Creating a Composite Image of the Hysteric
It is vital to understand that the creation of a history of the image of the hysteric is not the same thing as Charcot and Richer's attempt to place the diagnostic criteria applied to hysteria in the distant past (while ignoring the more recent past). What can be undertaken in a limited way (because of the extraordinary range of visual sources) is to sketch the visual aspects associated with the idea of hysteria at the turn of the century as a means of delineating the scope of the image. Thus this section will be devoted to a catalog of those visual qualities ascribed to the hys-
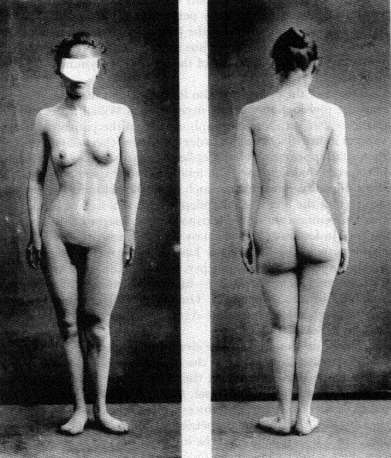
On the image of asymmetry of the epileptic, see plate XLI: "Asymetrie du
corps chez une epileptique," in F. Raymond and Pierre Janet, "Malformations
des mains en 'pinces de humard,'" Nouvelle iconographie de la Salpêtriée 10
(1897 ): 369-373 (an extract from their book Nécroses et idées fixes [Paris: F.
Alcan, 1898]).
Photo courtesy Wellcome Institute Library, London.
teric. We shall seek to sketch the boundaries of the representation of the visual nature of the hysteric in fin-de-siécle medical literature.
It is central to any understanding of this composite image that the desire of all of these studies, no matter what their national context, is to place themselves within the myth of the realism of the act of represen-

The face of the epileptic. From William Alexander, The Treatment of
Epilepsy (Edinburgh and London: Young J. Pentland, 1889), p. 107.
Photo courtesy Wellcome Institute Library, London.
tation and the highly specialized role that the physician (as interpreter) plays in reproducing and "reading" the image of the patient. And this reading has a clear relationship with the means of reproducing and disseminating the image of the hysteric. The startle effect has now blended into an idea of a realism that indicates a control by the scientist and the scientist alone over the new medium. (As anyone could make and possess photographs after the mid-1890s, it became more and more important for the scientific photograph to be the object of scientific interpretation. This attitude permitted many interpreters of the photograph of the patient seamlessly to become the interpreters of the new hermeticism of the X ray when it was introduced in 1895.) The reading of the photograph had also blended in with the aesthetic (or, perhaps better, artistic) tradition into which the "new" science of representation had placed the image of the hysteric. Charcot and Richer, in a paper they first published in the Journal of Nervous and Mental Disease in 1883, stated the case best. In noting the "immobile" physiognomy of a hysterical patient whose facial muscles had been electrically stimulated, they
Images of the alteration of the hair in the mentally ill are already evoked
in Darwin's study of the nature of expression. Here the image of the altered
appearance of the hair evokes older images of the diseases of the Eastern Jews.
From Dr. Räiuber, "Ein Fall von periodisch wiederkehrender Haarveräinderung
bei einem Epileptiker," [Virchows] Archiv für pathologische Anatomie und
Physiologie 97 (1884): 50-83, plate no. 2.
(Bethesda, Md.: National Library of Medicine.)
observe: "The physiognomy retained immobile, in a state of catalepsy. The same is true of the attitude and the gesture that accompanied it. The subject of this transformed into a sort of expressive statue, a motionless model, representing with striking accuracy most varied expressions, which artists, without doubt, might avail themselves of to a very great extent. The immobility of the attitudes thus provoked is eminently favorable to photographic reproduction."[83] They then reproduce a series of these photographs. This argument is similar to that critique by Walter Benjamin in his essay from the mid-1920s on the reproducibility of images in the age of technology.[84] For it is important to understand that observing is not sufficient. Charcot (and Richer) turn the object observed (the hysteric) into the work of art and then are able to commodify this work of art through the reproduction of her image within the scientific text. This is not quite like the cinematic examples that Benjamin brings. It is much more similar to the extensive photographic reproductions of "great works of art" which dominated the middle-class market for art during the 1880s and 1890s. Benjamin's discussion of the "exchange of glances" between the observed and the observer creates a critical context for the learning experience of the hysteric. For it seems that the exchange of glances in this system of representation is one between an aware hysteric and an unaware physician. But the Salpêtriére gave birth to other means of seeing difference and also of recording it.
