Part I
THE VIRUS AND ITS PUBLICS
Aids and Beyond:
Defining the Rules for Viral Traffic
Stephen S. Morse
The lesson of AIDS demonstrates that infectious diseases are not a vestige of our premodern past; instead, like disease in general, they are the price we pay for living in the organic world. AIDS came at a time of increasing complacency about infectious diseases. The striking successes achieved with antibiotics, together with widespread application of vaccines for many previously feared viral diseases, made many physicians and the public believe that infectious diseases were retreating and would in time be fully conquered. Although this view was disputed by virologists and many specialists in infectious diseases, it had become a commonplace to suggest that infectious diseases were about to become a thing of the past and that chronic, noninfectious diseases should be our major priorities.[1]
Donald A. Henderson, M.D., Dean Emeritus, School of Public Health, Johns Hopkins University (personal communication, 1989) recalls a speech at Johns Hopkins University in 1969 in which the surgeon general of the United States Public Health Service, expressing the optimism typical of this period, assured his audience that infectious diseases were now of marginal interest in the United States and that we should thus shift our focus of attention to the chronic diseases.
Rudely jolted back into an awareness of infectious diseases by AIDS, we now find ourselves in a period of great uncertainty, poised for the AIDS of the future. We cannot help but wonder what other catastrophes are waiting to pounce on us. In this essay I consider what we now know about the "AIDS of the future." In particular, I discuss the origins of "new" viruses and the question of whether their emergence can be anticipated and prevented.[2]Emerging viruses and viral evolution were the subject of a conference that I chaired in May 1989 ("Emerging Viruses: The Evolution of Viruses and Viral Diseases"), the first ever held on this subject. One purpose of the conference, which was sponsored by the National Institutes of Health with The Rockefeller University, was to unite historical, epidemiological, and molecular approaches. I am editing a book containing contributions by the participants. Several popular summaries of this conference have recently appeared; see, for example, Julie Ann Miller, "Diseases for Our Future," BioScience 39 (1989): 509-17. For a more technical summary, see Stephen S. Morse and Ann Schluederberg, "Emerging Viruses: The Evolution of Viruses and Viral Diseases," Journal of Infectious Diseases 162 (1990): 1-7.
I argue that AIDS and HIV are novel but that biological antecedents and parallels can be found in nature. The novelty of AIDS therefore probably reflects our imperfect knowledge of the natural world rather than a diabolical new development in viral evolution. It is of note, though, that the conditions favoring rapid dissemination of the virus were comparatively recent social developments of great importance. In essence,
I thank Dr. Richard L. Landau, editor, and the University of Chicago Press for their permission to reprint this essay, which appeared in modified form in the journal Perspectives in Biology and Medicine (34 [Spring 1991]: 387–409, © 1991, The University of Chicago) under the title "Emerging Viruses: Defining the Rules for Viral Traffic."
I also thank Dr. Daniel M. Fox for many helpful comments on this essay, especially on viral traffic and its implications. Many of the examples presented here were drawn from examples discussed at the conference "Emerging Viruses: The Evolution of Viruses and Viral Diseases" (see note 2 below). Special thanks to Dr. John R. La Montagne, Director, Division of Microbiology and Infectious Diseases, and Dr. Ann Schluederberg, Virology Program Director, National Institute of Allergy and Infectious Diseases of the National Institutes of Health; to Drs. Frank Fenner (Australian National University), Dennis M. Stark (The Rockefeller University), S. Gaylen Bradley (Medical College of Virginia), Paul J. Edelson (Cornell University Medical College), and Pravin Bhatt (Yale University School of Medicine); and to the speakers and members of the organizing committee of the conference on emerging viruses for their enthusiastic and generous response, including their sharing of unpublished data. I am grateful to historians Marilyn Gewirtz, Daniel J. Abrams, Daniel M. Fox, Mirko D. Grmek, and Edward Tenner for helpful discussions on historical approaches. Research in my laboratory is supported by grant RR 03121 from the National Institutes of Health, DHHS.
they served as highways to expedite "viral traffic," from animal sources to humans and from small or isolated human populations to larger groups. This "viral traffic," as I call it, is central to the origin of most epidemics of viral disease. Most "new" or "emerging" viruses are the result of changes in traffic patterns, which give viruses new highways. Perhaps most important, human actions often precipitate viral emergence. Apart from such obvious human factors as the role of behavior in HIV transmission, many episodes of emergence have been the result of agricultural or environmental changes brought about by human intervention. We therefore bear greater responsibility for emergence, and may have greater ability to influence it, than has been supposed.
The emphasis placed by scientists and the public on the diversity of viruses—of which the stress on the novelty of HIV is one example—may have made us oblivious to these recurrent patterns and common features shared by many emerging viruses. Most "new" viruses are of zoonotic (animal) origin and are not really new; instead, they are existing viruses that have been given new opportunities or new settings.[3]
This point has also been discussed in a very readable essay by Edwin D. Kilbourne, "Are New Diseases Really New?" Natural History 92 (December 1983): 28-32.
Viral evolution, while a fascinating phenomenon to scientists, has generally been less important per se as a mechanism of viral emergence than this transfer of existing or slightly modified viruses to new hosts. The optimistic message is that the possibly unpredictable path of viral evolution need not necessarily be fully charted before we can anticipate new diseases like AIDS. The central problem concerns the changing relationships between viruses and human society, reflecting changes in relationships between humans and their environment.In this regard, focusing on the uniqueness of AIDS has tended to obscure the many features that this virus shares with other viruses.[4]
See Howard M. Temin, "Is HIV Unique or Merely Different?" Journal of Acquired Immune Deficiency Syndromes 2 (1989): 1-9.
AIDS is unquestionably unusual, and its viral cause, human immunodeficiency virus (HIV), has many novel features. Nothing in our knowledge of viral disease prepared us for the unique features of AIDS. Much was known about interactions of viruses with the immune system, but a virus that caused human disease by depleting the cells responsible for specific immunity was unprecedented. AIDS was also one of the few documented examples of what appears to be a truly new virus entering the human population to cause a previously unknown disease (but see below). Most notably among its unusual properties, HIV has a predilection for T lymphocytes (and other cells) bearing the surface protein called CD4 (or T4). Various types of T lymphocytes are responsible for orchestrating and regulating all immune responses, as well as for carrying out certain types of immune functions known collectively as cell-mediated.Their roles are determined by specific proteins on the cell surface, which serve as recognition markers. T lymphocytes bearing the CD4 protein, colloquially known as "T4 cells," are generally responsible for turning on and amplifying immune responses. Without these CD4+ T cells, the body is unable to mobilize an immune response, so that the host becomes vulnerable to the opportunistic infections that are the hallmark of AIDS.
As was shown several years ago, the predilection of HIV for CD4+ T cells is due to the fact that the CD4 protein is a receptor for the virus.[5]
Angus G. Dalgleish et al., "The CD4 (T4) Antigen Is an Essential Component of the Receptor for the AIDS Retrovirus," Nature 312 (1984): 763-67; David Klatzmann et al., "T-Lymphocyte T4 Molecule Behaves as the Receptor for Human Retrovirus LAV," Nature 312 (1984): 767-70; P.J. Maddon et al., "The T4 Gene Encodes the AIDS Virus Receptor and Is Expressed in the Immune System and the Brain," Cell 47 (1986): 333-48.
That is, the virus enters T cells by attaching specifically to CD4 on the cell surface. Other viruses have specific receptors; what made HIV tragically unique was that its receptor was CD4 rather than some other protein on the cell surface. This allowed HIV access to the CD4+ T cell that is so crucial in the immune response. However, for reasons to be discussed, it seemed improbable that the property of infecting and killing CD4+ cells would be found in only one virus and not in any of its relatives.[6]It is hypothetically possible that a particular virus could be the only surviving member of an extinct group possessing a distinctive characteristic (in which case one might be forced to conclude that the characteristic would not have been of much survival value to the virus); however, the tendency in nature is usually the opposite: vestigial characteristics are often retained long past any apparent utility. Virtually nothing is known about viral "extinction," or even whether it occurs, except for the intentional case of smallpox. On the other hand, it is also possible, and actually not improbable, that a new characteristic could arise as a small change by mutation from an existing virus. Thus, CD4 tropism of HIV could have arisen by a fortuitous mutation in the env (viral envelope) protein required for attachment to the appropriate cell receptor for virus entry; such a mutation would enable the protein to attach to CD4 on cells. This was the view originally held by many people, including many virologists. Although HIV itself did not arise this way, for the very reasons discussed, one would suppose that an ancestor of HIV could have arisen in this fashion. Howard M. Temin has discussed the role of mutation; see "Is HIV Unique or Merely Different?" (referred to in note 4) and "Evolution of Cancer Genes as a Mutation-Driven Process," Cancer Research 48 (1988): 1697-1701. Alternatively, the virus could conceivably have acquired the capability for CD4 binding by picking up a host cellular gene for this property; retroviruses are well known for their propensity to exchange genetic information with host cells. It is hard to make any predictions about how important mutation is as a way of generating new viruses. My personal feeling is that, for statistical reasons, it is less important in human disease. Ours is only one of many mammalian species, and many other species are more numerous; if there is a finite probability of the critical step's happening in any particular species, the numerical chance of its happening first in humans is therefore compatatively small. However, such an event could someday happen, although perhaps at a lower frequency than would suit our own anthropocentrism.
