majority cluster in a middle range of two-tenths to half a hectare.[5]
The land below Escobines is mostly tierra, good land used as plowland. It is divided into a multitude of strips clearly delineated in spring when new growth is just breaking through the soil. All of the strips are narrow and measure less than a hectare but differ from each other in size. Some parcels of vega closest to dwellings are not arable; enclosed behind their own walls, they are regarded as huertas, kitchen gardens, intensively cultivated by spade and hoe.[6]
When most Escobinos made their living from the land, tierra extended beyond vega onto the gentler slopes of colluvial soils that could be plowed, and prados extended high up the shady north-facing slopes, as can be seen on topographic maps published in the 1930s. Now the prados of most difficult access have reverted to monte, sloped tierra has become prado, and an increasing proportion of vega is dedicated to fodder. As a consequence, land use and its designation is in such flux that the records in the land tax office, Hacienda, reflect at best a situation that may have prevailed at mid-century. At that time, one and a half square kilometers in the township were taxed as tierra and ten as prado, but much of the land was not taxed at all because its owners fell below the threshold of taxation (Catastro del Ayuntamiento 1954).
For a variety of reasons, official land records are untrustworthy indicators of the landed resources at a particular moment of any single individual or household.[7] That is, these records are poor
indicators of any particular individual's access to the fruits of plowland. Thus, one cannot infer from official records whether or not a certain individual or family had—out of dire need—to resort regularly to the fruits of monte. But the records in general do corroborate (see fig. 15) the villagers' view that access to land's bounty was basically unequal and that some people, much more than others, consumed nuts from monte as daily fare.[8]
Goitrogen Consumption in Escobines and in the Wider Region
Several kinds of evidence suggest that the consumption of chestnuts—a goitrogenous food (see chap. 2)—was far more widespread than people like to remember or physicians have ever considered probable (Kruger and Ebeling 1922; Cátedra 1988; Douglass 1975; Lisón Tolosana 1971). Architectural features such as the corredor , balcony, where chestnuts were cured in the open air, and the sardão, a rack above the fireplace where food, especially chestnuts, were preserved by smoke, testify to the cultural and dietary importance of the chestnut. Vestigial customs of giving chestnuts and hazelnuts to children and needy-looking individuals and innumerable verses in which an important place is given to chestnuts give additional testimony.
Vengan moras abondas
esti aão,
Que quita la fame
el castaão.
Pray for lots of berries
this year
Chestnuts will take away
our hunger.[9]
Furthermore, the great detail in which access to chestnuts is spelled out in the various historical ordenanzas , the regulations at the most local level of government, indicate the importance of chestnuts to at least some segment of the community (García Álvarez 1964: 81–82; Tuero 1974, article 5: 51–54). This was true not only in the upper Escobón, or Asturias in general: a diet in which chestnuts had a prominent place was widespread across the
Fig. 15.
Distribution of Plowland
A curve drawn between the points suggests the inequality of access to plowland.
north of Spain.[10] Chestnuts as dietary staple were replaced, for example, by potatoes as recently as 1960 in the villages of Galicia's mountainous interior (Fernández de Rota 1984).[11]
Most Escobinos were not landless, however, and did not rely on chestnut as a staple for an entire season or more. As owner, tenant, or sharecropper, Escobinos had access to tierra in the vega and to prado, in conjunction with communal resources. Until at least 1910, escanda was grown as part of the agricultural rotation system involving two enclosed vegas.
The crops in which these vegas were planted give important insight into the historical diet. The upper vega was planted in winter wheat, escanda, and after harvest in late summer, in turnips. The latter, maturing over fall and winter, made way for a late spring planting of corn. Meanwhile, the stubble in the lower vega was grazed communally, then plowed and planted in corn (in symbiosis with beans), and harvested in autumn. If, because of bad weather, the corn matured late, soil could not be prepared in time for a December sowing of escanda. In that event, the vega was left
fallow over the winter or planted in clover and in potatoes in the spring. Weather permitting, this planting could be quite early. The timing was important. Crops had to be harvested early enough so that the lower vega could be prepared for the second winter's planting of escanda. In this way, the major crops were alternated between the two vegas over the course of two years (fig. 16).
This kind of concerted planting regime in Escobines gradually fell apart early in the twentieth century under two influences (fig. 17). Individuals returning from the New World insisted on having more personal control over land they had come home to purchase outright. And a newly promulgated prohibition on small firearms allowed small grain-eating birds to multiply into a plague, devouring the ripening small-grained escanda. Because of these changes, cultivators of escanda became discouraged and let it decline. Jointly, these changes favored expansion of potato culture in the enclosed vegas. As escanda declined so did the turnip, because the (usually) later harvest of potato and corn did not allow the turnip to take root before winter.[12]
These changes had significant implications for diet and disease: maize and potatoes became the new staple subsistence crops. The change altered Escobinos' niacin and goitrogen profile. Niacin uptake, as discussed in chapter 3, diminished with the replacement of escanda by corn. Turnips ceased to be planted when late-maturing summer crops began to occupy both vegas; thus, this source of goitrogen ceased to be available to the poor, who customarily gleaned turnips. These changes meant that niacin consumption diminished in the diet of the landowning majority. The diet improved, however, insofar as one source of goitrogens was subtracted from the diet of the landless and poor. Agriculture changes in this regard were a nutritional leveler.
No Escobino admits to having eaten turnips (a goitrogenous plant) or turnip tops (Palacios Mateos and Ramos Duce 1965). But a mocking verse, chanted by Escobinos about their neighbors in El Texu, holds that "turnips got stuck in their throats":
Aquí en Escobines
Tenemos la cadera ancha
Vosotras teneislo arriba
La coxera en la garganta.
Fig. 16.
Crop Rotation I
A two-year cycle involving escanda , wheat, and turnips.
Here in Escobines
We've got it wide in the hips
You've got it wide
In your throats![13]
The allusion, in the context of intervillage rivalry, refers derisively to the consumption of turnips by non-Escobinos. Texuanas in this verse stand accused of being animals, of eating what Escobinas preferred to consider as fodder fit only for beasts. Texuanos, more often than Escobinos, may have had to descend to this dietary level because they lived within a village more socially stratified than Escobines and in greater proximity to señores. For El Texu had four casonas , great landed houses of gentry, surrounded by the
Fig. 17.
Crop Rotation II
A two-year cycle alternating between potatoes and corn.
lesser dwellings of labradores , cultivators. The gentry were the most proximate example of "los de la vega," and gentry do not exist except by contrast to humbler folk, in this case, the turnip eaters. Whatever the extent of turnip consumption, the genius of the verse resides in its association of turnips and goiter. While Escobinas sang it in rivalrous jest, in the wisdom of hindsight, it appears to be "folk etiology," an empirically derived insight.
Evidence of turnip consumption can be found throughout northern Spain. In this larger geographic area, the upper part of the turnip, rather than the knobby root, is dedicated primarily to human consumption, while the root itself feeds livestock over the winter. The stem and leaves are known as grelos in western Asturias and Galicia where they were an important part of the human
diet, at least until the introduction of new leguminous winter fodders in the 1960s (GEA, s.v. grelos).
If they did not consume turnips, landed Escobinos did—and do on a daily basis—consume berza , open leaf cabbage (brassica oleracea ). Escobinos may have lorded it over the Texuanos, derisively versifying as they did about the latter's consumption of turnips, but cabbage, to a lesser degree, is also goitrogenous. Berza, tenderized by frost and snow, is said to be especially delectable. Moreover, it is always available, for cabbages are grown on the perimeter of tierras in the vega, marking property lines. Cabbages are advantageous in this regard because they can remain standing yearround if flowering is delayed and their outer leaves are picked continually. Berza is so culturally ensconced that Escobinos tell stories of "replanting lines of cabbages after midnight" so as to secretly shift a furrow's width of property from one's neighbor to one's own. Tile shards are laid as testigos mudos , "silent witnesses," a meter or two below the berza roots to make such stealing more difficult. Plowland at one time was dedicated exclusively to the cultivation of food for human consumption, hence the standing witnesses—cabbage heads—had to become, and remain, an important element in the culinary tradition.
The consumption of berza has social significance, being a class marker. While an essential ingredient of daily fare for many Asturians, cabbage was until recently considered humble food, withheld from visitors at wedding banquets, in tourist-oriented restaurants, or in casas de labranza , rural bed and breakfasts. Nor was berza available in the ordinary town grocery stores of central Asturias, for every townswoman was expected to grow her own. Cabbage was, however, sold in the open city markets where the lower class purchased most of its produce—markets where the discerning rich also went from time to time to shop. But literature assiduously refuses to admit berza as a constituent in the diet of señores.[14] In other words, the urban middle class did not consume, or confess to eating, berza at their tables. To do so would apparently diminish the distinctions between classes.
Nor did the middle or upper class consume chestnuts, except as hand-warming street fare in winter. Urbanites purchased them from expatriate Pasiegos and Vaqueiros, rural migrants from marginated "ethnic" areas in the Cantabrian range. These people are
referred to in the literature as "despised peoples," echoing the Spanish term pueblos malditos (Tax Freeman 1979:24; Cátedra 1976, 1986). The Cagotes, a similar people on the French side of the Pyrenees, long fixed the imagination of outsiders, as did the Hurdeños of the mountains dividing Extremadura from Salamanca (Michel 1847, Maud 1896) (see chap. 7). The "ethnicity" of these people seems, however, to have faded away[15] over the same time that the incidence of deformities also diminished, presumably due to economic and dietary change.
The principal vegetal goitrogens in Asturias, therefore, are associated with and consumed in any large amount only by country people and the urban poor, though dietary segregation was never complete. Boundaries of culture or class are intentionally crossed with gastronomic "soul food": grelos are now served as a culinary specialty in the finer restaurants of Madrid's Galician quarter. But such boundary crossing occurs only at a safe distance, in the national capital, for example, where festive consumption of otherwise stigmatized foods signifies neither poverty nor rusticity. Goitrogenous foods, it can then be argued, mark symbolic class lines and, when ritually broken, reinforce them.
Unbeknown to most consumers, the symbolic food is also physiologically effective. Its goitrogens, when consumed on a regular basis as daily fare, promote the reproduction of stigmata thought to distinguish lowly people from "their betters." Habitual consumption of goitrogenous foods helps to distinguish gente de bien , the well off, from gente maldita , the cursed. In this way, symbol and biochemistry are linked. Morphologic stigma confirm primary unblessedness and justify social stratification.[16]
IDD: Vestige of Past Differences in Wealth?
Given that the symptoms of IDD generally take long to develop, and to some extent reflect the cost of the food consumed, one may well ask to what extent the distribution of IDD in a village actually reflects long-standing differences in wealth. A two-by-two distribution table should be able to test the strength of this idea (fig. 18).
It is important to keep in mind that before mid-century, Escobinas tended to become goitrous in their teens, earlier than they do now, and that it was largely the poorest households that
Fig. 18.
Theoretical Correlation of Poverty with Diet
High numbers found in upper left and lower
right boxes associate poverty with IDD.
after mid-century, sent their men to the mines, therefore poor households acceded earlier than other villager households to a diet richer in iodine. The materialist theory implicit in the two-by-two table could therefore, in 1972, be tested only on women age forty or older, born before 1933, whose goiters had been established before landed wealth in Escobines had ceased to be the principal indicator of income and diet. Goiters that have developed in younger women since the early 1950s could not, after all, be expected to correlate with wealth or poverty. In other words, the predicted distribution in the two-by-two table would be confounded by the inclusion of younger women, whose menfolk were the first to enter the mines. For the daughters of such men, though landless, were likely, because of the purchase of food grown elsewhere, to be more iodine replete than the daughters of the landed.
Likewise, it seemed inappropriate to hold strictly to the criteria of the IDD symptoms being either present or absent, for since everyone regardless of wealth lived in an iodine-deficient environment, ate goitrogenous cabbage as daily fare, and drank goitrogenous water, everyone was likely to have minor symptoms of deficiency "not inconsistent with a diagnosis of IDD." Therefore, I grouped women who had no symptoms at all with those who were obese or lethargic but not on medication, who had not been thyroidectomized, and whose thick necks were neither nodulated nor seen by their peers as goitrous. The distinction was made between the conspicuously symptomatic and everyone else.
The continuum of wealth required a similar distinction, between the conspicuously poor in this case and everyone else. The women neither poor nor wealthy in youth were grouped with the "wealthy," on the assumption that during their youth—not described as notably poor—they had not depended on goitrogenous nuts as a staple. Those who had been conspicuously poor in their girlhoods (difficult to establish from land records) I knew from autobiographical statements gathered during my years of focused participant observation. Women who had been very poor as girls made statements such as the following about themselves: "We rose before dawn to get chestnuts," "We lamented the scratch marks the brambles left on us, for those marks made it clear how we got our living!" (by foraging and herding goats, not cows), or "I never learned to milk a cow because we never had one" (as opposed to the wealthier woman who might also not know how to milk because her family had a servant), and "I got my meals as a day laborer," and "My family sent me to Castile for a year to scrub floors." The remainder of women, who had not experienced such poverty propelling them periodically into foraging, grew up presumably on the standard village diet based on cereals and tubers. This grouping resulted in the correlation of poverty with pathology shown in figure 19.
The distribution supports the original proposition—that the poor are more likely to be afflicted. According to figure 19, two-thirds (31 out of 47) of the poor who survived the reproductive years became goitrous or acquired symptoms not incompatible with a diagnosis of IDD, while less than half of those regularly consuming cultivated staples in their girlhood came down with clear and lasting symptoms (64 out of 146). In other words, poor girls had a distinctly higher probability of becoming goitrous.
Figures notwithstanding, Escobinas deny that wealth has anything to do with the distribution of goiter in the village. They point to well-off peers who have goiter. From their point of view, there are simply too many goitrous women in the older generation to discern any pattern at all. They disagreed with my "materialist perspective."
The Escobinas' view is understandable and anthropologically far more interesting than anything these statistics might be used to show. Any Escobina, whether or not her family cultivated much
Fig. 19.
Test of Materialist Hypothesis
land during her youth, had to face the possibility of becoming goitrous. Despite the well-known saying, "No goiter, not beautiful," Escobinas did not aspire to becoming goitrous. They were, however, conditioned psychologically to accept rather than resist a goitrous fate.
Escobinas maintain that goiters are distributed according to laws they cannot fathom. To try, as I tried, to understand such laws is to be impertinent, to demonstrate one's immaturity and question God. My questioning displayed to the older women my principal fault, a lack of resignation. "Conformate Renata," they would say "Cada cosa tiene su misterio." "Accept things as they are, Renata. Everything has its divine mystery." Mysterious things should be left in place. Believing this, Escobinas habitually prepared each other to accept these mysteries and tried assertively to deny that inequalities of land or diet have anything to do with the present distribution of goiter in the village.
In this sense, Escobinas are egalitarian, expressing solidarity in the face of a common threat. By refusing to acknowledge any pattern in the distribution of goiter, by viewing goitrousness as capricious fate, they deny goiter any social significance—at least among themselves.
Conclusion: Vulnerability and the Ethic of Equality
I have taken a materialist approach to goiter and have suggested how the distribution of land and wealth, the consumption of crops
and wild fruits, play a role in the distribution of goiter in this afflicted village and across northern Spain. What was most interesting about these findings was not the support they gave to the proposition that goiter is more likely to afflict the land-poor but that the villagers denied any such proposition: they did not want to believe that goiter and IDD were distributed among them in some systematic fashion that was basically a reflection of inequalities. It was far more socially rewarding for them to assert, in solidary fashion, that all Escobinas were equally exposed to fate's caprice.[17]
Their insistence on this belief suggests the emotional and cultural weight that stigma carries. I see it as meaning to them, "If somebody's got to be situated at the bottom of the regional hierarchy, it's more comfortable not sitting there alone. All of us Escobinos are equally there together." To give credence to the patent inequality within the village jeopardizes this psychological posture. Unwittingly, however, this posture strengthens the opponents of prophylaxis—who have everything to gain by viewing endemic village populations as undifferentiated products of inbreeding, rather than as products of social neglect or of maldistribution of resources.
I have shown how land and diet are part—but only a part—of the fabric of affliction and especially how goitrogens are consumed unevenly, making the landed less vulnerable to iodine deficiency than the rural landless. The next chapter explores how these vulnerabilities are expressed in language and folklore.
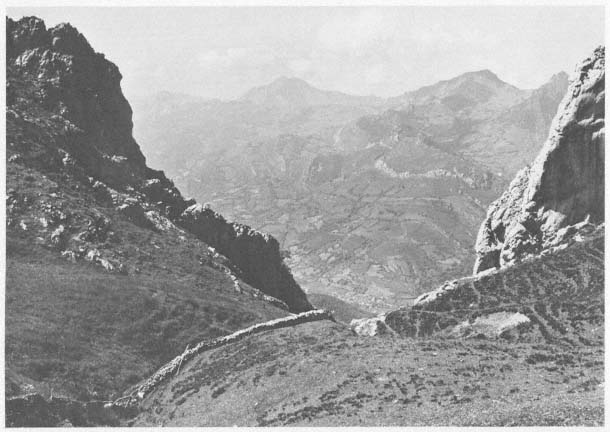
Karst, the classical landscape of IDD. Escobines is barely visible in the valley below.
Ofelia the storyteller.
Daughter and goitrous mother, from a nineteenth century glass plate.
(Courtesy, Joaquín López)
Asturian mining folk of the 1920s, when men as
well as women were conspicuously goitrous.
(Courtesy of Richard Detweiler)
Few elderly Escobinas in the 1960s were
so unguarded as to allow a close-up.

Haying break. In 1966 no one perceived this young woman as goitrous.
At least two of these girls, photographed in 1966, have recently undergone thyroidectomy.
Hypothyroid dwarf, 1908.
(Copy out of Ignacio Zuloaga, Lafuente Ferrari. Barcelona: Hogar del Libro. 1980, p. 22)
The painter Zuloaga came to be severely criticized for exporting unfavorable images of Spain.
Perhaps, then, it is not surprising that his extant notebooks do not reflect the IDD of the 1920s
of Las Hurdes, the endemic area he is said to have visited with Marañón and the king. The
criticism suggests widespread denial of endemic affliction. Denial, in turn, helps explain the
paucity of Spanish images of IDD and sets the stage for inaction.

Man with bilobular goiter.
Artists rarely portray goitrous women.
(Copy out of Jusepe de Ribera, Prints and Drawings
Jonathan Brown. Princeton: Trustees of Princeton
University, 1973: 182)
Two sisters epitomize the Asturian standard of
beauty of the 1920s; one has an unrecognized
juvenile goiter.
(Courtesy of Dr. Joaquín Fernández García)
Herbalist in Asturias, 1989, offering seaweed for both cellulitis and goiter.
Chapter Six
Narrative Accompaniments of Rural Character and Disrepute
Introduction
After examining the historical, social, agricultural, and dietary aspects of IDD among rural mountain people of northern Spain, we return here to a theme mentioned earlier in the ethnography, language.[1] This encompasses both the very localized vocabulary of affliction as it evolves and changes in one village and the villagers' narratives of everyday life in which affliction is an important feature. These narratives suggest, first of all, the innumerable ways IDD takes its toll psychologically, as it continually leads to caricature and casts in doubt the villagers' repute in the larger society. This folklore and its interpretation[2] help us to see the human cost of any chronic disease—endemic or nutritional—that is misrepresented, whether out of ignorance or design, either as hereditary defect or as ethnic character.
These narrative materials and the language in which they are cast are, second, presented as a resource that might well be used as a tool in epidemiological studies. While students of culture and social dynamics have long collected folklore as a source of insight into culture and social dynamics, health survey teams might benefit from looking for the ethnological accompaniments of the diseases they study: specialized vocabularies of affliction and tales of shame and stigma.
Vocabulary of Affliction
Bocio, Goiter
Goiter in Spanish is bocio, stemming from vocear, to voice—cry, clamor, scream, bawl. But in the Asturian dialect, the term is pepu or papu, derived from papar, to swallow soft food without chewing, to eat; hence, in a wider sense, to swallow, put up with, or to take in uncritically. There is an associated semantic field that is part of the meaning of the term pepu . A porridge or dumpling made of maize flour is papas, as in the refrain,
El que come munchas papas trabaya con ruinas vacas .
[Porridge eaters work with degenerate cows.]
Escobinos say of a poor housekeeper that for lack of a proper receptacle, she prepares papas in a wooden shoe. A papón is a credulous individual, lacking an appropriate measure of skepticism, hence an easy butt of a joke. The gerund ta papiando (ta from estar ) is to be self-absorbed or simply selfish. A goitrous person is a papudo or papuo (a ), a papiÿu, an onlooker with mouth wide open, one with a stupid gaze. A papo is any noticeable bulge, whether below the tip of the carved wooden shoe, the plump throat of a bird, or the overly well filled belly of a man. Paperes are cheeks, and paperas are mumps, or simply the stuffed-looking cheeks of a greedy eater. Cheeks referred to in this way may be natural or pathological, depending on context. In like fashion, papo may refer to the crop of a bird, a temporary or permanent lump in the throat, or a blocked esophagus. The creature invoked to frighten children into obedience is known in the region as paparresolla, a female humanoid who swallows up whole the body and breath of disobedient children, turning their air and substance into papos, excrescenses on her body.
The basic terms referring to goiter in Asturias are related, then, to ways of speaking or eating that have largely negative connotations. Goiter evokes words such as crude, rude, and greedy and words associated with the loss of power, voice, and wit. The Asturian saying, "He who has no goiter is not beautiful," may seem to be hopeful, but the associations of the term for goiter are far from beautiful.
Local Terms: así, Jubilado, and El Ay
Escobinos have a broad vocabulary and set of metaphors—hardly exclusive to the village, indeed many of them widespread in the Indo-European world—that are associated with a range of mental, behavioral, sensory, and motor deficits. For example, people are said to have hard skulls if ideas do not penetrate, to have closed tongues if their speech is difficult to understand, to be calloused if thorns do not hurt them. While these conditions might be related to IDD—to cretinism, congenital deafness, or the dermal conditions of hypothyroidism—they could just as well be the expressions of psychological stances or the result of trauma, and discussing them here would not advance our argument. Being general among Europeans, they have little comparative power. By contrast, we can advance our argument if we examine a set of Escobines terms referring to a continuum from "tetched" to frankly "cretinous."
Así, "that way," is the broadest category of deficit, a term assigned to people who for one reason or another are peculiar. The most frequent kind of así are withdrawn individuals, who "refuse to get out into the street." Es un así, "He's peculiar," is one who does not insert himself appropriately into civic life, isolates himself, for example, for months in el monte or in an abandoned hamlet, restricts himself to interaction with creatures not central to the economy, such as bees or feral pigs, or loses his sense of proper proportion when working with domestic animals, interacting with them as if they were humans. El Pintón was such a man, devoting so much attention to his pig, "La Pintona," that the pig's name became his mote, nickname, and was, in turn, passed onto the most peculiar of his offspring.
People are labeled así who cannot adequately carry out the activities normally expected of the members of one's sex. People who speak poorly or cannot carry a message, understand kinship relations, or handle money are así. Así men are those who cannot be trusted to handle a scythe safely in the fields or behave appropriately in a bar. Así women are those who, when exposed during their youth to lessons in reading or sewing, succeed in learning neither activity. Mature individuals who have been normal but start acting peculiarly and persist in doing so over time—especially if they remain suspicious, temperamental, or withdrawn—may
come to be known as así. Women who at an early age start losing their memory and neglecting their appearance may also, if their condition persists well beyond pregnancy and extended lactation, be labeled así.
Those men who become labeled early in life tend to remain labeled, but the women of Escobines hesitate to quickly label another woman. They know that stress may be episodic—when, for example, a heavy work load is lightened or a better diet can be afforded—and that the condition is likely to recede. They know which women in their own time or before them are known to have been especially agotada, drained, by longlasting overload of labor or emotional stress. Agotamiento, the nominative form of agotar, may lead to becoming así, to losing one's menses, or to premature death.[3] Fear of such adverse outcomes prompts family members and neighbors to try to ease whatever strain is on such a woman. Men, however, experience así episodes more rarely than women but far more frequently remain así for a lifetime. A majority of mozos entrados, confirmed bachelors, are considered así.
Jubilado is a more stringent category meaning "retired" and is used in two ways. A man retired from the mines is jubilado, usually because of age or silicosis, the same condition that in the United States is known as black lung (See Stedman's Medical Dictionary ). Early occupational retirement implies no mental, sensory, or behavioral defect. But a man labeled jubilado who has never worked for wages or taken an active decision-making role in traditional subsistence agriculture is considered to have some sort of mental or behavioral defect disqualifying him from marrying, seeking employment, or representing his household.
The term for the firmest category of deficiency is derived from the villagers' exclamation of dismay, "¡Ay!" The term is nominalized by placing an article before it, thus becoming El Ay . Escobinos, inclined by their pride and acute awareness of the smirks of the outside world, generally deny having such a term. The expression, not taught at school, refers, after all, to people who like themselves, but in an exaggerated way, are socially invisible. Yet, they use the term quite inadvertently. For example, when prompted by me to identify a household member who, though physically present, seemed removed from the conversation, they responded, "Oh, that's our El Ay."
El Ay is accepted as retarded already in infancy: he develops slowly, walks late and perhaps clumsily, and hardly learns to speak, expressing himself in "thick" monosyllables or by merely grunting. The three El Ay in the village were all grown men, born before or during autarchía, that is, before 1950.[4] All were able to perform labor-intensive tasks: fetch firewood, shovel manure, and, under supervision, keep track of stock in summer pasture. All three were members of families whose income was derived primarily from the land.[5]
It used to be said in the village, half in jest and half in resignation, "It's not so bad to have an El Ay in a family, for he can be a loyal, docile, and useful companion to an aging couple, when all the other offspring have sprung themselves loose from home." Occasionally, normal offspring are encouraged to stay single and are groomed for such a caretaker role, but only El Ay can be counted on to fulfill it, however clumsily. Unlike less behaviorally limited individuals, such as the jubilado or así, El Ay are not known to be temperamental.
Women may be así, but unlike the El Ay are never considered severely retarded and are never jubilada, perhaps because the labor demand on a woman, though high, is elastic. A woman, though severely limited behaviorally, is seen as useful in a range of activities all known as sus labores, her tasks—tasks appropriate to a woman. Since these can be as simple as fetching water or gathering nuts, a woman cannot, unless she is an invalid, remain inactive or "retired," as can a young man. If her speech is thick and limited, however, her walk or posture peculiar, and, though given the opportunity, she has learned neither to sew nor read, then it may be concluded that she is an irreversible así.[6] Then she may be joined in an achoramar union (see chap. 4) to a man who is himself a borderline retardate.
Terms from Officialdom and the Church: Subnormal and Inocente
Inocente, innocent, is an alternate way of speaking of some of the people to whom the above categories apply. In Castilian Spanish, the term is only an adjective, but in Escobines, inocente is usually used as a noun, referring to the individual who is simple, lacking
in guile, harmless, or lamblike. Villagers wishing to present in themselves or elicit in another an attitude of forgiveness tend to employ this term. For innocents, evoking as the term does the shared religious-moral background of all Escobinos, must be forgiven for failure of performance or breach of conduct. To use the term innocent is to appeal to the moral community, but villagers hesitate to apply it too broadly, for they wish to avoid saddling themselves with responsibility for persons who might, in fact, be able to help themselves.
Two examples illustrate this point. An obese, goitrous, retarded woman was considered an inocente by most Escobinos. She had borne five children out of wedlock. The priest, on behalf of the villagers, solicited a church institution in the lowlands to take four of her children. This solicitation was granted, relieving everyone. But neighbors did not accord this term to another obese and goitrous woman who was married, slovenly, and had more children than she could handle, for villagers wished to avoid putting efforts down a sinkhole. Instead, the neighbors considered her a cochona, a sow (female pig). Metaphorically, the attribution of inocente exonerates, and sow blames. Because the term inocente is put to such strategic use, it cannot be used to categorize or count the afflicted in Escobines.
Inocente can, however, serve as a point of departure for discussing the intricate web of implications, responsibilities, and evasions commonly practiced in a community and by the society surrounding that community, where unexplained affliction is prevalent. Neutral terms such as así, jubilado, and El Ay, and loaded terms such as inocente—and similar terms in other settings—may be received as alarms, suggesting to a keen epidemiologist that local or regional preoccupation with retardation reflects possibly more retardation than meets the eye. A localized, specialized vocabulary of retardation might alone be enough to draw professionals into making a serious inquiry into unexplained defects and retardation.[7] Had this been done in upland Asturias, epidemiological logic might sooner have brought into question environmental factors such as iodine deficiency.
Two conventional Spanish terms, sordo, deaf, and mudo, dumb—more often múo or múa in the village—also form part of
the vocabulary of affliction. Escobinos assume a congenitally deaf individual to be an inocente unless he or she proves otherwise. Thus, no attempt is made to teach sordos communicative skills such as sign language or lip reading. Escobinos do, however, hasten to point out the particular individuals who disconfirm their own stereotype, as, for example, David, who "though deaf, is intelligent and manages all of his widowed mother's livestock wisely." Mudo has less to do with the absence of vocalization than with the strange, disconcerting quality of sounds produced by some deaf Escobinos. Distinct from the sound of speech that is "human and Christian," the sounds of mudos are considered "animallike." Thus, though David may be both deaf and mute, he is referred to only as sordo, for he acts intelligently and avoids vocalization. Ceferino, also deaf and mute, does chores in the stable but carries little agricultural responsibility and asserts himself from time to time by bellowing; therefore, outside the presence of his immediate family, he is referred to derogatorily as El Mu . The only deaf Escobina is a member of a very socially marginated family and even within range of her family's hearing is referred to as La Múa and shooed away. Standing not quite upright, lurching, and bellowing back at her assailant, she corroborates the villagers' general view that múos are really more animal than human.
When Escobinos behave in these ways toward the deaf in their midst, they display a conceptual polarity—animal/human—to which their disrepute has made them acutely sensitive. This polarity is embedded in their use of a very conventional lexicon. The stories below will further illustrate this point.
New terms of affliction have come into common use in Escobines from the military, the mines, social security, and the census taker. An analfabeto is an illiterate adult, no cause posited. Analfabetismo, illiteracy, is as likely to stem from lack of exposure to schooling and written materials as from failure to learn what was taught. Inválido is an individual who has been disabled or is exempt, as from military service. Mutilado, mutilated, invidente, blind, and subnormal, mentally retarded, are official categories of disability or dependency opening up possibilities of government compensation or subsidy. Escobinos began using these terms in the 1970s, after national welfare programs had begun to be extended into the remote countryside, that is, after villagers had
begun to appreciate the monetary value of at least some labels. Given such an incentive, it is hardly surprising that Escobinos have begun to extend terms derived from officialdom onto the merely slow and undergrown, whom they previously called ruin .
We have seen here how the vocabulary of affliction has shifted as officialdom imposes itself on the village.[8] These shifts pose a continual challenge to investigators who might wish to employ colloquialisms as a tool in epidemiology. The task is challenging because the vocabulary of affliction is often embedded within the restricted code, where vocabulary and syntax are kept simple, and the speaker and listener both are assumed to have access to similar fields of information (Bernstein 1971).
Narratives of One-upmanship, Edification, and Disrepute
Below is a sample of narratives told in Escobines representing, as I see it, the local response to unexplained affliction and its accompanying disrepute. I suspect that stories very similar to these are likely to emerge wherever a broad spectrum of peculiarities—whether stemming from chronic, endemic, nutritional, or environmental causes—is generally but wrongly attributed to heredity or ethnicity. A body of folklore gathered from mysteriously afflicted peoples around the world might confirm such a hypothesis, but as far as I know, this effort is the first to make available such a sample from one community. The idea can be tested only when more folklore of affliction has been compiled.
These bodies of folklore will, of course, in their specific contents diverge greatly because of their creators' isolation and their embeddedness in larger cultural traditions. These themes are likely, however, to converge in several ways: in expressing a sense of isolation or margination from the larger society; in the defensive postures taken in the face of outsiders' possible contempt; in the attention concentrated on individuals or peoples more afflicted than themselves; and in the high degree of rivalry and insult carried out in the local idiom of affliction.
I believe it important to examine this folklore, not primarily for the sake of documenting or celebrating one more type of oral literature but to understand and deal with the responses common to
one kind of adversity: IDD. My impression, based on materials representing the cultural traditions of northern Iberia and the Franco-Cantabrian area, is that endemic IDD makes severely afflicted communities, such as the Cagotes of France, the Maragatos of León (Spain), and the Vaqueiros of western Asturias, appear to be discrete cultural traditions unrelated to the surrounding mainstream. The community's distinctiveness, considered as "ethnicity," is then used to justify that community's continued exclusion from the mainstream.