In many of these images the confusion between acquired pathognomonic signs and inherent ones is manifest. There evolves in the finde-siécle discussion of the physiognomy the assumption that there is an absolute relationship between the form of the skull and the shape of the face.[85] And given the emphasis on craniometric measurements as a means of speaking about the nature of the mind/psyche it is clear that the relationship between the structure of the face and the mind, already present in the physiognomy of Johann Caspar Lavater (and his predecessors) becomes an easy one. Francis Warner summarizes many of the discussions of his contemporaries, such as Charles Darwin, in The Expression of Emotions in Men and Animals (1872).[86] Warner stresses the "results of cerebral action upon muscles" rather than the "shape of the brain case" in seeking to find the source for the asymmetry on the face of the hysteric. She describes, however, the existence of faces that "express intellectuality" and others that express "vulgarity." The latter are an example of the "coincident defective or coarse development of the brain-case and face." The former are the result of "the nerve-muscular condition of the face" and are "more directly indicative of the intellectuality of the brain; hence we should study a face as the index of the brain, when it
is seen in action as well as when at rest." This view can be seen as representative of the medical literature of physiognomy at the turn of the century. The stress on the asymmetry of the face, an asymmetry caused by the forces of the mind, rather than the marked "vulgarity" of the mental defective, can be traced back to Philippe Pinel and his representation of the "manic" and the "idiot" at the very beginning of the century. The concept of asymmetry (indeed all faces become asymmetrical with the passage of time) can introduce the importance of an aesthetics of the face of the hysteric.
James Shaw stresses the "swelling of the upper lip" in cases of "chronic hysterical insanity" as well as a "facial expression [that] often indicates the presence of migraine."[87] The face of the hysteric, specifically the hemiplegia that marks the face of the hysteric at the Salpêtriére, is an overt sign of difference. It is a distortion of the normal face—the baseline for the "beauty" of the individual.[88] Anthropological literature of the eighteenth and nineteenth centuries had debated the meaning of the varieties of beauty, especially female beauty, throughout the world.[89] The consensus was that there was a "great chain of beauty" running from the beautiful down to the ugly races which was paralleled within each race by a normative—that is, healthy—appearance as opposed to a sick appearance. This pathology of appearance underlies the representation of the asymmetrical, unaesthetic face of the hysteric. In a paper by Hurst (1918) on battle fatigue, the face of the hysteric marks the individual who can be quickly cured and sent back into battle.[90]
But if the face is marked, it is the eyes that provide the real clue. The stigmata that mark the face are most apparent in the representation of the eyes. For both the "look" of the hysteric and the gaze of the physician mark the hysteric. Building upon the nosology of hysterical blindness developed by Charcot as well as the Philadelphia ophthalmologist George Edmund de Schweinitz, Walter Baer Weidler traces the qualities of the eyes from the "contractures, spasms and palsies" of the "eyelids and extra-ocular muscles" (i.e., the representation of the appearance of the eye) to the manifestation of hysterical blindness (amblyopia or amaurosis, partial or complete loss of vision).[91] In the work of L. Lattes and A. Sacerdote from the 1920s, similar changes in the quality of the face are described in the case of a hysterical pseudo-hemorrhage of the eye.[92] It is the quality of the gaze in the photographs of the patients that is striking. The physical anomalies represented also provide the signs for the meaning read into the physiognomy. The drooping lids or the black eye add a quality of the abnormal, of the pathological, to the gaze of the patient, marking him or her as diseased.
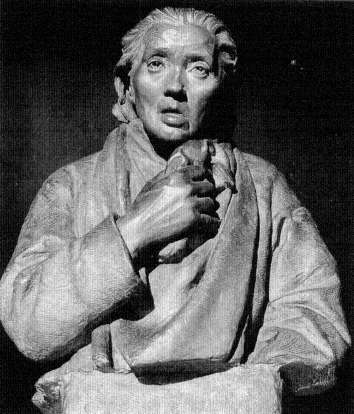
A sculpture of a case of hemiplegia from the teaching
collection of the Salpêtriére.
(Paris: The Salpêtriére.)