Thus, the discovery of this mechanism led to a search, ultimately successful, for other examples of viruses that infect or kill CD4 T cells. HIV belongs to the Lentivirus subfamily of retroviruses. One might expect that relatives of HIV among other lentiviruses would behave similarly; indeed, Luc Montagnier has pointed out that most, if not all, primate lentiviruses have a predilection for CD4+ lymphocytes of their hosts.[7]Luc Montagnier, "Origin and Evolution of HIVs and Their Role in AIDS Pathogenesis," Journal of Acquired Immune Deficiency Syndromes 1 (1988): 517-20.
In addition to these, some lentiviruses of other species, such as the bovine and feline immunodeficiency viruses, also appear to attack similar targets in their respective species.[8]Matthew A. Gonda et al., "Characterization and Molecular Cloning of a Bovine Lentivirus Related to Human Immunodeficiency Virus," Nature 330 (1987): 388-91; Niels C. Pedersen et al., "Isolat on of a T-Lymphotropic Virus from Domestic Cats with an Immunodeficiency Like Syndrome," Science 235 (1987): 790-93. These viruses were all characterized after the discovery of the CD4 tropism of HIV as researchers became alerted to the possibility that related viruses with this property might exist. The example of mouse thymic virus, discussed below, was the first case of an unrelated virus shown to cause a similar effect.
But the ability to infect and kill CD4+ T lymphocytes may not even be unique to retroviruses. Herpesviruses are DNA-containing viruses unrelated to HIV. In my laboratory we have found that a mouse herpesvirus, mouse thymic virus (MTLV; murid herpesvirus 3), can specifically kill CD4+ T lymphocytes developing in the thymus of young mice.[9]
Stephen S. Morse and Jay E. Valinsky, "Mouse Thymic Virus (MTLV): A Mammalian Herpesvirus Cytolytic for CD4+ (L3T4+) T Lymphocytes," Journal of Experimental Medicine 169 (1989): 591-96. The virus has been known since 1961. Rather than suggesting a common evolutionary relationship with HIV, which seems unlikely, this similarity probably indicates that unrelated organisms can evolve similar ways to go about a particular process. This apparent convergence is likely due to such limitations of the viral life-style as dependence on host cells.
T cells not possessing CD4 are not affected. Recent reports suggest that the recently described human herpesvirus 6 (HHV-6; also called HBLV) is probably T lymphotropic as well.[10]Dharam V. Ablashi et al., "HBLV (or HHV-6) in Human Cell Lines," Nature 329 (1987): 207; Carlos Lopez et al., "Characteristics of Human Herpesvirus-6," Journal of Infectious Diseases 157 (1988): 1271-73. HHV-6, although cytolytic for CD4+ T cells, probably does not enter the cell via a CD4 receptor.
In cell culture at least, HHV-6 can infect and kill cells bearing CD4.[11]Ablashi et al., "HBLV (or HHV-6) in Human Cell Lines."
Despite these worrisome properties, these viruses have never been associated with AIDS-like disease and are probably not responsible for any serious illnesses in mice or humans, although HHV-6 has been suggested as a possible cofactor for AIDS.[12]S. Z. Salahuddin et al., "Isolation of a New Virus, HBLV, in Patients with Lymphoproliferative Disorders," Science 234 (1986): 596-600.
The mouse virus does not appear to cause overt disease, even though individuals remain infected for life and chronically secrete virus, probably from T lymphocytes.[13]Wallace P. Rowe and Worth I. Capps, "A New Mouse Virus Causing Necrosis of the Thymus in Newborn Mice," Journal of Experimental Medicine 113 (1961): 831-44; Sue S. Cross et al., "Biology of Mouse Thymic Virus, a Herpesvirus of Mice, and the Antigenic Relationship to Mouse Cytomegalovirus," Infection and Immunity 26 (1979): 1186-95; Stephen S. Morse, "Mouse Thymic Necrosis Virus: A Novel Murine Lymphotropic Agent," Laboratory Animal Science 37 (1987): 717-25, and "Mouse Thymic Virus (MTLV; Murid Herpesvirus 3) Infection in Athymic Nude Mice: Evidence for a T Lymphocyte Requirement," Virology 163 (1988): 255-58. This does not rule out more subtle effects; we have recently found an association with autoimmune disease.
The human virus seems to cause roseola,a mild childhood disease, and may be one of the commonest of all human viruses.[14]
K. Yamanishi et al., "Identification of Human Herpesvirus-6 as a Causal Agent for Exanthem Subitum," Lancet 1 (1988): 1065-67; Lopez et al., "Characteristics of Human Herpesvirus-6."
I shall say more about HHV-6 later. We do not know why, unlike HIV, these apparently T lymphotropic infections rarely if ever cause severe disease and do not appear to result in AIDS-like syndromes. Although they might someday become the cause of new AIDS-like diseases, that is unlikely; in distinction to HIV, these viruses were probably in their respective host species for many generations and appear well adapted to their hosts.The lesson from such findings is that infectious agents do not develop in a vacuum but are the result of an ongoing evolutionary process. Most life forms existing today evolved from organisms already in existence, and viruses appear to be no exception. Appearance of viruses de novo seems extremely rare, for the same reasons that other species rarely arise de novo . Thus, "new" viruses are likely to come from existing viruses, and, in general, viruses of today have antecedents and relatives. In a sense, viruses have "parents" just as we do. As Luc Montagnier put it, "We're boarding a train that's already in motion. New species aren't being created. We're seeing the old ones evolve."[15]
Interview with Thomas Bass, Omni 11 (1988): 102-6, 128-34; remark quoted, p. 130.
It has taken us a long time to assimilate this lesson, and I am not sure that even now we fully grasp its implications. In the words of Joshua Lederberg, "the historiography of epidemic disease is one of the last refuges of the concept of special creationism."[16]Personal communication; see also note 2 above. For other comments by Lederberg on this subject, see Joshua Lederberg, "Medical Science, Infectious Disease, and the Unity of Humankind," Journal of the American Medical Association 260 (August 5, 1988): 684-85.
We still tend to think of each infectious agent as if it arose in a vacuum, and not as the result of an ongoing evolutionary process.Viruses show great variety, and in addition many of the viruses of greatest concern mutate rapidly and unpredictably.[17]
Esteban Domingo and John J. Holland, "High Error Rates, Population Equilibrium and Evolution of RNA Replication Systems," and Manfred Eigen and C. K. Biebricher, "Sequence Space and Quasispecies Distribution," both in RNA Genetics, ed. E. Domingo, J. J. Holland, and P. Ahlquist (Boca Raton, Fla.: CRC Press, 1988), 3: 3-36, 211-45; David Steinhauer and John J. Holland, "Rapid Evolution of RNA Viruses," Annual Reviews of Microbiology 41 (1987): 409-33. As these reviews show, HIV is highly variable but is not unique in this respect.
Because previously unrecognized viruses are involved, mechanisms of viral emergence must mirror the unpredictability of these mutations in the genotype. It was usually assumed that most emerging viruses had to arise through the evolution of a new variant, and the emphasis on variation in the viral genome may have engendered a widespread feeling that the significance of viral evolution is to generate unpredictable or unexpected new variants. As we cannot foretell the future, and thus cannot predict the future evolution of any organism, the problem of emerging viruses has always appeared insoluble because it seemed to require predicting the course of viral evolution—an impossible task.The valuable implication of evolutionary theory for viral origins is that if "new" viruses must arise from closely related preexisting viruses, it is not really essential to answer the question in those terms. While variability has undoubtedly contributed to the success of many of the
most troublesome viruses, including influenza, HIV, and many others, the more germane question is how an existing virus that normally infects one host species would be able to cross over into humans to become a human disease problem.[18]
This essay deals with emergence of human disease, but the principles apply equally to other species.
When restated this way, the seemingly insoluble problem of viral origins thus reduces to a more manageable (although not trivial) question of viral traffic, and attacking the problem includes better understanding and appreciating the viruses that already exist in nature, including some viruses not yet discovered. Even more usefully, however, by focusing attention on viral traffic, especially between species, this concept shifts attention to more approachable questions concerning conditions, or the "rules of the road" for viral traffic. What conditions, for example, on the part of the virus or of the host or in the environment, will permit a virus to infect people? Novelty will evolve—even new mechanisms of pathogenesis, as was the case with AIDS. But we may have some advance warning in nature if we know where to look (see also note 6). On the other hand, the factors leading a virus, perhaps as yet unseen in nature, toward emergence can be more more readily predicted and studied. In addition, some emerging viruses may already be in a human population, but they may be geographically isolated.This explanation allows us to consider viral emergence as a process in two major steps. The first step is the advent of what may at first seem to be (or, rarely, actually is) a "new" agent and its initial introduction into the human population. Depending on the virus, this step could have occurred recently or long ago, or it may even have occurred repeatedly before a successful infection. I have made this one step rather than two, because, for the reasons discussed above, a "new" agent is just as likely to be an "old" agent of another species. The virus may perhaps sometimes be slightly altered, although that is usually not necessary. The second step, dissemination in the human population, occurs once a virus infects its first human being. This model, then, presumes that emergence is simply a matter of a virus's getting into the human population and then spreading within the population. Many viruses may never achieve this second step. Although this simplification covers a multitude of sins, it provides a conceptual framework with which to begin. One consequence of this model is that—without requiring detailed advance knowledge of the virus—it permits us to analyze emergence by considering what contributes to each of these steps and what conditions could affect each step, the "traffic laws."
