| • | • | • |
Sakalava Perceptions of Possession and Madness
In Ambanja, when mediums and other informants describe possession they sometimes compare it to madness (adala, adalan̂a; also, marary saina,very saina/jery, “sick” or “lost mind”). Even though possession and madness are regarded as distinct categories of experience, they overlap somewhat in their causation, symptomatology, and treatment. According to Sakalava informants, possession and madness define a spectrum of symptoms where severity is an important distinction. In this model, tromba possession and madness occupy opposite poles, and possession sickness falls somewhere in between (see figure 10.1). This spectrum of experiences ranges from a good, powerful, and inescapable state to a destructive, dangerous, and frightening illness.
Tromba possession is distinct in that it is an accepted form of behavior and experience, involving periodic changes in personality, dress, and other characteristics as the medium moves in and out of trance. Although tromba spirits periodically may cause harm to a medium—making her sick if they are angry, for example—they are generally regarded as sacred, powerful, and beneficial entities that look after the medium, her kin, and her clients.
Njarinintsy, masoantoko, shay-tuan and bilo are evil, reckless, and uncontrollable spirits. Since they simultaneously are forms of spirit possession and sickness (marary), they occupy a position somewhere between tromba and madness. As described in chapter 9, a njarinintsy, for example, is a generic spirit that has no personal name. Although it possesses and controls the body of its victim, this (as well as other forms of possession sickness) is temporary, and it is regarded as a special form of illness that ceases when the spirit is driven from its victim. During fits of possession a victim may be described as being temporarily mad, suffering from a “sick mind” or “sick spirit” (marary saina) because she periodically and uncontrollably shouts obscenities, attacks people, or wanders aimlessly through the streets. If the harmful spirit(s) is not driven from the victim it may have long-lasting effects, ultimately driving her permanently insane or even killing her.
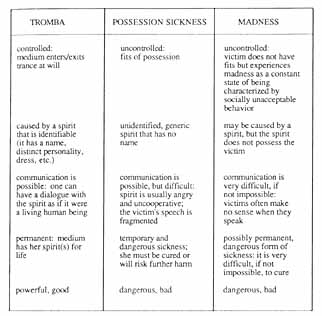
10.1. Characteristics of Possession and Madness (Sakalava interpretations).
Madness is a general illness category defined very broadly by more serious forms of deviant behavior which are fairly constant and long-term. Madness is a frightening problem, for, as an extreme illness category, it is very difficult to cure. It is defined in reference to possession, but it is not the same. Madness may be caused by an angry spirit, brought upon its victim by a tromba because she is resisting possession, or by a malicious spirit, such as a njarinintsy, which has been allowed to stay too long within her. One of the primary problems with madness, however, is it does not necessarily result from a foreign entity that actually resides in the victim. The intangibility of the problem is part of what makes it extremely difficult to treat.
Possession offers other clues for understanding Sakalava conceptions of madness. Whereas tromba is good (tsara) and sacred (masina), madness, like possession sickness, is bad (raty). Communication is also an important factor in distinguishing these categories from one anther. Tromba spirits have full-fledged personalities that enable them to converse and interact with the living. The speech of njarinintsy and similar spirits, on the other hand, is angry and garbled. The mad occupy the other polar extreme: they speak nonsense and this is a constant state for them, unlike the fits that characterize possession sickness.
Although madness may sometimes be confused with possession sickness (especially at onset), it is a distinct category because it is viewed as an extreme and potentially permanent state of being. In Ambanja there were two individuals who were often seen in public places and who were labeled as mad (adala, adalan̂afa). One was an Antandroy man who wore women’s clothing and who carried a stick, which he would swing at passersby. The second was a Comorean woman who, even though she had kin in town, preferred to sleep outside and eat out of garbage heaps. In contrast, the behavior of a victim of possession sickness may be very odd or frightening, but after a fit has ended she appears normal and does not remember what happened. The significance of the breaking of social norms in labeling the mad is evident in the manner in which the diminuitive term adaladala is applied. It is used, in a teasing way, to describe anyone who acts odd or silly. As the following story illustrates, a person must be seriously ill to be called adala or adalan̂a.
