Medical and Aesthetic Models for the Representation of the Hysteric
The image of the hysteric does not simply arise out of Jean-Martin Char-cot's personal interest in the visual representation of the hysteric at the Salpêtrière.[34] Charcot does not invent the act of "seeing" hysteria. His own interests in capturing the visual aspect of his patients combined with his own perception of his hysterical patients to record the image of his patients as early as his first years at the Salpêtrière, the 1860s. Charcot comes to his task of understanding his patient with a long personal need to see and represent the patient. But his view is not unique, it is part of a long-standing European tradition of representing the insane, into which the image of the hysteric must be fitted. Indeed, it is a tradition which is as much popular as it is scientific. For Moreau de Tours's image provides us with another context for the structuring of the hysteric—the world of the hypnotizable patient, the image of the mesmerizable female. For hysteria, from the eighteenth century, is a disease of the imagination, not a disease of the womb.
The image of the patients of the Viennese physician Franz Anton Mesmer and his students during the 1780s provides one of the keys to the representation of the hysteric at the end of the 1800s.[35] After his arrival in Paris in the winter of 1778, the representation of Mesmer becomes part of the tradition of representing the insane. In a contemporary cartoon reflecting a mesmerist session, it is not merely that the quack physician is indicated by his ass's ears. More important is that the patients gathered about the mesmerist's "tub" are represented in the traditional pose of the melancholic (with head on hand on knee) and the lovesick (swooning in the chair). The latter becomes identified retrospectively with the arc-en-cercle position of the hysteric (in some of the historical writing of the mid-twentieth century), because of the associa-
The image of the mesmerist.
(Paris: Bibliothèque nationale: Cabinet of Prints.)
tion of the hysteric with the sexual (in many different ways), while the melancholic vanishes from any consideration as a forerunner of the image of the hysteric. The visual representation of the mesmerist and the patient are all means of limiting the scope of the diseased to the identifiable individual.
The suppression of the political radicalism associated with one of the most influential groups under Nicolas Bergasse after the French Revolution meant that there was a general tendency to see the mesmeric patient as an asocial being who only shammed illness out of a sense of social uselessness. Likewise, the mesmerist was understood, not as a force for change, but as a quack. The cartoons of the patient and the physician from the 1780s had already carried that message. In one such image a mesmeric healer, wearing an ass head, begins to mesmerize a young, female sufferer.[36] Her position echoes the association of disease and sex-
The "ass-mesmerists."
(Paris: Bibliothèque nationale: Cabinet of Prints.)
uality in the arc-en-cercle position of the grand hysteric, as she begins to lie back in her chair as her moral seduction begins. Mirrored in the background is the representation of the sexual exploitation of the female patient by the mesmerist, warned against in the secret appendix to the Report of the Royal Commission on Mesmerism. Here the physician is as hypersexual as the patient.
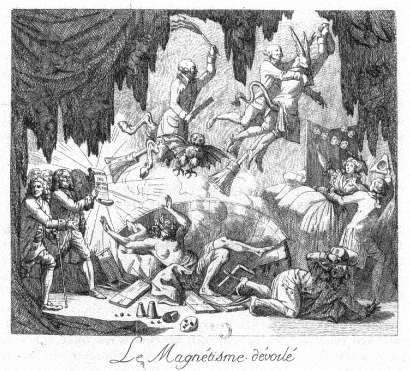
In another image the conceit of the ass-mesmerists is repeated.[37] They are being driven out of the scene by the shining truth of the report of the Royal Commission held by Benjamin Franklin. What is central to this image is that the mesmerists are represented as a compound sign. They are both madmen and devils. They are viewed as a parody of the images of the demonic evil spirits released from the mad as healed by Christ (and his saints) in the traditional iconography of madness. Here the split-hoofed image of the devil as well as the broomsticks associated with flying witches are employed. But this image of the healer is also that of the insane, for the split-hoofed figure is brandishing a scourge, which is one of the traditional icons of the insane. The figure of the arc-en-cercle in the representation of the patient is here reversed. The blindfolded, naked patient is seen in the closed mesmeric tub, not arched but collapsing inward. This can be seen as antithetical to another image of the mes-
merist healing process, the circle of "magnetized" hands, in which a seemingly unconscious female is represented in the left foreground; balancing the portrait of Mesmer, the healer, in the right foreground.[38] The imagery of this representation is tied to an understanding of the "meaning" of mesmerism and the mesmerist treatment in the course of the nineteenth century. The disrepute of the mesmerist, labeled as insane or demonically possessed, and thus in need of the sort of control represented by Franklin, Antoine-Laurent Lavoisier, and the Royal Commission, is carried over into the disrepute associated with the very naming of the treatment. The image of the physician, as well as the patient, is drawn into question in these associations. Such images remain associated with the idea of the hysteric through the visual representation of the patient.
