The Matrix
The development of a matrix helps to illustrate the interrelationship between public policy and innovation. In figure 3, the stages of the innovation continuum (from discovery to distribution) are on the horizontal axis. The two identified types of public policy (promote or inhibit) appear on the vertical axis.
Each box in the matrix contains examples of policies that reflect the coordinates. Thus, policies in box 1 promote innovation at the stage of discovery, and policies in box 4 inhibit innovation at the distribution stage. The matrix provides the organizing framework for the discussion in subsequent chapters.
Chapter 2 chronicles the evolution of innovation in the private sector and the preconditions for subsequent policy interventions. In the first half of this century, medical device technology and government institutions were quite independent and engaged in little meaningful interaction. Yet there were signs of change. Technological development was taking place in the private sector, and inventors overcame significant barriers to produce
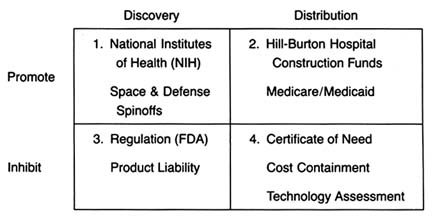
Figure 3. The policy matrix.
a variety of innovations. Public attitudes about the government's role in the innovative process underwent important and perceptible shifts, and public institutions were established that later would play pivotal roles in the device industry. Interaction came later. In terms of both technology development and government policy, World War II provided the transition to the modern environment.
Part II (chapters 3 through 8) follows the chronology of the boxes in the matrix. Policy trends are easily identified, as the numbers reflect the last four decades. In general, the policies of the 1950s (box 1) were dominated by promotion of innovation at the discovery stage, and the 1960s (box 2) saw promotion at the distribution stage, with consequent benefits for both discovery and distribution. The 1970s and 1980s did not completely reverse these trends, in that the policies initiated earlier continued. However, new concerns led to efforts to inhibit innovation. In the 1970s (box 3), significant efforts to increase regulation inhibited discovery; in the 1980s (box 4), concern about cost containment led to policies to inhibit product distribution. The chronology is not exact because some of the regulatory antecedents appeared before the policies were enforced. (The FDA had authority to regulate medical devices as early as 1938; the extension of authority with regulatory teeth, however, came in 1976.)
Subsequent policies did not replace earlier ones. Rather, policies were layered one on top of the other, so that public policy affected innovation at every step. To help us understand the proliferation of policies, each intervention is discussed in relation to the politics of its creation and evolution, the interest groups involved, the goals of the policymakers, and the changes over time.
Each chapter in part II relates to a box in the matrix presented in figure 3. Chapter 3 addresses how government policy promotes discovery (box 1). The NIH is the primary federal organization charged with supporting biomedical research, which has been accomplished through grants to researchers, primarily in universities. Some recent initiatives, most notably the Artificial Heart Program (AHP) at NIH, which is modeled on the experiences of the space program, have targeted specific device technologies. Additionally, chapter 3 looks at government sponsored research in space and defense that has had some interesting effects on medical device technology. Also discussed are recent political efforts to realign the key research institutions—universities, government scientists, and the industry—so that medical technology is transferred from the basic science of the laboratory into the hands of product producers. The chapter evaluates these three initiatives in relation to the medical device industry.
Chapter 4 focuses on policies that promote distribution (box 2). Public policy has played a pivotal role in shaping the size and the composition of the medical device market. Federal and state governments have developed a complex set of policies to pay for health care services. After years of disinterest in health services, federal spending on the growth of the hospital infrastructure began after World War II. Chapter 4 describes how the public role expanded significantly with the enactment of Medicare and Medicaid in the 1960s. The primary health policy goal undergirding public payment is to increase access to health care for those previously excluded, including the elderly, the disabled, and the indigent. Although these programs did not directly address the medical device industry, their impact on that industry was dramatic. Government programs continue to inject billions of dollars into the medical marketplace every year, and
medical technologies are a primary beneficiary. The design of these payment policies dramatically and idiosyncratically affects the size of the market for particular medical technologies.
A few examples illustrate the point. According to some estimates, in 1982 the government paid for over 41 percent of all medical expenditures.[30]
U.S. Department of Commerce, Bureau of the Census, Statistical Abstract of the United States, 1985 (Washington, D.C.: GPO, 1984), table 143.
The payment structure favored hospital based technologies over nonhospital products. Intensive care units, full of new life-support and monitoring equipment, were virtually unknown in 1960; in 1984, they accounted for 8 percent of all hospital beds. Congress extended Medicare coverage for all end-stage renal disease (ESRD) patients in 1972. Kidney dialysis, virtually nonexistent in 1960, was used by 80,000 patients in 1984 at a cost to the government of $1.8 billion.[31]U.S. Congress, Office of Technology Assessment, Federal Policiesand the Medical Devices Industry (Washington, D.C.: GPO, October 1984).