In other words, themes in the Escobines materials—which I expect to find corroborated in the oral literature of other marginated and afflicted peoples—suggest that a people of disrepute are people whose nutritional deprivation has resulted in appearance and behavior making them seem at best strange and at worst subhuman to members of the better-fed society around them. The concept of culture, used to set such people apart and deprive them of benefits enjoyed by the majority, is in this sense spurious. Culture or "ethnicity"[9] is then the mainstream's artifactual excuse for ignoring the dietary or environmental element that sets such a people apart.
Personal Narratives and Stories
What Escobinas tell each other is rarely considered a cuento or relato, a story. What they tell each other and the anthropologist is unlikely to be found in the collections of localized folklore[10] that, it has been argued, have been collected and published primarily to reinforce stratification in the larger society (Uría 1984; chaps. 7, 8).[11] Escobinas in any event hesitate to dignify as "story" the events, jokes, and stereotypic presentations of character which, just as do stories, merit repetition at least locally and give satisfaction. Whatever these relatively brief verbal exchanges are about, they tend to be cast in the restricted code in which vocabulary and syntax are kept simple and the intent of speaker and listener are left implicit (Bernstein 1971:127–128). This restrictedness makes them relatively inaccessible to the outsider and requires interpretation.
"Los Tres Ruines " (The Three Decrepits ). Several Escobinas over the course of my fieldwork told me the following story as if it were
a homely comic event. On the surface, it is amusing, but its repetition suggests a greater significance, the intent to create a favorable image on an outsider. It reflects the way Escobinas in the presence of outsiders, and in anticipation of the outsiders' negative impressions, try to turn these around.[12] To boost the reader over the hurdles posed by the habitually brief restricted code—a code that draws on unspoken but shared understandings—I have put in bold the words the speaker used when telling me the story. The words not in bold come from conversations heard over the course of long participant observation. One will note that while the story in bold, without interpolation, is too spare for any outsider to understand, it nevertheless reads smoothly. A more extensive interpretation follows the story.
You know, Renate, those days in midsummer when the grass has ripened on slopes facing away from the sun, slopes that are midway between the village and puerto (upland grazing lands)? You know when the grass ripens all at once in Nogales? Well those meadows are just far enough away so that everybody goes there for the whole day and stays out well into evening. When it's Nogales , it's close enough so that everybody vacates the village , including infants and elderly. (By contrast) When there's haying in Xueñes (she nods her head in the direction of a much higher and more distant parish of meadows) the infants and elders can't even go. In Nogales the grass is heavy with moisture and it takes a lot of effort to turn it all into hay. Everybody mows, turns, and rakes. Kids too who can't handle a rake go anyway and fetch water to quench the haymakers' thirst. You have to understand, can't you, that Nobody remains in town at all. The town is empty.
Well, on just such a day some forasteros (strangers)[13] coming through Escobines stopped to quench their thirst at the bar in the center of town , you know, the one with the bench in front. The bar to them looked open since the bench was occupied. Threemozos entrados (confirmed bachelors)[14]were sitting on that bench , dressed in paisano (traditional countrymen's attire)[15]and the strangers asked them for a drink, to which the little countrymen just grinned , they replied by shaking their heads in the direction of Nevona (the rocky ridge blocking Nogales from view). There sat those little men shaking their heads—ruin (worthless), enanitos (dwarfed), and mute!
Imagine, Renate, that affable threesome taking the sun and fresh air on the bench in the very center of town? What an impression those strangers must have gotten! As if all of us were like that. Imagine those three ruines, taking their ease in the sun, as if they were little lords.[16]
Ofelia, who told me this story, was known for the faded beauty of her youth. By the time I knew her, she was a widowed grandmother and had a wineskin of a goiter. She was also known for managing her property astutely and for her persistence in returning to her fields and meadows to lend a hand without having any compelling material need to do so, for she was confident that her posterity was secure: she received remittances from two well-off daughters in Argentina, and her son, the local entrepreneur, had started up the local, very profitable, trout farm. Early in my fieldwork, partly through this story, she conveyed to me her values and concerns and clearly delineated our future relationship, letting me know her acute sensitivity to physical defect and matters of reputation.
First, her story brought out that Escobinos are not lazy; they value work. Yet no one in Escobines is driven to work beyond his capacities, and so Escobinos value charity. Second, she put herself above both her fellow villagers and the story's strangers. City people—as these strangers are assumed to be—may have criteria , judgment but not more than she did. For was the pathetic joke not on the strangers? Was it not they, after all, in their eagerness to confirm their stereotype, who misjudged the whole by its parts—misjudged Escobines by a trio of decrepit dwarfs?
Strategically, Ofelia left out a part of the story often reported by others—that the Three Decrepits were, in fact, dressed in garments resembling those of respected elders but different from the latter in amusing detail, detail imperceptible to the decrepits themselves but labeling them as clowns and fools. By omitting this part of the story, Ofelia put herself above the general run of villagers who take uncharitable delight in this detail. Ofelia's deliberate omission allowed her to assume a pose more Christian than her fellow villagers, a pose that has never failed to annoy them. In this smug story, so economically told, Ofelia put herself above everyone, depicting both the strangers' and the threesome's judgment as very limited and her fellow villagers as uncharitable.
She had been put down decisively in her youth. Her fiancé, wealthy and returned from the Americas, without giving any explanation and in a manner unheard of in the village, abruptly canceled their engagement on the eve of the wedding. Gossip suggests the cause was an untimely abultamiento , swelling. Escobinas tell
me that in those days, in a woman who had recently conceived, the swelling of the neck normally preceded the swelling of breast or belly.[17] The fiancé, only recently returned, could hardly have been the cause of this swelling. Its untimely appearance is not likely to have created doubts about her virginity, for then as now weddings tended to be called after a woman found herself pregnant. Possibly, it was a question of paternity. More likely, however, the swelling cast doubt on the duration of Ofelia's beauty. This is what some Escobinas feel prompted the fiancé's abrupt move. At any rate, shortly after this putdown, she married a neighbor of more modest assets, with whom she had three children.
The firstborn daughter, as if to stave off any possibility of a mishap like her mother's, was married by poderes to an Escobino already resident in Argentina, long after it was no longer customary "to marry legally at a distance." The second daughter also emigrated to Argentina but remained single. And Alfonso, the last born, despite the fact that his economic success must have enhanced his marriageability, married an Escobina whose mother and aunts were all conspicuously goitrous. His, for him, uncharacteristic unenterprising way of searching for a partner suggests that the stigma of his mother narrowed the pool of partners he might draw from.
Ofelia concluded her story by showing me around the quarters of her house usually reserved from village eyes: a bedroom furnished in eyed walnut brought to a high polish, a gilded portrait of the Virgin of the Sacred Heart hung over the bed; the main upstairs room, a room seen by fellow villagers only on occasions when condolences are offered, a carved chestnut trunk of trousseau linens, and a delicate china service displayed in a fine walnut cabinet. Introducing me to her house in this way, Ofelia made me the witness of her religiosity, her material wealth, and her high housekeeping standards—attributes one might not suspect were one to rely on external cues: attendance rare at mass, activity rustic and outdoors, appearance conspicuously goitrous.
Subsequently, Ofelia and I had frequent conversations in her portal , the covered entrance that also gives access to what was once a pigsty but is now a service area she calls—rather grandly, shifting from the local idiom into Castilian—la bodega . The low rays of autumn penetrate the portal, warming her while she minds a grand-
child, mends, fluffs and restitches a mattress, and shells walnuts or chestnuts.
From time to time, she invited me again into her house but no farther than into the kitchen. There she showed me how to prepare her "special health salad," a dish not traditional in Escobines—made of onions and parsley from her garden, tomatoes, and canned tuna. While she exhorted me to follow her example, she evaded spelling out its health benefits, however, leaving me to surmise they lay in its iodine content. Unlike most other villagers, Ofelia could have learned from her daughters, who were sensitive to appearances and running a fashion boutique in Buenos Aires, about these benefits.[18] I did not question her further, for I responded to the boundaries Ofelia had set on our relationship. I should treat her with the special dignity she felt she deserved and never mention her goiter or the disrepute by which she always felt threatened.
She died of circulatory failure before I returned to the field. Had she been alive in 1984, I doubt that she and I would have more freely conversed about these health matters. Like so many victims the cause of whose disorder is mysterious or unknown, she excluded from our conversation any reference to her stigma.
"Cargando con los ruines" (Carting Our Worthless Men off to France) . Our second story takes place soon after World War I, when extranjeros , foreigners, were reportedly scouring the northern Spanish provinces for able-bodied men to repeople the French countryside. In German, the story would be known as Schadenfreude , joy in someone else's downfall. The sight of severe personal deprivation—the hobbling by of La Coxa, the stump-legged woman—tended to evoke this story, as did the stirring up of personally painful memories.[19]
It happened when I was a little girl, before the highway was built through town. The French came up El Camino Real (a dirt track connecting Escobines with downriver settlements) with carts and asked us for los que sobraban , our extra men. We didn't think we had any like that, not here where everyone is needed. Then they asked us for los ruines , our worthless men. They needed them in France, they said, to become husbands to countrywomen. Imagine that! Not that such a ruin around here could ever marry. Not the uncle of La Coxa! So they carted him off, muy volun-
tario , very willing. Other men accompanied him, you wouldn't know them because it happened long ago and they had few relatives. Those volunteers might not, around here, be seen as very fit, certainly not fit enough to become fathers and husbands, but they were good enough for the French women who married them and bore them franchutes , French brats. Imagine that, taking our derelicts and subsidizing them. War must have made France muy necesitáo , very needy indeed.
Members of backward and afflicted communities may assuage their feelings of deprivation by reminding themselves of the yet greater deprivation of others—too socially remote for solidary social identification. The story, told to me repeatedly before material conditions in the village had begun to improve at the accelerated pace of the 1970s, brought forth great hilarity. On these occasions, the tone felt like that produced in 1966 in an Escobines bar by a missionary's slide show depicting at a bush station mud-caked, be-feathered New Guineans, some of whom were deformed. This hilarity dismayed the missionary and puzzled me, until I was told, "It gives us the feeling, at last, of being somebody."
The deaf, poorly grown, and intellectually poorly endowed protagonists are put into these stories, in part, to demonstrate that Escobinos, whatever the visiting anthropologist might earlier have been told, are not all alike. Nevertheless, all the ruines the women told me about are male; Escobinas told me of no negative protagonists who were female. This concentration on only one sex suggests—if it is not an artifact produced by my conversing chiefly with women—either that such defects are found more often in the men of Escobines or villagers set higher standards for men. Women are the sex notably afflicted with goiter, and it is conceivable that women as a group would, for compensatory reasons, focus on the defects in men. A materialist explanation comes to mind, however, an explanation concerned with the value of labor: goiter runs no interference with the performance of "women's tasks," while neurological deficit interferes especially with tasks like sharpening and mowing, exclusively male activities.
"Rosita's Audacity ." This personal narrative is the kind of narrative most frequently told. Based on a real and recent event, it is intended to edify the listener and perhaps also validate the wisdom of the speaker.
Oh my lord, the woman you're looking for isn't here now. That Rosita (my elderly informant pronounces Rosita's name with uncolloquial precision, emphasizing the diminutive Castilian ending[20] and mimicking the gestures of a coquette) . . . is not here. She's gone off to marry and live in Sumonte don't you know? (Escobinas consider Sumonte a hardship post because it is situated two kilometers off the highway.) She bagged her man at last, gone down first to the city to get treatment for her . . . (her fingers and thumb describe the curve of her own neckline, but she avoids pronouncing the word pepu , goiter). She's no longer got it (rolling her eyes). Whatever they did to her down there . . . she married an old bachelor. Now Rosita and her husband are humped up with her in-laws, and they're harvesting escanda. (My interlocutor's voice drops.) She's pale and listless, gotten dried up, and her tongue's thick. Even her voice has changed. She's not pregnant. But she's no longer menstruating. Blood, you know, is everything.
My elderly informant, considered by her peers nongoitrous, is telling me how risky it is to interfere with either one's goiter or one's destiny. Escobinas accept medical intervention only after carefully considering its costs and benefits: as they see it, both goiterectomy and radiological treatment of goiter have been accompanied by severe negative side effects, not to be taken on lightly but acceptable when a goiter threatens to become cancerous. The older women had cautioned Rosita about these possibilities, but she had signed up for the operation anyway and was suffering now all the consequences the old wives had foreseen.
The style in which Rosita's story was told conveyed a further message. When she affected the name Rosita and had her goiter excised, she had taken on Castilian pretensions. Castilians, so far as Escobinas are aware, are not goitrous. Women who refuse to accept their divinely assigned destiny get penalized.[21] This affects their most interior femininity, their ability to bear children. Presumption backfires. Escobinas do not pretend to understand the mechanism by which such punishment is inflicted, but Rosita should have foreseen the practical consequences of getting operated for cosmetic reasons. Unlike the other goiters heretofore excised from Escobinas, Rosita's was neither asphyxiating her nor was it a life-threatening cancer, and she should not—certainly not while still "young" (of reproductive age)—have indulged her vanity.
Why, the women asked, did she have to be so bent on marriage? In their day, some tried to maintain, goiter made little difference in courtship and marriage. Even if nowadays goitrousness makes a young woman less marriageable, why should Rosita, already aging out of the marriage market, want so badly to get married? Why burden yourself with a man and in-laws in a hardship post? Why marry just to do field labor in Sumonte? Why huddle together with your parents-in-law, let your body be drained, and lose whatever harmony and prestige you have in your own home town?
Did she have to marry to have an offspring for her declining years? She would have been better off having a baby out of wedlock, as did her mother's cousins and aunts. Getting goiterectomized to get married was foolish. It ran the risk of losing her blood, her reproductive capacity. Is not marriage without the promise of any offspring pathetic?
Rosita paid a high opportunity cost for such a late and contrived marriage when offspring could hardly be guaranteed. Now her cautionary tale was presented over and over as a tale of vanity, false hope, poor judgment, and lack of resignation.
"The Story of the Crossbeam ." The last narrative offered here—a story within a story—illustrates the most privileged Escobino's preoccupation with disrepute. It was composed jointly by two men, an Escobino and a native of a village as remote as Sumonte. Both of the men are professionals: one an engineer (the first Escobino to ever have gotten a college education), the other a civil servant who has held several high administrative posts in counties on both sides of the Cantabrian range. They wrote this narrative into my notebook during the fiesta del Carmen of 1984—the fiesta that annually draws expatriates, tourists, relatives, and friends back to the village—and read it aloud to a small group of satisfied celebrants gathered together in the orchard of the engineer's weekend home in Escobines.
Even among annual festivities, the occasion was special—the first time the fiesta program was printed in Asturiano and local culinary and folkloric elements were featured as part of the festivities.[22] This year, Escobines emerged out of a long period of painful self-consciousness. Village development had become so accelerated
that the villagers' "inferiority" had become untenable both for themselves and for others. It was a propitious moment to speak to the myths, seen by outsiders as comic, that had long oppressed Escobinos.
It's been a long time, maybe centuries, that we Escobinos have in a denigrating way been called "the people of the crossbeam." It's been said we got this nickname because we tried to introduce a wooden beam into church, and instead of introducing it at right angles to the door, we tried to get it in crossways. When on a second attempt we failed to get it in we resorted to "greasing it up with butter" so as to get it into the temple.
This story is of course a reproach, meant to call into question the intelligence of Escobinos, our stubborn insistence on pursuing erroneous ways.
But since every village in this mountain region has its singular ways, and one can hardly prove that other villagers are better endowed with natural intelligence than are Escobinos, I, Domingo Montes Polés of Escobines, have set out to find a reasonable explanation for the emergence of this Story of the Crossbeam. Whatever the explanation, it has to accord with the undeniably high intelligence and common sense of Escobinos, with observations on other nearby villages, and with historical fact, which has presumably become distorted.
Reading about the Vaqueiros, the nomad people of the cow, gave me an illuminating insight. They alternate their place of residence, moving in search of graze between the lowlands and uplands. Long ago the people of the vega discriminated against them, prohibiting them from approaching the presbytery, the zone near the church altar. According to ancient formula, that zone is defined by the crossbeam reaching across the central nave. That crossbeam, in effect, divides the church into two zones—one for the clergy and nobility, the people of category; the other near the door, reserved for the lowly.
This separation of classes was taken in Pravia to such an extreme that a sign specified, "Beyond here the people of the cow may not proceed."[23] In Escobines no such sign, as far as we know, was ever posted. Nevertheless, the early aristocracy of our parish seat was aware of the immense stretch of good grazing land lying between it and puerto and very likely called in a group of Vaqueiros to exploit, on a profit-sharing basis, that graze for veal and milk. This arrangement seems to have produced the people of Escobines, different from those already residing in the area.
The rental agreement with the señoritos, the local aristocracy, put the newcomers into an inferior social position, normal to the feudal period. Social hierarchy had to be made manifest whenever the parish in all its
social and occupational levels—nobility, clergy, and commons—came together. For this there is no better occasion than mass. On such occasions the nobility made a point of manifesting its "superiority." It did this by preventing the lowly common people, the Escobinos, from "advancing beyond the crossbeam."
Small wonder Escobinos came to be known as "the people of the crossbeam" and small wonder, given the way we habitually mock each other, that this nickname came to be elaborated as a funny story—persisting to this day.
This story, speculative to be sure, starkly accuses us Escobinos of being the area's biggest asses. We, however, rejoice in our donkeyness, for against all odds we set goals and stick to them with tenacity.
Boldly then, we Escobinos stand tall, glowing in our patent and smashing reality.
This newly minted mythological explanation[24] for the local origins of disrepute delighted his audience. As social history it had a basic truth. Butter had been, in previous centuries, the medium of exchange between the lowly and the noble, though the more common fatty element in the diet of Escobines had been sheep fat. People from the uplands, unable to grow much grain, owed butter (made from cow's milk) instead of grain to their señores and retained very little butter for their own consumption.[25] In this sense, butter, as in "buttering up," was less a dietary substance than the medium of exchange symbolic of relations between the lowly and the noble. Butter was produced by those in intimate contact with animals and consumed freely by those who were not.
The consumers of butter were, indeed, the "people of the vega." These local gentry both consumed the Castilian olive oil brought down from the passes and the cream skimmed off by the local "donkey brains." Domingo rightly pointed out that they dominated, in part, by denigrating those whose close association with the animals marked them as inferior. But Domingo failed to mention—and this omission is significant—the other reason that Escobinos could be looked on as lowly: the deformity prevalent among them.
That omission from his explanation—and we cannot suppose that he had failed to hear about dietary deficiency and IDD, for the year was 1984, when the official campaign against goiter and cretinism was launched—suggests just how unspeakable goiter's stigma was even to him, intelligent and well grown. He was not goitrous, but
his sister, perennially hoarse, and his mother and all his aunts were conspicuously goitrous. The affliction did not prevent his extended family from running a very successful bar, store, and banquet hall in the center of the village. But it did make it easier for customers to grumble about the "burros y papudos," donkeys and defectives, who allegedly and only on rare occasions gave unsatisfactory service.
Domingo did approach the matter of village disrepute in several ways, however. He symbolically bridged the gap between classes and codes—between history and myth, between Castilian and local ways of speech, and between elaborated and restricted codes. In this way, he evoked the efforts exercised by the Asturianistas, the advocates of the vernacular tongue, to bring about significant change in attitudes toward local and provincial culture. His effort is similar to the efforts, also, of the eradicationists bent on eliminating deficiencies in the Asturian diet, as will be seen in chapter 7. Domingo's "origin myth," offered as an explanation for the disrepute he and his fellow Escobinos have long experienced, showed how effective such symbolic efforts can be in preparing marginated peoples to become confident members of the social mainstream.
Folklore as an Epidemiological Tool
The social scientist attuned to a people's lore will find history and social change reflected in it, although a public fond of "timeless" tales might resist such findings.[26] These Escobino narratives we have before us are grounded in time but also, to be sure, have a thematic quality that cuts over time and space, a quality that—once the search is made for them—will undoubtedly be found among other people unknowingly afflicted by toxic substances, mysterious microbes, and unidentified deficiencies. Should epidemiologists also wish to ascertain whether an anachronistic disease, such as endemic IDD, has actually disappeared, they might do worse than search out the people who have originated and recounted narratives in which such afflictions are reflected. Let me review these thematic reflections here.
The first story, "The Three Decrepits," records a rising self-consciousness as outsiders increasingly penetrate the villagers' isolation. The second, "Carting Our Worthless Men off to France," records villagers' emergent awareness of problems among other
European peoples. The third, "Rosita's Audacity," records the wary integration of Escobinos into national life and, especially, the nation's health and welfare programs. The fourth, "The Story of the Crossbeam," deals both with the long ago mythologized past and the acute sensibilities of the present; it forthrightly addresses the contempt that for so long villagers have suffered, suggesting that Escobinos are ready now to take the donkey by its tail, to reinterpret the stories of the past to serve their own future.
All these narratives point to affliction. The first one attempts to force a continuum of deficit into a simple dichotomy of "fit and unfit," a reassuring scheme, as comforting to Asturians as to the mestizos described by Greene. The second narrative takes a comparative stance toward affliction: how funny and reassuring it is to learn of other people worse off, reassuring to those who have not a clue that their own affliction is preventable. The third narrative struggles between accepting one's defect fatalistically or taking the risk of getting it treated. The fourth finds physical affliction too painful to deal with but contrives an upbeat explanation for disrepute that puts mockery and resentment into a safe historical corner.
These are narratives of the underdog and of the marginated man and woman. All are related to affliction and to the disrepute engendered by affliction. The narratives have identifiable themes such as embarrassment, insistent one-upmanship, and search for revitalization.
In a region where narratives like these are distributed unevenly, where they occur repeatedly in certain villages and not in others, such narratives suggest the presence of "mysterious" disorders and diseases that have yet to be explained—and if possible, prevented. Likewise, in a region where marginated ethnic groups are thought to be of mysterious origin, denigrating stories focused on them may suggest, as well, the presence of lingering diseases, diseases likely to be anachronistic, that will hopefully be prevented.
Narratives like these may be seen then as indexes of affliction—indicators of possible disease, indicators that need to be followed up by closely examining the populations to which they point. Local narratives, the ethnographer knows, are revelatory in a variety of ways and are surely revelatory about a people's health and disease. Collections of such narratives should be a part of the survey techniques aimed at revealing lingering and needless affliction.
Chapter Seven
Advocacy and Opposition: National and International
Introduction
This chapter examines what the foregoing ethnography of affliction could not address: the attitudinal, economic, and political forces outside the afflicted community—whether at the regional, national, or global level—which until 1984 impeded the initiation of iodine prophylaxis in Spain.
It has been shown that neither underdevelopment nor local resistance posed serious obstacles to prophylaxis. Thus, we are left with the question that has animated this investigation from the outset: what nonlocal obstacles prevent prophylactic knowledge and techniques from getting to the people, when these are not only well established in science but have long been proven to be cost-effective? What, beyond the confines of local communities, are the obstacles that continue even today to impede the diffusion of simple facts and useful techniques? Paralleling the stream of events leading up to the prevention of scurvy in the British navy or the removal of asbestos in American schools, this chapter may be seen as a case study in the diffusion (or nondiffusion) of knowledge and the development (or nondevelopment) of the public's "political will," which WHO's present eradication team sees as so necessary to getting a project moving (DeMaeyer, Lowenstein, and Thilly 1979).
The chapter is divided into five parts. The first introduces an-
other, even more deeply afflicted, region of Spain, Las Hurdes, so that we may obtain a compressed overview of how, over a long period of time, IDD has been represented and managed (or misrepresented and mismanaged). Las Hurdes is appropriate for this overview because its deformities, dwarfism and cretinism, in contrast to Asturias, have long been subjects of published inquiry and salient in the public mind. The second part examines attitudes toward goiter and cretinism and toward rural people in general, as expressed in public health policies of the preprophylactic period. The third part concentrates on the prophylactic era, when silent opposition, vested interests, and threatening civil war defeated the advocates of prophylaxis. The fourth part examines prophylactic developments in the context of the economic priorities and political constraints of the Franco era. The fifth part examines the more immediate antecedents of the very recent campaigns to eradicate endemic goiter and cretinism in Spain.
Las Hurdes: The Realism and Surrealism of Iodine Affliction
Las Hurdes is a mountainous enclave in west central Spain, in northern Cáceres, close to Portugal. Because of its "monsters" and "backwardness," it has long been subject to travelogues and medical studies. It was also the subject of a "surrealist" film by the famous Spanish filmmaker, Luis Buñuel. It is therefore emblematic, for myth and polemics surrounding the Hurdenos' plight unite into a highly charged whole. For many, Las Hurdes stands for isolation, affliction, neglect, subhuman living conditions, and subhuman beings.[1] For some medical investigators, Las Hurdes has represented the natural field experiment.[2] For other social and medical investigators, Las Hurdes has stood as an unconscionable expression of disorganization and misdirection in Spanish medicine and public health.[3] For church spokesmen, Las Hurdes has represented the investment of church and state in compassionate and even visionary efforts.[4] For the purpose of gaining an overview of iodine prophylaxis and the obstacles to it in Spain, one can hardly do better than examine a chronology of missions to, and representations of, Las Hurdes.
Conspicuous efforts on behalf of Las Hurdes began in 1922
when the most famous Spanish physician-statesman of the twentieth century, Gregorio Marañón, who had come to recognize this remote area as a dramatic instance of endocrine disorder, urged the king to accompany him there on a visit. This visit triggered royally sponsored development programs and the creation of the Goiter Commission, headed by Marañón himself (whose work is examined below).
As a result of this royal attention, Hurdeno children became, though only briefly, the first experimental subjects of dietary iodine supplementation in Spain. Pregnant Hurdena women were also offered prophylaxis "as a wedding present, to avoid the emergence of the goiter normally expected during pregnancy" (Vidal Jordana 1924, Marañón 1927).[5] Before the end of the 1920s, however, both programs were dropped in favor of more general measures aimed at modernization.
Roads were gradually built into the area, followed by welfare and education programs brought in under the auspices of a charitable foundation (Patronato de las Hurdes) headed by Marañón during the few years of the Spanish Republic. It was in this period that Buñuel filmed Tierra sin Pan (1933), Earth without Bread, often seen abroad as the last of Buñuel's surrealist art films.[6] It was made, according to Buñuel (1982), to draw attention to the plight of the Hurdenos and to prompt long-promised reforms.
The film depicts Hurdenos in a state of perpetual hunger, forever foraging in scrub and forest for whatever the land may offer. Their faces are haggard[7] and their feet bare in a rough and thorny landscape.[8] Normal-appearing Hurdeno men are shown only in labor migration, walking off in single file to the central plateau to mow grain for absentee landlords. Goitrous women, dwarfs, and cretins are filmed from low camera angles that emphasize monstrous deformations. Even the fosterage of abandoned city children,[9] official wards of nearby cities and one of the few sources of local income, was turned against the Hurdenos.[10] For these children were assumed to be syphilitic, having been born to unwed mothers presumed to be prostitutes.
Earth without Bread, surrealist or naturalist, appeared so excessively alarming that Marañón's foundation refused to subsidize a sound track for the film (Buñuel 1982), and officials prohibited its showing.[11] The Franco regime also withheld it from public view.
Indeed, Spanish audiences did not see the film until the winter of 1982–83, soon after the Socialists were voted into office. Since then, it has been shown several times on the national channel.
Nevertheless, toward the end of the 1940s, even without such cinematic promotion, the Franco regime in close alliance with the church began to vigorously promote human and economic development in the area. The aim was to turn Las Hurdes into a symbol of governmental benevolence and national "redemption" (de la Vega 1964). The Ministerio de Gobernación (Ministry of Internal Affairs) sponsored and ultimately oversaw most of these "redemptive" activities, which gradually eliminated malaria and hunger and according to de la Vega, also eradicated goiter (1964).
Indeed, converging forces had the effect of making goiter in Las Hurdes seem to disappear. State-sponsored labor-intensive reforestation after mid-century gradually replaced the forest products, the chestnuts and acorns of the subsistence economy, with a rapid growth timber economy and with previously scarce cash. Such changes replaced the goitrogenous staples of the traditional diet with cultivated and commercial foods. In the course of this dietary transformation, the elderly bearers of gross goiters gradually passed on, while others, less grossly afflicted than their elders, gradually came into maturity.
Popular mythology regarding the people of Las Hurdes held that they were "crossed with wolves," "degenerate vestiges of a primitive race," "descendants of escaped convicts, Moors, or Jews," or simply "representatives of the New World in Spain"[12] or "our own interior Guinea."[13] The traditionally high incidence of disfiguring goiters and dwarfism surely contributed to these myths of different racial origin, or racial degeneration.
There was also an identity dynamic at work. As Spain in the nineteenth century was forced to withdraw from its colonial and missionary enterprise, the foreign "other" was discovered closer to home.[14] Hurdenos conveniently came to represent that other against which normal fitness and level of civilization could be measured. As in Strabo's time, descriptions of these humanoids were disseminated among "civilized peoples" both Spanish and foreign. For instance, the French Guide Michelin in the 1970s still assigned two stars to Las Hurdes, in part because of the picturesque nature of the people, a "picturesqueness" the Hurdenos occasionally ex-
ploited and, as far as we know, came to resent and resist only recently (R. L. Fernandez 1986:423–427).[15]
Whatever the dynamics of identity among marginated peoples of the peninsula (see chap. 3), Spaniards after mid-twentieth century had the impression that the prevalence of gross deformity was declining in places like Las Hurdes. This impression was correct insofar as the "irreversible cases, God's preferred children" (de la Vega 1964:88), gradually lost their visibility and diminished in number as the severity of deficiency declined. The precipitousness of the drop was more reassuring than real, however, because many of the afflicted, having become institutionalized, ceased to be on view.
But to one group of medical workers—long focused on Las Hurdes and located at the Instituto Marañón, Spain's national center for experimental thyroidology, a branch of Consejo Superior de Investigaciones Científicas (CSIC), which, by 1989, had become the Centro de Estudios de Endocrinología Experimental—this decline in overt pathology still left a great deal of room for improvement. For years, a team headed by Dr. Francisco Escobar del Rey had been monitoring the dietary and endocrine state of Hurdeno children in feeding programs, finding the rate of urinary iodine excretion (chap. 2) generally low[16] and endocrine disorders alarmingly high, especially among those not included in the feeding programs.[17] Escobar used these findings to demonstrate that consanguinity plays a minor role, if any, in the high incidence of goiter and other endocrine disorders found among these children and thus ruled out consanguinity as the primary cause of IDD in Las Hurdes. He argued, both in foreign and in national journals (Escobar del Rey et al. 1981a , 1981b , 1984; Escobar del Rey 1983, 1985), and most recently in a special issue of Endocrinología (1987), that only generalized iodine prophylaxis would lower the incidence of endocrine disorder in all the children.[18] In 1983 and 1984, he circulated a letter, under the letterhead of the Subcommittee for the Study of Endemic Goiter and Iodine Deficiency of the European Thyroid Association, later published in Lancet, drawing attention of colleagues both at home and abroad to the continued un availability of iodized salt in Spain. This circulating letter is considered instrumental in "embarrassing the Ministry of Health" and animating it to correct the situation.[19]
Escobar's findings and recommendations were hardly contrary to expectations or new to thyroidology, but their publication in Spanish professional journals and in Lancet makes them noteworthy. Coming from a thyroidologist esteemed both by his national colleagues and by the international members of the WHO goiter eradication team,[20] the carefully presented findings suggest that Escobar set aside his experimental work (at the leading edge of thyroidology) to convince his colleagues in both medicine and public health to set aside their hereditary thinking. Where the health of marginated people is concerned, such thinking may often be a key obstacle to prophylaxis.
Attitudes: Medicine for the Rich, Charity for the Poor
Hygienic life becomes a necessity in individuals and communities only when culture [education] and civilization make dirt incompatible with human dignity and prosperity. If Spanish sociologists and legislators have not been able to broadly promote hygienic practices, it is because progressive ideas cannot take root in the generally ungrateful, uncultivated, social terrain that is Spain.
—Ministerio de Gobernación, 1909[21]
However tautological the belief expressed in the epigraph—that it is pointless to offer health education to poorly educated people and that people living in ignorance, hunger, and filth cannot be educated—it expresses a long-standing attitude underlying the inaction with which we are concerned here.[22]
The attitude is well known, even if only rarely so explicitly stated. When, in 1898, the Spanish medical fraternity (Colegio Oficial de Médicos ) promoted programs of voluntary health insurance and social security[23] agreed to administer them, rural people were excluded from coverage. Perhaps, from the point of view of the planners and physicians, who were urbanites, the very groundedness of people living on the land made insurance unnecessary, for it gave rural people the kind of security that the urban sectors lacked. In any case, private and public charitable institutions,
beneficencias, could service those in dire need, the certified poor and the officially landless.
Beneficencias were custodial institutions run by the church or local government. Medicine and public health, meanwhile, were under the Ministerio de Gobernación, the Ministry of Internal Affairs, which exercised no control over the beneficencias. This division of administration distributed authority and concern over health and welfare unevenly: "cultured" urbanites were the major recipients of medicine and public health, and "ungrateful and uncultured" country people were the recipients, at best, of charity.