The mesmerism patient is understood at the close of the nineteenth century to be one of the precursors of the fin-de-siècle hysteric. The image of the physician, as in the portraits of Charcot and Luys, must be quite different from that of the mesmerist; it must be separated from the image of the quack. Rather this image must be associated with the heroic image of the alienist, the image of Pinel as a force of social change (like Franklin). Merely changing the label of the mode of treatment from mesmerism to hypnotism or electrolization was not sufficient. The very relationship between the hysteric and the physician must be merged into the highest level of institutionalized medical representation—that of the image of science in the science of creating images.
The image of the hysteric in the medical literature of the nineteenth century is an essential image of deviance. It is an image that is taken—at least in its most radical form—out of another context. The central image of the hysteric, the essential attitudes passionnelles in Charcot's vocabulary of images, is a sign of quite a different disease—tetanus. The arc-en-cercle stage of Richer's image of grand hysteria (and its retrospective reading of the image of the swooning mesmerist patient) was consciously modeled on an image taken from the literature on the representation of anatomy and pathology for artists, rather than from a purely medical source.[39] Taken from the second edition of Sir Charles Bell's Essays on the Anatomy and Philosophy of Expression (1824), this image is rooted in a specific understanding of the nature of medical semiotics. Bell notes:
I throw in this sketch to remind the painter that in convulsion , although there may appear to him an accidental and deranged action of the muscular frame, there is no such thing in nature. It is a disease he is representing, which has definable symptoms, and it will ever present itself with the same characters.[40]
The range of the positions of the hysteric. Given best in Paul Richer, Études
cliniques sur le grande hystérie ou hystéro-épilepsie
(Paris: Delahaye & Lecrosnier, 1881), plate 5.
(Bethesda, Md.: National Library of Medicine.)

The opisthotonic position. From Sir Charles Bell's Essays on the
Anatomy and Philosophy of Expression (London: John Murray, 1824), p. 101.
(Bethesda, Md.: National Library of Medicine.)
Bell's observation may well hold true for tetanus, but the opisthotonic position chosen by him to represent the unalterability of the relationship between sign and causation is adapted by Charcot and later by Freud and given specific meaning in regard to the representation of the illness of the nerves and mind in the hysteric. One must note that Charcot is not the first "modern" scientist to call upon tetanus as his ontological representation for "seeing" the body. John Brown (1735-1788), in evolving the concept of the irritability of the muscles from the work of Albrecht von Hailer, argues that health and disease are not at all different states since the forces that produce each have the same action.[41] His example is a comparison of the normal contractions of the muscles and the pathological appearance of the opisthotonus in tetanus. The opisthotonus is one of the most striking manifestations of any disease. But it is also an almost infallible sign for the physician, since its outcome is almost surely negative. In a world in which the power of the physician lay, not in the ability to cure, but in the ability to foretell the course of a disease, the meaning of this sign for doctor and patient alike was clear. Thus Brown, Bell, and Charcot all call upon the image of the opisthotonus as a sign of the visual interpretability of disease and, therefore, the power of the physician's insight over the disease. At the end of the nineteenth century there was still a clear need to provide differential diagnosis between tetanus and hysteria for the practitioner. Among other signs, tetanus was described as presenting "persistent rigidity with
tendency to opisthotonos . . ." while hysteria presented "opisthotonos persistent, and intense rigidity between convulsions."[42] In seeing the patient, little distinction was made between organic and functional deficits.