For the first step, even apparently new viruses, such as HIV, have
usually left tracks; often we have just failed to spot them in time. The conceptual problem of viral evolution is also in the first step. But because the requirements of evolution constrain novelty somewhat, there are only a few ways a "new" virus can arise. It can be a truly new virus, a major evolutionary variant, arising by genetic processes such as (for example) mutation or recombination; it can be an existing virus of another species, introduced virtually unchanged or with minor variations into humans from the other species; or it may be an existing human virus of limited scope. The "truly" new virus or major variant is possible but, for the reasons discussed above, is likely to be a rare event. While it is unlikely that we can predict its occurrence, we fortunately will not often be required to do so.[19]
Howard Temin provides evidence that: number of neutral mutations can accumulate and lead in time to a virus possessing drastically different properties from its "parents." Therefore, he argues, it is impossible to predict what new variants will emerge. For an exposition of this argument, see his papers cited in note 6. On the other hand, other factors, such as the limited number of routes by which a virus can enter the body, impose certain constraints. It appears likely that the rules I have described here for the first step are the most important factors in the short run; on a longer time scale, over hundreds or thousands of years, genuine evolutionary change might occasionally be significant.
Several different factors can influence this first step profoundly. Many of the important changes responsible for new viral traffic are made by humans. Just as with other kinds of traffic, viral "traffic" has its traffic indicators, stop-and-go signals, and rules of the road. For example, certain types of environmental changes may be "go" signals for viral traffic. They act by increasing chances or frequency of introduction, or by favoring spread of a natural host or carrier (vector) for a virus. Deforestation and agricultural practices are among the factors most often responsible. To illustrate, I will sketch several instances of viral emergence. Although the examples may appear exotic at first, they will eventually come closer to home.[20]
Because of their number, I have not provided specific references for most of the examples mentioned. For some references, see also Morse and Schluederberg, "Emerging Viruses." Many examples were discussed at the May 1989 conference on emerging viruses, and a forthcoming volume (see note 2) on emerging viruses will describe many of them in greater detail. I am grateful to Karl M. Johnson for providing much of the information on the hemorrhagic fever viruses; to Drs. Robert G. Webster, Peter Palese, and Edwin D. Kilbourne for information on influenza; and to Dr. Thomas P. Monath for information on the arthropod-borne viruses. For the reader desiring additional detailed scientific information, at a more advanced level, and references, the following can be recommended: For background on viruses, viral diseases, and immunology, a general textbook of medical microbiology, such as Bernard D. Davis et al., Microbiology, 4th ed. (New York: Lippincott 1990), can be consulted. For a general treatment of infectious organisms and their hosts and of viruses as the causes of disease (principles of pathogenesis), see Cedric A. Mims, The Pathogenesis of Infectious Diseases, 3rd ed. (New York and London: Academic Press, 1987); see also Sir Macfarlane Burnet and David O. White, Natural History of Infectious Disease, 4th ed. (London and New York: Cambridge University Press, 1972), which has become a classic. Finally, for specific viruses, the most detailed reference is Bernard Fields, ed., Virology, 2nd ed. (New York: Raven Press, 1990).
Argentine hemorrhagic fever is caused by Junin virus. It emerged from obscurity to cause about 400–600 cases annually over an area of 100,000 square kilometers (up from the original 16,000 square kilometers of 1958). The emergence of Argentine hemorrhagic fever was precipitated by agricultural changes as people cleared the pampas for agriculture and began to plant maize. A natural host for this virus is a mouse, Calomys musculinus; infected individuals of this species chronically shed virus in their urine. Although this rodent was always in the Argentine pampas, it began to flourish when natural grassland was cleared and maize was planted, so that ultimately it outnumbered the other rodents. Studies show an enormous difference in numbers of this mouse in cornfields, as opposed to natural grasslands,[21]
Gloria de Villafañe et al., "Dinámica de las comunidades de roedores en agro-ecosistemas pampásicos," Medicina (Buenos Aires), 37, Suppl. 3 (1977): 128-40.
and the first recognition of Argentine hemorrhagic fever (1953) corresponds to increased corn planting in the region. Additional data corroborate the association. The rodent population fluctuates in a three- to five-year cycle, as does the incidence of Argentine hemorrhagic fever cases, and percentage of infected mice is higher in areas with many human Argentine hemorrhagicfever cases. Bolivian hemorrhagic fever is caused by a related virus (Machupo virus) with a similar story; here the rodent is Calomys callosus . For various economic reasons, agriculture, primarily cattle raising, increased in the affected areas of Bolivia over the past thirty years. Calomys callosus adapted well to the new conditions, with the result that more people came in contact with the virus carried by this rodent. Increasing agriculture caused increasing cases. In the 1960s about 1,000 cases were reported, with 20 percent mortality. A program of rodent control, trapping and killing infected mice, has been very effective; as a result, there have been no new cases since 1974. This decrease further indicates that the putative association of rodent and disease was correct. An Old World relative of these two viruses, the notorious Lassa fever of Africa, follows an almost identical pattern.[22]
The recognition of Lassa fever, and its astonishing mortality, was the subject of a popular book about fifteen years ago, Fever! The Hunt for a New Killer Virus, by John Fuller (New York: Reader's Digest Press, 1974). A recent incident was reported in the press (Lawrence K. Altman, "When an Exotic Virus Strikes: A Deadly Case of Lassa Fever," New York Times, February 28, 1989, p. C3).
The major natural host of this virus is another mouse, Mastomys natalensis , which adapts readily to humans, thriving on the food people leave and sharing human habitation. It unwittingly sheds Lassa fever virus, and humans become infected by contact.The unrelated Korean hemorrhagic fever (Hantaan) falls into the same pattern. The natural host is Apodemus , basically a field rodent, and people come in contact with infected animals during rice harvesting. Increased rice planting has provided food for Apodemus as well as for people, and prevalence of Korean hemorrhagic fever has increased accordingly.
Not all of these viruses originate in rodents, although a remarkable number do. A number of important disease-causing viruses are also transmitted by arthropod vectors, such as insects or ticks. Most of these are viruses that can infect both mammals and the arthropod vector, a rather rigorous requirement that bespeaks evolutionary intimacy, on the part of the virus, with both invertebrates and vertebrates. They cause diseases that usually have long histories, and the arthropod vectors (really, arthropod hosts) serve primarily to disseminate a virus or to transport it into new individuals from a natural zoonotic (animal) source. Factors encouraging the arthropod vector can be important in disease emergence, as is demonstrated by several arthropod-transmitted diseases that have emerged recently. Rift Valley fever, found in Africa, caused serious outbreaks in Egypt in 1977 and more recently in Mauritania; the infection is characterized by a fever, usually with hemorrhaging; is naturally transmitted by various mosquitoes; and normally infects ungulates, such as sheep. Because the larvae of most mosquitoes involved in virus transmission develop in water, the addition of large open sources of water
often increases the mosquito population and has a major impact on transmission. In Egypt, although it is not known for certain why the virus emerged, the Aswan high dam was a possible factor precipitating emergence. The factors were more clearly defined in the Mauritanian Rift Valley fever outbreaks. Here the human cases occurred near areas along the Senegal River where large dams (for hydroelectric power) had recently been constructed. Similarly, sporadic outbreaks in other parts of Africa were usually associated with unexpectedly heavy rains.
There have been several incidents of Oropouche fever, first seen in Trinidad around 1957, in the Amazon region of Brazil. Appearance of the disease coincided with the introduction of cacao as a cash crop to the Amazon region. The vector, a biting Culicoides midge, breeds well in empty cacao hulls discarded after harvesting. The virus is also widespread in Panama, where a number of cases have been reported since 1989, and in Venezuela, where a notable outbreak occurred in early 1990. I will have a few words shortly about Lyme disease, not viral but also arthropod borne.