This voluntaristic and class-based approach to medicine and public health was to prevail long beyond the turn of the century, even after rural people were drawn gradually into the compass of health programs. Vaccinations, for example, while widely offered, were not made obligatory even though the hazards of this voluntaristic approach were pointed out by professors in the national school of public health. Every year's new crop of medical students would hear of the Galician village so mistrustful of government and its newfangled medicines that villagers unanimously refused vaccination and were devastated in the next epidemic. The lesson students generally extracted from such anecdotes, however, was of the pervasiveness of villagers' ignorance, mistrust, and foolhardy stubbornness, attitudes that they, as future public health officers, could hardly expect to surmount (R. L. Fernandez 1986:436–444).[24] However infrequently villagers actually refused such vaccinations, the relating of this classic incident sufficed to corroborate the complacent view that public health largely wasted its efforts trying to serve the rural poor.[25]
This view prevailed only as long, of course, as the elite and growing middle classes of the nineteenth and twentieth centuries failed to experience any threat from the lower classes. Physicians and public health officers had in the mid-nineteenth century mobilized and proved themselves capable of acting decisively, even in the countryside, when urban Asturians felt themselves menaced by infectious epidemics. Indeed, Losada, the Asturian physician, was decorated with the government's prestigious Cruz de las Epidemias for carefully having mapped the distribution of cholera and typhus throughout rural and urban Asturias. Losada's epidemiological charts enabled localities to take specific and local-
ized preventive measures, first in 1834 and again in 1834, to stem the spread of these dreaded infectious diseases (Fernández-Ruiz 1965:164).
With the momentum of that success, Losada went on in 1841 to map with equal meticulousness the distribution of goiter in the province. We know that goiter was far more prevalent in wider Asturias than it is now and therefore could also be seen as a threat to urbanites.[26] The technique this time, however, ruled out infection as a cause and suggested no practical action, so that Losada's document has been lost to all but some private archive (Fernández-Ruiz 1965). It is perhaps speculative to ask whether the findings, mentioned only briefly by Fernández-Ruiz, dropped out of sight because they failed to support hereditary causation, the favored hypothesis.[27] Without evidence supporting either dietary or infectious causation, public health officers could safely revert to the traditional view and regard goiter as merely a condition of existence—if damaging, then damaging only to its victim. In other words, it could safely be ignored.
This complacent stance toward chronic and endemic conditions may be accounted for in part by lack of funding, a financial constraint that persisted into the late twentieth century. It became increasingly modifiable, however, when not only middle-class people but governmental or larger financial interests felt themselves threatened, as can be seen in examples taken from the Franco era. Late in the 1960s, officials were prompted to clean up a localized source of contaminated water in a major city only when the worker-residents of the "red" neighborhood dependent on it threatened to strike. Similar foci of localized noncommunicable diseases in depressed parts of the country were cleaned up only when in the early 1970s the Ministry of Tourism, hearing of foreign tourists' apprehension regarding their health while in Spain and anxious to ward off any possible loss of foreign exchange, demanded immediate remedial action. Public health was able to respond to that demand only when the Ministry of Tourism shifted its own funds to invest in improving the water system.[28]
A curious set of works known as topografías médicas, medical geographies, which appeared over a thirty-year span from before the turn of the century, point up the pervasiveness and depth of the general attitude toward chronic conditions. The series was orig-
inally sponsored by Roël, the Asturian physician bent on refuting French defamatory images of pellagra. He was to become an eminent member of the Spanish medical establishment, heading up beneficencias and receiving, like Losada, the Cross of Epidemiology and a seat in the Spanish Academy of Medicine. Accorded such status, he made it his mission, in the closing years of his life, to redeem Spain from the malign effects of consanguineous unions. Indeed, after the pellagra affair, he insisted more than ever that chronic disease in Spain stemmed from failure "to renew the blood" (renovar la sangre ; Fernández-Ruiz 1965:177). He also resolved, in his closing address to the academy, that he would redeem Spanish medicine from ignominy by founding
a national medicine grounded in the geographies of medicine of our fatherland. These geographies will emancipate Spain from its shameful dependence upon foreign medicine, which has humiliated and enslaved us (ibid.).
Roël willed his large fortune to make that goal possible. The academy henceforth, for at least thirty-five years, annually awarded prizes in Roél's name to what it judged the best topografía médica. A number of these prize winners are situated in Asturias (Vilar Ferrán 1921; Villaraín y Fernández 1923; Junceda 1936).
A singular feature of these topografías is a section called antropología, anthropology (e.g., Jove y Canella 1932). We are hardly surprised that customs and dress are discussed in this section, but we are more than a little surprised—given the explicit social and medical goal of these works and the state of biomedical knowledge about the cause of endemic goiter and cretinism—that deafness, dwarfishness, goiter, and "collective behavioral traits" such as sluggishness or illiteracy are also discussed as if they were ethnic traits or immutable individual dispositions. These "anthropological characteristics," since they are neither discussed in other sections such as Diet, Prevalent Diseases, or Pathology nor targeted for treatment or prevention—represent the hereditary view, apparently unshakable even in the second decade of the prophylactic era.
The medical geographies must not be understood as representing, at the time of their publication, the forefront of Spanish medicine. They do represent, however, a widely shared classificatory
scheme endorsed by the medical profession in Spain through at least the first third of the twentieth century. This scheme views endemic goiter and cretinism as immutable. It holds that it is the nature of some populations, especially when inbred, to be goitrous and cretinous. It implies that environmental or nutritional intervention cannot remedy this situation. If in the Spanish literature of the time that view is not explicitly stated, it is because it went uncontested and was not successfully refuted until the 1980s. Refutation of the hereditary view finally paved the way for prophylaxis.
Withhold or Divulge: Informing the Public
"The Grand Detour": A Career both Medical and Political
Spain's best-known twentieth-century physician-statesman and polymath-essayist, Gregorio Marañón (1887–1960), knew the breadth of endemic goiter and cretinism in Spain and was ideally situated to endorse and promote iodine prophylaxis at any level, local or national. His opposition to prophylaxis—his reasons for opposing it and his methods of doing so—must be closely examined to understand the obstacles to prophylaxis in Spain. Understanding his opposition will allow us to come to a fuller understanding of the kinds of subtle obstacles that may anywhere impede the flow of practical, health, and nutritional knowledge.
Marañón came into full professional and political stature at the beginning of the prophylactic era. He imported endocrinology into Spain and held the center of Spanish endocrinological teaching, investigation, and publication for at least two decades (Glick 1976). In the 1950s, he was appointed head of the Institute of Endocrinological Research, an arm of the prestigious CSIC, which after his death was renamed the Instituto Marañón.
So influential was Marañón, and seemingly so irreplaceable, that the Chair in Endocrinology created for him at the Universidad de Madrid remained vacant, at least through 1984. His medical publications were extensive and widely translated, and his basic text, Manual Diagnóstico Etiológico, lives on, having been repeatedly reissued, most recently in 1984 (Marañón y Balcells 1984; see
R. L. Fernandez 1986:386). His nonmedical publications in history and biography and his essays and reviews were equally extensive, compiled in the eight thick volumes of his Obras Completas . The 1987 centenary of his birthday was marked by the unveiling of sculpture, commemorative ceremonies, and a spread of essays in the nation's most prestigious newspaper, El País, written by political, literary, academic, and medical figures. Marañón is such a national resource even today, more than a quarter century after his death, that he is still above reproach. Research physicians who have labored to introduce prophylaxis in Spain still refuse to subject Marañón's position to critical examination (see Aranda Regules et al. 1986:9, Escobar del Rey 1987), as if doing so were to jeopardize the very gains they have made in overcoming iodine deficiency. Indeed, Endocrinología's 1987 supplement on endemic goiter and iodine deficiency in Spain is dedicated to him.
Moreover, Marañón's reissued and translated works and works derived from his own publications also are not subjected to critical scrutiny. For instance, The Climacteric (1919), translated into English and published in 1929, presents Marañón's views of the psychoendocrinological crises of menopausal women. These ideas were accepted by his colleague Botella-Llusía and successively elaborated from the 1940s to the present in many editions of the Endocrinology of Woman, a work well known to Spanish medical students. This work was translated and published in English in 1973 and reviewed briefly in the Journal of the American Medical Association (Dec. 10, 1973; 1363). No mention was made of the antiquated sections dealing with goiter, cretinism, and nutritional deficiency—sections that only adumbrate Marañón's position. Cloaked in the mantel of Marañón, Botella-Llusía recently served as rector of one of Spain's major universities.
As Spain's top endocrinologist, Marañón received difficult thyroid cases from all parts of the country. Las Hurdes so impressed itself on him as an example of misery, and perhaps also as a promising field site for endocrinological research, that in 1921 he brought, as we have said, the depressed area to the attention of the king, who, in turn, called for creation of the Goiter Commission, naming Marañón its head. In this capacity, Marañón persuaded the king, in 1922, to accompany him to Las Hurdes, urging on him, once he had been duly impressed by deprivation, to pro-
mote development of the area. Marañón, it is clear, was already convinced of the solution: the poor and monotonous diet and unhealthy inbreeding could gradually be relieved by opening Las Hurdes to the modernizing flow of goods, people, and ideas. This could only be accomplished by building roads and establishing institutions under the auspices of the crown (Marañón 1921). The royal journey may well be seen as the first exhibition of Marañón's political persona.
That he was bent on gradualism rather than rapid alleviation of specific deficiencies can be surmised from his opposition to prophylaxis, an opposition he held well before the 1927 Swiss goiter conference, where he explained his position relatively briefly (1928a ). To his colleagues in Spain, he expressed himself more fully, speaking of preserving, uncontaminated by non-Hurdeno intrusions, the human genetic resources of Las Hurdes (1927, 1928b ). The interests of the pure scientist committed to the rebirth of Spanish science always struggled in Marañón with those of the clinician and public health officer, not to mention those of the statesman and polymath intellectual.
Marañón's Goiter Commission went on to survey numerous endemic areas in Spain, including Asturias. He presented its results in 1927 at the First International Endemic Goiter Conference, in Switzerland, where the roster listed him as Spain's only delegate (Schweizer Kropfkommission 1928). Other countries, by contrast, sent several or even many of their most distinguished thyroidologists and public health officials.[29] The Swiss conveners had two goals: to provide a forum for research into endemic goiter and cretinism and to divulge knowledge of prophylaxis, that is, of "full salt," Vollsalz, sal completa, or iodized salt (Eggenberger 1928).
Many of the conference papers were of high quality, supporting arguments with careful, well-ordered detail. Marañón's paper, a shortened version of a lengthy but impressionistic monograph on endemic goiter and cretinism he had earlier presented to the Spanish Royal Academy of Medicine (1927), was descriptive. Arguing on the basis of having treated thyrotoxicosis in patients who had ingested iodine abusively (for weight reduction), he could not endorse the use of dietary iodine supplements. He called instead for economic development of the afflicted area. He called special attention to two afflicted areas, Asturias and Las Hurdes. In the
former, he found enormous goiters and a high incidence of cretinism; in the latter, he found smaller goiters accompanied by a broader spectrum of affliction and a higher incidence of dwarfism. He attributed both endemias to isolation, consanguinity, and a monotonous diet, acknowledging that in the Hurdeno diet the lack of bread and foods of animal origin imposed unusual stress. Marañón dismissed "hydrologic" and "tellurgic" theories as unable to account for the endemia in these areas, positing a not-yet-identified biologic vector that "manifests itself only where poverty and isolation predominate." He saw iodine prophylaxis as too specific to alleviate the wide spectrum of undernutrition and misery seen in Las Hurdes, and he proposed instead that roads be brought into the remote endemic areas on which "commerce will flow. These will bring the benefits of civilization. Development will reduce the monotony, inbreeding, and reliance on local, inadequate foodstuffs" (1928:396).
At the 1927 conference, in other words, after being exposed to a wide range of scientific arguments testifying to the efficacy of iodized salt, after taking a field trip to an asylum of dwarfs and misfits, and after visiting an endemic Swiss village in which, because of iodine prophylaxis, cretins were no longer being born, Marañón still proposed economic development as the appropriate response to endemic goiter and cretinism in Spain. He seemed unaware that this kind of approach had already been discredited as "the Grand Detour" by one of Switzerland's early advocates of prophylaxis (Hunziker 1924). He was to ignore iodine prophylaxis and uphold economic development for the remainder of his career.
His scientific and humanistic personas, it should be pointed out here, were invested in gradual improvement (assumed to accompany economic development) rather than in the abrupt elimination of iodine deficiency. He championed Las Hurdes as "an excellent field in which to pursue the study of endemic goiter" (1928b :398). Indeed, because foster children introduce undesirable "confounding variables" (1928b :399) into studies of consanguinity, he recommended suppressing mercenary fosterage. Consanguinity and lineages were to Marañón a matter of long-standing concern, for Marañón the historian and humanist was soon to write a book based on the meticulous study of an aristocratic pedigree.[30] One can imagine his interest in preserving for Spanish science and similar
future study a remote endemic area rich in investigative possibilities for endocrinology and human genetics.
The afflicted Hurdeno population remained so rich in investigative possibilities, in fact, that, as mentioned above, in 1984, the médico titular had to protect Hurdenos from too many poorly designed social and medical investigations. "If at one time the Hurdenos were a neglected population, they are now the most overstudied, exploited population in Spain" (R. L. Fernandez 1986:426).
Marañón may not have intended in any conscious way to preserve affliction. He may, in the 1920s, in the bloom of professional and personal political success and an improving economy, have believed that economic development would really proceed as projected, bringing the benefits of commerce and civilization and eliminating dietary deficiencies in Las Hurdes. But he could not have been so sanguine when, in the 1930s, Buñuel was making his film and the Republic's rural programs were foundering. Even then, after having witnessed Vidal Jordana's small-scale success with iodization (Vidal Jordana 1924), he failed to endorse iodized salt to achieve the limited goal that was then feasible, as we will see shortly.
The reason for his opposition to iodized salt became plainer at the Second International Goiter Conference, held in 1933 in Bern. Another Spanish delegate, Carrasco Cadenas, reports on Marañón's views expressed at the conference, claiming to have repeatedly seen in his clinic cases of iodine abuse: self-administered to raise metabolism and reduce weight. Such self-medication, according to him, had all too frequently resulted in thyrotoxicosis, an impressive medical emergency (Carrasco Cadenas 1934a ). Being an attentive clinician, these cases must have impressed him deeply. Indeed, "Marañón was a man who had a remarkable memory for clinical detail; he could recall the details of any case he had ever operated upon."[31]
By contrast to these cases of self-induced thyrotoxicosis, the ordinary cases of IDD, however numerous, suffocating, or disfiguringly "big as winebags" (Casal 1959, ref. 1759) rarely made their way to the clinic. These noncases may impress an anthropologist living for an extended period in afflicted villages, but outside the operating room, Marañón the clinician could hardly
have been as impressed. Indeed, Marañón the statesman-politician turned such victims, who rarely if ever were to become patients, over to the king. In other words, he compartmentalized his clinical and political personas, thereby separating therapeutics from prevention.
This interpretation, discounting any pecuniary or self-promoting motives, finds that the statesmanlike qualities of Marañón and his nutritional understanding weighed (from the point of view of prophylaxis) all too lightly against his medical knowledge and skill. In the end, he responded to the clinical demands for therapy, not to abstract needs for prevention.
It is difficult, however, to so generously interpret his continuing opposition to prophylaxis after the war, when he simply avoided addressing the issue. Silence alone need not mean opposition, but Marañón headed the institute dedicated to thyroidological and endocrinological research and, as far as can be inferred from the record, supported within those precincts no research on iodine prophylaxis. We will see shortly that, on however limited a scale, such research was going on elsewhere in Spain under other auspices.
After agreeing to preface a bicentennial edition of Casal's Historia natural y médica del Principado de Asturias (1759), Marañón rejected a singular opportunity to reopen discussion of the "regional disease." The preface by Buylla y Alegre of a previous edition (1900) had allegedly brought Casal up to date; there was therefore even a precedent for updating the famed medical geography. But Marañón writing eloquently on behalf of the eighteenth-century physician-investigator, turned down this last opportunity of his lifetime to bring prophylactic endocrinology in Spain within the compass of universal biomedical understanding.
Undoubtedly, his age, character, and vision of himself as well as his intellectual beliefs played a part in that silence. Marañón was concerned throughout his life, both as a physician and as a man who played a role in historic moments, to avoid polemics.[32] His belief in an endocrine base for innate dispositions, which he had explored in a number of works both historical and medical (see n. 30), remained apparently unshakable in these declining years. He did not believe what his eyes did see, the transformation— merely by the ingestion of a dietary supplement—of lethargic and
forgetful hypothyroid organisms into euthyroid individuals functioning in society with vigor and alertness.
His prestige in the Spanish system of seniority and hierarchy may have insulated him from challenges by Spanish colleagues, whether on the fixity of innate disposition or the merits of prophylaxis. But was he never challenged on these matters from colleagues abroad? He was well traveled, and he had long and vigorously espoused the idea of sparing the patient (Laín Entralgo 1964). Moreover, he had deliberately imported medical knowledge from abroad and stimulated Spanish colleagues to practice the critical scientific discourse he found so "thin" at home (Glick 1976).
Given this record, one might wonder if, confronted by foreign endocrinologists of international stature, such as those serving in the 1950s on the WHO eradication team, Marañón might not at last have reconsidered his opposition to prophylaxis. Is it too speculative to ask if the WHO thyroidologist team might not have spared one generation of Spaniards the debilitating effects of IDD? Might not similarly distinguished colleagues from abroad—mindful of Marañón's concern to introduce critical discourse into Spanish medicine—have been able to persuade him to open a national forum on iodine prophylaxis? What may have stood in the way of such an attempt at collegial persuasion is the team's resignation in the face of what they believed were national differences, however wrongly perceived. Here such stereotypes can be suggested but not pursued. They seem of the same order as those seen previously—perceptions preventing for decades the extension of public health measures to rural Spanish populations.
Carrasco Cadenas: A Moment of Truth but a Failure to Persuade
Marañón could have opened a forum on prophylaxis, but for a number of reasons about which we can only speculate, he did not do so. A leader in public health who tried but failed in his attempts to open such a forum was Dr. Enrique Carrasco Cadenas. Carrasco argued cogently on behalf of prophylaxis in the first of a special series of lectures, "Three Topics of Alimentary Hygiene in Need of Urgent Attention by Public Health," that he delivered in 1934 at the National School of Public Health, where he was a professor.
An academic colleague of Marañón's in the 1930s, he also served with him on the editorial board of Revista de Sanidad e Higiene Publica (RSHP) , the Spanish journal of public health, under whose imprimatur the lectures were published.
He gave the first lecture, "Endemic Goiter and Cretinism as Diseases of Nutritional Deficiency: Their Prophylaxis by Iodine," not long after returning from the Second International Endemic Goiter and Cretinism Conference, which he had attended with Marañón. Considering himself a loyal disciple of Marañón's, he based his argument whenever possible on Marañón's teaching; indeed, as Marañón's student, he was bound by the Hippocratic oath—as understood by his Spanish colleagues—to avoid contradicting his master-teacher (Guerra 1970:419–453). Acutely aware of their differences with regard to the virtues of iodine prophylaxis, he nevertheless deferred as much as possible to Marañón so as to appear to comply with that tradition. The required deference, bordering on obsequiousness, detracted from his argument. Here are some illustrative passages.
Marañón's original work "Goiter and Cretinism in Spain" is a key work known by everyone. Its publication signals the beginning of an era that still awaits new contributions (1934a :5). Marañón's work demonstrates the anti-toxic and anti-infectious function of the thyroid . . . functions carried out by internal secretion. When the organism is stressed it requires more of those secretions and hence the thyroid demands more of the raw material from which it produces thyroxine (ibid.:53). In sum these final contributions [regarding the need for the protein tyrosene to which iodine becomes attached] demonstrate just how correct were those individuals who insisted on the multiple causation of goiter and cretinism, who insisted that what was lacking was not just a single and specific element [my emphasis]. All of these causes are perfectly expressed in Marañón's conception of goiter as the result of a life-way that is unhygienic and a diet that in many aspects is defective (ibid.:56).
Avoiding any semblance of a confrontational approach, Carrasco then narrows down his master's imprecise notion of goitrogenicity:
[Our] investigations demonstrate what over the years in several countries has been confirmed: that these goitrogenic factors are in practice not operative, for endemic goiter does not occur unless those goitrogenic factors are accompanied by a real lack of iodine. As is to be expected, all the other deficiencies only accentuate goitrogenic action, making it rela-
tively more intense. . . . Without "hunger for iodine" endemic goiter fails to appear. Therefore public health must first of all manage the problem of iodine deficiency (ibid.:57).
And he points out how long it may take for economic development to have the desired effect:
Because of this, we are going to refute only those opposing opinions that merit being taken into account, without wasting our time on those who systematically [read dogmatically or self-interestedly] oppose iodization. . . . No one is going to dispute the desirability and even necessity of raising cultural and educational levels, or bringing the progress of our era to the impoverished regions. . . . But if we take this approach, Public Health will have to wait years and years, entire generations, for the more serious and unfortunate cases to disappear (ibid.:58).
Carrasco introduces case material from Quirós and Teverga, two counties in central Asturias geologically and geographically similar to the county in which Escobines is located. Two indicators are used as a measure of the endemia's severity: the ratio of the most severely afflicted, defined as cretins and deaf-mutes, to the merely goitrous[33] and the age of onset, the more telling indicator. Of the 316 schoolchildren examined in this area, 295 had palpable thyroids.
The children of these counties . . . are battling even now against goitrogenic influences. Normal thyroid glands, which are not palpable, are hardly found here . . . Moreover, all the infants five months and younger coming from these two counties and examined in the Maternal Unit of the hospital in Oviedo had palpable thyroids (ibid.:63–64).[34]
And he went on to point out the high incidence, which along with high prevalence, characterized this endemia:
The goiters seen in this endemia are therefore not only residual goiters stemming from conditions that no longer prevail, for if this were the case we would not be seeing young cretins and deaf-mutes, adenomas in small children, and goiters in the newborn. However diminished in intensity than before, the endemia continues to find new victims. Public Health will be responsible for these victims for a long time to come (ibid.:65).
Carrasco gave short shrift to the hereditary hypothesis:
If we wait for the endemia in Asturias to decline spontaneously, the race there will continue to be damaged.[35] The cost of such damage will have
to be borne by government institutions, which will harbor these useless and unfortunate lives until they live themselves out. People similarly afflicted in Appenzell [Switzerland] were for a long time considered to be vestiges of an ancient, stunted race, different from other races (ibid.: 65–66).
And he dismissed the racial argument:
But the theory of a different heredity is easily refuted: one observes that the offspring of these afflicted people, growing up under the protection of iodine prophylaxis, are attaining the average height of Swiss children born to unafflicted parents (ibid.:77).
As to the problematics of appropriate dosage, he recommended that "physiological requirements should determine the level at which salt should be iodized," pointing out that "iodized salt will not court the risks undertaken when pharmacological doses of iodine were administered in earlier pilot programs" (ibid.:67). He dealt sensitively with Marañón's concern about the ingestion of iodine in dangerous amounts capable of inducing thyrotoxicosis.
The intake of iodized table salt—as opposed to iodine tablets or iodized chocolate—is self-limiting. Therefore, iodized salt cannot engender life-threatening flareups (ibid.:80).
Finally, he deals with the public's right to know.
Iodization is most immediately effective where it is introduced without the public being apprised of any change in the composition of its salt (ibid.:71).
But efficacy, he argues, should not be the only consideration in choosing a prophylactic mode, for the citizens of the Spanish Republic have a right to know.
Therefore and above everything else, the public that is to be the target of prophylaxis will have to be persuaded by well-designed propaganda of the benefits of iodized salt. Full salt, sal completa , must be presented as an essential food and not as a medication. Second, the real extent of the damage wreaked by this endemia must be appreciated by the public. It must be informed that deafness and deaf-muteness—conditions widespread in Asturias—are one manifestation of iodine deficiency, as are the mentally retarded children spoken of in Asturias as parados [those whose development has been stunted and fixed]. The public should similarly be
informed that [spontaneous] abortions and "bad births" [fetal wastage] are yet another manifestation of this plague (ibid.:86).
Carrasco addresses himself to the continuum of defects Greene (1973, 1977) was later to describe in an Andean community, a continuum of defect also reflected, as we have seen in chapter 6, in the Escobines vocabularly of affliction.
The public must sensitively be shown that this sickness against which prophylactic salt is offered is manifest not only in thick necks and goiters but in damage far more intensive and extensive. The people residing in these areas are well acquainted with this burden, even if they are unaware of its cause (ibid.:86–87).
Finally, without naming names, he warns about "the enemies of prophylaxis" (and these must include Marañón himself) who
will undoubtedly find new etiologies for all sorts of familiar diseases like arthritis and thyrotoxicosis: a fantastic and convenient cause will be found for them, namely, iodized salt.
And he closes:
We must prepare ourselves to refute the imputation that iodized salt can have such negative influences and prejudicial effects. In anticipation of the ways of our enemies, we must first (in the field) study the diseases of the region. We must, in open forums, listen seriously to any reservations people might have about iodized salt, about its suspected adverse effects. Most important, we must first measure the ordinary basal metabolic rate before prophylaxis is even initiated, and at intervals thereafter, to ascertain what changes, if any, the salt induces. This [data] will be our best armament (ibid.:90).
As coauthors, Marañón and Carrasco, a decade earlier, had published an article on the value of routinely establishing basal metabolic rates as baseline data for evaluating the subsesquent progress of patients (Marañón and Carrasco Cadenas 1923). Carrasco's final remarks on monitoring metabolic rate were surely intended to remind Marañón of that collegiality and persuade him to endorse prophylaxis.
Though the many issues of RSHP routinely printed commentary on previous published articles, subsequent issues[36] printed no commentary on Carrasco's proposal. Since no reply came from Mara-
Fig. 20.
1930s Poster for Iodized Salt
ñón, whose specialty was endocrine disease and who, like Carrasco, served on the RSHP' s editorial board, no one else ventured to do so. Doing so would have intruded on Marañón's professional territory, violated the Hippocratic oath (as in Spain it was then understood), and shown a lack of proper professional respect.
Nothing of the quality of Carrasco's lecture in an open medical forum was to appear on the subject of prophylaxis in Spain for the next half-century. The Civil War erupted two years after his lecture was published. Even before the Loyalists were defeated, RSHP resumed publication, blazing the Nationalists' political colors on the usually black-and-white cover and blaming—in an editorial—the war and its sequela of diseases on the Republic (RSHP 1938).
Carrasco Cadenas disappeared toward the end of the Civil War. Some Asturian physicians remember his despair and suspect suicide; others say he disappeared into the Caribbean (see R. L. Fernandez 1986: Interviews with Physicians). Enríque García Comas, mentioned by Carrasco (1934a :81) as a member of his field team, told me in a telephone conversation his view of the man's disappearance.
After the war, Carrasco Cadenas did not go into exile but fell, instead, into substance abuse and simply and sadly degenerated before our eyes. With the fall of the Republic, the collective action he had advocated, promoted, and practiced on behalf of the miserable and poor—possible over only a brief number of years—came to an abrupt halt. Carrasco Cadenas under the Republic forged us into a team; when the Republic fell, our team was disbanded. (Enríque García Comas, telephone interview, 1984)
The Franco Years
Here, I will take four thematic approaches to iodine deficiency, treating research and advocacy, collective and individual prevention and treatment, the flow of technology and information and disinformation, and rising demands for health and prevention. I relate these approaches to the context of Spanish medical politics and patronage.
Censorship
When the war ended in Asturias, the prophylactic team's mission also came to an end. It was suppressed by the radical ideological shift imposed by the victorious Nationalists on the vanquished Republic. Early in the Franco period, this ideology expressed itself in the rejection of most collectivist activities, tainted by their identification with the defeated enemy. For health and welfare, this meant that idealistic collectivist approaches—such as espoused by Carrasco Cadenas in his 1934 lecture and executed in a limited way in a variety of programs before the eruption of the Civil War—were, whenever possible, set aside in favor of more individual approaches to disease.[37] In medicine, this meant treatment rather than prevention. As we saw in chapter 3, this meant that niacin (the antipellagra factor) was used only therapeutically, not preventively (Peraita 1940, Grande Covián y Jiménez García 1941:49–81).
The Comisión Central de Censura Sanitaria, the Central Committee for Censorship of Public Health (RSHP 1942:87ff.), expressed this anticollectivist and medical elitist approach on a different and larger scale. The committee was located in the Consejo General de Colegios Médicos, the general council of the regional medical fraternities. Created in 1898 as professional associations, these medical fraternities and their umbrella organization, the National Association of Physicians, have never been as independent as called for in the original design (de Miguel 1977). So it should be of little surprise to find that Francoist censorship over matters of health and welfare came to be lodged in the Colegios' central office. Technical matters of health were to be supervised by Sanidad (a division under the Ministerio de Gobernación) and those of health education at a popular level by the Vicesecretaria de Educación Popular, the undersecretary in charge of the press.
Some articles of the Censorship Act are relevant to our concerns:
Article One. Censorship rules will be enforced by the Colegios Médicos. Articles and announcements authorized at the provincial level must be approved at the national level before publication in other provinces.
Article Two. Advertisements for treatments and cures, unless approved by the Royal Academy of Medicine, are prohibited.
Article Three. Treatments and cures must not be described to the general public, for these descriptions, in lay language, are almost always clumsy
and stupid, lead to . . . confusion, false hopes, and the public's loss of confidence in medicine, and the disrepute of its practitioners. Descriptions of diseases and their therapies should be reserved exclusively for professional publication.
Article Four. Professional and political advertisement requires clear, clean, and exact composition, free of offensive words. The Commission of Censorship is authorized to censor texts expressed in bad Castilian, such expression being an insult to the dignity of our language.
Article Five. Medical services, except for those rendered officially to the poor, shall be given only for compensation.
Article Six. Articles omitting the stamp "Approved by the Censor" shall not be published. Approved publications thus acquire a value not necessarily previously ascribed to them.
Article Eight. The proclamation of medical specialization acquired abroad is prohibited, for such announcements put Spanish-trained physicians at a disadvantage.
Article Nine. Dermal medications must cite the name of the laboratory in which they have been produced. Products for losing or gaining weight must also cite the name of the laboratory.
Article Twelve. Cosmetic surgery will not be approved.
Article Eighteen. Announcements advertising painless treatment are prohibited.
These articles, longer and more elaborate than excerpted here, are followed by a warning about commercial advertising:
We are fully aware that the public is damaged by multiple aspects of commercial advertising, as by . . . pernicious industries, which we will control accordingly. Madrid, October 1941. Comisión Central de Censura Sanitaria.[38]
The articles make plain the impediment put on the free flow of health and medical information. Under these circumstances, the Spanish public outside of therapeutic circumstances was unlikely to become aware of the use of dietary niacin in the prevention of pellagra (Articles One, Two, Three, and Six). Nor, discouraged as the public was from seeking cosmetic surgery (Article Twelve)—which in the form of goiterectomies had been offered in Asturias since at least the 1920s (Torres 1925)—and therefore discouraged from seeking medical attention for goiter, was the public likely to
learn about iodine prophylaxis from physicians or about iodized salt prophylaxis from advertising (Articles Four, Six, and Eighteen). Neither could foreign medical experts freely dispense such information (Articles Five and Eight); nor were salt multinationals such as Solvay, the Belgian-American salt distributor with offices in Barcelona and Torrelavega,[39] free to do so. Moreover, the flow of information was curtailed. It was not likely that country women would be at ease explaining—at best in limited Castilian, at worst in Asturiano or Bable—their diverse, mystifying symptoms to a clinician (Article Four). Censorship would of course prohibit any advertising for sal completa such as had been seen in some endemic areas during the Republic.
Individual Prophylaxis in an Anticollective Context
In this anticollective context, some prophylaxis nevertheless reached some people at an individual level. Asturian physicians most commonly prescribed Lugol's solution: the daily ingestion of one glass of water containing one or two drops of a standard iodine solution.[40] Middle-class urban women now in middle age remember being given their daily bitter dose as children. To my knowledge, only one woman in Escobines knew of this method of prophylaxis and declined to subject herself to it.[41] Country physicians in other parts of Asturias, however, remember frequently prescribing Lugol's to goiter-prone women whom "they could trust" (not to abuse it) and to members of their families (R. L. Fernandez 1986:45–457). One physician is remembered as regularly injecting iodide into goiters (ibid.: 418).[42] Pharmacists remember keeping it in stock, but they have had little demand for it in recent years (ibid.: 417). Herbalists in Madrid remember stocking a "dark-colored iodized salt," which in 1984 the authorities required them to remove from the shelves (ibid.:404).