Charcot in seeing the hysteric evolves his own system of representing the disease. He sees the hysteric as suffering from a weakness of the nerves and the disease as being caused by a trauma (such as an accident or violence). Thus the hysteric patient was predisposed to the disease—at least once he or she was exposed to some traumatic event. It is clear that Charcot evolved this view through his treatment of the patients at the Salpêtrière—epileptic and hysterical female patients who were as different from him (and his class) as was possible.[43] The counterargument to this view was evolved by John Hughlings Jackson, whose initial interest was sparked by his wife's epilepsy. This view was one of universal susceptibility. Seeing the disease as a pattern of the dissolution of the higher functions of the nervous system through the presence of a lesion, Jackson understands the symptoms of the hysteric as signs of the lower (and therefore earlier) functions of the nervous system. This evolutionary model sees the symptoms of the hysteric as signs of the structure of the more primitive psychic organization. Both views—the view that calls upon trauma and biological predeterminism as well as the view that calls upon the model of the nervous system being layered to represent the evolutionary history of the mind—come to be absorbed in the fin-de-siècle debates about hysteria.[44]
As early as 1888, Sigmund Freud calls up the figure of the opisthotonus in the context of attacks of hystero-epilepsy.[45] He continues this argument as late as 1908 when he understands coition to be a form of "minor epilepsy." For "a hysterical attack is the reflex mechanism of the act of coition—a mechanism which is ready to hand in everybody, including women, and which we see coming into manifest operation when an unrestrained surrender is made to sexual activity."[46] Thus Freud explains the opisthotonus as the antithesis of the embrace—the internalized enactment of coitus. But this is an image that does not vanish, but is rather consistently transmuted.
Freud uses the image of the opisthotonus as the antithetical image to coitus within his initial reworking of Charcot's nosological criteria. Seeing the reality of the opisthotonus as the key to the somatic nature of hysteria meant understanding the concept of trauma as existing in real experience rather than in fantasy. Sándor Ferenczi, in his clinical diary of 1932, can call upon "a case in which in relaxation ('trance') opisthotonic positions did appear: when contact could be established with the patient, she reported that the position was a reaction to a feeling of
painful excitation in the genital passage, which the patient described as painful hunger: in this position, psychic unpleasure and defense against ardent desire are simultaneously represented."[47] Ferenczi traces this reaction formation back to the actual seduction of the female child by her father. All of these references—and Charcot's own vocabulary of images, especially the opisthotonus—stem from a vocabulary of images which clearly (at least in the medical literature of the nineteenth century) defined the line between the healthy and the diseased. The opisthotonus is a sign of the presence of a disease—whether a form of hysteroepilepsy or a signifier of pathological sexuality or a real seduction.
There is a one-to-one relationship between the sign and the meaning. Given Freud's own complicated formulas for the generation of symbolic meaning, already documented in detail in his 1900 Interpretation of Dreams , it is striking that in returning to the subject matter of the hysteric, which he and Josef Breuer had begun to explain in 1895 as the result of the suppression of real traumatic events—that is, precisely the sort of seduction of children by adults in authority (parents) to which Ferenczi, quite opposed by Freud, returns some three decades later—he reverts to a pattern of explanation that relies on the meaning of the visual image.