The disease that is sought is not in the eye. It is in the central nervous system, in the neural network that controls the eye. It is in the brain, the source of all hysteria, that the source of hysteria is to be found. The image of the brain becomes the image of the internal error of the hysteric. Jules Luys, in a paper of 1881, stresses this in both his text and in the accompanying images of localization.[93] E. Siemerling and J. Grasset see "cerebral-spinal degeneracy" as the source of hysteria.[94] In the work of the Hamburg physician Paul Steffens the localization of the lesion is represented in the post-mortem image of the brain.[95] All of these searches evoke the specter of the brain mythology that dominated much of the localization studies at the end of the century. The search after
The eyes and the sight of the hysteric. From Walter Baer Weidler,
"Some Ocular Manifestations of Hysteria," International Clinics ,
22d ser. 2 (1912): 249-261. Plate (fig. 5) opposite p. 252.
Photo courtesy Wellcome Institute Library, London.
the source of the anomalous appearance of the hysteric was quite parallel to the search after the origins of other neurological disorders. A. Alzheimer represented such a search in his 1911 paper on cerebral plaques, using photographs of dyed brain specimens as his visual proof of their existence.[96]
All of these images were seen as having parallel value. Each of them demanded (according to their interpreter) a trained eye to see and represent the source of the error. The interrelationship between the scientific drawing and the photograph, both understood as veridical in localizing the source of the pathology, stressed the gaze of the scientist, in seeing the nature of the brain through the interpretation of the symptoms.
For the hysteric, the symptoms are often written on the body. The
The brain of the hysteric. From Jules Luys, "Recherches nouvelles
sur les hémiplégies émotives," L'Encephale: Journal des Maladies
Mentales et Nerveuses 1 (1881): 378-398, plate 7.
(Bethesda, Md.: National Library of Medicine.)
The brain structure of the hysteric. From C. von Höb lin and A.
Alzheimer, "Ein Beitrag zur Klinik und pathologischen Anatomie der
Westphal-Strümpellschen Pseudosklerose," Zeitschrift für die
gesamte Neurologie und Psychiatrie 8 (1911): 203.
Photo courtesy Wellcome Institute Library, London.
function of the skin as the map of the body is one of the oldest topoi of medicine. Reading the skin meant reading into the nature of the patient, his or her actions, and his or her resultant diseases. The nineteenth-century literature on masturbatory disease is full of such images,[97] as is, not surprisingly, the literature on hysteria. The ability of the hysterics to record written images on their skin, the hypersensitivity to touch, became one of the most fascinating symptoms for the fin-de-siécle physician. In the "modern" Revue de l'hypnotisme a striking image of such "skin writing" appears.[98] In Saint Petersburg the fin-de-siécle image of the hysteric was brought into the context of the stigmata, not Charcot's, but the stigmata of Christ.[99] The discussion of the patient presented in this "difficult case of hysteria" centered on the suggestibility of young Roman Catholic girls. The search after unique or strange manifestations
The ulcerated skin of the hysteric. From S. Weir Mitchell, "Hysterical
Rapid Respiration, With Cases; Peculiar Form of Rupial Skin Disease
in an Hysterical Woman," Transactions of the College of Physicians of
Philadelphia 14 (1892): 233.
(Bethesda, Md.: National Library of Medicine.)
of hysteria led S. Weir Mitchell, whose rest cure had been generally accepted as the treatment of choice by the end of the century, to examine a case of a hysterical ulcer in a twenty-four-year-old woman.[100] The differential diagnosis to this ulcer was to the ulceration of syphilis, which was "verified by the microscope." S. Róna continued the work that Moriz Kaposi had begun in Vienna, looking at specific forms of the manifestation of skin eruptions which could be labeled hysteric.[101] Thomas D. Savill, in London, undertook a similar study of the skin of his child patients and saw their hysteria inscribed thereupon.[102] In 1900 Dr. Bettmann from the Heidelberg Clinic of Wilhelm Erb described a further case of "atypical" skin inflammation in the hysteric; in 1901, a case of hysterical gangrene was described in Buffalo; in 1919, a similar case in Pisa. By 1930 a major survey of the nature of hysterical skin diseases was produced by Roberto Casazza in Pavia.[103] All of these studies (and more) are extensively illustrated. All of them relate, on one level or another, to the general assumption (countered by Jean-Martin Charcot in his theory of hysteria) that syphilis or the predisposition to syphilis played a major role in the risk for hysteria.