There were risks, of course, in administering iodine in these difficult-to-control dosages. Some physicians, at least, were aware of the dangers of triggering toxic reactions by these crude self-dosage methods (ibid.:422, 428–430), and it is now clear that one drop of Lugol's solution in any ordinary glass of water amounts not to a physiological but rather a pharmacological dose, far exceeding the optimal range of dosage on the dose response curve (Aranda Regules et al. 1986).
Small-scale iodine prophylaxis such as described here did not, during the Franco era, come within the compass of official preventive medicine; nor did mass prophylaxis fall within that compass. Piedrola Gil wrote many editions of Medicina Preventive y Social, a basic text for medical students and physicians. Physicians and public health workers now approaching retirement age were introduced to its material in their student days and continue to use it as a basic reference, as do the more recently trained physicians using newer editions.[43] Six sections of the book which might plausibly discuss endemic goiter do not do so,[44] nor is the use of Lugol's solution or any other aspect of IDD discussed. These omissions are glaring in view of the fact that high-technology medicine with radiation and isotopes was rapidly becoming part of the panoply of Spanish medicine during the later Franco years. The omissions become almost incomprehensible when we hear of the alacrity with which Asturian country doctors embraced the "paper test"—the Yalow radioimmune assay (R. L. Fernandez 1986:428–430).
Ballesteros, the country doctor who worked in the 1960s and 1970s in a rustic endemic zone in Asturias not far from the area where Carrasco Cadenas had carried out his pilot study, made frequent use of the Yalow test. It was he who had to decide, when thyrotoxicosis seemed to threaten, whether or not to evacuate the patient on foot through rugged terrain by litter. It was professionally costly for him and costly to the community to decide in favor of an evacuation that might prove to have been unnecessary but would be tragic should the patient die while remaining at home. The paper test, which became available to him in 1973, relieved him of this guesswork, providing him with the necessary information for making an authoritative decision without anguish. But iodized salt, which would have made most of these tests unnecessary, remained unknown to this country physician until 1983 (ibid.).
Pilot Projects
Some progress toward mass prophylaxis was being made. A few Spanish physicians such as Ortiz de Landázuri, Morreale de Castro, Delor Castro, and Escobar del Rey carried on, in the postwar period, the research that was sooner or later to support the extension of prophylaxis in Spain.
Morreale de Castro el al. (1953) hoped to demonstrate the need for iodine supplementation. To this end, in several afflicted communities of the Sierra Nevada near Granada, she documented low levels[45] of iodine in the groundwater and correspondingly low levels of serum iodine. But she found the diet of these mountain-dwelling Granadinos so compounded by other deficiencies and the inclusion of vegetal goitrogens[46] that iodine prophylaxis alone would have been judged, as in Las Hurdes earlier, too specific a remedy for a broad spectrum of problems.
Elsewhere in Granada, such compounding variables were apparently fewer, for in some villages of the region, Ibáñez González (Ibáñez González et al. 1956) and Ortiz de Landázuri (1959) did manage to introduce dietary iodine supplements. They employed a salt iodized by Sal de las Roquetas, a subsidiary of the national saltworks, Torrevieja, on the Valencian coast.[47] Five years of supplementation produced excellent results, but soon after these were published, the endocrinologist Ortiz de Landázuri was transferred to distant Pamplona and thereby forced to drop the project. This transfer cut him and the Granadinos off from the Mediterranean source of supply, soon returning the villagers to their former state of nutritional deficiency. However, Ortiz de Landázuri resumed his labors in Pamplona, identified another iodine-deficient population (in Navarra), and prevailed on another saltworks to produce handcrafted iodized salt. Despite this handicap, Ortiz de Landázuri managed to form an escuela, a school, a tradition of investigative endocrinology that, now under Escobar's inspiration and guidance, is alive and well.[48] Both of the men who have headed this escuela have had the vision to associate investigation with prevention.
"Where Scientific Culture is Thin"
The publications cited here make bibliographic references in standard scientific form but almost exclusively to foreign work, taking no cognizance of Spanish investigations made outside the author's own department or narrow geographic zone of concern. Thus, Spanish investigators appear to discount or simply be unaware of the work of Spanish colleagues working on IDD. Such discontinuity is characteristic of
settings where scientific culture is relatively thin, where national schools are isolated from the mainsprings of Western science, . . . where scientific communication is difficult . . . [and where] barriers to scientific communication constitute the core of the structural deficiencies that have impeded the growth of science in modern Spain. (Glick 1976:287)
Escobar was, therefore, not surprised to learn that Delor Castro—an Asturian diabetologist working quite alone with only Marañón's and otherwise foreign references to guide him—had tried but failed to create an Asturian public informed about IDD. Delor Castro articulated this attempt most forcefully from the platform of the Instituto de Estudios Asturianos (IDEA) when he gave his ceremonial inaugural address—a topic of his own choosing—on being received into membership. IDEA is one of a series of prestigious and exclusive interdisciplinary scholarly fraternities created under Franco to promote regionalist studies while safely containing regionalist aspirations (Uría 1984)[49]
Delor Castro entitled his lecture "Patología Regional de Asturias," Regional Pathology of Asturias, a topic that followed up the regionalist theme developed by Casal, whose Historia Médica y Natural del Principado de Asturias was just being prepared for its bicentennial edition. After the usual opening remarks, Delor Castro (1958:5) launched into his subject.
We of this province lay claim to a special distinction for having two diseases we can claim as our own: pellagra and goiter. Both of them are grounded in this region.
He then briefly outlined the rise and decline of pellagra, "which few of the younger physicians of the province have seen, despite its historical identification with Asturias (ibid.)." Then, he turned to endemic goiter, "a disease now just as characteristically Asturian as it was in Casal's time. This, as everyone in this audience knows, is goiter (ibid.:7)." Cautiously and methodically, he made a case for iodine prophylaxis, grounding his presentation empirically on his clinical experience in Madrid and Gijón (a coastal city in Asturias), and theoretically on the literature of prophylaxis developed in Switzerland and the United States. His references stemmed mostly from the 1920s and 1930s and omitted—whether for strategic reasons or out of lack of awareness—any mention of Carrasco Cadenas.[50]
The epilogue (García Miñor 1958), composed by the evening's presiding officer and published as part of the volume, underscored the range of Delor Castro's work in the areas of diabetes and hematological investigations, areas where he had indeed made a contribution. But it made no mention of goiter, cretinism, or iodine deficiency, the only topics the evening's inaugural speaker had really addressed.
Delor Castro's name failed to be mentioned in the medical history of the province published by IDEA six years later. Indeed, its author claimed that "goiter was once widespread in the province, but like pellagra it gradually disappeared of its own accord; and the cases still to be seen are residues of an earlier era" (Fernández-Ruíz 1965:87)
The single small paragraph on Delor Castro in the Gran Encyclopedia Asturiana (GEA s.v. Delor Castro) likewise omits mention of anything pertaining to goiter and cretinism or of his membership in IDEA. His advocacy, in other words, was virtually erased from both the regional medical and public record and never came to the attention of advocates of prophylaxis in Madrid.[51]
Eleven years later, the Gran Encyclopedia Asturiana published an article on goiter. As if Delor Castro had not previously seized an Asturian forum to enlighten his colleagues about goiter and cretinism in Asturias, the article mystified its readers (GEA 1970: s.v. bocio ). It was written by Suárez-Lledó, then one of the region's few licensed practitioners of nuclear medicine, qualified to treat thyroid disease by nuclear means. He was reputed to use these means both effectively and "lucratively."[52] However, Suárez-Lledó avoided giving the encyclopedia's readership—a popular regional audience—any clear or useful information about the goiter endemia in the region. Rather, he parroted what Marañón had long ago said about goiter, added details in technical language about the physiology of iodine transport, and managed to bury mention of iodized salt in a long list of iodine-rich foods. Thereby, in one deft stroke, he avoided committing technical errors while managing to keep the public as unaware as ever about prophylaxis (ibid.).
When a nuclear physician, a goiter specialist, writes this way for a general audience, is he only misguided? Or might he be held responsible for disseminating self-serving disinformation?
Unrefuted Mischief: Greenwald
Delor Castro, it should here be noted, also purveyed some "information" of dubious value but not, as will become clear, for self-serving reasons. In his closing remarks, he cautiously revealed doubts cast on the theory of iodine deficiency, mentioning a slow-acting virus posited as active only in populations predisposed to a "mysterious factor x." Such a factor had long been entertained by Greenwald, writing frequently in the pages of Bulletin of the History of Medicine, pointing out—since populations recently contacted by Western explorers and colonists had not been reported as goitrous—the lack of historical evidence for environmental iodine deficiency. He posited, therefore, a slow-acting virus introducing itself into the postcontact situation. Delor Castro's speculation about "factor x" can undoubtedly be traced most directly to Greenwald, though Marañón had earlier expressed himself in similar terms.
Greenwald's antiprophylactic position was surprisingly well known in Spain given the paucity in the 1950s of medical publications from abroad. A list of endemic areas in Spain compiled by Greenwald (1958) has been widely cited in many Spanish publications on goiter, even again in Endocrinología (1987:14), suggesting that those opposed to prophylaxis in Spain not only provided an eager reception for his ideas but purveyed them widely. Indeed, Greenwald seems quite singlehandedly to have countered the theory of environmental iodine deficiency on a wide front (Merke 1971) and, at least in the pages of the Bulletin of the History of Medicine, has never been refuted. Moreover, Greenwald was taken seriously enough to be repeatedly cited (but not refuted) in the 1961 WHO volume in Spanish on endemic goiter (Clements et al. 1961), a collection previously available in English (Kelly and Snedden 1960). Greenwald's mischievous argument was widely diffused in Spain, while works written by people of the quality of Ortiz de Landázuri and the commitment of Delor Castro gained at best a very narrow readership.[53]
The censor in Madrid could conceivably have restrained the publication of Delor Castro's Patología Regional for violation of the Article III, for its discussion of a technical medical subject before
a lay audience. Since the booklet never came to the censor's or Escobar's attention in Madrid, however, it was probably subject only to provincial censorship. Most likely, the regional censor let the "regional pathology" slip by him, insensitive perhaps to the book's potentially inflammatory message of centralist neglect and rising sense of regional disadvantage. Although Delor Castro's book managed to slip by the censor, the mass prophylaxis envisioned in it became a reality only in 1983—after autonomía, regional autonomy, became for Asturians a political reality.
Obstacles Overcome and Obstacles Persisting
The Alarming Costs of Retardation
During the 1960s, Spanish migrant laborers by the tens of thousands were working in European industries, and by the late 1960s, Spain itself was drawing people from the countryside into its own industrial labor force. In fact, predictions were made of a possible upcoming shortage of healthy and sufficiently educated young people to staff all the positions opening up in the cities.
Del Rey Calero, a physician and medical professor in the Cádiz region, responded to this concern in the late 1960s by sending sociology and medical students into the countryside to gather data on population movements, epidemiology, and school performance. His students recorded high rural outmigration, low school performance, and endemic goiter and thyroid disease. Del Rey then argued that the Cádiz youngsters' poor school performance was related to poor health and undernutrition and predicted that these children, destined as adults for outmigration, would be unfit for the jobs beckoning them in Spain's industrial centers (Del Rey et al. 1969a, 1969b, 1970).
Soon after this series came out, the National Department of Public Health, then still controlled by the Ministerio de Gobernación, prepared a campaign for the prevention of mental retardation. Escobar, called in as consultant, tried but failed to draw attention to the role of iodine deficiency in mental retardation. This can be seen in the leftover campaign materials that make no mention of thyroid disease or iodine deficiency as contributing factors in retardation.[54] Nevertheless, they do demonstrate that the national
government was beginning to consider the industrial implications of an underdeveloped work force.
Spanish ministries and departments brought such campaign materials out in an accelerated fashion in the 1970s, for example, advising prospective parents to eat well, to get medical supervision during pregnancy, and in the event of previous fetal wastage or known familial defects, to obtain genetic counseling. As a consequence, subnormalidad, or mental retardation, became a common term even in the vocabulary of the villagers. At the same time, as people came to understand that one could actively improve the chances of bearing offspring with normal intelligence, traditional fatalism regarding the prevalence of parados receded.[55]
Developing "Political Will"
Newly developed tests screening for congenital hypothyroidism (CH), also known as sporadic cretinism (see chap. 2), in Spain brought this preventive awareness to the fore. Frontera-Izquierdo demonstrated that the incidence of CH in Madrid was the same as that found in other European capitals but was several times higher among the rural populations on the Mediterranean coast. He proposed that given his discrepancy, in the Mediterranean provinces screening should be made routine for CH and have priority over screening for other congenital conditions. While such screening might be expensive, its cost was small compared to the human, social, and economic cost of mental retardation. He submitted this argument to Anales Españoles de Pediatría (Frontera-Izquierdo 1980a ) but strategically sent it off also as a letter to the European Journal of Pediatrics (1980b :287), undoubtedly hoping to assure by this initiative a faster response than was likely to be the case were the issue confined to the national readership.
Indeed, CH screening was soon established in the Mediterranean provinces of Valencia, arousing favorable expectations in the public at large. When a several-month-old infant was discovered to be retarded and seemingly found to have passed CH screening as a false negative, the parents, a working class couple said to have been subsidized by the Socialist Party, brought suit against the allegedly negligent institution (El País 1981a, 1981b, 1981c ). In reporting this suit, the press explained congenital hypothyroidism
surprisingly well, without, however, making any mention of environmentally based hypothyroidism (congenital or otherwise). The report nevertheless increased the public's awareness of the preventability of much mental retardation. Journalistic reports of this lawsuit, in combination with other events and publications, seem to have contributed to the "political will" seen only recently as necessary for mass prophylaxis to get off the ground (DeMaeyer, Lowenstein, and Thilly 1979:3).
Simple and Accessible Information
In this regard, the publication of Control of Endemic Goiter by WHO (ibid.), published also in Spanish, played a signal role in Spain. In contrast to the volumes previously published on goiter by the World Health Organization and its regional sections (Kelly and Snedden 1960; Clements et al. 1961; Stanbury 1969; Dunn and Medeiros-Neto 1974; all published in Spanish), this volume avoided investigative reports but simply presented the most essential information about IDD and iodine prophylaxis—technical aspects of salt iodination, prevention of severe endemic goiter with iodinated oil, administrative and legal aspects of goiter control, and an overview of IDD and supplementation in the world. Most important, it stated quite simply that "the most important single causal factor is an inadequate content of iodine in food and consequently an insufficient dietary intake of iodine" (DeMaeyer, Lowenstein, and Thilly 1979:9). In just as simple a fashion, it described ways in which salt could be iodized without great capital outlays or very specialized technical knowledge.
What made the volume significantly different from its predecessors is that the simplicity of its basic information was not cast in doubt by a thick core of densely technical reports on recent research. The DeMaeyer, Lowenstein, and Thilly volume was so readily understandable, so attractive and small, that no country physician or health officer could casually exempt himself from participating in the action it proposed. However, one problem that characterized its predecessors persisted: any prophylactic action had by medical convention to rest on "good indicators of the severity of the endemia" (DeMaeyer, Lowenstein, and Thilly 1979:10).
"The Watchdog in the Cabbage Patch"
As to statistics—it's the old story of the perro hortalero, the watchdog over the vegetable garden. The watchdog, in this case the man in charge of clinical and epidemiological statistics, won't let anyone harvest the cabbages which he himself won't eat. Satiated and having no desire to eat them himself, he prevents anyone else from ever getting at them.
—Dr. F. J. Díaz Cadórniga
Dr. Cadórniga, the chairman of endocrinology at the Hospital of Our Lady of Covadonga in Oviedo and animator of the campaign to eradicate endemic goiter and cretinism in Asturias, explained to me by way of this story—often told about bureaucrats in Spain—why for a long time he could not get the necessary data on which to mount a campaign. Having received his medical training elsewhere in Spain he noticed that "an unusually high proportion of thyroid cases make up the case load on the endocrinology service here in Asturias." He therefore sought verification of his impression in epidemiological or hospital statistics. The statistician refused to work up the data, and the archivist refused, also, to allow Cadórniga to work it up himself. He proposed, then, to get the statistics himself in the mountainous zones where the thyroid cases seemed to originate, but his proposal was turned down. Eventually he persuaded colleagues to voluntarily join him in gathering the necessary data during vacation periods (R. L. Fernandez 1986: 440–445).
This extraordinary private initiative, taken early in the 1980s before the Socialists were voted into office, yielded the alarming data that, during the transition to autonomía, prompted the release of funding for an official regionwide survey. These results, in turn, demonstrated in conventional medical terms the need for mass prophylaxis (Aranda and Díaz Cadórniga 1985; Aranda Regules et al. 1986:9–16; Menéndez Torre et al. 1986).
The difficulty of crossing this data threshold had earlier, in the 1970s, also impressed an Asturian médico titular, an officially appointed country physician. Concerned about the endemic goiter he had found in his school-age patients, and having visited briefly in the United States and having learned about the existence there of iodized salt, he had written up the results of his own clinical survey[56] on the basis of which he solicited authorization to run a pilot
iodization program and materials for the proposed feeding program at the school. His proposal was flatly turned down by health officials and ignored by the regional press.
I had written on his behalf to Solvay, the salt company, to Dr. Severo Ochoa the Nobel Prize-winning physiologist from Asturias, and eventually (on Ochoa's recommendation) to Dr. Francisco Grande Covián (previously mentioned as the eminent nutritional physiologist working since the 1950s at the University of Minnesota).[57] Grande Covián, long an expatriate like Ochoa but recently repatriated, expressed interest in the doctor's problem but needed demonstration, by UIE and T4 levels, of the existence of the suspected endemia. Until he received such biochemical data, he could not refer the matter to the proper authorities.[58]
The sympathetic interest from so eminent a physician was gratifying to the country doctor, who could not, however, accommodate Grande Covián's request for the biochemical data, which was beyond his means. García Pérez saw himself defeated and let the matter rest. Cadórniga's volunteers eventually did obtain exceedingly low readings from his schoolchildren. These proved to be key in prompting the official follow-up. Meanwhile, however, the country doctor, who knew exactly what essential element the children were lacking, had to watch them languish in the schoolroom, stunted and inattentive.
Regional Campaigns
Elsewhere in Spain, there must have been other private initiatives like these, emerging out of a combination of factors, prominent among them the growing awareness of the preventability of some kinds of mental retardation and the forthright approach taken toward prophylaxis in the DeMaeyer volume. Tribuna Médica, the organ of the Colegio Oficial de Medicos, received by every accredited physician in Spain, announced in January 1983 the opening of a campaign to eradicate both endemic goiter and cretinism and congenital hypothyroidism in Galicia.[59] The campaign, designed by Galician pediatricians and WHO consultants from abroad, required careful preparation so as not to offend the public whose cooperation was essential. Only broad public compliance would reduce the
very high rates of mental retardation and physical stunting said to have been found among the rural children of Galicia's interior.[60]
Cadórniga and his team in Asturias, meanwhile, during the months preceding the national election of 1982, quietly ran a pilot survey to determine the level of IDD in samples of schoolchildren. Soon after the Socialists won the elections, both in Asturias and the majority of Spanish provinces, Sanidad in Madrid relinquished responsibility for public health in Asturias, transferring that responsibility to the Consejería de Sanidad, now the autonomous public health service of Asturias. On the basis of the alarming results (Aranda and Díaz Cadórniga 1985) the newly created Consejería ran an open regional survey to identify the areas in which schoolchildren were goitrous or subclinically hypothyroid. As expected, extensive iodine deficiency was found in three of the six areas into which the region was divided (Menéndez Torre et al. 1986, Aranda Regules et al. 1986).
Fifty-three percent of the schoolchildren in the eastern interior zone, where Escobines is situated, were found goitrous (WHO's classifications of OB, I, II), as were 21 percent in Asturias generally. Counting as goitrous only those classified as I and II, 29 percent were found goitrous in the eastern interior zone, and 8 percent in Asturias generally (Aranda Regules et al. 1986:36). Urinary iodine excretion in all zones fell below 63 mcg/dl (micrograms per deciliter), and in the zone where Escobines is situated, below 50 mcg/dl; desirable levels are between 100–200 mcg per day (ibid.:39). These findings served as the warrant for launching the campaign to eradicate goiter and cretinism in Asturias.
Old Industries, New Structures, and Resentful Bureaucracies
The widely diffused Asturian campaign materials created a demand for iodized salt, which, paradoxically, did not become available until late spring and summer 1984, when demand had slowed down. The Asturian authorities had anticipated that the arrival of iodized salt might long be delayed and thus prepared themselves to give, if necessary, preventive injections of Lipiodol. This they did in spring 1984.
Asturias was not alone in having to confront this supply problem. Sanidad (Public Health) in Madrid, still in charge of public health for the nonautonomous provinces, seemed unable to get iodized salt onto the market. This is almost inexplicable. Neither raw material nor technical expertise could have been serious impediments: Spain was Europe's largest salt producer, and free-flowing salt had long been available on the Spanish market. This demonstrated that Spain had the technical expertise to keep salt moisture-free at standardized levels—a requirement for the production of large volumes of high-quality iodized salt.
Legal and bureaucratic requirements had to be met, but they posed no formidable hurdles. The Food Code of 1976 defined iodized salt as "salt containing 10–15 milligrams of sodium iodide or potassium iodate per kilo" (BOE 12.2.1976) and in 1983 (BOE 6.1.1983), raised the required level to 60 milligrams per kilo.[61] Any Spanish salt manufacturer could produce iodized salt, provided he first obtained the necessary authorization from the health department.[62]
Markets may have posed a problem at one time, as is suggested in this excerpt from a letter written by Francisco A. Orovio, Division Chief, Derivatives and Petrochemicals, Solvay, on January 13, 1982.
. . . in answer to your inquiry regarding iodized salt. We were sufficiently aware of the problem[63] to take the trouble to obtain authorization to produce and sell iodized salt. Moreover, we have manufactured some quantities of such salt on a small scale, and distributed them at no cost in the provinces of Granada and Zamora, and found that despite our efforts there really was no market potential to justify production of iodized salt at an industrial scale [emphasis added].
In 1984, when the market had at last been created, the demand for iodized salt could not be met. There were antecedents: the newly created Ministry of Health and Consumer Affairs had convened the salt manufacturers in autumn 1983, apprising them of the new standard of iodization and of its plan—over winter 1983–84—to stimulate demand for iodized salt, this stimulation being an important part of its Campaign to Prevent Goiter and Cretinism. Indeed, television programs as popular as Sanchéz Ocaña's Mas vale prevenir, A Stitch in Time, had produced the desired demand.
As can be seen in the excerpt below from the interview with Dr. Nájera, head of the Ministry's Department of Education and Preventive Health, a certain peevishness seemed to characterize the relations among the ministry, the new autonomies, and the salt manufacturers.
People responded to our television campaign demanding the salt. But the salt industries let down our Ministry, failing to get it to the market on time, not until spring, when people had already forgotten about the winter's campaign. When finally it did appear, it was in Galerias Preciadas [an expensive department store], getting first to the people who least need it.
Under this present political system, what can a ministry do to obtain compliance? Nothing. Now it's up to the autonomous regions. We prepared plenty of materials for them. We sent out 20,000 copies of the new WHO book [DeMaeyer, Lowenstein and Thilly, 1979] to all the physicians in the country. And we prepared posters, slides, and teaching materials for them, too.
But it's not our business to poke into how the autonomous regions are doing with what they've opted to take on. For all I know, the officials in those autonomous regions may have discarded the materials prepared by my department.
Regional health officers in the newly autonomous regions were aware of these attitudes and of the historical lack of cooperation among departments and ministries—the encumbering verticality of structures. Thus, when regional health personnel, such as those in the Asturian Consejería, were at last legally capacitated to take charge of their own affairs, in this case to take action on behalf of subclinically hypothyroid children (Aranda Regules et al. 1986:38), they counted on Lipiodol to safely surmount the shortcomings of the ministry (ibid.:10).[64]
Lipiodol was an ambiguous triumph for the advocates of prophylaxis, however. Traditional opponents of prophylaxis still occupied important desks, even in regional bureaucracies. Dr. F. Nuño, for instance, in 1984 the technical director of the Asturian Consejería and in that capacity the administrative head of the campaign to eradicate goiter and cretinism, had years earlier, as head of the Delegación de Sanidad in Asturias in 1972, assured me that
the former endemia is declining of its own accord. The incidence of goiter is negligible. Therefore we have no need for statistics on goiter and cre-
tinism. To introduce iodine prophylaxis into Asturias would not only be superfluous but expensive. (Dr. F. Nuño, Aug. 1972)
Yet Nuño was still in 1984 blocking prophylaxis wherever he could, refusing, for example, to obtain the authorization that would allow iodized salt to be marketed in the economical units of fifty or a hundred kilos preferred by Asturian country women.[65] His attitude put him at odds with Dr. Cadórniga, who had been appointed medical head of the campaign. When circumstances—which he had helped to create—required the use of Lipiodol injections, then Dr. Nuño may have felt himself vindicated, for, indeed, prophylaxis in this form proved to be expensive.
The View from the Bottom Line
Financial, specifically pharmaceutical, interests may have posed more of an obstacle to prophylaxis over the years than has so far been suggested. Several propositions can be explored by making some simple calculations. These calculations are based on advertisements in one issue of Endocrinología (July 1984). The analysis, only suggestive, looks at the proportion of full-page advertisements for thyroid medications in relation to all full-page advertisements. Those for thyroid medications represented a third of all the full-page ads.
Proposition 1: If the cost of advertising is proportional to incidence, 35 percent of the patients on an endocrinology service will be treated for thyroid conditions. It turns out that this proposition is not supported, for in Madrid, the only clinical service in Spain for which statistics were available (Laher Montoya n.d.), 17 percent of the patients were diagnosed with thyroid disorder, a figure the author considered alarmingly high and indicative of possibly underlying iodine deficiency.[66] Consequently, the proportion of monies spent advertising thyroid medication in a journal of endocrinology appears to be twice as large as the proportion of thyroid patients admitted into a Madrid endocrine unit.
Proposition 2: If an endocrinologist's income—legitimate and through kickbacks (de Miguel 1977)—is a reflection of the medications he prescribes, then a third of the prescriptions written by endocrinologists will be written for thyroid medication. If this
proposition does not hold up under scrutiny, then it must be supposed that a diagnosis of thyroid disorder is worth twice as much as other diagnoses to the prescriber. Statistics are unfortunately unavailable for demonstrating the proposition in either of its forms.
Proposition 3: Pharmaceutical advertisements are a kind of gamble reflecting hoped-for profits. The ENDOFREN ad (see fig. 21) and the following story would seem, at least under this initial, albeit very informal, scrutiny, to bear out this proposition.
Diiodotyrosene and reserpine are ENDOFREN's principal components, as the fine print makes clear. These compounds, according to my understanding of iodine physiology, seemed of dubious value in treating hyperthyroidism. Puzzled, I telephoned Dr. Escobar, then serving on the editorial board of Endocrinología, who commented on ENDOFREN as follows:
ENDOFREN is a compound useless for treating the disorders it purports to treat. Indeed, it has no specific action at all. Diiodotyrosene seemed, twenty years ago, a promising medication. One of the pharmaceutical houses in the United States gambled a lot on producing a batch before checking it through the FDA, which didn't let it pass. The manufacturer held on to it in the event it could be loaded off on someone overseas, which proved to be someone in Spain.
When I saw the ad in the journal I telephoned the editorial board of Endocrinología to let them know my outrage. It will not be run again. (Sept. 12, 1984)
Later, I could trace ENDOFREN only to BAMA, a tiny pharmaceutical house in Barcelona, now apparently out of business. Even its principal ingredient, diiodotyrosene, was untraceable in the International Guide to Pharmaceutical Products. The reserpine figuring in its description is a vasodilator. It might, for a short while, actually calm down the woman so artfully depicted on the verge of thyrotoxicosis.
Conclusion
We end on a tantalizing note of possible international, probably American, involvement in the production and promotion of a dubious drug to be used in treating thyroid pathology. No doubt there has been American involvement. The economic power and the inventive and productive potential, of the American pharmaceutical
Fig. 21
Advertisement for ENDOFREN
industry has made it a major actor in the therapeutics of most countries. These have benefited from its discoveries and sometimes have been mortgaged to its mistakes.
But the emphasis here has been on the regional and national contexts in Spain itself. Only to a limited extent has it been on the international factors that account for a sixty-year delay in implementing simple but cost-effective dietary supplements that prevent IDD. One draws back from calculating how many human lives have been tormented, stunted, or wasted by this delay. This chapter has looked primarily at the actors involved, at the men whose favorite theory or excessive loyalty—whether personal, bureaucratic, or political—prevented them from vigorously promoting the simplest of remedies. And it has looked at men who struggled early on and under discouraging circumstances to bring prophylaxis to those in need of it. Even here, to focus on personality alone—and it is not easy in these circumstances to avoid the fugitive satisfaction of blaming or praising—is to hang too much on ad hominem argument.
It is to miss the institutional frameworks within which persons act. These, in the end, are the enduring configurations that deserve our attention. Persons and personalities come and go, and some can have the greatest influence in their circumstance, men like Franco, of course, and physician-statesmen like Marañón. Institutions, however, not personalities, form the persisting framework within which people act. Institutions facilitate or block the flow of images and information. They, too, put the stamp of approval on attitudes and reward those individuals or classes holding the "correct" ones. Institutions promote or hinder the formation of a "political will." As admonitory as one may be tempted to be, to a Marañón or a mischievous Greenwald, it is nevertheless on institutions that accounts such as this must seek to have their influence.
Chapter Eight
Closing the Gap between Therapy and Prevention
What has been learned in this study? This investigation has revealed institutional inertia in one country tantamount to a conspiracy of silence.[1] This inertia has acted to maintain pervasive ignorance about the cause and preventability of endemic goiter and cretinism—an affliction that, since the 1920s, has been easily prevented through a simple additive to salt. This silence and the concomitant apathy and inaction have produced human wastage that can hardly be measured on a world scale. For though Spain is the case in focus, such inertia has a much wider presence in world health. The sheer numbers affected on this scale by iodine deficiency may perhaps be estimated, but the loss of human vitality, economic viability, and sense of well-being cannot be measured.
Even in the small mountain village studied in this work, the human wastage of IDD is difficult to measure, for how can one assess the stigma of dwarfism and deformity, the pervasive sense of inferiority, also often of lethargy, or the burden of a community's disrepute? Without attempting to assess this diffuse wastage of the last sixty years in any more precise terms than the preceding chapters have already shown, some reasonable estimates of clinical pathology can, however, be made: the number of goiters needlessly experienced, the number of goiterectomies that could have been prevented, and their cost.
Since mass iodization became feasible in the 1920s, three generations of women have grown up in Escobines, a village of some
800. These, it can be retrospectively estimated from the prevalence of goiter in 1972,[2] developed a total of at least 258 goiters of grade II or higher. Fifteen of these have been excised, and before the end of the century, a total of at least thirty will have been excised.[3] The surgical/hospital cost of the present number of goiterectomies alone has cost the state $30,000 (assuming a very low cost of $2,000 per goiterectomy) and will, at today's prices, cost at least another $30,000. In a regional population of one million in which the prevalence of goiter and goiterectomization may be substantially lower—at a rate conservatively estimated at one-fourth that of Escobines—we calculate 1,470 goiters of grade II or higher (having subtracted goiters attributable to causes other than iodine deficiency). At a rate of one goiterectomy for every two hundred Asturians, the state has already spent an estimated $4,540,000. As Carrasco Cadenas once predicted, the state's outlay has come to be vastly greater than anything that might have been spent for prevention, even had it totally subsidized iodization from the moment mass supplementation became both technologically feasible and safe.
What has been calculated here is only, of course, a small part of the state's total outlay on IDD in Asturias. Other costs associated with IDD are, for example, subsidies to the families of retardates kept at home, remedial education, Spain's first boarding school for the deaf, a wealth of medications, clinical visits, scanners, and, undoubtedly, extensive medical treatments for thyroid cancer.[4] When the specific surgical costs for goiterectomies, as calculated above, are added to these diffuse clinical, educational, and social costs (also now borne by the state), the cost of inaction multiplies.
This investigation has shown the forces sustaining ignorance and silence. It has also shown how, in the case of Asturias and Spain, that silence of sixty years was at last broken. So this study is another contribution to our knowledge of how basic information and basic techniques—not only for the prevention of IDD but for other preventive measures such as the reduction of smoking and lung cancer, the avoidance of bottle baby syndrome, the promotion of immunization, the propagation of rehydration techniques and safer sex practices—might be deployed to break through ignorance and silence elsewhere. For while we have examined here the deinstitutionalization of a specific ignorance in Asturias and Spain,
the problems of persistent ignorance in respect to health practices are found worldwide.
The institutionalization of ignorance concerning a product as homely as iodized salt is difficult for many of us to imagine. Having grown up under the protective commercial umbrella of iodized salt ("when it rains, it pours"), we do not think of prevention of iodine deficiency as a medical issue. But where salt manufacturers, for whatever reason, have failed to seize a market advantage over their competitors by promoting along with their product an ounce of prevention, then prevention remains by default within the domain of public health and medicine. And if the representatives of public health fail to see an urgent need to promote iodine supplementation, or physicians treat disease without at the same time teaching prevention, then inertia is pervasive, and ignorance persists.