The association between images of the tetanal opisthotonus is in no way limited to the neurological literature coming out of the Salpêtrière or out of the Viennese schools of psychoanalysis. During World War I, Arthur F. Hurst reflected on the relationship between the hysterical etiology of "war contractures" ("battle fatigue" or posttraumatic neurosis) as opposed to those contractures which have their origin in a localized infection.[48] For Hurst the question of the differential diagnosis of hysterical contracture (here localized in contrast to the full-body opisthotonus) as opposed to localized tetanus is questionable. It is clear that in time of war the duration of the cure—a "single sitting by persuasion and reeducation" in the first case or "months of treatment" in the latter—would place emphasis on seeing the majority of such cases as quickly healable. The assumption in Hurst's presentation is that the confusion between real (i.e., somatic) and hysterical contractures advocated by continental neurologists such as Josef Babinski and Jules Froment marks a faulty distinction between a biological and a psychological illness.[49] Such an argument would be parallel to Freud's attempt to collapse the distinction between real epilepsy and hysterical epilepsy. The images of the case of tetanus as opposed to the hysteric are, however, quite illuminating. For the half-body portrait of the soldier with his wound prominently displayed relates the image of the contracted arm
to the entire individual; the hysterical arm stands alone. Here the role of the representation of the arm comes to play a central role. The case described, that of "Sergt. M" who "was wounded in the right forearm on April 10, 1917," is "recognized as hysterical. . . as the deformity was identical with that shown in a photograph of a so-called reflex contracture in Babinski and Froment's book." It is the representation of the hysteric which defines the disease and which defines both the treatment of the disease and the patient's response: "On the day of admission the hand was continuously manipulated, the patient being persuaded at the same time that it would rapidly relax. In ten minutes complete relaxation was obtained and the deformity disappeared." The relationship between seeing correctly and the patient's response is here made absolute. As Elaine Showalter notes, the transition from the image of the female pet patient of nineteenth-century clinical psychiatry to the image of the male sufferer from traumatic neurosis (shell shock) meant a drastic realignment of the presuppositions of gender.[50] Hurst sees the male hysteric as ill but as quickly curable, a factor that sets the soldier apart from the long tradition of more or less professional (i.e., long-term) female patients at the Salpêtriére. What he teaches his hysterics is to see themselves as "men"—to confront their illness and return to service.
Jean-Martin Charcot (and his colleague Paul Richer) provide the reader (and viewer) of these late nineteenth-century images of the hysteric with a set of antecedent images from sources other than the unspoken one of the mesmerist.[51] In their study of the representation of the insane—specifically the hysteric in the art of the West—they create their own history and conclude it with a clinical chapter outlining their "universal" nosological categories of hysteria, which they see as "valid for all countries, all times, all races."[52] Charcot and Richer begin by outlining the representation of possession in religious art from the early middle ages through the seventeenth century. They offer sixty-seven illustrations, often in line form, to provide visual proof of the continuity between the images of the Catholic mystic and the modern hysteric. Beginning with the fifth-century representation of possession in the Romanesque mosaics of Ravenna to images of Saint Catherine of Sienna, Charcot and Richer begin to build their case for the parallel (and therefore the universality) of their visual categories of hysteria.
The assumption is that there is an explicit continuity between Catholic religious experience, as represented by the practitioners, and the neurological pathologies of nineteenth-century France.[53] Thus the aesthetic representation of ecstasy becomes a clinical sign of psychopathology. Their movement is however not merely on the level of the equation of

The image of the possessed as the hysteric. From J.-M. Charcot
and Paul Richer, Les Dénoniaques dans l'art (Paris: Adrien Delahaye
et Emile Lecrosnier, 1887), p. 4.
Photo courtesy Wellcome Institute Library, London.
the religious-aesthetic and the clinical. For they cite one image (and text) from the general realm of medicine, and that is Sir Charles Bell's image of opisthotonus. The passage they quote is identical to the one cited above. Their argument is that the image of opisthotonus is parallel to a number of the images of possession that they offer, specifically the early seventeenth-century image of Saint Nilus by Domenicho Zampieri called Domenichino (1581-1641). Like their discussion of a sketch for the child in Raphael's Transfiguration , there is a stated assumption that the reality of the symptoms of hysteria are exactly parallel to the immutable reality of the symptoms of tetanus. In their final chapter, on the contemporary representation of the hysteric, Charcot and Richer draw on the images of the stages of the "hysterical convulsion" which Charcot had established in the 1880s. The parodies of religious experiences, from the position of prayer to the position of crucifixion find their visual representations in this chapter,[54] as does the classic arc-en-cercle position of the opisthotonus taken from Bell.[55]
What is most striking from the viewpoint of the history of the representation of the hysteric is that there is a continuity to the overall reception of the image of the hysteric which transcends the school of the

One of the topoi used to depict the history of the hysteric is this sketch
for the child in Raphael's Transfiguration . From J.-M. Charcot and Paul
Richer, Les Démoniaques dans l'art (Paris: Adrien Delahaye et Emile
Lecrosnier, 1887), p. 29.
Photo courtesy Wellcome Institute Library, London.
The self-crucified hysteric. From J.-M. Charcot and Paul Richer, Les
Démoniaques dans l'art (Paris: Adrien Delahaye et Emile Lecrosnier, 1887),
p. 100, lower image.