In all these cases, expanding agriculture, often accompanied by deforestation, played a major role in precipitating emergence—that is, in introducing a zoonotic (animal) virus into a new population. The role of agriculture seems logical on consideration. After all, if many "new" viruses are zoonotic, how would people come in contact with animal species bearing unfamiliar zoonotic viruses? Agricultural practices, as well as increased human habitation, may change the ecology of an area to allow a previously minor species to proliferate, as in the cases above. Expanding human habitation in a region, which may include or be the result of clearing land for agriculture, may also put people in direct contact with new animal species (and thus their viruses), as in the example of monkeypox. Monkeypox is an African virus that is related to smallpox but causes a milder form of illness upon infecting humans. It has often been named as a possible successor to smallpox following the recent eradication of the human virus. Monkeypox is so called because it was first identified in infected monkeys, but it is actually a virus of rodents, especially squirrels. People become infected when they develop settlements at the edge of the rainforest and, encroaching on the forest, come in contact with infected rodents inhabiting the forest.[23]
Z. Jezek and Frank Fenner, Human Monkeypox, Monographs in Virology, vol. 17 (Basel: S. Karger, 1988). Fortunately, monkeypox has only a limited ability to spread from person to person and therefore is probably not a major threat, at least in its present form. Frank Fenner considers human monkeypox a transient phenomenon in areas undergoing transition from forest to cleared land. He points out that risk of exposure to monkeypox increases as people begin to encroach on the forest but that the risk decreases considerably after deforestation is largely complete in an area.
More remarkably, the same principles also often apply to viruses whose emergence can clearly be ascribed to viral evolution. Influenza A virus is one of the few known examples (aside from some arguable cases, such as HIV, it may be the only example) of such a virus. Every twenty
years or so, influenza A undergoes a major antigenic shift in one key protein, known as the hemagglutinin (H) protein, and a pandemic results.[24]
Robert G. Webster and R. Rott, "Influenza Virus A Pathogenicity: The Pivotal Role of Hemagglutinin," Cell 50 (1987): 665-66. Robert Webster (personal communication) calls influenza the oldest emerging virus that is still emerging.
Although most changes in influenza virus H proteins occur by so-called antigenic drift, involving the accumulation of random mutations (this drift can lead to the smaller influenza epidemics seen every few years), new pandemic influenza viruses arise by a different route, that of major antigenic shifts. These invariably involve a reassortment of viral genes carried by different influenza strains. Thus, the important event in generating new pandemic influenza strains has, oddly, been not mutational evolution but a reshuffling of existing genes. Where do the genes come from? It has recently been found that most influenza genes are maintained in wildfowl; every known subtype of the H protein can be found in waterfowl. A number of virologists believe that pigs are an important "mixing vessel," allowing influenza virus to make a transition from birds to humans.[25]H. Kida, K. F. Shortridge, and R. G. Webster, "Origin of the Hemagglutinin Gene of H3N2 Influenza Viruses from Pigs in China," Virology 162 (1988): 160-66. In contrast, Chinese scientists believe that the pig is the recipient (getting virus from people) rather than the donor; see Zhu Ji-ming, "Human Virus Diseases in China: Research and Control," Impact of Science on Society 150 (1988): 137-47.
Every major flu epidemic known has originated in south China, which has also long practiced a traditional and unique form of integrated pig-duck farming.[26]Christoph Scholtissek and Ernest Naylor, "Fish Farming and Influenza Pandemics," Nature 331 (1988): 215. For further information on the traditional Chinese pig-duck agriculture systems, see K. Ruddle and G. Zhong, Integrated Agriculture-Aquaculture in South China: The Dike-Pond System of the Zhujiang Delta (New York: Cambridge University Press, 1988). I thank Wallace Parham, U.S. Congress Office of Technology Assessment, for valuable information on this subject.
Agriculture may play the leading role in emergence of this virus as well. Here, too, viral traffic—reassortant viruses from the mixing of animal influenza strains and the transmission of the resulting virus to humans—is more important than viral evolution for human disease.Human immunodeficiency virus is a more difficult case. Where did HIV come from? We do not know the origin of HIV, but a probable primate origin is often suggested and appears highly plausible, at least for HIV-2. The origin of HIV-1 is more problematic. The existence of animal lentiviruses with a predilection for CD4+ T lymphocytes strongly suggests the possibility of a zoonotic origin for HIV at some time in the past. What is currently unknown is how and when the virus was first introduced into humans.[27]
It is also unknown how many times the virus may have been previously (but unsuccessfully) introduced to humans. A great deal has been written on the origins of HIV. For an excellent discussion of several aspects of this question, see Mirko D. Grmek, Histoire du SIDA (Paris: Payot, 1989; English trans., History of AIDS [Princeton, N.J.: Princeton University Press, 1990]). A chapter by Gerald Myers in my forthcoming volume on emerging viruses (note 2) will consider the origin and spread of HIV. For an earlier discussion of these views, see T. F. Smith et al., "The Phylogenetic History of Immunodeficiency Viruses," Nature 333 (1988): 573-75 (and accompanying "News and Views" commentary by David Penney, "Origins of the AIDS Virus," 494-95). See also S. Conner and S. Kingman, The Search for the Virus (London: Penguin Books, 1988); and Montagnier, "Origin and Evolution of HIVs." An alternative hypothesis, that HIV-1 is an ancient virus in humans, has been suggested, notably by Montagnier.
The principles involved in these examples apply to all types of infectious diseases in all parts of the world. For example, it is hard to imagine a part of the world more heavily populated and thoroughly explored than the northeastern United States, but Lyme disease, the media's star disease of the 1989 and 1990 summer seasons, follows the same principles. Although bacterial rather than viral, Lyme disease is also zoonotic, being naturally found in several other mammals and probably originating in wild mice, and is transmitted by a tick. It is not clear why Lyme disease has recently emerged, but conditions favoring increased contact of people and infected tick vectors are likely to be principal reasons. These conditions appear to include changes in forestland around
houses. Malaria, a major cause of death worldwide, is caused by a protozoan parasite and not a virus. It is so widespread that one can hardly consider it emerging. But the recent completion of a new highway (SR 364) through the Amazonian rainforest of Brazil resulted in a massive increase in malaria cases in the region.[28]
Thomas Lovejoy, personal communication, May 1989; Richard House, "Malaria Spreads in Brazil as Development Opens Up the Amazon," Washington Post, July 18, 1989, p. 5.
The second step, dissemination within the human population, is obviously crucial. Not only for newly introduced viruses, but also for many viruses long established in humans, emergence is the result of increased or accelerated dissemination. For this step, there is a vast epidemiological literature, which it is beyond the scope of this essay to review. Instead, I will mention a few recent developments, extending the metaphor of viral traffic by adding traffic in the more familiar sense. Modern transportation offers rich possibilities for rapid dissemination of new or exotic viruses. Recently a man who contracted Lassa fever while visiting Africa became sick after returning to the United States.[29]
Altman, "When an Exotic Virus Strikes." This example demonstrates how comparatively easy it is for a disease to be spread rapidly by travel.
As another example, HIV undoubtedly traveled along the Mombasa-Kinshasa highway and came to the United States presumably through travel.[30]I thank Gerald Myers for this example. See also Conner and Kingman, The Search for the Virus, pp. 212ff, and Peter Piot et al., "AIDS: An International Perspective," Science 239 (1988): 573-79.
I have already mentioned malaria and the Brazilian highway. Of course, this is hardly a new phenomenon in infectious diseases, as witness the classic example of bubonic plague. In this vein, the dissemination of dengue and yellow fever, both transmitted by the same species of mosquito, is a particularly instructive example. The viruses and the mosquitoes were both probably spread by the African slave trade. It has been suggested that the mosquitoes that spread these diseases were inadvertently carried to the New World in the large open water containers on slave vessels. The mosquitoes lay their eggs in water, where the larvae hatch and develop; availability of water is therefore a major factor in population growth for many mosquito species. Plus ça change: A new, and more aggressive, mosquito, Aedes albopictus (the Asian tiger mosquito), was recently found in the United States and is now established in seventeen states. An effective vector for dengue and several other mosquito-borne viruses, the mosquito was introduced into the United States in 1985 in containers of used tires imported into Houston, Texas, from Asia. Wet tires are known as excellent breeding grounds for several species of mosquitoes, and have been shown to harbor many more tiger mosquito larvae than dry tires. Thus, carriers of disease are still themselves carried, however inadvertently, in commerce.Human population movements are of obvious importance for disseminating viruses. Migration to cities from remote areas may pose a particular challenge. People in a remote area may come in contact with
an isolated virus, as in the examples of monkeypox and Lassa fever. If they move to a city, an increasingly common event, they bring their diseases with them. The population growth strains the city's infrastructure and can cause serious problems, as shown by the impressive expansion of dengue virus (a mosquito-borne infection). In many tropical cities open water storage is used increasingly as the city enlarges; as a result, additional breeding grounds are provided for mosquito vectors. At the same time, the high density of these urban areas places infected people and susceptible people in close contact, so that a cycle of infection is established.
Public health measures—such as mosquito control programs, health certification of travelers, and health inspection of imported livestock—have traditionally been directed to combating this stage, which has generally been the most vulnerable to attack. These programs have been instrumental in containing many potential threats, but they also have several drawbacks. Their success with the targeted diseases depends on vigilance and assiduity. Sadly, even when adequate weapons to combat disease are available, we may fail to use them effectively. As a case in point, the recent resurgence of measles in some U.S. cities seems largely due to the failure to ensure that all children are adequately immunized early in life. Efforts may fall victim to their own success, being prematurely relaxed or abandoned, usually to save money; as a result, the conditions that precipitated the program in the first place may reestablish themselves. Many mosquito control programs have met with this fate after initial partial success. These programs are reactive and can generally succeed only with known diseases, although some programs may confer broader benefits. Most of these programs also cannot contain viruses that can spread efficiently from person to person, such as influenza. Present strategy with influenza is to attempt to track emerging new strains and to immunize when feasible.