It seems appropriate to recall here just how pervasive was the institutionalization of this specific ignorance, for it extended even into the ranks of the practitioners of modern medicine: ordinary Spanish physicians in the 1970s were aware neither of collective iodine prophylaxis nor of the existence of iodized salt. It must be pointed out that their lack of awareness of mass prophylaxis did not stem from indifference, for, whatever their trepidation, at the individual level, many physicians did prescribe iodine prophylaxis for both urban and rural Spanish women, advising them to routinely take drops of iodine in a daily glass of water.[5] Physicians, aware of the potential for abuse in this practice, prescribed iodine drops only guardedly. Thus, the demand for individual prophylaxis remained very limited and any overt demand for mass prophylaxis—of which the public and the majority of physicians remained unaware—failed to arise.
The WHO goiter eradication team expresses that demand as "political will" (DeMaeyer, Lowenstein, and Thilly 1979) and sees it as necessary for getting prophylaxis under way. What the eradication team fails to recognize is that ignorance of the existence of mass prophylaxis can prevent the political will from arising.
The concurring forces that sustained this specific ignorance within the nation for so long have here come to light—a distinguished physician-statemen's benign but neglectful silence, the thinness of scientific discourse, the medical convention requiring uncritical deference toward former teachers, the state's censorship
over matters of health, and last, but surely not least, class interests. War and its aftermath contributed as well.
Forces outside the nation also helped to institutionalize ignorance. Paradoxically, the primary force here has been the development of high-technology medicine and a highly specialized thyroidology. After midcentury, when Spain was recovering from war and isolation, the blandishments of advanced medicine became seductive. Spanish medicine embraced these approaches to therapy partly because it had long been isolated and wished, without delay, to integrate itself into international biomedicine. The Spanish public, in its stead, embraced advanced medicine for its promise of relief. Outside the embrace stood iodine prophylaxis (and presumably other preventive techniques), at that time hardly a part of general medicine in the United States and certainly not a part of high-technology medicine.
An anachronism was created: while the goiters of Spanish villagers were subjected to scanners and radiation treatment by iodine isotopes, the villagers' underlying iodine deficiency failed to be addressed or even revealed. In Spain, this disparity between the technologies of prevention and cure persisted for three decades. Over an even longer period, many Spanish physicians either remained unaware of mass prophylaxis or—comfortably situated within a strictly compartmentalized curative medicine—did little to extend their patients' or the public's understanding of how deficiency could be prevented. To be sure, we know of only a few physicians who actually withheld knowledge of mass prophylaxis from the public. But though such apparent intentionality was the exception, where there is institutionalized ignorance, the effect on a local populace is the same as if physicians, in particular, and medicine, in general, were conspiratorially blocking the flow of critical information.
Meanwhile, no cautionary statements in textbooks or in the documentation accompanying scanners or other advanced medical apparatus generated in the United States or in other centers of biomedicine pointed out the impropriety of applying high-technology solutions at an individual level while ignoring low-technology solutions at a population level. However understandable, since the mission of advanced medicine was therapy and not prevention, this omission was short-sighted, born of compartmentalized approaches
to health. It was born, also, of indifference to or unawareness of the social, political, and cultural contexts of those receiving the new medical technology.
I hope that this ethnography of affliction has made vivid one context where the cart of high-technology medicine was put before the horse of prevention. There are similar contexts around the world, for the appeal of high-technology medicine is everywhere seductive, attractive to physicians and the public alike.
Action in the Spanish context was delayed for many reasons, and the overcompartmentalization of therapeutics, keeping it separate from prevention, has been only one support of inaction. But if we remember how pervasive was the institutionalization of ignorance about prophylaxis in Spain, then we, looking out on the many contexts abroad where people are needful of relief, can, at the least, insist on the broadest awareness of these contexts. We can insist that simple preventive knowledge be diffused along with high technology.
We can encourage that textbooks, diagnostic manuals, physicians' desk references, and the literature accompanying the high-technology medical apparatus exported to other countries explicitly state the assumptions—that is, the social and cultural contexts, the infrastructures and superstructures—on which their use is based. A statement of such assumptions in the case of iodine prophylaxis might read something like this:
Optimal dietary iodine (where this book, manual, brochure, piece of apparatus was produced) is assured by a diversified diet including the use of iodized salt. Where dietary supplements are not routinely available, the physician must not assume that symptoms bringing the patient into the clinic stem from other than dietary causes. Therefore, iodine status must be checked, and if found inadequate, it must be corrected. No iodine-deficient patient should be assumed to be an isolated case of malnutrition. Rather, a single case of iodine deficiency should make the clinician suspect possible dietary deficiency in the population, which should be checked and if found deficient, corrected. High-technology medicine is too hastily or inappropriately used if low-technology measures preventing the appearance of the world's most common thyroid disorders are not at the same time implemented .
Had such a statement been standard in any text of internal medicine, any desk reference or diagnostic manual, and any piece
of apparatus used in the diagnosis or treatment of thyroid disease, the ignorance of prophylaxis could hardly have persisted in Spain for so long. Had our implicit assumptions been clearly stated, it would have been difficult for Spanish medicine to adopt scanners, advanced surgical techniques, or the Yalow test without at the same time adopting the preventive measures shown in this ethnography to have been so grievously lacking.
Two further issues concerning hereditarian thinking and closed and open political structures deserve final comment here. This investigation has elucidated the obstacles to iodine prophylaxis in a specific case. But the ethnographic approach to elucidating these obstacles can be applied to any adversity or to any hazardous condition seeming to escape general notice, especially the notice of those physicians and health authorities who take a narrow view of their mission.
The genealogical method that is part of this ethnographic approach is especially applicable, I believe, to subpopulations whose habitual exposure to unknown hazardous substances or mysterious deficiencies wrongly make them candidates for an unwanted and prejudicial "ethnicity" that, once the hazard is eliminated, proves to be spurious. Without dismissing inherited metabolic error as irrelevant, we have elucidated how an endemia has been misrepresented as resulting from inbreeding and the proliferation of inherited defects. We have also elucidated the props of such hereditarian thinking.
This investigation has focused less on the larger political-economic issues concerning the kind of society in which knowledge of endemic disease is likely to be suppressed. While this study clearly recommends the need for knowledge of the social and cultural context in which new medical technologies are implemented (or not implemented), it has had less to say about these matters of political economy. It is clear, on the one hand, that authoritarian regimes, such as found in Spain under the Franco dictatorship, provide propitious climates for the perpetuation of institutionalized ignorance. The third estate, in its various forms, including the academic milieu out of which a study such as this derives, are, in such regimes, kept under tight control in their critique and in their offering of alternate views of national policies.
On the other hand, it must be acknowledged—as did Carrasco
Cadenas in his own time—that dictatorships and other coercive systems have been quite effective at promoting some broadly preventive health measures.[6] The introduction of mass-scale prophylaxis into democracies may be, indeed, more difficult than into other kinds of political systems. At an official level, the Soviet Union and its former satellites, for example, have addressed the problem of iodine deficiency far more broadly than has the West.[7] Needless to say, there is a very high price to be paid for the efficiency such authoritarian regimes may have—when moved by self-interest—in making the trains run on time or in implementing iodine prophylaxis efficiently.
In open societies such as ours in which studies such as this are more readily generated, we are bound to recognize the way that increasing specialization coupled with overemphasis on profitability in the drug and medical industry can act as a kind of authoritarianism, preventing the right hand from knowing what the left hand is doing. All the more reason, therefore, to insist on the ethnography of affliction, that is, the study of disease and suffering in its widest possible social and cultural context.
Appendix
Quantification
At the local level, we can make a reasonable estimate of the human and financial cost of the most quantifiable aspect of IDD, goiter, extrapolating it from the goiter seen in Escobines. The reader is reminded that the estimate will be on the low side because the affliction was then in decline.
Since the burden of goiter in Asturias weighs chiefly on women, the count begins with females born in Escobines since 1904. Those born before this year would not have profited as dramatically as the younger women just entering their reproductive years when mass iodine prophylaxis became technically feasible and safe. While any year near the turn of the century could serve as an appropriate divider, 1904 is chosen because the census of 1934 happens to be available, allowing us to deal with ten-year cohorts.[1]
Against this background, the cost of needless affliction in Escobines can now be quantified. The census of 1934 counted eighty women age 20 to 29 born between 1905 and 1914. These, combined with the 178 girls in the same census born between 1915 and 1934, plus the 203 women and girls, according to the 1972 census, born since 1934, a total of 461 females, were needlessly exposed to iodine deficiency.[2] Extrapolating from the 56 percent of the older women in the survey of 1972 who were goitrous or had conspicuous symptoms compatible with a diagnosis of IDD in this century,[3] we calculate that at least 258 Escobinas must have been needlessly afflicted.
An unknown number of the older women figuring in the census of 1972 have been treated for dermal and endocrine conditions, and six (at least) of the older women have had goiterectomies at state expense. Younger Escobinas, born since 1934, are less visibly goitrous but have sought treatment to a much greater extent; they have been exposed to diagnostic and therapeutic radiation, and nine, probably an undercount, have been goiterectomized.[4]
These fifteen known goiterectomies averaged a week's stay in the hospital at state expense, adding up (at an estimated $2,000 per stay) to a minimum cost of $30,000—a sum far larger than the cost to the state of the iodized salt required by 750 people over fifty years, even if the consumer were to bear no portion of that cost. The cost of goiter in Asturias—as borne alone by the state—can be extrapolated from these village calculations. Fifteen goiterectomies in a notably endemic village of 750 means that about one villager in fifty has already been goiterectomized.[5]
Concerned only with rural goiter, and knowing that 30 percent of the Asturian population is still rural, we can extrapolate from this one-fiftieth,[6] yielding 1,500 goiterectomies. Because we know that goiters also appear sporadically in populations not iodine deficient, we must subtract 2 percent of these from the total. This yields 1,470 Asturian goiterectomies that, without a doubt, could have been prevented by iodized salt.[7]
Over the approximately thirty years in which poor rural women have been getting goiterectomized, these 1,470 average to about 40 goiterectomies per year. They will continue to be performed at this rate or higher—because of rising sensitivity and increasing medicalization of services—as the established goiters of the 1980s come to the attention of physicians. Only when the schoolchildren who are now receiving prophylaxis come to maturity will this rate decline. Thus, another 800[8] must be added to the 1,470, yielding 2,270 goiterectomies that could have been prevented—at an estimated cost to the state of $4,540,000. Whatever the magnitude of the underestimate of goiterectomies per year, and it may be great,[9] the vast majority of these excised thyroids would never have become goitrous had iodine supplements become available in a timely way.
Recommendations
I. On the managing of information:
A. The names of chronic and nutritional diseases should, whenever possible, relate to prevention.
The International Classification of Diseases (ICD) should, for example, cross-index goiter, cretinism, and hypothyroidism, referring the reader to iodine deficiency disorders, IDD, thereby alerting him to the possibility of prevention.
B. General literature of IDD control should avoid mystification, for the readership may include congressmen or intelligent members of the lay public, as well as country physicians and public health officers.
Specialized symbols such as "µ" should be used, if at all, only in conjunction with the spelling out of the word (microgram) so as to uphold crucial distinctions between "µ" and "mg" (milligram). Rates of iodine intake or excretion and levels of iodization can then be discussed with utmost clarity.
Glossaries can also reduce mystification.
Care should be taken that definitions for terms central to discussion of assessment and control of IDD—such as UIE (urinary iodine excretion)—are included in standard medical dictionaries.
Acronyms should be chosen only after carefully checking the literature: one medical dictionary defines IDD as "insulin dependent diabetes."
II. On fostering the theme of prevention in standard medical textbooks:
A. Prevention should precede any discussion of pathology.
B. Texts such as Harrison's should be adapted to conform to the needs of the less affluent contexts into which they are disseminated.[10]
Incentives should be developed to require authors to take those contexts into account.
Any medical work intended for translation or export should state its assumptions about nutritional status.
A thyroidology text, for example, should state forthrightly that "it must not be assumed that the population is iodine replete."
III. Agencies and International Organizations:
A. Where biochemical or clinical measures of endemicity cannot readily be obtained, institutions such as WHO or ACC/SCN should promote the early recognition of chronic and nutritional endemias by according recognition to alternative—social or visual (or other)—indicators.
B. Whistle-blowers should be encouraged.
From within the medical establishment (such as Dr. Cadorniga in Asturias) or outside it (such as social scientists doing fieldwork among marginated peoples).
C. WHO eradication teams should include nonmedical personnel, for obstacles within medicine and difficult for physicians to discern.
D. IDD control teams should distribute information widely in order to bypass professional opposition concentrated in the upper echelons of a national medical hierarchy.
WHO should not assume that knowledge about prophylaxis will trickle down.
WHO should consistently diffuse works aimed as clearly at the country practitioner as at upper levels of public health and medicine.
E. It is wrong to assume that health matters must be addressed exclusively from inside medicine or public health.
Commercial rather than governmental distribution of iodizated salt is likely, at least in some countries, to be more successful.
IV. On obstacles in industry:
A. Stocks of ordinary salt may have to be bought up, and plant conversions subsidized, before salt manufacturers will produce iodized salt.
B. Covert opposition within the pharmaceutical industry may have to be addressed.
Disappearance of a pool of (thyroid) patients may threaten industry with loss of income.
C. Appropriate information on low-technology prevention should accompany the export of high-technology medical equipment.
V. On medical opposition:
A. Dialogue should be encouraged between the medical opponents and proponents of prophylaxis,
Because covert opposition can defeat a campaign even after launching.
B. An eradication team handicaps itself by assuming that opposition to prophylaxis is based on a fixed and unchangeable "cultural mentality."
Medical opposition is more likely to be based on inertia, class interest, or a resolvable misunderstanding.
If a prominent opponent of prophylaxis fails to be persuaded by his own national colleagues, esteemed foreign colleagues should try to persuade him.
Notes
Chapter 1 Introduction
1. In researching Spain's medical literature, I have found references to endemic goiter and cretinism, or IDD, in twenty-two out of Spain's fifty provinces (the publications are treated in detail in chap. 7). The reports suggest that focal areas of affliction in nine provinces (Almería, Badajoz, Cáceres, La Coruña, Lugo, Navarra, Orense, Pontevedra, and Santander) have an incidence and prevalence of IDD as severe as that reported for Oviedo (Asturias); five provinces have areas judged half as severe as Oviedo's (Cádiz, Granada, Málaga, Salamanca, and Alava); and four provinces have areas judged one-fourth as severe (Valencia, Vizcaya, Zaragoza, and Guipuzcoa). The populations of each of these provinces (taken from España, Anuario Estadístico 1975 ) were weighted according to these estimates, the estimate of affliction being derived from that number by the same means as originally calculated for Asturias (see chap. 8). One should be able to derive a much better estimate of the degree of IDD in Spain from clinical and surgical data. This, however, has not yet been compiled, and the raw data on which such compilations could be based is unavailable to those who would compile it (see chap. 7).
2. NYT, Dec. 4, 1988, p. 1.
3. Mead expressed this opinion on the platform of an invited symposium at the 1976 annual meetings of the American Anthropological Association.
4. The quoted phrase is examined at length in chap. 7.
5. ''A child's encounter in the field, witnessed by the parent, may create an emotional charge powerful enough to redirect the investigation" (R. L. Fernandez 1987 b :187).
6. Some of the grade 2 goiters, buried in fat or strategically concealed under garments, were also difficult to ascertain by vision alone.
Chapter Two Iodine: An Essential Dietary Element
1. The element iodine is found in nature only in combination with other elements, such as NaI, sodium iodide, or NaIO, sodium iodate. It occurs as a free element only transiently in chemical or biochemical reactions. The reader is asked to bear in mind that iodine may refer to any of these forms.
2. I have synthetized my presentation for this section and for the remainder of this chapter from the following sources. The WHO works by Clements (1961) and Dunn and Medeiros-Neto (1974) gave me my original understanding, which was complemented by further reading in Pitt-Rivers (1961), Netter (1965), Acta Endocrinológica (1973), Stanbury (1969, 1978), Utiger (1979), Tepperman (1980), Thompson and Thompson (1980), Medvei (1982), Matovinovic (1983), Krenning and Hennemann (1983), Fisher (1983), and Harrison's . My understanding of what was known in the early days of prophylaxis comes from the Schweizer Kropfkommission (1928), Carrasco Cadenas (1934 a ), Plummer (1936), and Salter (1940).
3. The seaweed believed to have such a virtue was known in Asturian as ocle, in Castilian as ocla or sargazo .
4. La Canilona is a cleft in the Asturian coastal cliffs where seaweed, because of heavy currents, tends in stormy water to accumulate. Asturians have long harvested seaweed as a cash crop from this and other dangerous coastal sites, cured it, and—ignorant of its final uses—sold it to merchants transporting it to distant industries.
5. Commercial feed in the United States is supplemented with calcium iodate (Purina labels, for example, state this clearly); commercial feed in Spain, even under the Purina label, was at the time of this investigation not supplemented. Other feed grown on the Spanish plains is naturally rich in iodide (César Cifuentes, pers. comm.). Livestock passes iodide into the human food chain by way of milk and meat or indirectly when livestock manure is dropped onto cropland.
6. UIE is a rate measurable as micrograms of iodide per gram of creatinine excreted per day. Creatinine is a normal metabolic waste.
7. The term cretinism may come from Swiss patois creitin (L. Christianum), referring to popular usage, which holds that these creatures, though idiotic and deformed, are nevertheless human and therefore potentially Christian ( OED ). Other etymological works suggest roots in early forms of the word "creature," in its sense of innocence or dependence.
8. Iodine deficiency was not so severe as to make cretinism endemic.
9. Hunziker (1924), Plummer (1936), American Public Health and Hygeia articles spanning 1922-1937, and Morton's Salt advertisements all testify to the broad diffusion of this information.
10. I have gained the impression in Escobines, where nowadays only females manifest goitrousness in the higher grades, that in this village cretinism and deaf-mutism affect mostly males. Since male embryos are not known to be more vulnerable to maternal iodine deficiency than female embryos, I speculate that Escobines females born deaf or deficient have a harder time surviving infancy or childhood.
11. MIT is monoiodotyrosene, and DIT is diiodotyrosene. One of each kind are joined to make T3, the more potent of the hormones; two DITs are joined to make T4.
12. The Manihot, Brassica, and Crucifera plant families are high in goitrogens.
13. Unlike cabbage or cassava, the goitrogenicity of these nuts is not well known, probably because, relative to other foods, they are viewed as insignificant in human diets.
14. Only later was it statistically shown that the crisis would have occurred spontaneously without supplementation, though perhaps not in so accelerated a fashion.
15. Very old women in the mountain community of Río Aller not far from Escobines spoke with resentment of just such peremptory intervention. To achieve the desired cosmetic effect, such women were thyroidectomized on a rustic table in the local schoolhouse.
16. Iodine can be conveyed by injecting iodized oil, Lipiodol, an additive product that became available only after mid-century. Public health authorities have injected remote populations with it, those in New Guinea and in the Andes, for example, where safe and sufficient levels of dietary iodine could not be assured. Lipiodol affords protection for a span of from three to five years. Injections have also been found useful in less remote areas, as in Asturias, where, in 1983 at the inception of the campaign to eradicate goiter and cretinism, iodized salt had still not appeared on the market. A cheaper, oral form of iodized oil suspension promises soon to supplant the injected form (Francisco Escobar del Rey, pers. comm.). Basil S. Hetzel gives a fuller account of the development and use of iodized oil (1989, see pp. 58-67 and 111-116).
17. It did not, for example, seem plausible to Severo Ochoa, the Asturian-born recipient of the Nobel Prize in physiology, nor to his compatriot Grande Covián, a nutritional physiologist of international stature, that Asturians could still, in 1980, given the declining incidence of goiter, be experiencing iodine deficiency (pers. comms.).
18. RAI procedures became available in Asturias in the 1960s and were reported as novel procedures by Suárez-Lledó (1962). A more detailed chronology is given in chap. 7.
19. The thyroid disorders possibly resulting from the fallout of nuclear devices—such as those that befell the people of Eniwetok in the Pacific
or the "Downwinders" of Utah and Nevada (Ball 1986)—lie outside of this consideration.
20. CONN and The Merck Manual in Spanish translation, which were the most common desk references of Asturian country physicians, reflect the overwhelming diagnostic/curative emphasis that fills the stage vacated by prevention.
21. Propylthiouracil is one example of an antithyroid agent.
22. Pharmacologic doses of iodine have an altogether different effect than do physiological doses.
23. Toxic coma is sometimes classified, for example, as a psychiatric disorder, ignoring its possible origin in complications of simple goiter.
24. The particular manifestation of defect in the cretin—whether of bone growth retardation, of incoordination, of sexual or thyroidal agenesis, or of sensory and neural loss resulting in deaf-mutism or in reduced intellectual function—depends on the timing and intensity of hormone deficiency both early in utero and in early postnatal life.
Chapter Three Diet and Image in Asturias
1. The name of the village is a pseudonym, to protect the villagers from any unfavorable attention this study might draw. I remind the reader that though prophylaxis was begun in 1984, many villagers still bear signs of the endemia and will bear them for the remainder of their lives.
2. Escobin os (plural form of Escobino) are the people of the village and in a restricted sense, refers only to its males, while Escobin as refers exclusively to its females.
3. In 1987, the single telephone was replaced by telephones in many private village residences.
4. While the term isolation might better characterize the geographic situation of these upland people, they use the term abandonment (from v. abandonar ). Thereby, they put the emphasis not on geography but on relationships between themselves and the larger surrounding society.
5. The demand for injections was so high in Escobines that when penicillin came along, the practicante, eager to reduce his work load, trained two village women to inject it.
6. The reference more complete than Bootello (1934) is lost. During the years of the Spanish Republic, a series of articles, brief notices, and statistical tables in RSHP gave information on water quality and content, from which this conclusion in drawn.
7. Entry into the European Community's common market, the EC (known as EEC in the U.S.), flooded Spain with milk produced under
subsidized agricultural programs. Many small Asturian producers could not compete with the prices of these external milk products.
8. Jane Buikstra, pers. comm.
9. Carvings and paintings of the Middle Ages depicting goitrous people testify to the presence of IDD in alpine Europe; ceramic figurines testify to IDD in the pre-Columbian Andes (for examples, see Merke 1971 and 1984).
10. Middens, for example, in La Cueva de los Azules, 15 kilometers from the mouth of El Sella in the Bay of Biscay, testify to the importance of seafood in the diet of the Asturiense period (Juan Fernández-Tresguerres 1980).
11. The quotes are not taken from Strabo's text directly but from La Gran Enciclopedia Asturiana (GEA s.v. Estrabón).
12. Middle-class urban Asturians, when speaking of their past, habitually introduce this phrase. It has been reiterated to them in Spanish school texts and in the Gran Enciclopedia Asturiana (s.v. Estrabón), but in fact, I have not been able to find this exact phrasing in Strabo's works in either Spanish or English. Its use testifies to the broad diffusion of this stereotype.
13. Some fraction of rural Asturian schoolchildren must have had sensory and motor impediments, and undoubtedly some of these stemmed from IDD, though their teachers could not have known this.
14. Spaniards often speak of the "divine mission." King Juan Carlos spoke of it at a stately occasion honoring the Contadora nations ( El País Panorama, Oct. 22, 1984, p. 19).
15. Throughout the 1960s and 1970s, the villagers would reiterate this phrase, and others like it, to us. The theme will be treated in greater detail in chap. 6.
16. Ruiz de la Peña is a native Asturian and a notable historian of Asturias; he is published more widely in Spain than the brief GEA s.v. reference might suggest. I have chosen to cite his article from the encyclopedia because, in contrast to the scholarly audience to which he usually addresses himself, the encyclopedia article is directed at a much broader audience, and we are concerned here with popular ideas.
In a later section of the same article, Ruiz de la Peña resists this traditional abandonist view and writes, however metaphorically, of the restoration of the lost Gothic Kingdom in the form of a special autonomous principality. This inversion conveys just how heavily the old image of wild rebellion and subsequent margination has weighed on Asturians.
17. Title exempted nobles from taxation; thus, hidalgos on the central plateau and farther south, because they were titled, did not pay taxes. And Basques, because they were situated close to the border and needed
to secure it, were accorded hidalgo status and therefore exempted from both taxes and military duty (Greenwood 1977).
A large proportion of Asturians bore the title for different reasons: (1) for being descendants of those who fought in the Reconquest, (2) for genealogically having proved in the courts of the fifteenth through eighteenth century their "limpieza de sangre" (purity of blood), i.e., that neither Jews nor Moors figured among their ancestors. The latter condition was relatively easy to establish in Asturias where, through the mid-nineteenth century, well over 90 percent of the population was rural. As the lowest rank of nobility (after caballeros who obtained their titles through military service), hidalgos were exempt from taxes and from torture in jail and could not be jailed for debt. Much of the privileges of title disappeared in the nineteenth century, 1830 being the last year in Asturias when hidalgos were still listed officially. Recommended reading: Noel Salomon, La vida Rural Castellana en Tiempos de Felipe II. Madrid: Ariel (1982); also Ramón Prieto Bances, Los hidalgos asturianos en el siglo diez y siete (Oviedo: Universidad de Oviedo), pp. 761-870. (The above paragraph resulted from a pers. conv. with Eloy Goméz Pellón.)
But the notion of hidalgo lingered on in Asturias, perhaps because—even after the waning of privileges—many Asturians continued to be exempt from taxation, owning too little land to be taxed.
18. "The Story of the Crossbeam" in chap. 6 illustrates an Escobino explanation of the village's disrepute. Villagers present themselves in that story as historically displaced Vaqueiros, recipients of a trade foisted off on landless, hardworking innocents.
19. One of Marañón's disciples examined the type in a psychological study of the 1930s (Goyanes 1932 a ); and Martín-Santos's Tiempos de Silencio (1961) carried it over into the postwar novel.
20. Llanes and Gijón were the principal points of entry on the coast.
21. Apparently, it was not well known that Asturians consumed fish, game, seafood, and a variety of cheeses, along with porridge, which was reputed to be their daily fare.
22. The long time needed for maturation limited the number of crops that could be grown in a two-field system, the dietary aspects of which are discussed in chap. 5.
23. The date of the arrival of maize in Asturias is disputed, though it is widely believed that the first corn from the New World was brought in one of Columbus's ships and first planted near Grado, an Asturian county not far from the coast, from where it spread into the plowlands near Oviedo, the provincial capital.
24. Corn lacks the glutens that yeast acts on to make a wheaten mass rise. "Corn bread" in the United States is made light with eggs or made
in combination with flour that can be raised. Asturians, aspiring to eat in a civilized manner, contrived a corn loaf, borona , made of a mass of corn-meal and water baked on the hearth under a covering of chestnut leaves and ashes. Unlike porridge, it could be sliced and therefore passed off as "bread."
25. When introduced to Europeans, maize was not accompanied by the culinary techniques employed in the pre-Columbian Americas. These techniques entailed soaking the corn with line, a process that releases the small amounts of niacin contained in corn. Native American peoples whose principal staple was corn employed these techniques, knowingly or not, thereby preventing pellagra.
26. Only in 1937 was it demonstrated that there was no disease vector but rather a deficiency of nicotinic acid, a vitamin that American nutritional authorities five years later decided to rename niacin (Roe 1973:125-127; Sydenstrecker 1958).
27. The Marañón work is a preface to the bicentennial republication of Casal's Historia Natural del Principado de Asturias, published first in 1759.
28. The painter was Roussel, mentioned both by Roél (see citation below) and (Roe 1973).
29. Roél's original work was not to be found in either the Madrid or the Oviedo medical libraries.
30. To call a disease a divine affliction is in modern terms equivalent to "washing one's hands of it" or "blaming the victim"—classifying it away so as to avoid intervening.
31. At the turn of the century, pellagra still figured in the list of "reportable diseases" and was one of the "low-level killers" (GEA s.v. Sanidad).
32. The ratio of the value of a parcel's annual yield to the value of that land on the market was much lower than the ratio normally considered profitable (García Fernández 1980).
33. The term suggests an even division by half, which may at one time have been the original arrangement. In Asturias, however, the term was widely used for a great variety of unequal sharecropping arrangements.
34. Native cattle were also traditionally selected for their ability to recover rapidly on spring pasture after a winter of extremely short rations.
35. Chap. 5 elaborates on the introduction of nonlocal food.
36. The well-known short story Borona by Leopoldo Alas (1894) develops the symbolic-affective aspects of this dietary staple. The story treats borona as a longed-for "soul food," ironically believed by the story's dying protagonist to contain healing properties.
37. Bread as "blessing" is offered in the ritual known in Asturias as
pan de ánimas, pan bendito, or pan de caridad . The practice is a vestige of the eulogia widely practiced in Western Europe in the twelfth century, holding on through the twentieth century in a number of mountain communities, such as in Sainte-Engrâce of the French Pyrenees (Ott 1981).
38. As if to clinch this point of hereditary defect—expressed as mala sangre or bad blood—the communities that remained goitrous were the very ones in which Asturiano was spoken in a form least comprehensible to outsiders, a vernacular known as lo mas cerrado, the most closed up. The pejorative connotation of ''closed up" is thick-headed.
39. Village population levels may generally have been 30 percent higher than those recorded at the turn of the century. The Escobines population numbered approximately 750 at the turn of the century and again in 1972, while the census of 1934 records a population of 1,034. "We were like this in those days," the older women would say, thrusting their upturned hands toward me, the digits compacted together. The gesture indicated "the tightly packed crowd" of Escobines just before the Civil War was to erupt. I have no reason to believe that other villages did not experience similar expansion and contraction due to the forces discussed here. Also see Fernandez and Fernandez 1988.
40. Evidence of this extension of cultivation is found in the municipal topographic maps (Servicio Topográfico, Oviedo, 1934).
41. The contrasting term, "delocalization" (of the food supply), was introduced to nutritional anthropology by Pelto, as mentioned by Messer (1984).
42. Mountain women were more successful at this than men because they could persuade Nationalist guards to let them through the passes without paying fines. Several Escobinas report that they were initiated into commerce in this way.
43. Grande Covián was by then a well-known reseacher and was coming to be known in international circles. Later, he was called to the University of Minnesota, where he pursued nutritional-physiological research for many years.
44. The censorship code is discussed in detail in chap. 7.
45. Regionalism, waxing since the death of Franco, has brought Asturian regional products such as sidra back into popularity. Regionalism culminated in autonomía, official regional autonomy. After the "traditional regions"—the Basque country, Galicia, and Cataluña—had struggled for their autonomía, Asturias attained it without any.
46. Ballesteros, pers. comm., see R. L. Fernandez (1986:428); also GEA s.v. Sanidad.
47. Dr. Francisco Escobar del Ray, pers. comm.
Chapter Four Kinship and Affliction
1. Justice Downwind: America's Nuclear Testing Program in the 1950s offers an example of such an issue in court (Ball 1986).
2. Chap. 2 explains the logic of the need for speaking of symptoms "not inconsistent with a diagnosis of IDD."
3. The name is disguised; the dates are not.
4. Primos who are offspring of such unions of sibling exchange were called—in the generation that is now very elderly— primos hermanos, sibling cousins. Younger Escobinos maintain that the term means the same as primo, first cousin. Escobinos who in the 1970s and 1980s were still speaking of primos hermanos were most often, however, referring not to the "blood tie" or degree of genetic relatedness but to the special affective quality arising out of the roce, rub or friction, that accompanies some relationships. Roce is likely to characterize the relationship of primos hermanos, because they have in common more blood and property than do most other relatives. Thus, they might well be called "cousins doubly over."
Primos hermanos, as the term is used now in Escobines, is vestigial: as the practice of sibling exchange dies out, the relational specificity of the term is lost, replaced by affective and figurative connotations.
5. Escobinos use the expression casarse por el papa, to get married by the pope. The monetary and other arrangements made with the local priest for such a marriage are not likely to be reviewed by any papal office.
6. The word atrocar in Asturiano means reserving a place for a particular person, or seizing a place that others also desire; also, a child's game (Novo Mier 1979; GEA s.v. atrocar). Since siblings cannot all be ready for marriage at the same time and atrueque can only be realized when the four individuals who make up the two couples have attained the age of marriage, the specialized meaning in Escobines corresponds rather closely to "reserving a place for a particular person."
7. The Western system cannot be perfectly heterogenetic since the number of ancestors cannot expand backward indefinitely. Most of us are not aware of what anthropologists specialized in kinship call "genealogical collapse" (Robin Fox, pers. com.).
8. Here are two more examples of such verses:
|
|
9. Differential in marital age is a concept known as DMA by historians of the family (Goody 1983:129).
10. These figures are approximate but not identical to those given in other publications arising out of this field material. The exact number is always a problem because of emigration and return, comings and goings between Spanish cities and the village, unsettled young couples changing location between parents and in-laws, and Asturian urbanites who still "come home to make hay and harvest potatoes." All of these create trasiego, constant movement in and out of the village.