Photo courtesy Wellcome Institute Library, London.
Salpêtriére. Thus if we return to the British images taken from Arthur F. Hurst's study of hysterical contractures, we can see that Charcot and Richer, in citing images from Louis Basile Carré de Montgeron's account of the Jansenist miracles,[56] had already set the stage for the representation of the nonfunctional limb as a primary sign of hysteria. The link between the female and the victim of shell shock is made through the representation of the body part that makes them unable to be mobile in a society that demands mobility as a sign of group identity. The meaning ascribed to mobility from the eighteenth century to the twentieth century is quite different (the middle-class woman becomes a full member of the new religious sect when she is healed; the soldier returns to his fighting unit when he is healed). But central to the image of cure is the image of mobility. The visibly nonfunctional limb, with the alteration in gait or in posture, marks the hysteric as diseased. The images taken from the history of religion have already provided a model for the representation of the affected area as the target for healing. The analogy between the mentally ill and the enthusiastic and/or rigorous fundamentalism of religious schismatics such as the Jansenists had already been made by Philippe Pinel in the wake of the French Revolution. Citing a range of British sources in a French Catholic context, Pinel was forced to see the hypermoralism of the Jansenists as setting them apart from French society. He labeled them the pathological equivalents of the Methodists.[57] Charcot's citation of Jansenism as the central visual clue to the history of hysteria ties the image of the hysteric, not merely
The religious cure of the "hysteric." From Louis Basile Carré de Montgeron,
La verité des miracles operés par l'intercession de M. de Pêris et autres
appellans demontrée contre M. L'archevêque de Sens , 3 vols. (Cologne: Chez
les libraires de la Campagie, 1745-47), as reproduced in J.-M. Charcot and Paul
Richer, Les Démoniaques dans l'art (Paris: Adrien Delahaye et Emile Lecrosnier,
1887), p. 81.
Photo courtesy Wellcome Institute Library, London.
to "religion" but to the religion of spiritual excess, to religions such as Methodism and, in a specific manner that will be discussed below, to the mystical religion of the Eastern Jews.[58]
The religious rigidity and the enthusiasm of the Jansenists came to stand for the perversion of the spirit which was as pathological as the diseases of the hysteric. Paul Regnard brings a series of the attitudes passionnelles in his photographs of Augustine from the second volume of the Iconographie de la Salpêtriére .[59] These images mimic the positions of the Jansenists, but they are without doubt images of pathology. The parallels make both sets of images pathognomonic.[60] As with the images of the Jansenists, the images of the hysterics are closely associated with visual hallucinations, with the seeing of what is not there as a sign of the falsification of the imagination. William Hammond, in his 1876 history of hysteria, continued this "liberal" discourse of the Salpêtriére which associated disease and religion. He noted that "in these undeveloped forms of both diseases, as noticed among the Jansenist convulsionnaires, the affected individuals appeared as if struck by the sight of some object before unseen, and the contemplation of which filled them with the most ravishing joy."[61] Here the pathologization of seeing is the mirror image of the clinical gaze of Charcot, who sees the disease, the disease of the fantasy, the disease of religion.
Thus Charcot and Richer undertake what many scientists of the nineteenth and twentieth centuries do—to write the history of their own discovery in order to show its universality across time (if not across cultures). But this history of the representation of hysteria, drawing on the power of the new secularized religion of science in displacing its antecedent Christianity, becomes the model through which the hysteric is visually categorized. This tradition does not stop with Richer and Charcot. Students of Charcot's provide some of the later material. Henry Meige (after 1901 the editor of the Nouvelle Iconographie de la Salpêtriére ) and Jean Heitz both contribute essays to the Nouvelle Iconographie de la Salpêtriére on the artistic image of the hysteric well into the twentieth century.[62] Within the German tradition, the physician-historian-art critic Eugen Holländer incorporates many of these images in writing his history of the image of the impaired in classical art.[63] Holläinder quotes liberally from the same visual sources as Charcot and Richer—citing Raphael and the various images of religious possession. Jean Rousselot continues this image in his study of medicine in art into the post-World War II era.[64] His work begins with the representation of the Greeks, such as the Bacchic scene of "dying Bacchante," now in the Uffizi. He comments in his caption: "In point of fact, a depiction of hysteria. At

The representation of religious ecstasy as pathological sign. From
Paul Regnard, Les maladies épidémiques de l'esprit: sorcellerie magnétisme,
morphinisme, délire des grandeurs (Paris: E. Plon, Nourrit et Cie., 1887), p. 95.