The Case of Victoria
One of the more spectacular public displays of njarinintsy violence that I witnessed occurred one afternoon on the main street of Ambanja. As this case illustrates, the application of the label of possession sickness became increasingly problematic, eventually leading those who knew Victoria to relabel her as mad (adalan̂a).
One afternoon I was standing in line in the Peasant’s Bank. Suddenly all three bank tellers ducked behind the counter just as a rush of water flew through the air and hit a crowd of people to my right. I spun around and saw a woman in her thirties standing on the veranda. It was my neighbor Victoria, who often suffered from attacks of njarinintsy. She was soaking wet, holding a bucket in the hand of her limp right arm, and she had a faraway stare. I also noticed that she had one black eye. An older woman started to yell at Victoria, telling her to get away from the bank and leave her alone. Instead, Victoria suddenly made another rush for the interior of the bank, threatening the woman with her empty bucket, waving it in her direction as if to pitch more water on her. Two young men escorted the older woman out, and Victoria, after wandering around the bank for a minute or two longer, departed, walking aimlessly, as if drunk, down the main street and past the post office. The three bank employees, giggling nervously, peered out from under the counter and, then, cautiously, stood up and continued their work. When the older woman was out of sight two customers explained to the rest of us in line that the woman whom Victoria was aiming for was her nasty (masiaka) mother-in-law.
Victoria had been plagued by njarinintsy for over a year; as she told me once, “I suffer too much” (Izaho mijaly loatra). She could often be seen wandering through the streets of Ambanja, wailing and crying, and she argued on a daily basis with her spouse and his kin. Within the last three months her fits of possession happened so frequently that some of my neighbors joked that you could tell the time of day by when Victoria would wander by. Others were disturbed by her behavior: as an old schoolteacher of hers sadly explained, these days it was more common to see Victoria in a possessed state than out of one. He and others stated that njarinintsy should not be like that—generally the victim has fits and then she is fine, but Victoria always seemed to be possessed. One of her friends speculated that perhaps Victoria had been sick for so long from njarinintsy possession that it had started to drive her insane (adalan̂a), that she had started to lose her mind (very jery).
All who knew Victoria agreed that her story was very sad (mampalahelo). Victoria was Sakalava from a nearby village. After completing two years of high school she had met her (common law) husband, who was a truck driver for a northern transport company, and she dropped out of school to accompany him to Diégo where he lived. She had been a gifted student and soon found work at a local business as a bookkeeper. Victoria had always hoped to finish her studies at the private French School there, something that her husband had promised he would help her do if she came to live with him. But ten years later and after having had three children, she was still working long hours. She still dreamed of learning more French and studying Italian. Two years ago her husband had lost his job and he had insisted that they return to Ambanja, a town she hated. There had been much tension (and violence) in her marriage during the last four years. This had increased within the past eighteen months, after her husband had learned that she had secretly had an abortion. As a neighbor explained: “Her husband became very angry with her, and he beat her on and off for several days. The noise was terrible!…Two neighbors had to go to the house to stop him.…Now her mother-in-law is angry at her, because she won’t do anything she is told.”
At this point the attacks of njarinintsy began. Her in-laws took her to two healers, but neither succeeded in driving the spirit(s) from her. They then summoned Victoria’s mother and sister, who lived in a village thirty kilometers from Ambanja. As Victoria’s sister later explained, they took her to a series of expensive healers, but all were unable to encourage a spirit of any kind to speak. Even when a kalanoro made all sorts of promises to leave very expensive items at a sacred spot for the spirit to consume, the only signs that Victoria was troubled by spirits were that she would sob uncontrollably and thrash about on the floor during the healing sessions. Her kin had become increasingly worried, because now they were not sure how to cure (mitaha) Victoria. Her mother and sister went home, leaving her in her husband’s care.