Many of these studies of the skin (such as that of Weir Mitchell) relate the appearance of the skin to the state of the genitalia, either in
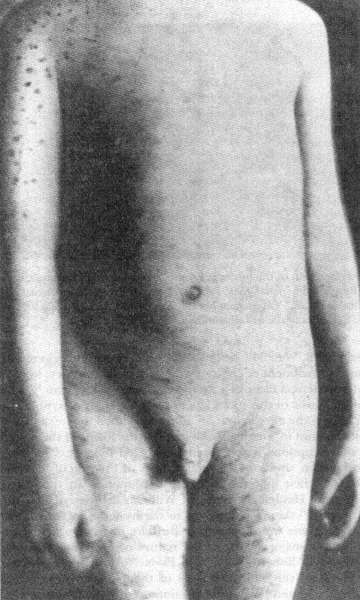
The association between the syphilitic and the hysteric was made as
much on dermatologic evidence (as seen on the skin) as on psychological
evidence. From Thomas D. Savill, "A Clinical Lecture on Hysterical Skin
Symptoms and Eruptions," The Lancet (January 30, 1904): 273-278, p. 276.
(Bethesda, Md.: National Library of Medicine.)
terms of gynecological examinations that are part of the case study or in terms of a discussion of the appearance of the skin in the genital regions. Charcot associated hysteria with the area of the ovaries, those areas of heightened sensitivity in the hysteric, a touch upon which could actually create hysterical episodes. This fascination with the compression of the ovaries as therapy as well as etiology is linked in the medical discourse of the period with the fascination about hysterical ischuria, the retention of urine and feces. The number of charts of the genital regions are legion, yet the number of detailed (and illustrated) studies of the form and structure of the genitalia are few. De Sinéty, a histologist at the College de France, published a series of unillustrated case studies of the genitalia of female hysterics in the mid-1870s, supporting Charcot's thesis of the centrality of sexual stimulation for the creation of the hysterical episode.[104] With the introduction of X-ray analysis there was even an attempt to represent the pelvic structure of the hysterical female, as a means of representing the disease.[105] The X ray was but a technical innovation. For the fantasies about internalized hysteria had existed prior to Charcot.[106] In 1847 Eliogoro Guitti had presented an illustrated study of the hysterical gut.[107]
The representation of the extremities, especially the hand and the foot, reflect not only the importance laid upon the hand and foot as signs of religious possession (stigmata, paralysis) but also the physical signs associated with epilepsy. Paul Sollier presents a case of contracture of the hand in a male hysteric in the fourth volume of the Nouvelle Iconographie de la Salpêtriére .[108] Some of the studies, such as those of Hurst, concentrate on the problem of hysterical contractures, such as Charcot's "glove anaesthesia" in the hysterical traumatic paralysis of the hand; others on the appearance of the hand, its coloration (usually blue, according to Gilles de la Tourette[109] ) and marked swelling.[110] The legs are similarly examined for the contractures of "hysterical paraplegia" (and their cure).[111] The images taken from Charcot's schematic representation of areas of anesthesia reappear over and over again to illustrate cases of the diminished ability to feel (and often to move) the limbs.[112]
The visual representation of posture and paralysis is used as a mode of visual proof of Charcot's nosological categories.[113] In an essay from the very first issue of the Nouvelle Iconographie de la Salpêtriére in 1888, by Georges Gilles de la Tourette, we are not only made to see the hemiplegic patient but also his gait, through a schematic representation.[114] In this case, described by Henri Lamarque and Emile Bitot, there is a comment on the plate that they had intended to use a photograph but an accident at the last moment ruined the plate and they were forced to
The X ray permitted the physician to see within the hysteric.
From Jose M. Jorge, "Coxalgia histérica," Revista de la Asociacion
Medica Argentina 32 (1920): 18-29, plate opposite p. 80.
(Bethesda, Md.: National Library of Medicine.)