The modern world also offers additional gateways for viral traffic. For example, as has tragically been demonstrated with HIV, such medical procedures as blood transfusion and tissue transplantation offer the donor's viruses direct access to new hosts. Since many viruses, including HIV, are not able to spread efficiently from person to person, these procedures circumvent the lack of effective means of transmission. As these lifesaving procedures become more widely used, and as the scarcity of donors forces medical centers to look farther afield, it is reasonable to expect more instances. Agriculture again provides an interesting analogy. Viroids, small pieces of genetic information that lack the protein
coat normally needed by viruses to infect host cells, are spread, as far as we know, entirely by mechanical transmission on agricultural implements such as pruning knives and harvesters. It is speculation, but the evolution of viroids could very likely have been shaped, unbeknownst to its human agents, by these human activities.
How do we assess the nature of a viral threat? Before we address this question, let us put aside one class of emerging viruses that occasionally make the news (and rightfully so) but that probably would not represent a major threat. These are viruses that have only recently been identified because of advances in diagnostic technology, but have probably been with us a long time. Two recent examples are non-A, non-B hepatitis and human herpesvirus 6, both viruses that have been discovered within the last three years. In the case of non-A, non-B hepatitis, there is considerable evidence that the virus had been a major cause of post-transfusion hepatitis for years, but the virus itself remained elusive. The application of molecular technology, using DNA cloning, finally made it possible to identify the virus.[31]
Qui-Lim Choo et al., "Isolation of a cDNA Clone Derived from a Blood-Borne Non-A, Non-B Viral Hepatitis Genome," Science 244 (1989): 359-62.
I have already mentioned human herpesvirus 6 (HHV-6).[32]Another T lymphotropic human herpesvirus, dubbed "human herpesvirus 7" (HHV-7), has recently been described (N. Frenkel et al., "Isolation of a New Herpesvirus from Human CD4+ T Cells," Proceedings of the National Academy of Sciences (USA) 87 (1990): 748-52).
HHV-6 was originally reported from Robert Gallo's laboratory under the name "human B lymphotropic virus" (HBLV); it was discovered fortuitously when it interfered with the growth of HIV isolates in tissue culture. At first thought rare, HHV-6 was later associated with the very common childhood disease called roseola. Since roseola has been known for many years,[33]J. Zahorsky, "Roseola Infantilis," Pediatrics 22 (1910): 60.
it is likely that HHV-6 has been a ubiquitous virus for decades, probably centuries. Many known diseases in search of causes can be placed in this category. There are likely to be many surprises here, but few threats, because the viruses are already widely disseminated. On the other hand, the importance of technological advances in making these discoveries cannot be overemphasized. These viruses became apparent because the means were developed to demonstrate their existence.[34]A few words on the importance of technology in disease recognition may be appropriate here. The recognition of HIV was dependent on the previous development of methods for growing T lymphocytes in culture, including key methods that were developed in Gallo's laboratory. For an excellent discussion of the history of HIV and of the role of technology in the discovery of HIV, see Grmek, Historie du SIDA. In a more general sense, the introduction of tissue culture methods, in the 1940s, was a major breakthrough in the study and characterization of viruses. The identification of non-A, non-B hepatitis virus (now called hepatitis C virus), described above, is another example of the successful application of technology. It can be expected that new tools for detection will uncover new viruses. In particular, many new avenues are opened by the recent development of an exceptionally sensitive technique—the polymerase chain reaction, or PCR (Randall K. Saiki et al., "Primer-Directed Enzymatic Amplification of DNA with a Thermostable DNA Polymerase," Science 239 (1988): 487-91; Chin-Yih Ou et al., "DNA Amplification for Direct Detection of HIV-1 in DNA of Peripheral Blood Mononuclear Cells," Science 239 (1988): 295-97). PCR is capable of detecting one HIV-infected cell in a hundred thousand (Richard A. Gibbs and Jeffrey S. Chamberlain, "The Polymerase Chain Reaction: A Meeting Report," Genes and Development 3 (1989): 1095-98). Because PCR can detect and amplify DNA in minuscule amounts of sample, and is comparatively undemanding, it is rapidly finding favor in many applications. PCR has great potential for disease archaeology and the study of evolution. One difficulty with conventional virological methods is that they often require a sample that has been carefully handled. It is often difficult to detect viable virus, for example, in fixed tissues or in samples that have been stored carelessly or for long periods. By PCR many otherwise intractable samples can now be tested, even mummified human bodies 7,000 years old (Svante Pääbo, "Ancient DNA: Extraction, Characterization, Molecular Cloning, and Enzymatic Amplification," Proceedings of the National Academy of Sciences (USA) 86 (1989): 1937; S. Pääbo, R. G. Higuchi, and Allan C. Wilson, "Ancient DNA and the Polymerase Chain Reaction: The Emerging Field of Molecular Archaeology," Journal of Biological Chemistry 264 (1989): 9709). This technique also has possibilities for detecting viral genetic information in ancient samples. There have been many speculations about the antiquity of HIV and AIDS. Mirko Grmek (personal communication, Paris, July 1989) has suggested using PCR to test for HIV or HIV-like viruses in century-old tissues preserved in pathological museums, and this would be quite a feasible way to determine whether HIV infection might have existed then. Even older samples can be tested for specific viruses. PCR techniques are available now for detecting entire families of viruses based on limited genetic resemblances and offer powerful tools for studying viral "paleontology" and evolution (see, for example, David H. Mack and John J. Sninsky, "A Sensitive Method for the Identification of Uncharacterized Viruses Related to Known Virus Groups: Hepadnavirus Model System," Proceedings of the National Academy of Sciences (USA) 85 (1988): 6977-81; Andy Shih, Ravi Misra, and Mark G. Rush, "Detection of Multiple, Novel Reverse Transcriptase Coding Sequences in Human Nucleic Acids: Relation to Primate Retroviruses," Journal of Virology 63 (1989): 64-75. As a result, one can now "go fishing" for viral ancestors and relatives in formerly untestable samples. PCR makes multiple copies of the specific piece of DNA it detects, and the resulting product can be analyzed and compared with known viruses. This capability is a boon for the study of viral evolution over long periods of time. Such study was previously impossible because, as has often been remarked by viral evolutionists, "viruses have left no fossil footprints" (quote from Darryl C. Reanney, "Evolutionary Virology: A Molecular Overview," in The Human Herpesviruses, ed. André J. Nahmias, W. R. Dowdle, and Raymond R. Schinazi (New York: Elsevier, 1981), p. 519; for a more recent review of molecular evolutionary studies of viruses, see Adrian Gibbs, "Molecular Evolution of Viruses: 'Trees,' 'Clocks' and 'Modules,'" Journal of Cell Science Supp. 7 (1987): 319-37, and earlier forms could only be inferred from vestigial genetic information in existing viruses.
It is conceivable that a change in some critical condition could cause one of these already widespread viruses to become a threat, but such an occurrence appears unlikely.Predicting the greatest threats is a more difficult task, made more difficult by significant gaps in our knowledge. Of course, we cannot foretell the future. Many would say that the only sure bet is that the next threat will be one not on any list today, as was the case with AIDS. That is why I think it is much more important and useful to emphasize the general principles underlying viral emergence, rather than to attempt to compile a list. However, since I am flinging about a plethora of virus names as examples, I list here some of the viruses that might be
perceived as future threats. Several have already been discussed. Most lists would probably include the following: influenza; the hantaviruses (Hantaan, Seoul, and related viruses); Rift Valley fever; yellow fever; dengue fever; Junin (Argentine hemorrhagic fever); Lassa fever; Marburg and Ebola viruses (members of the family Filoviridae); and various encephalitides, all arthropod borne, such as Japanese encephalitis, Venezuelan equine encephalitis, and Eastern equine encephalitis.
Influenza, of course, is familiar. The hantaviruses—Hantaan, Seoul, and related viruses—cause hemorrhagic fevers with renal syndrome (that is, fevers accompanied by severe bleeding and kidney involvement); these viruses, found in Asia, Europe, and the United States, are naturally occurring viruses of rodents (in the case of Hantaan, a rodent called Apodemus agrarius ). Seoul virus is found in rats, including urban rats in Korea as well as in Baltimore and other American cities. James Le Duc has recently found a possible association between this virus and chronic renal disease in people living in inner-city Baltimore.[35]
James LeDuc, personal communication, May 1989.