Two nights after the episode in the bank Victoria struck again. She had wandered aimlessly into a bar where her husband was drinking with his brother, some friends, and two women reputed to be prostitutes. As the proprietor later explained in disbelief, Victoria had suddenly rushed behind the bar, grabbing bottles of expensive imported whiskey and rum and smashing them on the floor. Her husband jumped up and grabbed her, dragged her out into the street, and then he began to pound her with his fists. His brother and two other men finally stopped him, and Victoria was escorted home. The next day her in-laws again summoned Victoria’s mother and sister, and told them to take her home to their village. By this time everyone who knew Victoria was certain that she was not sick with possession sickness but was insane. Within the week her sister and mother came from their village and, after spending the night, they took her to the provincial hospital in Diégo. I later learned from her sister that Victoria had spent one month in the asylum and that she was now “quite content [tamana] living by herself in Diégo.…She has not suffered from an attack since we brought her there.”
Victoria’s story reveals how kin, as well as members of the community at large, were actively involved in assessing Victoria’s problem and, ultimately, relabeling it as madness rather than possession sickness. Several factors led to this reassessment of her condition. First, her fits were not short-lived, but instead had begun to dominate her life—to see her out of a possessed state had become an unusual event. The level of violent behavior was typical of njarinintsy, but the frequency of her unusual social misconduct led others to believe that it was more than this. Even the most gifted healers of the region could not drive any spirit from her. Furthermore, if she had a spirit, it was odd that it would never talk, even in fragmented speech. The decision to take Victoria to the asylum was one of last resort, only after the efforts of a series of indigenous healers had failed.
The Limitations of Clinical Medicine
As Victoria’s story illustrates, clinical medicine (and, more specifically, psychiatry) provides one option of last resort for extreme cases of possession and madness. The choice to go to the psychiatrist or the exorcist is a personal matter and the actions of patients and their kin reveal no particular trend of favoring one over the other. More often, however, patients leave the asylum for the exorcists, rather than the other way around.
As I have argued elsewhere (Sharp, in press), the efficacy of psychiatric medicine in northern Madagascar is hampered by a multitude of factors. Problems in part result from a reliance on drug therapy in a country where prescribed medications are often unavailable in local pharmacies (cf. Sachs and Tomson 1992; Vogel and Stephens 1989; for contrast see Lee et al. 1991; Silverman, Lee, and Lydecker, 1986; and Silverman, Lydecker, and Lee, 1990). The practice of isolating patients from kin while they are in the asylum also runs contrary to indigenous therapeutic practices.[3] In turn, as others have argued (Zola 1978; see also Dunk 1989; Lock 1984; Ong 1988; Pappas 1990), the medicalization of disorder often empowers the doctor while silencing the patient. To quote Taussig (1980b: 8), this leads to “the alienation of the patient’s self-understanding and capacity” to articulate the causes of her suffering. In Madagascar, a reliance on Western-derived clinical approaches means that the psychiatrist and patient have radically different perceptions of illness. In essence, they suffer from what I have referred to as “conflicting epistemological realities” that block treatment.[4] Clinical medicine denies the legitimacy of the subjective experience of possession.
Ethnic differences between patients and clinicians are also significant. Malagasy doctors working in the north are generally strangers to the region and rarely see possession (or know that a patient is possessed). Several factors account for this: some informants stated that it is taboo (fady) for njarinintsy victims, for example, to receive injections, and mediums are generally reluctant to mention their spirits to doctors for fear of being ostracized. Also, Sakalava—regardless of whether or not they have spirits—generally avoid clinics because they do not want to come into contact with Merina doctors.
As this chapter will show, exorcism is likewise an extreme choice of therapy, yet a few Sakalava opt for it because it offers powerful alternatives for those who have endured great suffering. Even though exorcisms are painful and frustrating for patients, exorcists are successful healers because they first accept and then transform the patient’s explanations for and experiences of possession and madness. During Protestant healing rituals possession is viewed as an appropriate idiom for describing illness, and madness is redefined as normative, not deviant, behavior. Ultimately this approach carries significant implications for the empowerment of both the patient and the healer and it may lead to a permanent transformation of the patient’s identity.