11. Detailed discussion of household form over time is found in Fernandez and Fernandez (1988).
12. It will be remembered from chap. 1 that my villagewide inspection was limited to those goiters that could be assessed visually, hence those classified by WHO standards as Grade Two or higher. Beyond the goiters open to such casual inspection were those that were personally brought to my attention. Whatever the percentages here, they are an underreport since only a fraction of the lesser grade goiters, under these circumstances, could be included.
13. The incidence of consanguinity in the older group is not as high as the reader may have expected from the discussion on inbreeding. This is because I applied stringent criteria requiring both self-recognition and genealogical demonstration, not hearsay. Precipitous drops in consanguinity with decreasing age have been noted elsewhere in Europe and are known as the breakdown of isolates, but the level of consanguinity in Escobines was higher than any of those reported (Moroni 1969, cited in Bodmer and Cavalli-Sforza 1976). (Since the criteria of consanguinity were not made explicit in these works, they are not exactly comparable to mine.)
14. Drops in consanguinity have been attributed to increased migration accompanying industrial development (Moroni 1969, cited in Bodruer 1974). External emigration has not, however, been the decisive factor for the drop in Escobines. As will be seen in the genealogical charts, emigration was much higher earlier in the century than it is now.
15. The spouse from elsewhere is known as esposa forastera . In both of these cases, the marriage was performed in Cuba, one esposa coming
from Grado in the Asturian lowlands, the other from Zamorra on the Meseta. Both couples, curiously, are childless.
16. The settlement names are fictitious, and the map slightly disguises the terrain.
17. Robin Fox spoke about ''messy relationships" when amplifying some aspects of his work among the Tory Islanders (pers. comm., Fox 1978).
18. Tree diagrams do seem to be visualized by elder, male, Escobinos. Men saw themselves at the center of bilateral kinship networks, such as were directly taken down by J. W. Fernandez in this Asturian field situation and by Fox (1978) in the Tory Islands. I, however, found myself in the field unable to take down the women's "genealogical gossip" in its full horizontal spread, compromised as I was with conventional (male) methodology and diagrams. Unable to record it in its full extent, I felt procrustean, cutting off family limbs. Fortunately, our large number of tree diagrams, complemented by field notes and stories, have allowed me to reassemble these limbs.
19. Por el hilo se saca el ovillo, por el pasado a lo no venido, is one example of such thread imagery, which may be translated as "untangle the thread, and you'll get a whole (ball of) yarn (story)." Particularly common is the image of a skein or a ball of yarn, the self, becoming unwound over a lifetime. Escobinas also know themselves to be related as fibers, irregularly pounded into a fabric of felt. An Escobina employed this image when speaking of her portion of the fabric as being particularly thin: she had been conceived by a Guardia Civil passing through the village on a short assignment and was born to an unwed mother who bore no further children. This did indeed make the number of her blood relatives "too thin for protection." The latent reference here is to a slipper made of inferior felt fabric, too thin to protect the foot from the heavy wooden shoe ( madreña ) worn over it.
20. Escobinas speak of intermingled blood as sangre toda mezclada .
21. The double occurrence of first names also suggests the atrueque relationship. All but the most common first names, like María and Manuel, are commonly bequeathed.
22. "The Ballad of the Hide-Aways" records that mockery. It was composed by Rafaél García and recited onto tape by his son Tino at the Fiesta de Carmen of 1984.
23. The last name Polés (a pseudonym) is common both in Escobines and El Texu. The last name of Jesús, Flor's husband, is Polés. Flor recognized the details of marriage between these villages to be confused, for property disputes entangled the issues. This made it impossible for
her to completely recount the relationships. She assumed her in-laws and aunt [21] were related, making some Polés both her own and her husband's cousins.
24. Instead of Gerardo, Azucena married an offspring of her father's cousin.
25. Salvador is also the descendent of two intricately intertwined branches of the families Rabín and Avello, which figure on our Genealogy G57.
26. El Mecánico is a respected elder appearing in Genealogy 3b. He and his siblings practiced atrueque, but only he had offspring.
27. The casual observer would attribute Paco's disability to Down's syndrome and assume he was the last of the couple's four offspring. In fact, he was third, born in rapid succession after his sisters. Chusín, his very bright brother, was born ten years later, just as Flor's menstrual periods were waning and her goiter was becoming nodulated.
28. The relationship through the father is distant but proximate through Ignacio's mother, a sister of the man [27] married to Irene. This is seen more clearly on Genealogy 3b where Jesusa and Ignacio reappear.
29. Flor must have been about 4'7", coming up barely to my collarbone (I am 5'4").
30. The Spanish word subnormal has appeared in the village vocabulary only since the late 1960s, when families retaining retardates at home began to be subsidized. With or without subsidies, Escobinos have always kept retardates at home. When the opportunity presented itself, they readily, however, latched onto subsidies and their accompanying terminology.
31. The suffix ona exaggerates and caricatures the noun to which it is attached; thus, moco becomes mocona, "the Big Fat Snot-faced Woman."
32. Dr. Joaquín Fernández García, a hematologist, was the visiting physician. He grew up in a nearby village, married an Escobina, and became well acquainted with her relatives and former neighbors.
33. The atrueque relationship is here again suggested by the almost identical naming of two women: Luisa Rabín del Cuadro and Luisa del Cuadro Rabín. The redundancy of names has been caricatured in two poems by Ceferino Díaz. (See J. W. Fernandez 1988b for a critical appraisal of these poems.)
34. For lack of better evidence, I did not, however, count this as a consanguineous union.
35. The aunt is María Leo, the daughter of Leo, who figures on Genealogy 3a.
36. Victoria is the daughter of one Gregorio (not on the chart) whose
father had come from another high-lying village in search of whetstone, which he prepared and with his son Gregín sold across the north of Spain.
37. The spouse of Rosa Tras Casas is a grandson of Francisco, her paternal great-grandfather; Rosa and her husband are related in yet another way, for they are both offspring of the Mazán cousins (not shown).
38. This is not the only case of the afflicted's vulnerability to exploitation. For similar cases, see R. L. Fernandez (1986, chap. 4).
Chapter Five Land and Diet
1. No official calculation has been made for this figure. I calculated it by inspecting the topographic maps of the county and relating them to maps at Hacienda, the provincial bureau of taxation. These are based on U.S. photographs made in the course of military overflights of the 1950s.
2. Consonant with my use of pseudonyms, I have correctly represented the relationships of mountains, rivers, and land but disguised their particularities.
3. Vecinos in its meaning as neighbor is a common word, but it also has more restrictive legal meanings. See, for example, Behar (1986).
4. The number is indefinite because land is registered according to the owner's official place of residence. Outmarriage therefore makes it difficult to ascertain the number exactly, since property tends to accompany marriage. Furthermore, transfers, divisions, and consolidations of property are often not registered in the year or even decade in which the transaction occurs. Some meadows totally escape registry because they fail to be disclosed at the angle from which the area has been photographed. The households we sampled work an average of 15 parcels of land, which results in more than 2,000 parcels. But this number does not reflect the households made up of one or two elderly people, many of whom have already passed on their land.
5. These were calculated after inspecting the Catastro of 1964, the land records of Escobines filed in the Ayuntamiento, the county office.
6. Jesús García Fernández (1980) calls cortijo what Escobinos consider huerta. The land types, though called by different names in different localities, are similarly divided throughout much of Asturias.
7. Hacienda, the provincial land registry office, is an excellent source for obtaining raw data from which a picture of the landholding pattern in any particular community can be drawn, such as, for example, the range and average size of parcels, their modal size, and the average number of parcels held in a particular name. But Hacienda is a poor source for obtaining the kind of information needed here, information that would tell
us how much plowland, during a particular woman's youth, was available to feed that mature woman of today. Such information could help us decide whether a particular individual had regular access to cultivated crops or had regularly to resort to the fruits of monte.
For several reasons, this kind of information cannot be obtained from Hacienda: the land worked by a household may be held under several names; these named individuals may be living or dead, villagers or absentee landowners (few of these remain on the books), and do not necessarily reside in the household making use of the land; the disparity between registered owner and cultivator occurs in part because Escobinos hesitate to pay the cost of officially transferring title, for another part because transfers may only be tentative, awaiting the demise of a parent or the return of an emigrant; some women, on marriage or later, transfer the land coming to them from their parents into their husband's name, but many do not; grown siblings may refuse to agree to the inheritance assigned them by lot, and sibling groups may prefer to hold the parental inheritance intact; neighbors, friends, and relatives may work plots not their own and for convenience lend or rent out other plots.
8. Inequalities such as these are common in the Iberian Peninsula, though ideologies of equality tend to mask them. They have been documented very thoroughly for one Portuguese village by Brian Juan O'Neill (1987).
9. The verse parallels one from the coast:
|
Ethnomedicine is covertly expressed in this verse. It suggests an appreciation of the dietary mechanism that compensates for the goitrogens in chestnut. Even if this is not explicitly understood, one is grateful when chestnuts are complemented by sea urchins in times of famine. In technical language, the goitrogenous food is complemented by food rich in iodine.
10. Douglass (1975) mentions their use in Basque country, as does Lisón Tolosana (1971) in Galicia. Folklore, law, architecture, and cookery in all these areas bear witness to the widespread use of chestnut, at least at some earlier time.
11. Individuals have long known that endemic goiter is prevalent in
these Galician villages (Fernández de Rota, pers. comm.). Galician officials acknowledge widespread endemic goiter in the 1980s; see chap. 7.
12. Occasionally, turnips and other lesser winter crops made way for the planting of early potatoes, androxines . But weather was too unreliable to permit this on a regular basis. They are named for antróxu, Carnival, the time of year in which they are planted.
13. The verse is difficult to translate because of a sexual innuendo. Coxera is usually a garage, and it can be a storehouse, as J. W. Fernandez translates it (J. W. Fernandez 1977:470). In this context, coxera can also be translated as the seat of fertility, moved from its proper place between the hips up to the throat. The mocking Escobinas have apparently surmised some relationship between infertility and goiter, even if they seem only to be denigrating the appearance of Texuanas, who in the Escobinas' opinion are more goitrous than themselves. The verse goes on to implicate chestnut skins in the same manner:
|
Texuanas are here accused of being careless housekeepers, not bothering to remove the interior skin of the chestnuts, which, if eaten, is associated with goiter. The verse does not make clear whether carelessness or goitrousness is the more serious fault. But to those who chant it, the verse makes very clear that slovenliness may be linked to deformity.
14. For example, Medio (1953), Alas (1884, 1894), Laforet (1944), Quiroga (1952, 1973).
15. Vaqueiros, for example, have blended so much into general Asturian society that by 1984, ordinary Asturians had to be recruited to represent "the Vaqueiro couple" in the wedding set up in the Vaqueiro zone as a tourist attraction. The Hurdenos, through reforestation of their land, have likewise lost some of the distinctiveness, based on misery, that had for decades been considered a tourist attraction. See chap. 7.
16. In this light, it is hardly surprising to learn that "white" tortillas, made of wheaten flour are regularly consumed by the upper classes in Mexico, while "yellow" tortillas, made of maize, are consumed by the lower classes, and that "taste'' for one color or the other is considered a class marker.
17. It will be seen in chap. 6 that in fact Escobinas did not always successfully deny meaning to goiter. The insult "¡ papuda !" (goitrous), in the
occasional heated exchanges I witnessed, signaled a turning from insult to blows.
Chapter Six Narrative Accompaniments of Rural Character and Disrepute
1. The verse in the epigraph that opens this work is translated from T. Cuesta (1880). The line refers to the women of two industrial centers, Pola de Lena and Mieres, in the south central part of Asturias. J. W. Fernandez captured the spirit of the verse in translating it for me but to do so had to omit one of the place-names. The verse suggests the extent to which endemic goiter became part not only of oral narrative but also literary production.
2. The vast ethnographic work of Franz Boas rests to an important extent on the collection of folklore, which was used to give insight into culture and the differences among cultures. His students constitute a large segment of twentieth-century anthropology and collect folklore assiduously. The study of acculturation or group psychology has often been the purpose behind these collections.
3. " La Piriquina " is one of these women, precociously menopausal at age thirty and labeled as "oligophrenic" in the archives of La Collaóna, the Asturian mental institution in which, from time to time, she has been a patient. Her role as a balladeer is described by J. W. Fernandez (1988 b ).
4. The age of these severely retarded individuals is significant. None born since the end of autarchia have survived into adulthood. I interpret this to mean that by the 1950s, the diet had, however slightly, improved enough to prevent fetal cretinism. It could also be interpreted to mean that endemic cretins, in recent times, have died young. Nothing I have heard or seen in the village supports such an interpretation.
5. This was the case until the mid-1970s. Flor la Tabernera's retarded son moved into the home of his brother Chusín after she died. Since Chusín heads up a construction firm and no longer works the land, few labor-intensive chores remain for this el ay to do.
6. Even while being considered así a woman can be curiosa, clever, handy, or privy to special knowledge or having special aptitudes. For example, the woman Chusina, while expressing some traits and conduct that seemed to me at first not inconsistent with a diagnosis of IDD, has distinguished herself as a spontaneous versifying commentator on village doings. On learning more about her, I discovered she was an alcoholic.
7. Vinjoy, the first school in Spain for the deaf, was established in Asturias in the 1950s (GEA s.v. Vinjoy), undoubtedly because of the higher incidence of deafness in Asturias. The reason for that higher incidence
was, as far as I have been able to ascertain, never explored. Had the clues couched in the vernacular been followed up, specialists might have related Asturian deafness to a high incidence of Penred's syndrome, congenital deafness produced by maternal hypothroidism, and decided to prevent it.
8. People have a tendency to create euphemisms to escape the harsh realities of labeling. Because of this, specialized vocabularies of affliction and insult are likely to always have been shifting.
9. Davydd J. Greenwood in "Continuity in Change: Spanish Basque Ethnicity as a Historical Process" does not restrict his attention to the interplay of ethnicity and pathology, as I do here. He makes a major contribution in arguing that ethnicity "is that part of the culture of a group that accounts for its origin and character, thereby differentiating it from other groups within large-scale political units and setting the tone for its relationships with those groups and with the government. It is a useful concept only when applied to groups incorporated into a large-scale institutional system. Thus, the symbols of ethnic identity and the institutional context of intergroup relations must be studied together as they develop over time." His argument centers on Basque identity, not an identity of "disrepute" such as I argue here.
Nevertheless, his proposal to restrict the use of ethnicity to the relationship of groups incorporated into—or (I would add) marginated from—large-scale institutional systems helps us focus on the unequal access to resources, too often disguised when we speak loosely or atomistically of "cultures" or "ethnicities."
10. Collections from the central mining zone are numerous, as can be seen in IDEA's list of publications.
11. Uría describes how Francoism bent the documentation of vernacular languages and lore to support political ends. The tales selected for publication during the Franco years almost uniformly emphasized the rusticity, ignorance, even animality of the rural Asturian; i.e., they were a selective (mis)representation of the whole spectrum of rural folklore. Noble aspects of rural character rarely surfaced in this literature, even though there were notable precedents, as, for example, Clarin's characterization of El Parroco de Vericueto (Alas 1894).
12. I do not mean to exclude men from also having this concern. I did not, however, find myself in one-to-one situations with men when such stories were told.
13. Foreigners are referred to as extranjeros, and strangers are referred to as forasteros —people not known locally. To villagers, the latter are an important category of people because they represent the larger society by which they feel judged.
hence confirmed bachelors. The "confirmed" may be a consequence of their own disinterest in marrying or of the obstacles the community places in the way of their marrying (see Fernandez and Fernandez 1988).
15. This attire consists of black corduroy pants, white shirt, black vest, and black beret, a dress now worn rarely in these villages, except by the members of the oldest generation and especially by its most distinguished representatives.
16. Presumiendo y tomando el sol como señoritos!
17. Indeed, such swelling—consonant with the physiology of pregnancy under conditions of iodine deficiency—was taken as a first sign of pregnancy not only in Escobines but throughout the ancient world.
18. Iodine prophylaxis was initiated in Argentina in the 1950s (Clements et al. 1961).
19. The story seemed to be used as a psychological prop, to distance oneself from the stories women had told me of their own deprivation, whether of losing a cow, scrubbing floors for a señor, or spending years in Castile as a maid.
20. The local diminutive would be ina .
21. Castigan a las que no se conforman a la cruz .
22. Cabbage or berza was included on the menu. Locally created verses, those not drawn from the folkloric collections published under the Franco regime were declaimed.
23. Soon after writing the story into my notebook, the men thought to add the following sentence: "Such a sign has been preserved in the Church of Saint Martyr of Pravia (Asturias)." Pravia is in western Asturias.
24. The explanation was given a new twist but basically synthesized from speculative articles explaining the long-standing prejudice against Vaqueiros.
25. The census of the Marqués de Ensenada, an official census of the late eighteenth century, inventoried people, land, stock, agricultural production, and rent and tax obligations. The answers to its query in Escobines are missing, but nearby upland municipios —Cabrales and Onís—record that rental payments were made in butter (or stock).
26. This resistance was expressed at the Princeton University Fairy Tale Conference, March 1984.
Chapter Seven Advocacy and Opposition: National and International
1. See Michel (1847), Maud (1896), Buñuel (1934), and de la Vega (1964).
2. See, for example, Marañón (1927, 1928), a series of articles in Revista Clínica de España (a series of articles by Villar Ortiz, Yanez Polo
Conde Yague, and Rojas-Hidalgo and others over the years 1975 through 1981), and the Chronological Bibliography Bearing on IDD in Spain (R. L. Fernandez 1986:361-398). The médico titular in Las Hurdes has tried to dissuade numerous other investigators from using the local population as a natural field experiment (Dr. Javier Durán, pers. comm.). Also see R. L. Fernandez (1986:423).
3. See R. L. Fernandez (1986:445-453) and Jesús de Miguel (pers. comm.).
4. Marañón (1927), de la Vega (1964).
5. The documentation on these programs is indirect. Marañón (1927) reports on a work without title by Vidal Jordana which was to be published in 1928. He gives no results or explanation for the lack of follow-through, and I was unable to find any references to Vidal Jordana's program in the literature until just before this work went to press (Vidal Jordana 1924, 1927).
6. Earth without Bread is usually listed in university film catalog headings as art or film history. A well-known critic of travel literature kindly viewed the film with me and saw it as surrealist (Mary Pratt, pers. comm.). But Richard Herr (1971), in his chapter on the Second Republic, holds that Buñuel turned away from surrealist cinema to make poignant realism.
7. W. Eugene Smith's still photographs of Spanish villagers—were widely diffused in the 1950s—reinforce this impression.
8. The narration does not explain that Hurdenos, like other rural people where soil is poor, search the thorny terrain for leguminous plant material rich in nitrogen. In Las Hurdes, it is used to fertilize minuscule terraces of cultivated land wrested from steep washes.
9. One child, reported by the narrator to have died soon after the film was completed, is depicted lying in the street and ridden with flies.
10. The sending cities were Cáceres and Ciudad Rodrigo (de la Vega 1964).
11. Buñuel applied to El Patronato de Las Hurdes to sonorize the film. Marañón flatly turned the application down and suggested Buñuel dedicate himself to filming "sunnier aspects of Hurdeno life, such as their dances." Buñuel, claiming to have seen his name on a list of persona non grata, definitively left Spain soon after this interview. He later sonorized the film in France.
12. The quoted phrases come from the introduction to de la Vega (1964).
13. The narrator in Buñuel's Earth without Bread uses this phrase.
14. The idea of "the other" is developed by Todorov (1987).
15. Velázquez painted a number of Hurdeno dwarfs (Brown 1986). For a long time, Hurdenos exploited their most deformed as a resource
selling them to the court (Jonathan Brown, pers. comm.) or turning them into professional beggars (de la Vega 1964).
16. The average UIE was below 25 (Escobar del Rey et al. 1981 a :198: 233-246).
17. The children eating exclusively at home were four times as goitrous as those taking all their meals in the feeding programs, and their T4 was correspondingly low (Sánchez-Franco et al. 1983).
18. The sequence of medical articles on Las Hurdes is too extensive to be fully developed here (see R. L. Fernandez 1986:374-381, Escobar del Rey 1987).
19. Dr. Javier Durán spoke of Escobar's letter this way (R. L. Fernandez 1986:423-427), as did others. The national department of health, formerly a division under the Ministry of Internal Affairs, became the independent Ministry of Health in the post-Franco years.
20. Dr. John B. Stanbury (pers. comm., letter 1978).
21. The passage was cited in de Miguel (1979).
22. This part is based largely on my reading of works by Jesús de Miguel (1976, 1977, 1979).
23. Social security is now known as Instituto Nacional de Previsión.
24. Dr. Radhamés Hernández Mejía, professor of preventive medicine at the University of Oviedo, shared this folklore of public health with me.
25. The same incident is mentioned in GEA (s.v. Sanidad).
26. Goiter is found even now in the cities and middle class (see R. L. Fernandez 1986: Appendix C: Thyroid Disorder in Middle-Class Women, pp., 458-464; also Laher-Montoya n.d., and Rodríguez Cuartero 1976).
27. Losada's work was untraceable in Spanish medical libraries.
28. The incident of contaminated water in a worker barrio of Vallodolid is well known to public health physicians. Professors openly spoke of it in class, even during the later Franco years (Hernández Mejía, pers. comm.). No one I asked could cite documents referring to this incident. Nor could I, in 1984, obtain documentation on Tourism's decisive move.
29. The United States, for example, sent Davenport (1932) and Kimball, among others. Most European countries sent several delegates, as did Japan and Indonesia.
30. Marañón pursued the theme of glandular determinism both medically and popularly. Curious about the interaction of inherited temperament, pathology, and worldly affairs, he investigated, through history and literature, prominent Spanish figures such as Don Juan (1928), and El Conde Duque de Olivares, the powerful adviser to Philip the IV (1936, 1939) and prompted others to similar explorations (Goyanes 1932 a , 1932 b ; (Jimena) de la Vega 1935).
31. The remark is that of a retired colleague (Enrique García Comas, pers. comm.). See interviews in the Appendix (R. L. Fernandez 1986: 431).
32. Marañón and a small group of friends, accepting the inevitability of a vote in favor of the Republic, had tried to smooth the transition from monarchy to Republic. The actual signing of the papers effecting that transition were signed in Marañón's home. Later on, as a friend of the Republic, he had gone into exile. The occasion of his return was grand: Franco went personally to meet Marañón at the airport, where both figures were photographed (published and commented on in ABC, a Madrid daily) bowing to each other as if replaying Velázquez's historical representation of the surrender of Breda (Felipe Ruíz Martín, pers. comm.).
33. Out of 650 afflicted individuals in a set of nearby communities, 8.6 percent were cretins and 4.9 percent were deaf-mutes. Carrasco does not give the size of the total population from which the afflicted were drawn. Perhaps we are to surmise they were all afflicted.
34. Apart from those women expected to have perinatal complications, in the 1930s, only the wealthier country women tended to give birth in clinics and hospitals.
35. Aún causará en la raza muchos estragos .
36. In 1936, RSHP went into a hiatus, resuming publication in 1938. I did not continue to check for any follow-up after 1945.
37. This might appear to be at odds with what the Falange, Franco's political party, so enthusiastically tried to promote: that individuals accept their small place in the organizational hierarchies of the nation. Such an ideology can be seen as collectivist. Because of this apparent similarity, I used the word ''tainted" in the previous sentence. The issue was not so much the rejection of collectivism per se but the rejection of projects tainted by association with the Republic.
38. To my knowledge, this censorship was not abrogated during Franco's time, though it is quite possible that as time went on, it ceased to be rigorously enforced (Hernández Mejía, pers. comm.).
39. Torrelavega is in Santander, the coastal province bordering on eastern Asturias.
40. This is a dosage now considered well above any optimal intake of iodine on the dose-response curve.
41. This Escobina had heard about prophylactic iodine from a cousin who had gone on to medical school, but she declined his suggestions for taking it. Attitudes toward prevention were to change, however. In 1987, her granddaughter, age 23, was advised to undergo a thyroidectomy to avert a possible cancer of the thyroid. The goiter was apparent to no one
in the community, not even to herself. While she was then the youngest Escobina to undergo this operation, by 1989, two of the young woman's peers had been scheduled for it as well.
42. José Luis García García, an anthropologist working in western Asturias, kindly gathered this information for me.
43. The earlier editions were not traceable. Dr. Nájera, in 1984 head of the section of Health Education in the Ministry of Public Health, became familiar with it during her medical training in the late 1950s (R. L. Fernandez 1986:401-403) and continues to use it as a basic reference. All the clinical physicians I interviewed also relied on it as their basic text (1986:423-457). Some of these older physicians did not until recently own the text. Dr. Ballesteros, for example, remembering the scarcity of books during his medical training in the 1950s tells that, as a clinician, he relied for years on the notes he had taken during his student years (1986:428-430). The first post-Franco edition, published in 1979, somewhat updates the treatment of IDD, and the 1987 edition is completely revised.
44. The sections are chapters: 39, Food and Public Health; 42, Additives; 52, The State and Social Medicine; 54, Consanguinity; 58, Genetics and Inheritance; 61, Chronic Diseases.
45. The group found 0.25 microgram of iodide per liter.
46. The goitrogenous hazard was never addressed by Marañón. It came within the compass of established medical knowledge of the 1930s (Cameron 1935; Medvei 1982) while Marañón headed up the Patronato.
47. Ráfols, a chemist employed by the national salt works, was in charge of this small-scale production. In a number of publications both house and professional, Ráfols subsequently advocated expanding the production of iodized salt. See salt correspondence (R. L. Fernandez 1986:406-412). His efforts were ignored by the industry.
48. Landázuri may have been somewhat freer than other researchers to introduce prophylaxis. He was reputed to be a member of Opus Dei, the lay religious organization of technocrats (and others), whose loyalty to state and religion went relatively unquestioned. His well-known submission to a demanding discipline seemed to license him to engage in activities generally denied others.
49. The centralized government tolerated only a folkloric kind of regionalism, one that celebrated quaint marginal activities such as folkloric dances and the distinct rustic speechways of very local comarcas (naturally bounded geographic zones). Speechways were a proper scholarly focus only when relating to rural subsistence or other activities supporting a comfortable nostalgia, as can be seen in the long list of publications put out by IDEA.
50. Given the scarcity of foreign exchange, few current publications
were available to him, but he did make two references to post-World War II work from abroad.
51. I managed in 1978 to interview the aging Delor Castro in his threadbare office located at the top of a four-story walkup. He was too unaccustomed to an accent like mine for us to communicate very effectively. Nevertheless, he seemed amazed that I knew of his book: "Someone . . . so far away . . . when it was ignored by my colleagues!" He tried to tell me of estrangement from colleagues and the names and institutions that had dropped out of his life. While I, understanding him only with great difficulty, could get no grounded facts, I did gather that he felt himself professionally sanctioned and ignored.
52. The quote comes from an advocate of prophylaxis who, for obvious reasons, must here remain anonymous.
53. Another example of a Spanish advocate of prophylaxis ignored in his own country is Espinós, a Valencian physician who, like Delor Castro, spoke out about IDD on the threshold of his retirement in 1967. Such delayed outspokenness may not be for nought. Together with men like Altava Alegre and Alteve Vidal (1975), the limited radius of their diffusion may yet help to raise the demand for prophylaxis.
54. Materials left over from the health campaigns of the 1970s were kindly made available to me in June 1984 in the Education Section of the Ministry of Health.
55. Parados is the term, according to Carrasco Cadenas, that is used to speak of the "children who had become developmentally fixed" in central Asturias.
56. His survey reported goiter in 33 percent of the schoolchildren (García Pérez 1977, unpublished MS).
57. See correspondence (R. L. Fernandez 1986:406-414, 422, 435-436).
58. See correspondence (R. L. Fernandez 1986:406-414, 435-436).
59. Galicia is the most northwestern province of Spain, borders Asturias on the west, and has a climate similar to that of Asturias. The two provinces are considered so similar as to be called hermanos, sibling provinces.
60. La Voz de Galicia published a series of articles on the subject in 1983.
61. See Salt correspondence (R. L. Fernandez 1986:407-415).
62. A letter from Manuel Broto (Apr. 23, 1982) of the Unión Salinera de España specifies these facts, which are updated by Ráfols (R. L. Fernandez 1986:413).
63. I had written the Director of Solvay (Dec. 4, 1981): "I am a human ecologist trying to identify the obstacles that prevent distribution of
iodized salt in Spain. I understand that (1) Solvay of Santander manufactures iodized salt only for export, and there is no other iodized salt on the market in Spain, and (2) there is at least a limited need for iodized salt in Spain; a physician in Asturias cannot obtain it for use in a pilot project for children residing in a zone of endemic goiter. Please correct me if the first of these facts should be wrong."
64. Similar emergency action was taken by Extremeño health personnel on behalf of people in its more afflicted zones, such as Las Hurdes.
65. Such large units of salt are convenient for rural households that slaughter at home and preserve the year's supply of pork with salt.
66. The article, written in the mid-1970s, was to my knowledge never published.
Chapter Eight Closing the Gap between Therapy and Prevention
1. Conspiracy not so much in the sense of a planned conspiracy for evil ends but rather—as in the second definition in Webster's Second International —a concurrence or general tendency, as of circumstances leading to one event.
2. See extended work-up of these figures in the Appendix.
3. Just before going to press, two more young "goiterless" Escobinas told me of having been scheduled for goiterectomies in the near future.
4. Nodulated goiters greatly increase the risk of thyroid cancer (Fierro-Benitez et al. 1973).
5. As late as 1981, Piedrola Gil was still describing this self-medication in Medicina Preventiva .
6. Indeed, the head of the Austro-Hungarian empire once mandated dietary iodine supplements for all the troops (Peter Drucker, pers. comm.). The supplement, however, seems to have been given in pharmacological amounts and was administered to the segment of the population least likely to be experiencing iodine deficiency.
7. See Matovinovic (1983) and Kelly and Snedden (1960:81-91). Any computer search of more recent medical publications reveals the extensiveness of this effort in much of eastern Europe and the Soviet Union.
Appendix
1. See Fernandez and Fernandez 1988 for a detailed demographic presentation of Escobines.
2. This figure counts a small but unknown number of women twice, those infants in 1934 who were counted again in 1972 in the cohort of
women age 30 to 39. This overcount, however, is offset by an unknown number of women born and deceased between 1934 and 1972, who do not at all enter the count of the needlessly afflicted.
3. The calculation is expressed as (0.56 x 461).
4. Others may have failed to come to my attention. The most recent goiterectomy was performed in 1987 on a 23-year-old Escobina whose goiter had not been apparent to her fellow villagers. See chap. 7, n. 41.
5. The calculation is expressed as (15/750 = 20/1,000 = 1/50).
6. The calculation is expressed as (300,000/200 = 1,500).
7. The rate of 1 goiter in 200 appied to a population of 300,000 yields 1,500 goiterectomies. Two percent may be assumed to be goiters not caused by iodine deficiency. Hence 1,500-30 = 1,470 (1,500 x 0.02).
8. This calculation is expressed as (20 x 40), 20 years times 40 per year.
9. Dr. Cadórniga, the head of the endocrinology service in the main hospital of the province, could give no exact figures (see below) but estimated ''a number per week." If we take this number as five, then there are about 250 goiterectomies in this hospital per year. There are, in addition, private hospitals and clinics in the region where such operations may also be performed. Goiterectomies have been done in Asturias since the 1920s but became frequent in the public hospital in the 1950s. At 250 per year for 30 years, this larger total estimate is 7,500 or $15,000,000.
10. Works such as Warren and Adel (1984) do take context into account, but their outreach is very limited.
References
ACC/SCN
1988. The Prevention and Control of Iodine Deficiency Disorders. United Nations, Administrative Committee on Coordination—Subcommittee on Nutrition. ACC/SCN State-of-the-art Series, Nutrition Policy Discussion Paper No. 3. By Basil S. Hetzel, with discussion by F. Delange, J. B. Stanbury, and F. E. Viteri and introduction by M. Lotfi and J. B. Mason.
Acta Endocrinológica
1973. International Symposium on Endemic Goiter, Innsbruck, Austria 507. Oct. 1972. Supplementum 179 accompanies vol. 74. Copenhagen: Periodica.
Alas, Leopold
1884. La Regenta. Oviedo.
1894. El Parroco de Vericueto. In: Cuentos.
1970. Borona. s.v. GEA 1970.
Altava Alegre, V., and J. T. Altava Vidal
1975. Profilaxis del bocio endémico. Anotaciones a la metódica actual. Rev. Esp. Enf. Ap. Digest SLV 105:105–112.
American Journal of Public Health
1924–1935. Sample of articles touching on goiter from 1924 through 1935: 1924:1038–1042; 1929:128; 1929:1090–1097; 1932:49–64; 1933:1115–1123; 1934:187; 1935:1285–1295.