The 1970s brought a new set of concerns to the policy arena—primarily product safety. Chapter 5 explores how the government inhibited discovery of medical devices through safety regulations (box 3). Regulation of medical devices is the primary vehicle for reducing risks of adverse reactions to these products. The federal government and, to a lesser extent, the states have recognized that certain medical products present unacceptable risks and require government intervention through safety and efficacy regulation.
Food and drug regulation dates back to the turn of the century. Congress extended the jurisdiction of the FDA to cover medical devices in 1938; the FDA acquired significantly more extensive regulatory powers under the 1976 Medical Device Amendments to the Federal Food, Drug, and Cosmetic Act, one of the many pieces of consumer protection legislation of the 1970s. The stated goal of these amendments was to "provide for the safety and effectiveness of medical devices intended for human use."[32]
Preamble to Medical Devices Amendment, Public Law 94-295, 90 Stat. 539.
The FDA's jurisdiction is over producers, and its regulations affect firms at the development stage. Cardiac pacemakers and intrauterine devices (IUDs) are used in this chapter to illustrate the impact of regulation on device technology. Because the law focuses on perceived risks associated with medical devices, the riskier the product, the more likely it will encounter the inhibiting forces of the FDA.Chapter 6 continues the discussion of policies that inhibit device discovery (box 3). Although it has antecedents in early
common-law rules, there was an explosion in product liability suits in the 1970s. Product liability seeks to inhibit the manufacture and use of devices if they are determined to be unsafe. However, state courts use completely different tools from FDA regulators to accomplish this substantially similar goal. Liability law in general has a less well-recognized, but clearly related, health mission. Its goal is to compensate individuals injured by defective products and to deter others from producing harmful products. It functions as a part of the health care system in that income to pay for medical costs, as well as noneconomic damage, is transferred from the producers of products to the consumers of products. It is essentially a form of insurance coverage for risk. The law includes both a compensatory and a safety function. The product liability system applies to all consumer products; medical products are included in this broad net. Product liability law, in terms of both the costs and availability of insurance and the consequences of lawsuits, can have a significant, indeed a crippling, impact on some producers.
Chapter 7 analyzes the series of recently imposed mechanisms that inhibit distribution of medical devices (box 4). These policies focus on cost containment rather than on safety, though some seek to control costs through evaluation of product quality. Concern about health care costs in the 1970s and 1980s has affected the momentum of federal and state payment programs. Efforts to restructure the system to control costs have had substantial effects on some segments of the medical device marketplace. Cost-containment strategies began with state based Certificate of Need programs and expanded to a variety of cost-control forms through technology assessment mechanisms. The goal of assessment processes is to ensure that only the "best" technologies are distributed—other technologies should be abandoned. Chapter 7 focuses on federal efforts to institutionalize technology assessment beyond the existing policymaking bodies. In addition, the new payment system under Medicare, known as the Prospective Payment System (PPS), was instituted to control the wildly escalating costs of Medicare. This program has created a new set of idiosyncratic effects on medical device technology.
Chapter 8 introduces the emerging issues of a global marketplace. These issues do not appear within the matrix because it is
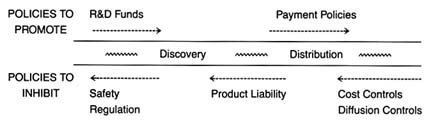
Figure 4. Policies affecting medical device innovation.
unclear whether the international market and the policies of foreign governments regarding medical technology will help domestic medical device producers (that is, promote distribution) or pose a competitive threat to domestic producers (that is, inhibit distribution). Through a brief look at three major markets—Japan, the emerging European Community, and China—these challenges will be assessed.
Part III provides a prognosis. Returning to the innovation continuum, the discussion in chapter 9 falls into three sections (figure 4). The first analyzes the present policy environment at both the discovery and the distribution stages, with illustrations of creative industry strategies that respond to policy incentives. The second section discusses pending policy reforms and their possible effect on the flow of new products. The third section discusses interactions among the various policies that are the inevitable consequences of policy proliferation. Some ways to improve the policy process are discussed.
Chapter 10 looks to the future. The contributions of medical devices to the fight against disease have been critical. However, there are dangers posed by misuse and overuse. The medical arms race must be managed with an understanding of the economic, political, and moral dimensions of medical technology.
The development and application of an analytical framework to the medical device industry only scratches the surface. Further empirical work is necessary to improve our understanding of medical technologies, of the process of innovation, and of the impact of government institutions on the private sector. It is hoped that the issues raised in this book will encourage this research. We must strive for rational policy reform grounded in an understanding of the values and goals of our health care system.
Finally, this study makes clear that policy proliferation is inherent in our political system and reflects the complexity of technology. The system has many benefits, but it also has costs and limitations. It is useful to step back and view the whole landscape to observe the dynamic interactions between the public and the private sectors. In the case of our patient—medical devices—reform may indeed be a matter of life and death.