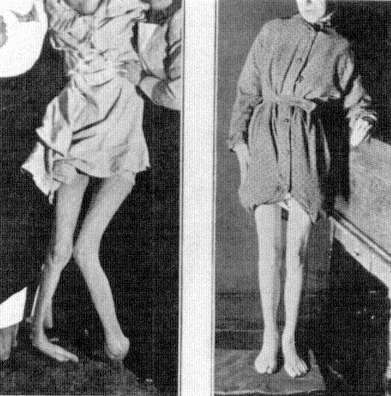
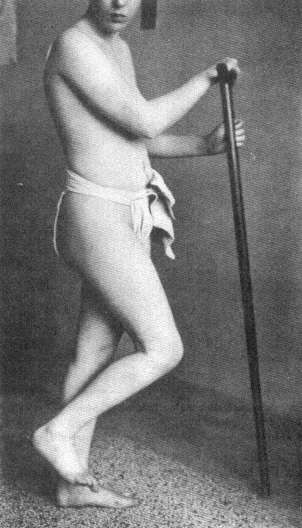
use a photolithograph. The form of the representation becomes central to its message. For the photograph remains more real than any other mode of representing the hysteric. Thus in an essay by Byrom Bramwell—one of the leading Scottish specialists on nervous diseases such as hysteria and, one can add, one of the leading believers in a set pathognomonic representation of disease—the photograph remains the central proof for the differential diagnosis between "hysteria" and its contractures and other forms of organic disease.[115] But this photograph has been quite evidently cut to remove the presence of the physician or nurse whose hands remain supporting the patient. A similar undertaking can be seen in the photograph contracture represented in the essay by A. Steindler in Iowa City, except here the patient is given a staff on which to rest.[116]
The realism of the photograph concentrates the gaze of the physician-reader on the representation of the disease in the image of the patient. Peter Davidson follows this lead with his presentation of a case of hystero-catalepsy from Liverpool.[117] The number and range of Davidson's
The hysterical gut as an internal manifestation of the disease.
Eliogoro Guitti, "Osservazioni Cliniche," Giornale per Servire ai
Progressi della Patologia e della Terapeutica , 2d ser. 22 (1847): 229-258,
plate following p. 258.
(Bethesda, Md.: National Library of Medicine.)
cases (running from rheumatoid arthritis to hystero-catalepsy) would have enabled the author to illustrate any (or indeed all) of his cases. He chose to illustrate the case of hystero-catalepsy. As late as in 1930, in an essay by Prince P. Barker, at the Veterans' Hospital in Tuskegee, Alabama, the image of the hysteric black comes to represent the image of the hysteric whose limbs are frozen.[118] Using Charcot's categories ex-
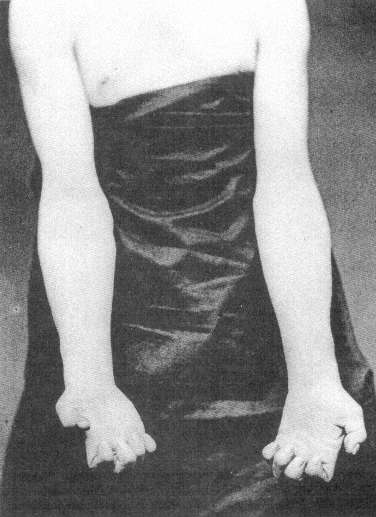
The hand of the male hysteric. From Paul Sollier, "Contracture Volontaire
chez un Hystérique," Nouvelles Iconographie de la Salpêtriére 4 (1891): 100-106,
plate opposite p. 106.
Photo courtesy Wellcome Institute Library, London.
The posture of the schematic "patient." From Henri Lamarque and
Emile Bitot, "Sur un cas d'hystérotraumatisrne chez l'homme,"
Bulletins de la Société d'Anatomie et de Physiologie Normales et
Pathologiques de Bordeaux 9 (1888): 242-257, plate with
figures 6 and 8.
(Bethesda, Md.: National Library of Medicine.)
A "doctored" photograph of the hysteric. From Byrom Bramwell, "Clinical
Lecture on a Case of Hysterical Contracture," Edinburgh Medical Journal ,
ns 1 (1897): 128-138, plate 5.
(Bethesda, Md.: National Library of Medicine.)
Above and verso: The hysteric posed. From A. Steindler, "On Hysterical
Contractures," International Clinics , 4th ser. 45 (1935): 221-229, fig. 2,
opposite p. 222.
Photos courtesy Wellcome Institute Library, London.