Yellow fever, a mosquito-borne disease characterized by fever and jaundice, originated in Africa and is now widespread in Africa and South America; it probably originated as a virus of monkeys. Dengue fever, a virus in the same family that is also transmitted by the same mosquitoes as yellow fever, probably also originated in the Old World but is now in tropical areas worldwide (Africa, Asia, the south Pacific, South America, and the Caribbean). Other viruses, classified by virologists as members of the Arenavirus family, cause hemorrhagic fevers and are natural infections of rodents. These include Junin (Argentine hemorrhagic fever) and Machupo (Bolivian hemorrhagic fever), and the once infamous (because of its high mortality rate in Western medical missionaries who first came in contact with the virus in the early 1970s) Lassa fever of West Africa, which originated in the rodent Mastomys natalensis , all of which viruses were discussed above. Among viruses believed to have originated in monkeys or apes are two related African viruses, Marburg and Ebola, which cause fever with hemorrhage; the unrelated HIV also can be placed in this category. The various equine encephalitides are mosquito borne but tend to have natural animal hosts as well.
Of the viruses listed, I think that influenza, dengue, and the hantaviruses are of greatest potential importance to North America; the recent outbreaks of Oropouche in the Caribbean and Central America are also notable. All these viruses either are widening their scope (dengue, hantaviruses, and recently Oropouche) or still cause recurrent pandemics
(influenza). Because of its proximity, dengue might be a special concern. It is widespread in Asia and is also spreading over the Caribbean basin. A dengue outbreak in Cuba in 1981 involved over 300,000 cases. Under certain circumstances an individual who was previously infected with one variety (technically, subtype) of dengue virus can develop a severe form known as dengue hemorrhagic fever upon later infection with a different subtype. The frequency of dengue hemorrhagic fever is increasing as several subtypes of dengue virus extend their range. Aside from the viruses I have listed, there is also always a likelihood that other, as yet undescribed or presently obscure, zoonotic viruses may emerge, as did HIV and Lassa fever. That is why I have emphasized the principles and used these viruses only as examples.
Although the framework offered here identifies the essential conditions for viral emergence, there is still a great deal to learn. Consider influenza. With all the possibilities for recombination, and many human infections annually (perhaps 100,000,000), pandemic influenza strains appear only once every twenty years or so. Why? To put the question in more technical terms, what restrains the emergence of new viruses? Comparatively little is known about this fascinating question, although some patterns are beginning to appear. We also only vaguely understand what factors are required for efficient transmission of viruses in humans. Apart from influenza, many of the other viruses discussed here—such as Junin (Argentine hemorrhagic fever), Marburg, Hantaan, and Lassa fever—fortunately have limited ability to spread from person to person. They would have been devastating if they had that ability or if they were to acquire it. We also need to know more about the mechanisms and determinants of interspecies transfer of viruses. This is a complex matter involving both viral and host factors, but some information is already available and the question is susceptible to further scientific attack. Equally little is known about constraints on viral evolution. In particular, the role of natural selection in shaping or restraining viral evolution has been little explored. Certainly, constraints operate at the level of the virus—host interaction and the maintenance of the virus in nature. In order to survive, viruses must be maintained in nature in some living host. This requirement alone must impose strong selective pressures on a virus.
Even with these gaps in knowledge, we now possess, at least embryonically, the necessary intellectual foundation and tools for attacking these questions, and are faced with the challenge of dealing with the problem of disease emergence. We are not outside the problem; we are
learning that emerging viruses do not come as a malevolent rain from above. Human actions have influenced many of these calamities, including HIV. This is, perhaps, both the good news and the bad: We are not completely helpless; but before we can begin to do something, this issue must become a social and economic priority. In many ways, this may prove to be a harder problem than the virological one. However, the essential conclusion is that we must learn to be aware of the consequences of our own actions.
Despite its limitations, the historical record provides clues to traffic patterns. As McNeill has noted, new diseases tend to emerge when populations cross disease boundaries.[36]
William H. McNeill, Plagues and Peoples (Garden City, N.Y.: Doubleday, 1976). His recent essay "Control and Catastrophe in Human Affairs," Daedalus 118 (Winter 1989): 1-12, giving his views on human attempts to control catastrophic events, may also be of interest.
Recurrent patterns, and near recurrences, abound in history. As pointed out by Elizabeth Fee and Daniel Fox in their Introduction to this volume, such recurrences can be misleading when they are used as analogies. However, they can also be instructive when viewed as manifestations of similar biological processes and traffic patterns that have continued throughout history. The historic association of bubonic plague with rats, and its entry at seaports, is well known.[37]Philip Zeigler, The Black Death (New York: Harper and Row, 1969); Robert S. Gottfried, The Black Death (New York: Free Press, 1983). As a non-historian, I have sometimes idly wondered whether the history of Europe would have been different if the people of this period had known sooner about this association and if the simple metal rat-catcher that prevents rats from leaving ships had been available in the Middle Ages.
Hence the concern when a virus resembling Hantaan was found only a few years ago in rats living around Baltimore harbor. Although an imperfect analogy, the discovery should remind us that the historic association of rodents, ports, and disease dissemination is not an antiquarian oddity.More recently the epidemiology of AIDS itself—although, tragically, not its effects—could have been inferred from what was known about hepatitis B, which had a remarkably similar epidemiology. Long before the viral etiology of AIDS was defined, epidemiologists had demonstrated the similarity of transmission patterns for AIDS and for hepatitis B, with identical high-risk practices and risk groups.[38]
W. Thomas London and Baruch S. Blumberg, "Comments on the Role of Epidemiology in the Investigation of Hepatitis B Virus," Epidemiologic Reviews 7 (1985): 59-79.
This information began pointing the way toward suitable precautions to limit spread.If we had a science of traffic patterns, part biology and part social science, we might have made these inferences more readily, with many lives saved. Perhaps such a field may be struggling to emerge, and among those in the forefront might be mentioned Joshua Lederberg, Baruch Blumberg, Frank Fenner, Edwin Kilbourne, Karl M. Johnson, Thomas Monath, Christoph Scholtissek, Luc Montagnier, D. A. Henderson, Mirko Grmek, William McNeill, the late Fernand Braudel, and Daniel Fox.
Enthusiasm, of course, must be tempered by reality. Even if such a science were developed, and even if there were universal agreement on an agenda, it will probably never be possible to anticipate or prevent every episode of disease emergence. Aside from human factors, our
knowledge and ability to act will always be imperfect: not every consequence can be anticipated, the world is too complex, and the generation of new pathogens by viral evolution, however constrained and rare it may be, is still possible. At the moment perhaps the most we can hope for realistically is to begin making inroads into the problem.
Why has it taken so long to develop such thinking? For one thing, we may have been misled by our own preconceptions. Virologists and microbiologists have been concerned with the properties of the disease agents—physical and molecular—and of the diseases they cause, and have tended to concentrate on the particular, possibly to the detriment of defining features in common. Until very recently there were many examples of viral traffic and some examples of mutations, but we had not critically evaluated the contributions of each mechanism to viral emergence. It also seemed too daunting a problem. But, as the examples discussed here should demonstrate, the variations in the agents themselves may be less crucial than the traffic laws, the conditions that allow introduction and dissemination in the human population. While this idea is possibly a logical extension of the Darwinian emphasis on natural selection in the environment, it is nevertheless rarely considered. An appropriate global emphasis on conditions, as in historical thinking, would therefore be valuable in combination with the powerful molecular tools now available for virus detection.
Biological scientists may also find it difficult to believe that people themselves bear much of the responsibility for what may seem at first to be natural processes. Historians and social scientists are more accustomed than virologists and microbiologists to think in terms of the consequences of human actions, and of conditions that cause or permit certain developments, and try to infer these predisposing conditions from the results. This perspective is valuable and complements the kind of analytic and causal thinking in which biological scientists are trained. As the historian Marc Bloch put it, "The virus [sic] of the Black Death was the prime cause of the depopulation of Europe. But the epidemic spread so rapidly only by virture of certain social—and, therefore, in their underlying nature, mental—conditions."[39]
Marc Bloch, The Historian's Craft, trans. Peter Putnam (New York: Knopf, 1953), chap. 5, quoted sentences, p. 194.
Like every other kind of traffic, viral traffic is increasing. What we are now learning about viral emergence shifts the burden to society at large, to all of us. The conditions I have described are really manmade. Consequently, we need to develop greater sensitivity to our environment and the complex ecological relationships that have evolved. In many cases viral emergence follows deforestation and is another unanticipated
consequence of despoiling the environment. As deforestation progresses worldwide, as human activities continue to alter the environment, as population influx into Third World cities continues unabated, as every part of the world becomes more accessible, one would expect disease emergence to accelerate. Our first line of defense is to recognize that these and similar human activities can have serious health consequences, and to anticipate these consequences. We need effective strategies to deal proactively, before their spread becomes critical, with viruses as yet unrecognized and with those that disseminate efficiently. To put it simply, if we are often the engineers of viral traffic, we need better traffic engineering. We need viral traffic studies and road maps of disease. I mean this not only literally, in the sense of medical geography, but also metaphorically. When agricultural development is desirable, it would also be wise to consider and plan for disease emergence as a possible side effect. Environmental impact surveys, conducted thoroughly and systematically, should also include consideration of the microbial and viral fauna in the region.