The image is an engraving of a photograph taken from the Iconographie
de la Salpêtriée .
(Bethesda, Md.: National Library of Medicine.)
the far right, a hysterical woman, her body bent in the shape of an arc." All of these works assume a continuity of the meaning of the image of the hysteric from the ancient Greeks to their contemporaries. And all of them stress the continuity between the ancient representation of religious experience (rather than images of pathology) and modern experiences of disease (rather than religion). This asymmetry provides a powerful subtext for the association between images of religion and those labeled in the popular mind as being associated with categories constructed as or labeled as religious ones—such as the Catholic (or at least the Catholic cleric) and, in an equally complex manner, the Jew.
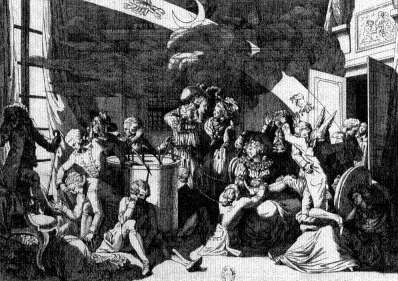
The "warfare between theology and science," to paraphrase the title of A. D. White's classic nineteenth-century study,[65] which is played out within the secularized Christian discourse of late nineteenth-century psychopathology, is nowhere more clearly evident than in Paul Regnard's 1887 monograph (with 120 images) on the visual relationship between magnetism, morphinism, and madness, which begins with the visual equation between the witch and the mad.[66] Regnard, a physician and the professor of physiology at the National School of Agronomy, was the coeditor (with Désire-Magloire Bourneville of the Bicêtre) of the original, three-volume edition of the Iconographie photographique de la Salpêtriére[67] as well as a well-received medical atlas.[68] His study of 1887, which is dedicated to "cher maitre," Charcot, assumes the interrelationship of all forms of mass hysteria. His first example is the witch. He provides a series of plates from Abraham Palingh's study of witchcraft to document the visual representation of the witch as the "grand hysteric."[69] In this context Regnard brings in other images of demonic possession from the Renaissance to the seventeenth century (p. 41), including—as one of the images that becomes standard to the repertoire of visual proof—the figure of the boy from Raphael's Transfiguration (P. 59).
It is assumed that these pathological positions are indicative of the association with other forms of possession, such as hysteria. To make this absolutely clear in the reader's eye, he reproduces, in the form of drawings which thus resemble the format of the earlier images he has reproduced, a series of photographic images from the Iconographie photographique de la Salpêtriére . Of these the image of the gaze, the hallucination as experienced by the observer rather than the hysteric, stands as the icon of pathology (p. 87). Regnard makes similar visual claims in associating the image of the hysteric with that of the sleepwalker, the drug addict, and the person suffering from monomania. Images are produced that draw on the visual association of abnormal states—there is
The image of the witch. From Abraham Palingh, 't Afgeruckt Mom-Aansight
der Tooverye: Daar in het bedrogh der gewaande Toverye, naakt ontdeckt,
en emt gezone Redenen en exemplen dezer Eeuwe aangewezen wort (Amsterdam:
Andries van Damme, 1725), p. 50, as used in Paul Regnard, Les maladies êpidémiques
de l'esprit: sorcellerie magnétisme, morphinisme, délire des grandeurs (Paris: E. Plon,
Nourrit et Cie., 1887), p. 19.
(Bethesda, Md.: National Library of Medicine.)
The representation of a visual hallucination, the centrality of the eye
and the gaze. From Paul Regnard, Les maladies êpidémiques de l'esprit:
sorcellerie magnétisme, morphinisme, délire des grandeurs (Paris: E. Plon,
Nourrit et Cie., 1887), p. 87.