Anuario Estadístico Oficial
1970. Madrid.
1975. Madrid.
Aranda, A., M. J. Obregón, et al.
1981. Estudio piloto para la detección precoz de hipotiroidismo congénito en España. Endocrinología 28(3):85–90.
Aranda, R. J., and F. Díaz Cadórniga
1985. Bocio endemico en el Principado de Asturias. Monografías Universidad de Oviedo.
Aranda Regules, A., et al.
1986. Bocio endémico en Asturias. Consejería de Sanidad, Asturias.
Ball, Howard
1986. Justice Downwind: America's Nuclear Testing Program in the 1950s. Oxford: Oxford University Press.
Behar, Ruth
1986. Santa María del Monte: The Presence of the Past in a Leonese Village. Princeton: Princeton University Press.
Bernard, R. J.
1975. Peasant Diet in Eighteenth-Century Gevaudan. In: European Diet from Pre-Industrial to Modern times, ed. Elborg and Robert Forster. New York: Harper Torchbooks.
Bernstein, Basil
1971. Class, Codes, and Control. Vol. I. London: Routledge and Kegan Paul.
Bodmer, W. F., and L. L. Cavalli-Sforza
1976. Genetics, Evolution, and Man. San Francisco: W. H. Freeman.
Boletín Oficial del Estado
1944. Ley de Bases de Sanidad Nacional. BOE 1611:1587–1601.
1983. Reglamentación Ténico-Sanitaria para la Elaboración, Circulación y Comercio de la Sal y Salmueras Comestibles 14433:15261–15264.
Bolton, Ralph
1979. Hypoglycemia and Aggression among the Qolla. Ethnology 12:227–257.
Bootello, A.
1934. Nuestros primeros resultados en el estudio del yodo en los alimentos españoles. Rev. San. Hig. Públ.(1):506–507.
1935. Determinación del yodo en productos biológicos. Rev. San. Hig. Públ. (2)(np).
Botella-Llusía, José
1973. Endocrinology of Woman. Philadelphia: Saunders.
Brown, Jonathan
1986. Velázquez: Painter and Courtier. New Haven: Yale University Press.
Buchbinder, Georgeda
1977. Endemic Cretinism among the Maring: A By-product of Culture Contact. In: Nutrition and Anthropology in Ac-
tion, ed. Fitzgerald Pp. 106–116. Assen/Amersterdam: Van Gorcum.
Buñuel, Luis
1934. Earth without Bread .
1982. Mi Ultimo Suspiro, Memorias. Barcelona: Plaza y Janes.
Buylla y Alegre, A., and R. Sarandeses y Alvarez
1900. Memorias de Historia Natural y Médica de Asturias por el Doctor Don Gaspar Casal, annotated by Buylla. Oviedo (Spain).
Calderín, Dr. A. M.
1942. Vitaminas y Sordera: Experiencia carencial del Madrid rojo: Julio 1936-marzo 1939. Rev. San. Hig. Públ.:420–445.
Cameron, A. T.
1935. Recent Advances in Endocrinology. Philadelphia: P. Blakiston's.
Carrasco Cadenas, E.
1934a . Temas de higiene alimenticia de urgente atención sanitaria: Tres Conferencias. "El bocio y cretinismo endémico como enfermedad por carencias alimenticias. Su profilaxis yódica." Public. Esc. Nac. Sanidad:3–142. Madrid: Escuela Nacional de Sanidad.
1934b . Estadística y Epidemiología, Estado actual de actividad del foco de bocio endémico de Asturias. Rev. San. Hig. Públ. (1):497.
Casal, Gaspar
1959. Historia Natural, y Médica del Principado de Asturias. Bicentennial edition of work originally published in 1759. Oviedo: Excma. Diputación Provincial de Oviedo.
Catastro del Ayuntamiento
1954. Hacienda, Ovideo.
Cátedra, María
1976. ¿Que es ser Vaqueiro de Alzada? (el mito popular). Expresiones de la Cultura del Pueblo. Madrid: Centro de Estudios del Valle de los Caídos. Pp. 155–182.
1979. Vaqueiros y pescadores. Madrid: AKAL.
1986. Mito e historia de los Vaqueiros de Alzada (el mito intelectual). Madrid: AIC (Analisis y Investigaciones Culturales (26) enero-marzo; Ministerio de Cultura. Pp. 11–28.
1988. La muerte y otros mundos: Enfermedad, suicidio, muerte y más allá entre los vaqueiros de Alzada. Gijón: Júcar.
Cavalli-Sforza, Luigi Luca
1981. The Genetics of Human Populations. San Francisco: W. H. Freeman.
Clements, F. W., et al.
1961. El Bocio endémico. Geneva: OMS (WHO). The Spanish edition of Kelly and Snedden 1960.
Comisión Central de Censura Sanitaria
1942. Normas aprobadas por la Superioridad para la aplicación de la censura sanitaria por las Comisiones provincials. Rev. San. Hig. Públ.:87ff.
CONN
n.d. An annual handbook that keeps Spanish country physicians up to date with biomedical advances made in the Englishspeaking world.
Connolly, Kevin J., Peter O. D. Pharoah, and Basil S. Hetzel
1979. Fetal Iodine Deficiency and Motor Performance during Childhood. The Lancet:1149–1151.
Crenson, Matthew A.
1971. The Un-Politics of Air Pollution. Baltimore: Johns Hopkins University Press.
Cuesta, Teodoro
1880. Andalucía y Asturias. (A poetic duel between an Andaluz and an Asturiano). Mieres (Asturias).
Davenport, Charles B.
1932. The Genetical Factor in Endemic Goiter. Washington, D.C.: Carnegie Inst. of Washington.
DeLong, G. Robert, Jacob Robbins, and Peter G. Condliffe
1989. Iodine and the Brain. New York: Plenum.
Delor Castro, Ramon
1958. Patología Regional de Asturias. Oviedo: IDEA.
Del Rey Calero, J., et al.
1969a . Estudio del bocio endémico en la zona de la sierra de la provincia de Cádiz. Rev. San. Hig. Públ. 43:65–81.
1969b . Conocimiento. Acción y Política en medicina; conferencia dictada a los estudiantes de Medicina de Valladolid. Rev. San. Hig. Públ. 43:175–191.
1970. El test de Goodenough en escolares de diversas zonas de la provincia de Cádiz. Rev. San. Hig. Públ. 44:1235–1251.
DeMaeyer, E. M., F. W. Lowenstein, and C. H. Thilly
1979. The Control of Endemic Goitre. Geneva: WHO.
Douglass, William A.
1975. Echalar and Murelaga: Opportunity and Rural Exodux in Two Spanish Basque Villages. New York: St. Martin's Press.
Dunn, John T., and Geraldo A. Medeiros-Neto. eds.
1974. Endemic Goiter and Cretinism: Continuing Threats to World Health. Washington, D.C.: PAHO (Pan American Health Association).
Eggenberger, H.
1928. Five-Year Pilot Iodization in Appenzell. In: Schweizer Kropfkommission, Bericht über die International Kropfkonferenz in Bern. Aug. 24–26. Bern: Verlag Hans Huber.
Elorza, Antonio
1984. De una revolución lejana. El País Panorama Oct. 17:11.
El País
1981a . Denuncian el incumplimiento del Plan Preventivo de la Subnormalidad en Valencia. June 23.
1981b . La Sanidad, entre la autonomía y el centralismo. Dec. 16.
1981c . Plan Preventivo de la Subnormalidad. Dec. 26.
1981d . Tribunales: Querella por presunta negligencia en la aplicación del Plan de Prevención de la Subnormalidad. Dec. 26.
1982a . Nuevas autoridades sanitarias. Tribuna Libre, Pedro Azarco. 29 Jan.
1982b . La situación de la farmacovigilancia, en lo que a personal se refiere, es caótica. 5 Feb.
1982c . Pobreza de recursos para el control en España de los medicamentos. 2 May.
1984. El gasto español en medicamentos es el mas elevado de Europa. 11 Jun.
Endocrinología
1984. Eighteen full-page advertisements. 28(3).
1987. Director invitado Dr. Francisco Escubar del Rev: Bocio Endémico y Deficiencia de Yodo en España. Endocrinología (34), Suplemento 2, Julio. Barcelona: Ediciones Doyma.
Escobar del Rey, F.
1983. Untitled notes for a report to the European Thyroid Association.
1985. Goitre and Iodine Deficiency in Spain. The Lancet 1985: ii:149 (Lancet 1985:290–292).
1987. Director invitado: Bocio Endémico y Deficiencia de yodo en España. Endocrinología (34), Suplemento 2, Julio. Barcelona: Ediciones Doyma.
Escobar del Rey, F., et al.
1968. El bocio de la región de las Hurdes: Estudio preliminar. Rev. San. Hig. Públ. (52)311.
1972. El Bocio endémico de Las Hurdes: I. Incidencia del bocio en las poblaciones escolar y pre-escolar. Rev. Clin. Esp. 128:101–106.
1973. El Bocio endémico de Las Hurdes: II. Parámetros que indican la existencia de una deficiencia de iodo. Rev. Clin. Esp. 130:7–18.
1981a . A Survey of Schoolchildren from a Severe Endemic Goitre Area in Spain. Q. J. Med. 50 (198):233–246.
1981b . Protocolo para el estudio del bocio endémico. Endocrinología 28(2):43–48.
1984. Evolución de la endemia bociosa de Atienza (Guadalajara) tras la administración de Lipiodol. Endocrinología (31):97.
Espinós Gisbert, Domingo
1967. Discursos leído ante la Real Academia de Medicina de Valencia en la Recepción del Academico electo, el da 16 de mayo y contestación por el académico numerario Vicente Sanchis Bayarrí. Valencia: Papelería Vila.
Esteban Velasco, J., F. Morata García, R. J. de la Higuera, R. Ibáñez González
1962. Bocio endémico en la Alpujarra (Granada), estudiado con I 131. Rev. Clin. Esp. (84):170–179.
Fernandez, James W.
1976. La Poesía en Moción: Siendo Desplazado por Diversiones, por Burlas y por la Muerte en el País Asturiano. In: Temas de Anthropología Española, C. Lison Tolosana, ed. Pp. 131–157. Madrid: Akal.
1977. Poetry in Motion: Being Moved by Amusement, by Mockery and by Mortality in the Asturian Countryside. New Literary History (VIII):459–483.
1984a . "En torno a una vaca ratina: Metáforas vivas y la cultura que ello implica." Lletres Asturianes. Vol. 13:43–53. Oviedo.
1984b . Convivial Attitudes: The Ironic Play of Tropes in an International Kayak Festival in Northern Spain. In: Text, Play, and Story: The Construction and Reconstruction of Self and Society. 1983 Proceedings of the American Ethnological Society, Edward M. Bruner, ed. Pp. 199–229. Washington, D.C.: American Ethnological Society.
1985. "Campos Léxicos (Desplazamiento Semantico y Movimi-
ento Regionalista)." Lletres Asturianes 18, Boletin Oficial de l'Academia de la Llingua Asturiana, Principau d'Asturies. Oviedo. Pp. 55–69.
1986a . "Lo Común en la comunidad rural en Asturias: Diferencias de parecer, Divergencias de lectura," In: Culturas Populares: Diferencias, Divergencias, Conflictos. Coloquio Hispano-Francés 1984. Madrid: Casa de Velázquez. Pp. 185–195.
1986b . Persuasions and Performances: The Play of Tropes in Culture. Bloomington: University of Indiana.
1988a . The Call to the Commons: Decline and Recommitment in Asturias, Spain. In: The Question of the Commons: The Culture and Ecology of Communal Resources, Bonnie McCay and James M. Acheson, eds. Tucson: University of Arizona Press.
1988b . El dominio del tropo: Poesía popular y convivencia social, Gracián y Costa en el Campo. Anales de la Fundación Joaquín Costa . No. 5. Madrid. Pp. 21–35.
1988c . Andalusia on Our Minds: Two Contrasting Places in Spain as Seen in a Vernacular Poetic Duel of the Late 19th Century. Cultural Anthropology 3(1):21–35.
Fernandez, Renate Lellep
1979. The Decline of Breastfeeding: Interplay of Images and Policies. In: Breastfeeding and Food Policy in a Hungry World, Dana Raphael, ed. New York: Academic Press.
1980. La Lactancia materna: Progressión de imagenes en su desuso. In: La Antropología Médica en España, Michael Kenny y Jesús M. de Miguel, eds. Barcelona: Anagrama.
1986. Ethnography of Nutritional Deficiency in a Spanish Mountain Village: Analysis of Public Health's Delay in Preventing Iodine Deficiency Disorders (IDD). Ann Arbor: University Microfilms International.
1987a . Cheesemaking as a Living Cultural Resource in Covadonga National Park, Spain. In: Proceedings of First International Conference on Cultural Parks, held at Mesa Verde NP. Denver: National Park Service and the Colorado Historical Society. Pp. 335–341.
1987b . Children, Parents and Fieldwork: Reciprocal Impacts. In: Children in the Field: Anthropological Experiences, Joan Cassell, ed. Philadelphia: Temple University Press.
1987c . Reflections on the Fotonovela and Its Readers' Responses.
In: Latin American Masses and Minorities: Their Images and Realities, Dan C. Hazen, ed. Madison: University of Wisconsin Press, SLALAM.
1988. Biocultural Belief and Iodine Prophylaxis. Soc. Sci. and Med. 27 (6):587–596.
1989a . El método genealógico y el estudio de las enfermedades carenciales de yodo. JANO, Medicina y Humanidades (865):64–74.
1989b . Creencia biocultural y profilaxis con productos yodados. JANO, Medicina y Humanidades (865):84–87.
Fernandez, James W., and Renate L. Fernandez
1976. El Escenario de la Romería Asturiana. In: Expresiones Actuales de la Cultura del Pueblo, Anales de Moral Social y Economica. Madrid: Centro de Estudios Sociales del Valle de los Caídos.
1988. Under One Roof: Household Formation and Cultural Ideals in an Asturian Mountain Village. J. of Family History 13(1):123–142.
Fernández Alonso, Manuel, F. Tuero Bertrand, and J. L. Novalín
1978. Edad Moderna I. Volumen VII in the series Historia de Asturias. Gijón: Ayalga.
Fernández de Rota, José Antonio
1984. Antropología de un Viejo Paisaje Callego. Madrid: Siglo Veintiuno.
Fernández-Ruiz, César
1965. Historia Médica del Principado de Asturias. Oviedo: IDEA (Instituto de Estudios Asturianos).
Fernández-Tresguerres Velasco, Juan A.
1980. El Aziliense en las provincias de Asturias y Santander. Santander, Spain: Ministerio de Cultura.
Fierro-Benitez, Rodrigo, et al.
1968. Iodized Oil in the Prevention of Endemic Goiter and Associated Defects in the Andean Region of Ecuador: I. Program Design, Effects on Goiter Prevalence, Thyroid Function, and Iodine Excretion. II. Effects on Neuro-Motor Development and Somatic Growth in Children before Two Years. V. Effect on Intelligence of Iodine in Oil Administered to Young Andean Children: A Preliminary Report. In: Endemic Goiter, John B. Stanbury, ed. Washington, D.C.: PAHO. Pp. 306–396.
1973. Thyroid Cancer, Quervain's Thyroiditis and Hashimoto's
Disease in an Endemic Goiter Andean Area. In: Acta Endocrinological Supplementum 179:86–87.
Fisher, D. A.
1983. Thyroid Disorders. In: The Metabolic Basis of Inherited Disease. 5th ed. Pp. 231–269.
Fitzgerald, Thomas K., ed.
1987. Nutrition and Anthropology in Action. Assen, Netherlands: Van Gorcum.
Fox, Robin
1967. Kinship and Marriage: An Anthropological Perspective. Baltimore: Penguin Books.
1978. The Tory Islanders: A People of the Celtic Fringe. New York: Cambridge University Press.
Frontera-Izquierdo, P., et al.
1980a . Programas de despistaje neonatal del hipotiroidismo, editorial. An. Esp. Pediat. 13:104.
1980b . PKU and Neonatal Hypothyroidisim in Spain: Priority of Screening for Neonatal Hypothyroidism. Eur. J. Pediatrics 133:297.
Gaitán, E.
1984. Volatile Goitrogens in an Andean Population. In: Dunn and Medeiros-Neto 1974.
Gajdusek, D. C., and R. M. Garruto
1975. The Focus of Hyperendemic Goiter, Cretinism, and Associated Deaf-Mutism in Western New Guinea. In: Biosocial Interrelations in Population Adaptation, E. Watts, F. E. Johnston, and G. W. Lasker, eds. The Hague; Mouton. Pp. 267–285.
García Álvarez, Benjamín
1964. Concejos de Parroquias de Asturias. Lena, Spain: Gráfica Lena.
García Dory, Miguel Angel, and Silvio Martínez Vicente
1988. La ganadería en España: Desarrollo integrado o dependencia? Madrid: Ediciones Universitarios.
García Fernández, Jesús
1980. Sociedad y organización tradicional del espacio en Asturias. Gijón (Asturias):IDEA.
García Miñor, Antonio
1958. Epilogio. In: Patología Regional de Asturias. Delor Castro.
García Pérez, Manuel
1979. Encuesta sobre el bocio y otras enfermedades cronicas, Campo de Caso. (unpublished ms.)
1980. Proyecto sanitario para los pueblos del Alto Nalón. (unpublished ms.)
García Roél, Faustino
1980. La Pelagra en Asturias. Oviedo.
GEA
see Gran Enciclopedia Asturiana
Glick, Thomas
1976. On the Diffusion of a Medical Speciality: Marañón and the Crisis of Endocrinology in Spain. J. Hist. Biol. 9(2):287–300.
González García, Isabel
1972. La Economía Salinera en la Asturias Medieval. Oviedo: Asturiensia Medievalia, 1, Univ. de Oviedo.
González Villarón, L. F., et al.
1975a . El Bocio endémico en la provincia de Salamanca: I. Distribución geográfica y grado de incidencia. Rev. Clin. Esp. 136:227–233.
1975b . II. Estudio sobre factores etiológicos. Rev. Clin. Esp. 136:303–312.
1978. El bocio endémico en la provincia de Salamanca: III. Estudio de la triyodotironina, tiroxina y hormona tirotropa en los habitantes de la zona. Rev. Clin. Esp. 148:137–140.
Goody, Jack
1983. The Development of the Family and Marriage in Europe. New York: Cambridge University Press.
Goyanes Capdevilla, Jose
1932a . Del sentimiento cómico en la vida y en el arte: Ensayo estético-psicológico. Madrid: M. Aguilar.
1932b . Tipología de El Quijote: Ensayo sobre la estructura psicosomática de los personajes de la novela. Prólogo Marañón. Madrid.
Gran Enciclopedia Asturiana, La (GEA)
1970. Gijón, Spain.
Grande Covián, Francisco
1940. La secreción láctea durante la hipoalimentación. Rev. San. Hig. Públ.: 180–188.
1943. Dietas fisiológicas máxima y mínima en el régimen de alimentación del hombre adulto. Rev. San. Hig. Públ.
1975. Dietética y Nutrición. In: Historia Universal de la Medicina. Dirigida por Pedro Laín Entralgo. Tomo VII:248–251. Madrid: Salvat.
1988. Nutrición y salud. Madrid: Ediciones Temas de Hoy.
Grande Covián, F., and F. Jiménez García
1941. Tratamiento de la pelagra por el ácido nicotinico. Rev. San. Hig. Públ.: 49–81.
Greene, Lawrence S.
1973. Physical Growth and Development, Neurological Maturation and Behavioral Functioning in Two Ecuadorian Andean Communities in Which Goiter Is Endemic. Am. J. of Physical Anthropology 38(1):119–133.
1977a . Editor, Malnutrition, Behavior, and Social Organization. New York: Academic Press.
1977b . Hyperendemic Goiter, Cretinism, and Social Organization in Highland Ecuador. In: Malnutrition, Behavior, and Social Organization. New York: Academic Press. Pp. 55–93.
Greenwald, I.
1958. Notes on the History of Goiter in Spain and among the Jews. Bull. Hist. Med. 32:121–136.
Greenwood, Davydd J.
1977. Continuity in Change: Spanish Basque Ethnicity as a Historical Process. In: Ethnic Conflict in the Western World, Milton J. Esman, ed. Ithaca and London: Cornell University Press. Pp. 81–102.
Guerra, Francisco
1970. Medical Education in Iberoamerica, Iberian Roots. In: The History of Medical Education. UCLA Forum in Medical Sciences 12. Berkeley: University California Press. Pp. 419–453.
Harrison's (see Petersdorf)
Herr, Richard
1971. An Historical Essay on Modern Spain. Berkeley, Los Angeles, London: University of California Press.
Hetzel, Basil
1983. Iodine Deficiency Disorders (IDD) and Their Eradication. Lancet (Nov. 12):1126–1129.
1988. The Prevention and Control of Iodine Deficiency Disorders (with discussion by F. Delange, J. B. Stanbury, and F. E. Vitri and introduction by M. Lotfi and J. B. Mason). United Nations, Administrative Committee on Coordination—Subcommittee on Nutrition. ACC/SCN State-of-the-Art Series, Nutrition Policy Discussion, Paper No. 3.
1989. The Story of Iodine Deficiency: An International Challenge in Nutrition. Oxford: Oxford University Press.
Hetzel, Basil S., John T. Dunn, and John B. Stanbury, eds.
1987. The Prevention and Control of Iodine Deficiency Disorders. Amsterdam, New York, Oxford: Elsevier.
Hetzel, B. S., and B. J. Potter
1984. Iodine Deficiency and the Role of Thyroid Hormones in Brain Development. In: Neurobiology of the Trace Elements, I. E. Dreosti and R. M. Smith, eds. Clifton, N.J.: Humana Press.
Hunziker, Dr. med. Heinrich
1924. Die Prophylaxe der groszen Schilddruse, gleichzeitig ein Stück vergleichende Kliimatologie der Schweiz und ein Leitfaden fur systematische naturwissenschaftliche Forschunger, Mit enimen Beitrag von Dr. med. Hans Eggenberger. Bern: Verlag Enrst Bircher.
Hygeia
1926–1935. Survey of articles, brief reports, and letters related to goiter and its prophylaxis: 1926:173; 1928:595–596, 598; 1929:830; 1930: 574, 857; 1932:118–120; 1933:1011–1014, 1037; 1934: 572; 1935:722–735, 874–877, 1114–1116.
Ibáñez González, R., A. Guiraun, F. Escobar del Rey, F. Morata Garcia, and E. Ortiz de Landázuri
1956. Resultados obtenidos con la profilaxis de sal completa en el bocio endémico. Rev. Clin. Esp. (61):285–290.
Ibáñez González, R., F. Morata Garcia, F. Rodríguez Moreno, and E. Ortiz de Landázuri
1959. Resultados obtenidos en el profilaxis del bocio endémico en la Alpujarra (Granada). Rev. San. Hig. Públ. (33):157–170.
International Classification of Diseases (ICD)
1979. ICD.9.CM. Vol. 1, Diseases Tabular List. Ann Arbor: Commission of Professional and Hospital Activities.
Jackson, Gabriel
1984. "Datos para comprender el octubre de '34." El País (Oct. 23):11.
Jove y Canella, José María
1923. Topografía médica del concejo de San Martin del Rey Aurelio. Madrid: Imprenta de la Ciudad Lineal.
1932. Topografía médica del término municipal de Sobrescobio. Madrid.
Junceda, Eladio
1936. Topografía médica del concejo de Navia. Madrid: Imprenta de J. Cosano.
Kelly, F. C., and W. W. Snedden
1960. Endemic Goitre, WHO Monograph Series, No. 44. Geneva: WHO.
Kleinman, Arthur
1980. Patients and Healers in the Context of Culture: An Exploration of the Borderland between Anthropology, Medicine, and Psychiatry. Berkeley, Los Angeles, London: University of California Press.
Kleinman, Arthur, and Byron Good, eds.
1985. Culture and Depression. Berkeley, Los Angeles, London: University of California Press.
Knowler, William C., et al.
1981. Diabetes Incidence in Pima Indians: Contributions of Obesity and Parental Diabetes. American J. of Epidemiology 113(2):144ff.
1983. Diabetes Mellitus in the Pima Indians: Genetic and Evolutionary Considerations. American J. of Physical Anthropology 62:107–114.
Konner, Melvin
1982. The Tangled Wing. New York: Holt, Rinehart and Winston.
Koshland, Daniel
1987. "Immortality and Risk Assessment." Science, Apr. 17, vol. 236, no. 4799, p. 241.
Kranzler, Henry R., and Andrew P. Vayda
1977. Disruption of Iodine Supply as a Result of Development: Endemic Goiter and Cretinism. In: Glimpses of Ecology, J. S. Singh and B. Goapl, eds. Jaipur: International Scientific Publ. Pp. 511–518.
Krenning, E. P., and G. Hennemann
1983. Strategy in Thyroid Evaluation. In: Thyroid Diseases, World Federation of Nuclear Medicine and Biology, Christian Beckers, ed. New York: Pergamon Press. Pp. 107–111.
Kruger, F., and W. Ebeling
1922. La Castaña en el nord-oeste de la Península Ibérica. Estudio etnográfico-linguístico. Anales del Instituto de Linguística. Universidad de Cuyo, Mendoza (Argentina).
Laderman, Carol
1984. Wives and Midwives: Childbirth and Nutrition in Rural Malaysia. Berkeley, Los Angeles, London: University of California Press.
Laforet, Carmen
1944. Nada. Barcelona: Ediciones Destino.
Laher Montoya, Elena
n.d. Extracto de la tesis doctoral: Problemas médico-sociales de las tiroidopatias, un estudio en la Seguridad Social. Dir., Prof. G. Piedrola Gil, Departamento de Medicina Preventiva, Universidad de Madrid. Unpublished. (Extract found in the medical library of the Universidad Complutense in Madrid. Author's references suggest the date must be 1973 or later.)
Laín Entralgo, Pedro
1964. Marañón y el Enfermo. Revista de Occidente (then an irregular publication, the year's entire issue.)
Lancet, The
1979. Endemic Goiter and Cretinism, editorial (Dec. 1:1165–1166).
1983. Editorial. Pp. 1121–1122.
La Nueva España
1984. Salud, Lo que Vd. debe saber de Bocio y Tiroides. 27 May.
Lewellen, T. C.
1981. Aggression and Hypoglycemia in the Andes: Another Look at the Evidence, with CA comment. Current Anthropology 22(4):347–363.
Linazasoro, J. M., et al.
1970. Walnut and Its Action on Thyroxene Excretion. Endocrinology 86:696–700.
Lindenbaum, Shirley
1979. Kuru Sorcery, Disease, and Danger in the New Guinea Highland. Palo Alto: Mayfield Publ. Company.
Lisón Tolosana, Carmelo
1971. Antropología Cultural de Galicia. Madrid: Siglo Veintiuno.
Marañón, Gregorio
1921. El Problema de las Hurdes. El Liberal, Madrid. 27 August. Reprinted in Obras Completas, Tomo IV:55–57.
1927. Bocio y Cretinismo: Estudio sobre la epidemia española y la patogenia de esta enfermedad. Madrid: Editorial Paez.
1928a . Resumé de l'etat actuel du probleme du goitre endemique en Espagne. In: Schweizer Kropfkommission. Pp. 389–401.
1928b . El bocio en España y sus condiciones patogénicas. Anales Acad. Med. Quir. Esp. (15):1–86.
1929. The Climacteric (The Critical Age). Translation by K. S.
Stevens from the original in Spanish published in 1919. St. Louis: C. V. Mosby.
1936. El Conde-Duque de Olivares: La pasión de mandar. Madrid: Espasa-Calpa.
1943. Don Juan: Ensayos sobre el origén de su leyenda. Madrid: Espasa-Calpe.
1972. Obras Completas. Tomos I–VII. Introducción por Pedro Laín Entralgo.
Marañón, Gregorio, and Alfonso Balcells
1984. Manual Diagnóstico Etiólogico, 13th ed. Madrid: Espasa-Calpe.
Marañón, Gregorio, and E. Carrasco Cadenas
1923. Sobre el valor clínico de la determinación del metabolismo basal. Arch. Med. Gral. y Espec. (12):117.
Marino Aguiar, Manuel
1967. Aplicación de un micrométodo rápido a la determinación del contenido en yodo de las aguas potables. Rev. San. Hig. Públ.: 343–355.
Martin, Cal
1978. Keepers of the Game. Berkeley, Los Angeles, London: University of California Press.
Martínez Fernández, Jesus, and J. Manuel Junceda Avello
1969. Ensayo biológico sobre los hombres y los pueblos de la Asturias primitiva. Oviedo: IDEA.
Matovinovic, Josip
1983. Endemic Goiter and Cretenism at the Dawn of the Third Millennium. Annual Review of Nutrition (3):341–412.
Maud, J. M.
1896. Disliked Peoples of Europe. London.
Mead, Margaret
1977. Contemporary Implications of the State of the Art. In: Malnutrition, Behavior and Social Organization, Lawrence Greene, ed. Pp. 259–266.
Medio, Dolores
1953. Nosotros los Ribero. Barcelona: Ediciones Destino
Medvei, Victor Cornelius
1982. A History of Endocrinology. Boston: MTP Press.
Menéndez Pidal, Ramon
1950. Orígenes del español. Madrid: Espase-Calpa.
1962. El dialecto leonés. Oviedo: IDEA.
Menéndez Torre, E. L., J. Aranda Regules, F. Díaz Cadórniga, P. Boix Pallares, J. Aller Granda, and A. Rabal Artal
1986. Estudio epidemiológico del bocio endémico en la población infantil asturiana. Endocrinología 1(33):16.
The Merck Manual
1982. Thyroid, Thyroid Hormone Formation. In: The Manual of Diagnosis and Therapy. Rahway N. J.: Merck.
Merke, F. Prof. Dr. Med. (Basel)
1971. Geschichte und Ikonographi des endemischen Kropfes und Kretinismus. Bern: Verlag Hans Huber.
1984. History and Iconography of Endemic Goitre and Cretinism. Berne: Hans Huber.
Mertz, Walter
1981. The Essential Trace Elements. Science 213:1332–1338.
Messer, Ellen
1984. Anthropological Perspectives on Diet. Ann. Rev. Anthrop. 3:205–249.
Michel, Francois
1847. Histoires des races maudites de la France et de l'Espagne. Paris: Ed. A. Franck.
de Miguel, Jesús
1976. Health in the Mediterranean Region, Vols. 1 and 2. Ann Arbor: University Microfilms.
1977. The Role of the Medical Profession in a Non-Democratic Country: The Case of Spain. In: Health and the Division of Labour, Margaret Stacey, ed. New York: Prodist
1979. La Sociedad enferma: Las bases sociales de la política sanitaria española. Madrid: Akal.
Ministerio de Hacienda
1972. Las Salinas de Torrevieja y la Mata Dirección General del Patrimonio del Estado, Nueva Compañía Arrendataria de las Salinas de Torrevieja, S.A. (in-house publication)
Mintz, Jerome
1982. The Anarchists of Casas Viejas. Chicago: University of Chicago Press.
Montagu, Ashley
1972. Sociogenic Brain Damage. American Anthropologist 74(4): 1045–1061.
Morreale de Castro, G., F. Escobar del Rey, R. J. Mora Lara, E. Ortiz de Landázuri
1953. Bases científicas que aconsejan el empleo de la sal iodada en la profilaxis del bocio endémico. Rev. Clin. Esp. (50): 285–289.
Morata-García, F., and J. Esteban Velasco
1962. Profilaxis con sal iodada: Efectos de su supresión en una localidad endémica. Rev. San. Hig. Públ.: 599–604.
Moroni, A.
1961. "Sources, Reliability and Usefulness of Consanguinity Data with Special Reference to Catholic Records." World Health Organization Chronical (15):465–172.
1969. Historical Demography, Human Ecology, and Consanguinity. International Union for the Scientific Study of Population.
Muñoz Rodríguez, M.
1963. Bocio endémico en reclutas. Rev. San. Hig. Públ.: 41–52.
National Academy of Sciences, Committe on Food and Nutrition
1970. Iodine Nutriture in the U.S. Summary of a Conference Oct. 31, 1970.
Neira, Jesús, and Ma. Rosario Piñeiro
1989. Diccionario de los Bables de Asturias. Oviedo: IDEA.
Netter, Frank
1965. Endocrine System and Selected Metabolic Diseases. New York: CIBA.
Netting, Robert
1981. Balancing on an Alp: Ecological Change and Continuity in a Swiss Mountain Community. New York: Cambridge University Press.
Novo Mier, Lorenzo
1979. Dicionariu Xeneral de la Llingua Asturiana. Oviedo: Asturlibros.
O'Neill, Brian Juan
1987. Social Inequality in a Portuguese Hamlet: Land, Late Marriage, and Bastardy, 1870–1978. New York: Cambridge University Press.
Ortiz de Landázuri, E. et al.