How might such studies be done? Until a more systematic approach can be defined, we have only the rudiments of an answer, but some generalizations can be made. Certain activities, notably the sorts of environmental changes I have discussed, should be recognized as potentially hazardous, especially in tropical regions. Surveys can test for a known virus when there is a proposed expansion of conditions favorable to viral transmission in areas where this virus is endemic. For example, in view of the history of Argentine hemorrhagic fever, plans to clear new areas of the pampas could trigger field surveys to test for the presence of Junin virus in local rodents. Plans for dam building in certain parts of Africa should bring Rift Valley fever to mind, with appropriate field surveys for this virus.
Unknown viruses will present more of a challenge. One can work from analogy with known examples, and search for viral relatives in similar environments. We do not know what other viruses exist in nature, but using the biotechnological tools now available (such as PCR, discussed in note 34) for broad and rapid testing, we can make more systematic efforts to find out. Fenner has noted that our knowledge of arbo (arthropod-borne) viruses increased dramatically in the 1950s and 1960s largely because the Rockefeller Foundation funded a program to screen for arboviruses in the field by the methods then available.[40]
Frank Fenner, "Keynote Address," in Viral and Mycoplasmal Infections of Laboratory Rodents, ed. Pravin N. Bhatt et al. (Orlando, Fla.: Academic Press, 1986), p. 21; amplified in personal communication, November 1989.
This screening was done mostly by simple biological assays in which samples of ground-up mosquitoes were injected into mice in order to detect virusespathogenic for mammals that might be present in the mosquitoes. Crude as this sort of screening was, it yielded many new viruses. However, such screening has many disadvantages and is not cost-effective. It is also difficult to evaluate the actual human or animal disease potential of the viruses discovered in this way. Present technology makes it much easier to identify families of viruses in human, primate, rodent, or arthropod populations by broad-based PCR and serological techniques.
Industrialized nations must learn to assist the Third World in financing the needed planning and protective measures to accompany development projects. In many cases relatively simple measures could help greatly, if they are chosen well and if there is sufficient global resolve to implement them. For example, rebuilding water systems in tropical cities to reduce or eliminate open water sources could have a real impact on dengue. Perhaps such projects could someday become priorities before their need reaches the crisis stage. In the intellectual arena our best strategy may be to encourage expanded attempts to find answers to the scientific questions mentioned above, and to forge stronger alliances between molecular virology and such organism-based approaches as field biology, evolutionary biology, and pathogenesis (mechanisms of disease and host-virus interactions). Several scientists have expressed concern that field virologists will soon be in critically short supply; with a paucity of training programs and trainees, the outlook for the future is bleak. In the Third World, for example, there are few well-staffed and thoroughly equipped field laboratories, and their number is decreasing.
The tragedy of AIDS has spurred us on to a consideration of these issues, but it is an unfortunate comment on human nature that such adversity is required before these issues are considered at all. Even with AIDS, the virological problems were largely secondary to a social problem: the failure to recognize the threat and mobilize responses in a timely way.[41]
Randy Shilts, And the Band Played On: Politics, People, and the AIDS Epidemic (New York: St. Martin's Press, 1987), describes many of these failures and their disastrous consequences.
The "moral equivalent" of war, as many leaders have learned to their chagrin, is a poor substitute for the actual thing. It is hard to sustain fervor without a visible adversary. There are also insufficient economic incentives to mobilize concerted action in advance of a crisis. One can only hope that the value of doing so will be appreciated before we are in the throes of another crisis. Ironically, the costs are likely to be small in comparison with major military projects. As Henderson has pointed out, the eradication of smallpox, a landmark in infectious disease control, was accomplished at a total cost of about $300 million.[42]Donald Henderson, personal communication May 1989, February 1991; and D. A. Henderson, in F. Fenner et al., Smallpox and Its Eradication (Geneva: World Health Organization, 1988). Dr. Henderson directed the world smallpox eradication program.
It is unlikely that infectious diseases will ever be totally eliminated. Our desire to believe that they can be eliminated may reflect the irrational feelings of terror and loss of control that thoughts of these diseases inspire.[43]
The subject of much literature, from antiquity to now. Susan Sontag, AIDS and Its Metaphors (New York: Farrar, Straus and Giroux, 1988), demonstrates the power of these images even now.
We have no recourse but to confront these feelings and to deal constructively with them. Even in this highly technological age, we cannot control our biological milieu. At the same time, we must recognize the role that we ourselves play in shaping this milieu. We are part of a complex, interlinked world that we can alter but do not fully control, and science is the study of this complexity. The periodic appearance of "new" infectious diseases serves to remind us of this reality.Causes, Cases, And Cohorts:
The Role Of Epidemiology In The Historical Construction Of AIDS
Gerald M. Oppenheimer
In his history of the HIV (human immunodeficiency virus) epidemic, Mirko Grmek reports that the term acquired immune deficiency syndrome , the first generally accepted name for this new disorder, was coined at a 1982 meeting held at the Centers for Disease Control (CDC) in Atlanta. Thereafter, the CDC epidemiologists spread and legitimated the neologism by using it extensively in official publications.[1]
Mirko D. Grmek, Histoire du SIDA (Paris: Payot, 1989), pp. 58-61. The descriptive term acquired immunodeficiency syndrome, or AIDS, became synonymous with the new disorder; it has recently been replaced by human immunodeficiency virus (HIV) infection. Though, in general, this essay uses the new acronym, in discussing specific studies it will employ whatever term was used by the investigators reporting.
By attributing to the CDC the power to control the name of the disease, Grmek indirectly demonstrates how prominent a part that agency and its epidemiologists played in defining this new "medical mystery."In this essay I examine the role of epidemiologists, in the CDC and elsewhere, in characterizing HIV infection. Faced with a new disease of unknown origin, epidemiologists and their collaborators constructed, over time, hypothetical models to explain the disorder in order to contain it. Prior to the isolation of a causal virus, epidemiologists played a central role in defining the new syndrome, developing first a "life-style" model and later a model based on hepatitis B. Though subsequently supplanted from their special position by virologists and other "bench" scientists working in laboratories (who named the virus and thereby redesignated the disease), epidemiologists have continued to define important dimensions of the disorder and to raise disquieting questions. Specifically, they were concerned with discovering risk factors for HIV infection, its modes of transmission, the natural history of the disease, the extent to which it had spread within population groups, and the projection of future prevalence and incidence rates.
This is a substantially revised and updated version of the chapter entitled "In the Eye of the Storm: The Epidemiological Construction of AIDS," in AIDS: The Burdens of History , ed. Elizabeth Fee and Daniel M. Fox (Berkeley: University of California Press, 1988), pp. 267–300. This essay has benefited from the generous comments of Ronald Bayer, Ben Brody, Elizabeth Fee, Daniel M. Fox, Robert Padgug, and Anne Stone.
Although epidemiologists have increasingly lost to biomedical scientists the power to construct the meaning of the HIV infection, epidemiologists in the CDC retain an important prerogative: they continue to frame the population-based definition of AIDS. Because the CDC has responsibility for monitoring infection in the United States, it has formulated, over time, the surveillance definitions of AIDS. Recently this population-based definition, as well as the reporting system itself, has been found deficient by demographers and quantitative social scientists. Their critiques raise the possibility that the power of epidemiologists to frame the disorder, already limited by biomedical scientists, may be further eroded by social scientists newly attracted to the study of AIDS. Nonetheless, since 1981 epidemiology has had a profound effect on the characterization of HIV infection in the United States. To a large degree, that characterization reflects something of the nature and concerns of American epidemiology itself.
Epidemiology, unlike virology, has a strong social dimension in that it explicitly incorporates perceptions of a population's social relations, behavioral patterns, and experiences into its explanations of disease processes. Given their training, epidemiologists fairly consistently defined HIV infection as a biological process occurring within a determinant social matrix. That the infection was first identified among young male homosexuals and intravenous drug users certainly reinforced that professional proclivity.
The results of this exercise in epidemiological imagination were complex and equivocal. On the one hand, the epidemiologists' approach may have skewed the choice of models and hypotheses, determined which data were excluded from consideration until later in the epidemic, and offered scientific justification for popular prejudice, particularly against gay men. On the other hand, the epidemiological approach gave the new disease a human face. By defining the behaviors and the multiple social experiences of groups as risk factors for the disease, epidemiology countered attempts to reduce the etiology of HIV infection to a virus alone. In addition, epidemiology offered the possibility of primary prevention in the form of health education and follow-up, particularly important in the absence of a vaccine or a successful therapy.
The various characterizations of HIV infection examined in this essay will span the period from early 1981, when physicians first encountered anomalous medical facts, to mid-1990, when epidemiologists had attempted to define the distribution of the HIV across subpopulations; to project future rates of HIV infection and illness for the population as
a whole; and to establish wih some specificity the natural history of the new disease. This essay draws almost entirely on the medical literature of the period.