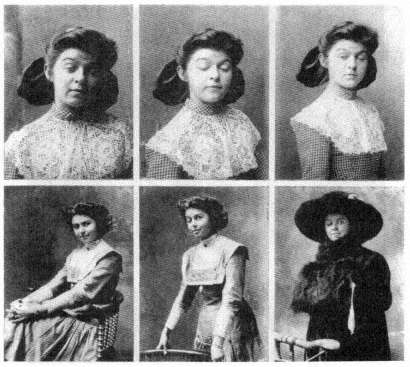
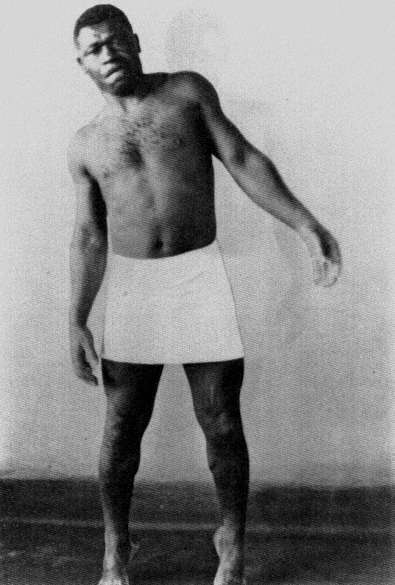
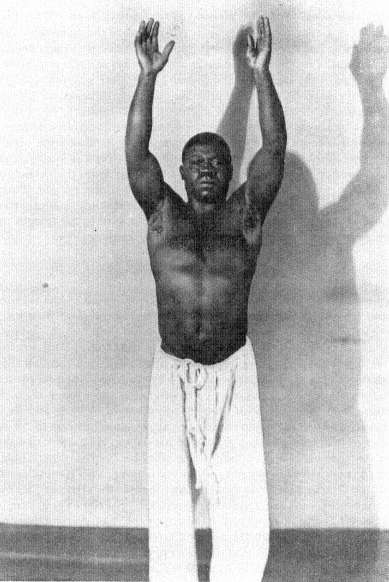
pressly, Barker shows three images. First, an image of the "normal," that is, pathological, posture of the patient; second, an image that in its blurred state is to represent the range of motion in the patient; and finally, an image of the body restored through "etherization and suggestion." Here the impact of the cinema on the idea of realism is evident. Whereas in the work of Lamarque and Bitot such an image would be understood as ruined, here it reveals a further aspect of the realism associated with the act of photographing.
One last form of realistic representation of the hysteric should be discussed. For throughout the vast literature of hysteria (and other forms of mental illness) in the nineteenth century there are uncountable
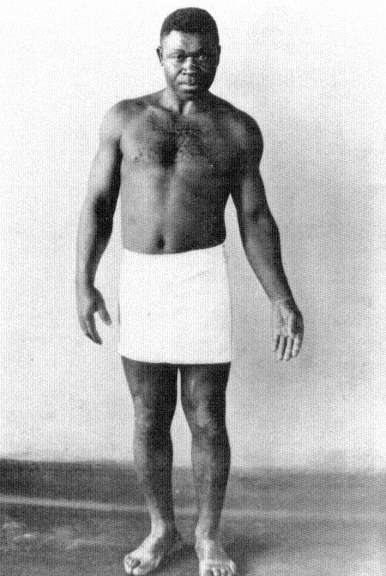
The illusion of movement in representing the hysteric. From Prince P.
Barker, "The Diagnosis and Treatment of Hysterical Paralysis," United
States Veteran's Bureau Medical Bulletin 6 (1930): 663-670, 3 plates
following p. 670.
(Bethesda, Md.: National Library of Medicine.)
charts, graphs, and statistical tables. It is virtually unimportant what source one uses. From the medical periodicals in France[119] to those in Japan[120] or Germany,[121] one consistent image of the hysteric is that of the scientific reduction of the sufferer and the disease to schematic representations. The cry of these images is that they are the real, transcendent image of the hysteric. Like Galton's composite photographs (which will be discussed below), they give the observer an image of the totality of the disease. This fantasy of reducing the complexity of hysteria to statistics or charts rests on a notion of nineteenth-century science that everything is reducible to nonverbal form (read: mathematical), and that is precisely the claim of the photograph. For once, it is said, you eliminate narrative, you remove the subjective aspect from the evaluation of the disease and you have a real representation of the patient. Thus the use of charts and statistics in representing the hysteric is another visual means of creating an image of the disease, as sure as the images of the skin, or brain, or cellular structure of the hysteric.