1959. Resultados obtenidos con la profilaxis del bocio endémico (Alpujarra-Granada). Rev. de Med. EG Navarra III:24–31.
Ott, Sandra
1981. The Circle of Mountains. Oxford: Oxford University Press.
Padrones de distinción de estado
n.d. Cangas de Narcea (Asturias).
Palacios Mateos, J. M., and F. Ramos Duce
1965. Contenido en 1–5 vinil 2 toxicohidrina (Goitrina) en las hojas de nabiza (Grelos). Rev. Clin. Esp. (98):382–384.
1972. El Programa Español de Educación en Alimentación y Nutricion. Rev. San. Hig. Públ.: 1125–1135.
Peraita, Manuel
1940. Sobre el tratamiento por el ácido nicotínico de los síntomas nerviosos y metales de los pelagrosos. Rev. San. Hig. Públ.: 482–503.
Petersdorf, R. G., et al.
1983. Harrison's Principles of Internal Medicine. 10th ed. New York: McGraw Hill. Prensa Médica-Mexicana publishes it as Principios de Medicina Interna .
Piedrola Gil, G.
1970. Medicina preventiva y social. Madrid: AMARD ediciones.
Piedrola Gil, G., and P. Trincado Dopereiro
1982. Bocio endémico como enfermedad social, su prevencion. In: Medicina Preventiva y Social, Higiene y Sanidad Ambiental. Madrid: AMARD. Pp. 367–374.
Pitt-Rivers, Rosalind
1961. Advances in Thyroid Research, Transaction of the Fourth International Goitre Conference, London, July 1960. New York: Pergamon Press.
Plummer, William A.
1936. The Quest for Iodine. Hygeia (June 1936):527–571.
Prieto Bances, Ramón
1976. Obra escrita. 2 vols. Oviedo: Universidad de Oviedo.
Quiroga, Elena
1952. La Sangre. Barcelona: Ediciones Destino.
1973. Viento del Norte. Barcelona: Ediciones Destino.
Ráfols, José María
1956. La preparación de la sal completa. Rev. Clin. Esp. (60):285.
Redondo Pizarro, F.
1969. Alimentación y salud. Rev. San. Hig. Públ: 503–515.
Región, La
1982. Asturias es una de las regiones con la tasa de enfermos de bocio mas alta de España. 12 Nov.
Revista de Endocrinología
1987. Bocio endémico y Deficit de Yodo en España. Director invitado: F. Escobar del Rey. Vol. 34, suplemento 2, Julio 1987. Barcelona: Doyma.
Revista de Sanidad e Higiene Pubica (Rev. San. Hig. Públ.)
1938. Número extraordinario.
1942. Comisión Central de Censura Sanitaria: Normas aprobadas.
1951. Editorial: España en la OMS. P. 359.
1953. Editorial: Los hospitales y la medicine preventiva. P. 506.
1961. Review of Clements's Endemic Goiter . Rev. San. Hig. Públ.: 480.
de Roches, V.
1976. Les pariáh de la France et l'Espagne. Paris: Hachette.
Rodríguez Cuartero, A.
1976. Bocios intratorácicos. Rev. Clin. Esp. 142:337–341.
Roe, Daphne
1973. A Plague of Corn: The Social History of Pellagra. Ithaca: Cornell University Press.
Ruiz de la Peña, Ignacio
1970. Asturias en la Alta Edad Media. GEA (vol. 2):105–109.
Salter, William Thomas
1940. The Endocrine Function of Iodine. Cambridge: Harvard University Press.
Sánchez-Franco, F., et al.
1974. Influence of Sex Phase of Menstrual Cycle on Thyrotropin, TSH Response to TRH. Dept. de Endocrinología Experimental, Instituto G. Marañón, CSIC. Rev. Clin. Esp. (136):736.
Sánchez-Franco, F., L. Cacicedo, G. Morreale de Escobar, and F. Escobar del Rey
1983. Nutrition and iodine versus genetic factors in endemic goiter. J. Endocrinol. Invest. (6):185–187.
Sánchez Guijo, F.
1975. Aspectos inmunológicos en una población con bocio y cretinismo endémicos. Rev. Clin. Esp. 139:509–512.
Sánchez-Martín, J. A., and J. M. Linazasoro
1969. Efecto bociógeno de distintas semillas vegetales y su acción sobre la excreción de la tiroxina. In: Conference Proceedings: III. Reunión Asoc. Europ. Tiroides, Athens.
Schweizer Kropfkommission
1928. Bericht über die Internationale Kropfkonferenz in Bern 24–26 August 1927. Berne: Verlag Hans Huber.
Scheper-Hughes, Nancy
1979. Saints, Scholars, and Schizophrenics: Mental Illness in Rural Ireland. Berkeley, Los Angeles, London: University of California Press.
Servicio Topográfico
n.d. Hacienda, Oviedo.
Shapiro, Martin F.
1982. Medical Aid to the Spanish Republic during the Civil War (1936–1939). Annals of Internal Medicine 97:119–124.
Shilts, Randy
1988. And the Band Played On. New York: Penguin.
Silberschmid, W.
1928. Schlusswort. In: Schweizer Kropfkommission.
Stanbury, John B., ed.
1969. Endemic Goiter. Report of the Meeting of the PAHO Group on Research in Endemic Goiter held in Puebla, Mexico, 27–29 June 1968. Washington, D.C.: PAHO.
1978. Familial Goiter. Chap. 10 in: The Metabolic Basis of Inherited Disease, 4th ed., Stanbury, Wyngaarden, and Fredrickson, eds. Pp. 206–239.
Stanbury, J. B., and B. S. Hetzel
1980. Endemic Goiter and Endemic Cretinism: Iodine Nutrition in Health and Disease. New York: Wiley.
Suárez-Lledó, J.
1962. Nuestra experiencia en el tratamiento del hipertiroidismo y cancer de tiroides con iodo radiactivo. Rev Ibérica de Endocrinología X(49):7–16.
1970. Bocio s.v. in GEA. Gijón.
Sydenstrecker, Virgil
1958. The History of Pellagra: Its Recognition as a Disorder of Nutrition and Its Conquest. American J. Clinical Nutrition 6:409–414.
Tax Freeman, Susan
1979. The Pasiegos. Chicago: University of Chicago Press.
Tepperman, Jay
1980. Metabolic and Endocrine Physiology. Chicago: Yearbook Medical Publishers.
Thompson, James W., and Margaret W. Thompson
1980. Genetics and Medicine, 3d ed. Philadelphia: W. B. Saunders.
Todorov, Tzvetan
1987. The Conquest of America: The Question of the Other. New York: Harper and Row.
Torres, Eduardo S.
1925. Estudios sobre el bocio. Gijón: Publicaciones La Industria.
Tribuna Médica
1982. Campaña de Erradicación del Bocio (Galicia) 5 Feb.
1982. En Un Año El Centro de Diagnóstico de Alteraciones Metabólicas Detectó 18 Casos. 5 Feb.
Tuero Bertrand, Francisco
1970. Ordenanzas Rurales. GEA s.v. ordenanzas.
1974. Ordenanzas Rurales. Oviedo.
Tuero Bertrand, Francisco, and Gonzalo Anes
1978. Edad Modern II. El Antiguo Régimen: Economía y socie-
dad. Volume VIII in series Historia de Asturias. Gijón: Ayalga.
Uría, Jorge
1984. Cultura oficial e ideología en la asturias franquista: El IDEA. Ethos 12. Oviedo: Universidad de Oviedo.
Utiger, Robert D.
1979. Hypothyroidism. Chap. 33 in: Endocrinology, Leslie V. DeGroot, ed. Vol. 1. San Francisco: Grune and Stratton.
Vademecum Internacional de Especialidades Farmaceúticas y Biológicas n.d. Annual. Madrid: Editorial Daimon-Vademecum.
Vayda, Andrew P.
1979. Review of Malnutrition, Behavior and Social Organization, Lawrence Greene, ed. Human Ecology 7(4):371–373.
de la Vega, Jimena
1935. La Herencia fisìopatológica. Madrid: Espasa-Calpe.
de la Vega, Leandro
1964. Las Hurdes, leyenda y verdad. Madrid: SIE.
Vidal Jordana, J.
1924. La profilaxis del bocio endémico por el yodo y su aplicación en Las Hurdes. Arch. Esp. Endocrinol. y Nutr. (1):69–71.
1927. El bocio endémico en Las Hurdes. Arch. Esp. Endocrinol. y Nutr. (5):245–266.
Vilar Ferrán
1921. Topografía médica de Cabrales. Madrid.
Villaraín y Fernáandez, José
1923. Topografía médica del concejo de Illas. Madrid.
Vivanco, F., J. M. Palacios, F. Ramos, M. A. Busturia, and A. Muro
1972. El Bocio endémico en España, estudio de la correlación entre incidencia de bocio y contenido en iodo de las aguas de bebida. Instituto Nacional de Nutricíon. Rev. Clin. Esp. 123:425–432.
Voz de Asturias
1984. Sanidad infantil: Aún mucho por hacer en nuestra región. 30 Aug.
Voz de Galicia
1984. La Xunta ultima el programa de la lucha contra el bocio. 30 Jun.
1984. Las grandes cadenas de alimentación colaboraran en el programa contra el bocio endémico. 30 Oct.
1985. La educación sanitaria y el uso de sal yodada, bases del plan de erradicación del bocio endémico. 19 Jan.
1985. La Xunta de Galicia le declara la guerra al bocio. 27 Mar.
Warren, Kenneth S., and A. F. Mahmoud Adel
1984. Tropical and Geographical Medicine. New York: McGraw-Hill.
Zurita Juárez, Ma. Cruz
1958. Aprovechamiento de glándulas endocrinas con destino a la industria opoterápica. Rev. San. Hig. Públ.: 623–647.
Index
A
Advertising, 29 , 164 , 168 , 180 -181, 200 n. 9
Agriculture, 57 -60, 107 -119
crops, 41 , 55 , 109 , 115
dairy, 63
pastoralism, 94
potato, 58
sharecropping, 54
transhumance, 53
Anales Españolas de Pediatria, 175
Anthropology, 6 -9, 12 , 44 , 152 , 157
fieldwork of, xi , 86 -88
and genealogies, 81
and "heredity," 67
holistic, 11
and incidentalist approach to IDD, 6
as nutritional ethnography, 65
"proper focus" of, 8 -9
Aranda, R. J. and F. Díaz Cadórniga, 177 , 179
Aranda Regules, R. J., 16 , 45 , 154 , 168 , 177 , 179 , 181
Asturianistas, 51 , 142
Asturias: abandonist view of, 52
alcoholism in, 63
and austerity, 63 -64
and autarchy, 53 , 61 -63
black lung, 127
black-marketeering in, 45 , 62
colonization of, 49
Consejería de Sanidad, 179 , 181
Covadonga, 51
defamatory images of, 17 , 47 -50
dependency upon world market, 63
estimated cost of goiterectomies in, 194 , 223 n. 9
and "fat cows," 60 -61
languages of, 50 -51
physical description of, 46 -47
as region of hidalgos,52
Authoritarian governments and prophylaxis, 192
Autonomía and shift in health administration, 174 , 181
B
Barriers to scientific communication, 171
Basal metabolic rate as "armament," 163
Basedow, 30
Biochemical and symbolic systems, linked, 119
Biochemical data, "appropriateness" of, 178
Biomedicine, villagers' (putative) rejection of, 17
Blood: as "bad," 96 , 206 n. 38
intermingled, 81 , 209 n. 20
as reproductive capacity, 138 -139
Bocio (goiter), etymology of, 125
Bottom line, view from, 182 -183
Brain function and IDD, 31 , 38 , 39
Bread, 49
as food and blessing (pan bendito ), 60 , 206 n. 37
"official," 62
Breeding isolate, 105
Buchbinder, Georgeda, 6 , 26
Bulletin of the History of Medicine,173
Buñuel, Luis, 145 , 157
Burden of dependency, 92 -99
Butter, as social medium, 140 -141, 216 n. 25
C
Campaign to eradicate IDD, 13 , 34 -35, 177 -178
poster for, 164
Caricature, 43 , 45 , 88 , 101 , 124 , 140
buffoons and idiots, 88
Carrasco Cadenas, E., xi , xii , 157 , 159 , 162 , 166 , 171 , 187
Carting our worthless men off to France, 136 -137, 142 -143
Casal, Gaspar, 56 , 157 -158
Case history, 3
as ethnography, 17
Cátedra, María, 113
See also "Despised peoples"
Causation, 18 , 67 , 104 -105
Censorship, 62 , 166 -169, 172 -173, 180
Census, 12
Centro de Studios de Endocrinología Experimental, 148 .
See also Instituto Marañón
Chestnut, dietary importance of, 113 -119
Classificatory schemes, 37 , 152 -153, 179
Class interest, 8 , 188
Clements, F. W., 17 , 46 , 173 , 176
Colegio Oficial de Médicos, 149 , 166 , 178
Collectivist action, 165 -166
Collegial persuasion, 159 , 163
Congenital hypothyroidism (CH), 38 , 39 , 178
false negative, 175 -176
Connolly, Kevin J., Peter O. D. Pharoah, and Basil S. Hetzel, 31
Consanguinity, 17 -18, 75 -80
mercenary fosterage as "confounding variable," 156
Consejo Superior de Investigaciones Cientificas (SCIC), xii , 148 , 153
Conspiracy of silence, 186
Cosmetic surgery, 137 , 167
Cost of IDD, estimate of, 193 -194
Cousins, 69 , 72
doubly-over, 207 n. 4
Cretinism, 27 -28, 37 -39, 161
sporadic, 38
Cretins, village of, and Marañón, 156
D
Davenport, Charles B., 218 n. 29
Deaf-mutism, 129 -130, 161 , 162
Penred's syndrome, 215 n. 7
School for Deaf, 214 n. 7
and tolerance of isolation, 94
Degeneration and demystification, 51
Delong, G. Robert, Jacob Robbins, and Peter G. Condliffe, 31
Delor Castro, Ramón, 171 , 183 , 176
DeMaeyer, E. M., F. W. Lowenstein, and C. H. Thilly, 14 , 144 , 178 , 181
Democracy and prophylaxis, 192
"Despised peoples," 53 , 118 -119, 140
and spurious ethnicity, 132 , 213 n. 15
Dialect. See Language
Díaz Cadórniga, F., xii , 177 , 179 , 182
Diet: corn based, 55
dual, 25 , 53 , 143
effect of U.S. trade on Spanish, 63
and industrialization, 57
and land typology, 107
and pilgrimage, 53
proto-historic, 48
Dietary: policies, France, 57
revolution, 63
status, 112
Dietary stress and defamatory images, 48 -50
Diiodotyrosene, 183
Disease, problems in classification of, 23 , 37 -38
Disinformation, medical, xi , 172
DNA and "blood," 81
Dose: pharmacological vs. physiological, 30 , 168 , 230
problems of control, 162 , 168
of trace element, 23
Dose response curve, 22 , 26 , 168
Douglass, William, 113
Drinking water, 47 , 151 , 170 , 218 n. 28
and iodine status, 25
Dunn, John T., 17
Dunn, John T., and Geraldo A. Medeiros-Neto, 14 -15, 176
Dwarfism, 145 -146, 156 , 217 n. 15
E
Earth without Bread (film), 146 -147
Economy and IDD, 7 , 44 , 58 , 104 , 106 , 139 , 147 , 155 -156, 161
Egalitarian ethic, 106 , 122 -123
Endemia, 14 -15
recognition of, 177
unacknowledged, 13
Endocrine base of disposition, 158 , 218 n. 30
Endocrinología,148 , 173 , 182 -183
Endocrinology, 153
introduction into Spain, 4
prophylactic, 158
tradition of investigative, 170
ENDOFREN, 183 -184
"Enemies of prophylaxis," 163
Enzyme defect, 37
Epidemiology and anthropology, compared, 14
Escobar del Rey, Francisco, xii , 31 , 148 , 154 , 169 , 174
Escobines, 3 , 41 -46
demography, 75 -82, 206 n. 39
goitrousness in, 78
goiterectomies in, 194
La Pista, 77
wealth distribution in, 123
Essentialness of nutritional microelements, 21 -24
Estrogen and IDD, 30 -31
Ethnicity: as "character," 124
as spurious, 118 -119, 131 -132, 191
as sum of immutable individual dispositions, 152
Euphemisms of affliction, 127
European Community (EC), 47 , 202 n. 7
European Thyroid Association, 148
F
Falange and collective action, 219 n. 37
FDA (U.S.), 183
Feeding program, 148 , 178
Female hormones and IDD, 15
Females and cretinism, 201 n. 10
Fernández García, Joaquin, xii , 210 n. 32
Fernández-Ruiz, Cesar, 80 , 151 , 152 , 172
Fetal wastage, 163 , 175
Fierro-Benitez, Rodrigo, 7 , 38
Folklore: and epidemiology, 124 -125, 142 -143
and idiom of affliction, 131 -132
and regionalism, 200 n. 49
Folklore, ethno-medical or dietary, 24 , 73 , 113 , 116 -117, 125 , 207 n. 8, 212 n. 9, 213 n. 13, 214 n. 1, 215 n. 11
as poetic duel, 214 n. 1
Folklore, general, 207 -208 n. 8, 209 nn. 19, 22, 214 n. 3, 215 n. 11, 220 n. 49
Folk remedy for IDD, 24
ocle as, 200 n. 3
Food: chain and IDD, 24 , 25 , 48
as class marker, 118 , 213 n. 16
code, 180
goitrogenous, 32 -34
and nutritional profile, 55 , 59 -60
policy, 57 , 63 -64
Food supply: delocalization of, 45 , 59 , 73
relocalization of, 61
Fox, Robin, and "messy genealogical gossip," 81 , 207 n. 7
Franco and Marañón, 4 , 10 , 121 , 219 n. 32
Frontera-Izquierdo, 175
G
García Álvarez, Benjamin, 109 , 113
García Comas, Enrique, 165
García Pérez, Manuel, xii , 177 -178
Genealogical collapse, 207 n. 7
Genealogical method, 12 , 86 , 89 -92, 191
Gender and IDD, 119 , 128 , 137 , 139 , 214 n. 6
Genotype, 88 , 92 , 100
Geology and IDD, 6 , 47
Glandular determinism, 58 -59, 218 n. 30
Glick, Thomas, 4 , 153 , 159 , 171
"God's preferred children," 148
Goiter: as adaptation and "woman's problem," 30 , 119 , 139
as "attractive," 80 ;
belt in U.S., 24
cosmetic surgery and, 167
grades of, 12 , 15
multiple causation of, 160
recent eruption in U.S., 26
as "regional disease," 171
as social disease, 11
timing of emergence of, 119
Goiter Commission, Spain, 146 , 154
Goiter, excision of (goiterectomy), 13 , 87 , 99
number of, 187
and replacement hormone, 36
Goitrogens and IDD, 17 , 32 -35, 170
Government and iodization, 26
"Grand detour" (Ein grosser Umweg ), 4 , 153 -159
Grande Covián, Francisco, 61 , 64 , 178
Grande Covián, Francisco, and F. Jiménez García, 62 , 166
Grandparents, expanding number of, 74
Greene, Lawrence, 7 , 31 , 143
Greenwald, I., 173 , 185
Groundwater: as goitrogenic, 33
iodine content of, 170
Guerra, Francisco, 160
Guide Michelin,147
H
Hacienda, 112 , 211 -212 n. 7
Health, wealth, and love, 73 -75
Health care and prevention, rising demand for, 165 , 179 , 188
Herbalists, 168
Heredity and IDD. See Metabolic error
Heredity as explanation, 66 , 149 , 151 -152, 161
Heterogenetic monogamy, 105
Hetzel, Basil, 2 , 5 , 38
Hidalgo, inversion of meaning in Asturias, 52 , 203 n. 17
Hippocratic Oath, 160 , 165
Homeostasis, corporeal vs. cerebral, 22 , 29 , 31
Hormone replacement after goiterectomy, 36 , 38 , 95
Households, distribution of, 75
"Hungry foods," 32
Hunters and foragers, 48
Hunziker, Heinrich, 4 , 156
Hyperthyroidism, 36 -37, 87 , 98 -99
Hypothyroidism, 17 , 35 -36, 87 , 98 -99, 176
and lethargy, 8
I
IDD: as accentuating social stratification, 106
and anthropology, 6
cost to state, 187
incidence of, 37
psychological toll of, 95 , 124
recent eruption of, 6 , 7
wide spectrum of affliction, 163
"Idiocy of rural life," 40
Idiom of affliction and folklore, 131
Ignorance, institutionalization of, 10 , 18 , 188
Imagery: of exoneration and blame, 129
of relationships and intermingled blood, 81
Images: as distancing device, 135
external influences upon, 63 -64
flow of, 185
women's, 81 -82, 209 n. 1
Image(s), defamatory, 55 , 56
of Asturians as barbarians, 49
of deaf-mutes, 130
of pellagra, 152
of speechway, 50
Inaction, logic of, 18 , 141
uncertain costs of, 6
Inbreeding, 33 -34
and supplementation, 66
Incest, diagram of, 84
Indicators of IDD: "anthropological
traits," 22
biochemical and ethnographic, 16
drinking water, 25
folklore, 18
Individual prophylaxis in an anticollective context, 168 -169
Infant formula, 45 , 64
Information, blocked flow of, 185
Inheritance, partible, 68 -73
Innate disposition and endocrine base, 158
Instituto de Estudios Asturianos (IDEA), 171
Instituto Marañón, 140 , 153 , 158
International Conference on Goiter and Cretinism: First, 4
Second, 157 , 160
International Guide to Pharmaceutical Products, 183
International Thyroid Conference, 64
Iodine, 20 -40
abuse of, 155
adventitous, 25 , 200 n. 5
atmospheric transport of, 24
bound by estrogen, 15
as essential, 21 -24
intake assumed optimal, 20
as precipitating toxicosis, 29 -30
in rock salt, 7
in solution, 168
as "too specific a remedy," 156 , 169 -170
Iodine deficiency: as contributing factor in mental retardation, 174
as permissive, 100
at risk at global scale, 2
at risk in Spain, 1
WHO definition of, 27
Iodization: by commercial route, 26 -27
experimental, 146
Iodized oil injection (Lipiodol), 67 , 179 , 181 -182, 201 n. 16
K
Karst, 46 -47
Kelly, F. C. and W. W. Snedden, 173 , 176
Kinship: as compromise, 66 -73
embarrassment about, 72
image of, 82
and inbreeding, 17
model of "ideal," 67
Knowledge: dissemination of, 4 , 18 , 169
flow, 192
forfeited, 105
misapplication of, 2
popular, 4
Kuru, as social disease, 11
L
Labor, agricultural, and retardation, 94 -95, 128
Land: access to fruits of, 106 -107
fragmentation, 54 , 68
yield/cost ratio, 58
Landlessness and IDD, 18
foraging, 109
Landscape, dietary, 107 -111
Language: Asturiano, 139 , 168
as "deformed," 51
dialect, 17
"dignity of," 167
restricted code, 131 -132
Lindenbaum, Shirley, 11
Lugol's solution, 168 -169
M
Marañón, Gregorio (1887-1960), 4 -5, 146 , 153 -159, 185
and memory for clinical detail, 157 , 219 n. 31
persona(s) of, 155 -157
Marañón, Gregorio y Alfonso Balcells, 30 , 153
Marañón, Gregorio y E. Carrasco Cadenas, 163
Marques de Ensenada, 216 n. 25
Marriage and the ecclesiastical vs. material imperatives, 68 -73
Marriage of convenience, 86 , 92 , 104
Materialist: explanation, 137
hypothesis tested, 121 -122
perspective, 106
Matovinovic, Josip, 5 , 22 , 27
"Me, I'm marrying for love," 92
Mead, Margaret, 8 -9
Medical and dietary observations on selected individuals, 98 -100
Medical mischief, unrefuted, 173 -174
Medicina Preventiva y Social, as lacking section on prophylaxis of IDD, 169
Medicine: vs. charity, 150
curative, vs. preventive, 5 , 169
nuclear, 10 , 15
and tolerance for criticism, 160 -161
Menstruation and IDD, 98 , 127
Mental retardation: decline of, 214 n. 4
economic cost of, 175
Metabolic error and IDD, 33 , 92
Middle class, goiter in, 13 , 218 n. 26
Migration, 43 , 61 , 64
IDD as cause or effect of, 6 -7, 77 , 105
de Miguel, Jesús, 166 , 182
Ministerio de Gobernación, 147 , 149 , 174
Ministry of Health, 148 , 180 , 218 n. 19
Ministry of Tourism, and drinking water, 151
Models of monogamy, 74
Monetary value of retardates, 131
Morreale de Castro, G., 169 -170
N
Narrative protagonists: Ofelia, 134 -137
Rosita, 96 , 98 , 137 , 143
Tabernera, 89 -92, 100
"Uncle Peter's People," 89
Narratives: of affliction, 67 -68, 142 -143
of margination and isolation, 131 , 142 -143
in medical education, 150
Narratives, collection of, 12
as part of anthropological method, 80
National Academy of Sciences (U.S.), 26
National School of Public Health, Spain, 159
Natural field experiment, 7 , 32 , 105 , 145
Natural selection by outmigration, 97
"Nerves" and IDD, 95
Niacin, 55 , 59 , 115
as anti-pelagra factor, 62 , 205 nn. 25, 26
Nicknames, 83 , 94 , 101 , 126
"No goiter not beautiful," 80 , 125
"Not inconsistent with . . . ," 88
Nuño, F., 181 -182
O
Ochoa, Severo, 178 , 201 n. 17
Old industries, new structures, and resentful bureaucracies, 177 -182
Ordenanzas, local regulations, 113
Organification, 22
"Origin myth," 142
Ortiz de Landázuri, E., 169 , 170 , 173
P
"Papal dispensation," 69
"Paper test" (the Yalow radioimmune assay), 169
Partible inheritance, 68 -73, 94
Pathology of IDD: codified by quadrant, 85
and division of labor, 49
estimates of, 186
and ethnicity, 131
as iatrogenic and secondary to simple goiter, 36
as idiopathic, 20 , 33 -35
and quest for treatment, 10
Patología Regional de Asturias,171
Pedigrees and genealogy, 18 , 67
Pellagra, 55 -57
and corn processing, 205 n. 25
as "regional disease," 171
Penred's syndrome, 215 n. 7
Pharmaceutical(s), consumption of, 45 , 64 , 215
industry, 184 -185
Phenotype, 100
Physicians and nutritional deficiency, habituation to sight of, 65 , 201 n. 17
Piedrola Gil, G., 169
Pilot projects, 169 -170
"Plausible deniability," and absence of biochemical data, 16
Political will: and lawsuit, 175 -177
making use of knowledge, 3 , 145 , 175
and middle class, 151 , 175
Population pyramid, Escobines, 76
Poverty, 18
and vulnerability to IDD, 25 , 32 , 75 , 121
Pregnancy and IDD, 34 , 87 , 98 , 135 , 146 , 163 , 175 , 216 n. 17
pathology of pregnancy seen as "normal," 98 -99
Preventability, public's growing awareness of, 176 -178
Primary care, 2 , 3 , 17 , 43
Prophylaxis, individual, 168 -169
Prophylaxis, mass: cost effectiveness of, 5 , 11 , 144
delay in implementing, 5 , 27
inception of, 6
opposition to, 156 , 170
rejection of, 8
Pseudonym of village, 202 n. 1
Q
Quantification of IDD, 35 , 77 , 121 , 177 , 193 -194, 199 n. 1, 200 n. 6
R
Racial degeneration, myth of, 147 , 162
"Racist" anthropology, 8 -9
Radioactive iodine (RAI), 36 , 138 , 201 n. 18
Regional autonomy, 174
campaigns for, 178 -179
Reportable disease: IDD as a non-, 77
pelagra as, 205 n. 31
Reproductive pool, 75 -79, 135
Reputation, 7
for foolishness, 42 -43
Restricted code (language). See Language
Retardate as boon to aged parents, 128
Retardation, 87
industrial implications of, 174 -175
monetary value of, 131
Revista de Sanidad e Higiene Pública (RSHP), 160 , 163 , 166
Right to know, the public's, 162
Roël, Faustino, 56 , 152
S
Salt: market for iodized, 180
Morton's Salt, 200 n. 9
mined, 25
sal de Roquetas, 170
solar, 53
Solvay, 168 , 178 , 180
Schoolchildren: 7 , 179
"stunted and inattentive," 178
T4/T3 ratio and cerebral function, 31
Screening, mass, 39
Scurvy, delay in implementing knowledge about, 2 , 144
Selection by outmigration, 105
Sense of abandonment, 51 -54
Sibling exchange, 69 -73
Simple and accessible information, 176 -178
Sites of IDD endemias: 6 , 7 , 26 -27, 70 , 175 , 180 , 222 n. 6
Social exclusion, 105
Socialists, 13 , 44 , 147
Social stratification and IDD, 7 , 105 , 117 -118, 132 , 140 -142
Sociogenic brain damage, 39
Sodium iodide, 180 , 200 n. 1
"Soul food," 119 , 205 n. 36
Soviet Union and prophylaxis, 192
Spanish Civil War, 43 , 61 , 165
Spanish Royal Academy of Medicine, 4 , 152 , 155
Sporadic cretinism, 175
Stanbury, John, 22 , 29 , 176
Statistics: and the "cabbage patch," 177
"no need" for, 181
Stigma, 86 , 119 , 135 -136, 141
difficulties of investigating, 12
Strabo (63 B.C.-A.D. 24), 48 , 147 , 203 n. 12
Supplementation, 25 , 34 -35
experimental, 146
as "locally ideal," 22
"Surrealism," disease as, 145
Survey: "appropriate" if biochemical, 15 -16, 176
official, 179
by palpation, 161
by visual inspection, 77
Switzerland, xi , 4 , 26 , 28 , 47 , 162
T
Television campaign and IDD (Sanchez Ocaña), 180
Theories of endemic goiter and cretinism: "bad blood," 94
biologic vector, 173
dietary, 29 -31
gradual spontaneous decline, 10
inbreeding, 66 -67, 104 -105
innate vulnerability, 25
mysterious factor "x," 173
underdevelopment, 10 , 17
"Thinness of critical scientific discourse," 159 , 188
Thiocyanate, 32
"Three Decrepits, The," narrative of, 132
Thyroid: cancer of, 30
medication, 182
palpability of, 161
Thyroid pathology, 10
autoimmunologic origin, 37
monetary value of (to physician), 183
and nuclear fallout, 201 n. 19
thyrotoxicosis, 29 , 157 , 163 , 202 n. 23
Thyroid stimulating hormone (TSH) and view of goiter as adaptive, 30
Thyroxin differentiation into T4 and T3, 7 , 16 , 22 , 178
T4/T3 ratio and brain function, 31
Topografías médicas,151
Tourism, 44 -45, 97 , 101
Toxicity of trace elements, 22
Turnip, dietary importance of, 114 -119
U
Underdevelopment, 10
as explanation for non-prophylaxis, 17 -18, 155
Uprising and strikes, 61 , 64
Urinary Iodine Excretion (UIE) rate, 16 , 27 , 148 , 178 , 179 , 200 n. 6, 218 n. 16
Useless thyroid medication and American involvement, 183
V
Vaqueiros, a transhumant people, 53 , 119 , 132 , 140
Velázquez, Franco, and Marañón, 219 n. 32
Vocabulary of deficit, 86 , 91 -92, 126 -131, 175 , 215 n. 8
Vollsalz, complete (iodized) salt, 4 , 155
W
Weight control and iodine, 155 , 167 , 168
"When it rains, it pours," 188
WHO (World Health Organization), 14 -15, 27 , 176 , 179 , 188
Wildfoods and goitrogens, 110
Women: and comparative behavioral deficit compared to that of men, 128 , 137
eosmetic and social effects of IDD, xiii , 15
and stress, 127
COMPARATIVE STUDIES OF HEALTH SYSTEMS AND MEDICAL CARE
General Editor
John M. Janzen
Founding Editor
Charles Leslie
Editorial Board
Don Bates, M.D.,
McGill University
Frederick L. Dunn, M.D.,
University of California, San Francisco
Kris Heggenhougen,
University of London
Brigitte Jordan,
Michigan State University
Patricia L. Rosenfield,
Carnegie Corporation
Paul U. Unschuld,
University of Munich
Francis Zimmermann,
Centre National de la Recherche Scientifique
For a complete list of titles in this series, please contact the
Sales Department
University of California Press
2120 Berkeley Way
Berkeley, CA 94720
Designer: U.C. Press Staff
Compositor: Prestige Typography
Text: 11/13 Caledonia
Display: Caledonia
Printer: Braun-Brumfield, Inc.
Binder: Braun-Brumfield, Inc.
Preferred Citation: Fernandez, Renate Lellep. A Simple Matter of Salt: An Ethnography of Nutritional Deficiency in Spain. Berkeley: University of California Press, c1990 1990. http://ark.cdlib.org/ark:/13030/ft2d5nb1b2/