(Bethesda, Md.: National Library of Medicine.)
always the assumption that there is a normal image of the productive, healthy human, and the deviant is marked by external signs, such as position, clothing, handwriting, and so on. These signs represent the symptoms of mental disorder, and all are interrelated because the signs are interrelated. But more than this is shown by moving from the witch (and the torture and cruelty inflicted on the witch [p. 33] to the miracles associated [as in Charcot] with healing the hysteric, to use his term [pp. 133, 135]. Religion and its hypocrisy, its antithetical relationship to the act of modern medical healing, are cited, and the cures of the church are ascribed to the nature of the disease entity—to hysteria. The cure of the disease of hysteria is the mass hysteria of religion. The model for this is the antiquated one of homeopathic medicine—like curing like. It is clear that Regnard, like Charcot and Richer, is looking for a more modern approach to therapy—to electrization or to the newly relabeled science of hypnotism—for their cure, not to religion. For the church, representing the institutionalization of religion in contemporary society, is the root cause of the hysteria, not its cure.
The other central model cited by Charcot and Richer in their scientific work is the model of the epileptic.[70] Stemming from Charcot's initial observations on his patients in the Salpêtriére showing the symptoms of "hystero-epilepsy" (his own composite category, which Freud borrowed), the visual image of the difference of the hysteric stems to no little degree from the tradition of representing the epileptic.[71] The image of the epileptic is in many ways parallel to that of the hysteric. Thus the "simulation" of the hysteric is paralleled by the "contradictions and exaggerations of sentiment [which] are salient characteristics of epileptics," according to Cesare Lombroso. He continues: "Epilepsy has a disastrous effect on the character. It destroys the moral sense, causes irritability, alters the sensations through constant hallucinations and delusions, deadens the natural feelings or leads them into morbid channels."[72] This need to see the pathological character of the epileptic as parallel to his or her disease is replicated in the visual image of the epileptic. While many of the visual images of the epileptic in the medical literature of the nineteenth century deal with the problems of localizing the brain lesion,[73] there is also a tradition of representing the symptoms of epilepsy through representing the patient. Charles Féré, in the Nouvelle Iconographie de la Salpêtriére , represents hysteria as literally written on the skin of the hysteric.[74] The parallel image is to be found in the representation of hysterical ulceration.[75] If one examines L. Pierce Clark's argument from 1898 that there are "tetanoid seizures in epilepsy," one can see the argument coming full circle to the organic model

The sensitive skin of the epileptic becomes a tabula rasa upon which
the disease can be inscribed. From Charles Féré, "Note sur un cas de
mélanodermie récurrente chez un épileptique apathique," Nouvelle
iconographie de la Salpêtriére , 10 N.F. (1897): 332-339.
(Bethesda, Md.: National Library of Medicine.)
of tetanus.[76] Indeed, the fascination with the marking of the signs and symptoms of disease on the body permeates the image of the epileptic in ways other than the search for the Jacksonian brain "lesion" that must necessarily cause the seizures.[77] Thus there are images of the malformed hands of an epileptic woman or of the corporeal asymmetry of the epileptic female.[78]
The image of the epileptic is also found within the tradition of representing the physiognomy of the insane. Thus William Alexander provides the reader with a photograph of each of the patients whose cases he reports in his 1889 study in order to present their physiognomy.[79] It is the visual appearance of the epileptic that provides the clue to his or her special, hidden flaw. The lesion must, in some overt way, write itself on the body. Some essays, such as on the baldness[80] or the altered appearance of the hair[81] of an epileptic man as a sign of his illness, are more than reminiscent of the extraordinary images of the "plinca polonica" or "Judenkratze," the fantasy skin disease attributed by Western dermatologists to the Jews of the East. In some of the recent historical literature on the history of epilepsy, much of the same tradition cited by Charcot and Richer reappear—now in the context of documenting the ongoing history of epilepsy. Thus images of religious ecstasy and possession from the early Middle Ages appear as precursors of the image of the epileptic.[82]
All of these images relate to the idea of the hysteric as continuous over time and across cultures. This is the basic assumption of the definition of a positivistic disease entity at the close of the nineteenth century. Disease is real only if it is universal. And it is universal only if it can be seen and the act of seeing reproduced. This latter axiom is rarely stated (except by the head of the Salpêtriére's photographic service, Albert Londe), but it is assumed. Thus the image of the impaired patient is the touchstone for the reality of the disease.