Epidemiology And Public Health
Epidemiology played a key role in the AIDS epidemic for at least two reasons—one institutional, the other scientific. The institutional link was the Centers for Disease Control (CDC) in Atlanta. Part of the Public Health Service, which falls under the jurisdiction of the U.S. Department of Health and Human Services, the CDC is responsible for monitoring morbidity and mortality trends in the United States and for responding to acute outbreaks of disease—infectious disease in particular. To fulfill its mission, the CDC depends heavily on case reports, surveillance, and epidemiological investigations.
Epidemiology is particularly well suited to explore, portray, and explain new medical phenomena. It seeks to measure and analyze the occurrence and distribution of diseases and other health-related conditions in human populations, acting both as a sentinel who warns of shifts in disease patterns and as a scout who seizes on such shifts to discover their etiology.
For example, by systematically collecting data on the frequency of disorders in populations or subgroups through surveillance programs, epidemiologists can discern changes in the distribution of diseases in the community. Observations of these distributions, and their variation in subgroups, lead to hypotheses concerning the relationship between the disease and variables that may affect its natural history and clinical course. Using different study designs, epidemiologists attempt to measure, reject, or refine the relative significance of such hypothetical associations. The ultimate objective of these studies is to isolate the causal variables of the disease in question. An intermediate goal is to discover a point in the natural history of the disease where intervention might alter its course, even if its etiology remains unknown.
Epidemiologists tend to believe in multifactorial disease models. They assume, that is, that intervention is possible at several points, even in the absence of a known "first cause." The major premise of the multifactorial model is, as the name implies, that a given disease may have a number of causes or antecedents, a combination of which may be needed to produce the disorder. The "web of causes," therefore, may be interdicted at more than one vulnerable point.[2]
Brian MacMahon and Thomas F. Pugh, Epidemiology (Boston: Little, Brown, 1970), p. 25. See also John M. Last, ed., A Dictionary of Epidemiology (New York: Oxford University Press, 1983), S.V. "multiple causation."
The power of the multifactorial model is that it can incorporate any measurable factor relevant to and statistically associated with the disease or disorder of interest. Unlike the reductionist paradigm of the germ theory, the multicausal model embraces a variety of environmental and social factors. The model's strength, however, is also its weakness. The multifactorial model allows the researcher to cast a very wide net. Scientists may attempt to incorporate many possible explanatory variables whose putative causal connections with the disease in question may be plausible for a number of reasons—scientific, logical, historical, experiential, and so forth. Variables may be drawn in (or left out) as a function of the social values of the scientists, the working group, or the society. When included in the model, embraced by the professionals, and published in the scientific press, such value judgments appear to be objective, well-grounded scientific statements.
Epidemiology is an applied science that responds to two kinds of disorder within the community: one caused by the disease directly, and the other the product of the fears it has aroused. Consequently, epidemiology bore the initial responsibility of outlining the direction of research, generating hypotheses, and synthesizing the results. In the face of a fatal disorder of unknown origin and indefinite proportions, epidemiology offered a set of procedures (for example, case definition, verification, and count) that swiftly generated results and then authenticated them, giving the public a sense of definite progress. The content of this science, by providing and naming concepts (for example, "risk groups"), made the epidemic potentially less frightening by making it appear more likely that the disease would eventually be understood and controlled.
Case Finding And Surveillance
The initial discoveries heralding a new disorder of unknown origin were made by physicians treating patients in Los Angeles hospitals. Michael Gottlieb and his colleagues alerted the CDC that between October 1980 and May 1981 five young, previously healthy homosexual men had been treated for biopsy-confirmed Pneumocystis carinii pneumonia (PCP). PCP is a protozoan-produced condition that occurs almost exclusively in persons with severely suppressed or defective immune systems. On June 5, 1981, a short paper describing the patients was published by the CDC in its Morbidity and Mortality Weekly Report (MMWR) .[3]
U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, Reports on AIDS Published in the Morbidity and Mortality Weekly Report, June 1981 through February 1986 (Springfield, Va.: National Technical Information Service, 1986), pp. 1-2 (hereafter cited as MMWR).
Gottlieb's communication to the CDC was closely followed by another from New York City and San Francisco, which reported that, in the thirty months prior to July 1981, Kaposi's sarcoma (KS) had been diagnosed in twenty-six male homosexuals between twenty-six and fifty-one years of age.[4]
MMWR, pp. 2-4.
A rare cancer in the United States, KS occurred in this country primarily in elderly males and immunosuppressed transplant recipients. Its manifestation in a relatively large number of young men was considered highly unusual.An editorial note in the issue of MMWR that had published Gottlieb's paper hypothesized that "the fact that these patients were all homosexuals suggests an association between some aspect of a homosexual lifestyle or disease acquired through sexual contact and Pneumocystis pneumonia in this population."[5]
Ibid., p. 2.
The conjecture that some aspect of homosexuality predisposed the patients to immune dysfunction and infections was made on the basis of only five cases from a single community, a broad generalization to formulate from so small a sample.The basis for that sweeping hypothesis lay in a rough mixture of analysis and opinion. The CDC had just completed a cooperative study with a number of gay community health clinics. It was a multiyear, multisite study of risk factors for hepatitis B, a disease which can be sexually transmitted and whose prevalence is very high among homosexual men.[6]
David G. Ostrow, "Homosexuality and Sexually Transmitted Diseases," in Sexually Transmitted Diseases, ed. Yehudi M. Felman (New York: Churchill Livingston, 1986), p. 210. See also M. T. Schreeder et al., "Hepatitis B in Homosexual Men: Prevalence of Infection and Factors Related to Transmission," Journal of Infectious Diseases 146 (1982): 7-15.
In analyzing the interrelation of life-style and hepatitis B, the researchers found that blood markers for the disease were significantly associated with, among other factors, a large number of male sexual partners and with sexual practices that involved anal contact.The CDC-associated study took place against a background of other investigations that pointed to an increase in the incidence as well as the types of sexually transmitted diseases (STDs) in homosexual men.[7]
William W. Darrow, "Sexual Behavior in America," in Sexually Transmitted Diseases, ed. Felman, pp. 269-71.
Analysts linked this epidemic of STDs to gay liberation and the attendant life-style of bars, discos, and bathhouses and of anonymous sexual partners.[8]Terry Alan Sandholzer, "Factors Affecting the Incidence and Management of Sexually Transmitted Diseases in Homosexual Men, in Sexually Transmitted Diseases in Homosexual Men, ed. David G. Ostrow, Terry Alan Sandholzer, and Yehudi M. Felman (New York: Plenum Medical Book Company, 1983), p. 5.
The combination of the CDC's recent work on risk factors for hepatitis B transmission, which had increased its awareness of gay life-style and sexuality and its knowledge of the epidemicity of STDs among subgroups within the gay community, probably accounts in part for the hypothesis suggested in the MMWR . One might fairly infer that the CDC was prematurely ready to find the etiology of this mysterious disorder in an exotic subculture. This inference is strengthened by the ensuing scientific work of epidemiologists within and outside the CDC,
who found in gay culture—particularly in its perceived "extreme" and "nonnormative" aspects (that is, "promiscuity" and recreational drugs)—the crucial clue to the cause of the new syndrome.
Part of the reason for the CDC's speedy adoption of the "life-style" hypothesis was, most likely, that in certain previous outbreaks of diseases of uncertain origin (in particular, legionnaires' disease in 1976), CDC officials had been criticized for committing themselves to a microbial hypothesis without having paid sufficient attention to alternative causative theories.[9]
See U.S. Congress, House of Representatives, Subcommittee on Consumer Protection and Finance, Committee on Interstate and Foreign Commerce, Hearings on Legionnaires' Disease, November 23-24, 1976, 94th Cong. For a defense of the CDC, see Barbara J. Culliton, "Legion Fever: Postmortem on an Investigation That Failed," Science 194 (1976): 1025-27.
Such criticism probably influenced their desire to throw a causative net widely in the case of HIV infection.[10]Stephen Schultz, M.D., former deputy commissioner, New York City Department of Health, personal communication, July 22, 1987.
A special task force on KS and opportunistic infections was established at the CDC in mid-1981 and charged with the surveillance of all new cases. As a preliminary step, the CDC had to define what constituted a case. It initially described a case as "a person who 1) has either biopsy-proven KS or biopsy-proven, life-threatening opportunistic infection, 2) is under age 60, and 3) has no history of either immunosuppressive underlying illness or immunosuppressive therapy."[11]
MMWR, p. 9.
By September 1982, when the CDC first used the term AIDS in the MMWR , it refined this description to define an AIDS case as one with "a disease at least moderately predictive of a defect in cell-mediated immunity, occurring in a person with no known cause for diminished resistance to that disease." Included among the diseases were KS, PCP, and a specific list of "other opportunistic infections," a list which the CDC has amended over the years.[12]Ibid., pp. 18, 95-97.
On September 1, 1987, the CDC significantly modified its case definition. It not only included new medical conditions such as HIV-related encephalopathy (dementia) and wasting syndrome but, for the first time, counted as cases those who, along with a positive antibody test, have had only a presumptive (that is, non-laboratory-confirmed) diagnosis for certain diseases, such as PCP and KS. Preliminary evidence indicates that 12 percent of cases diagnosed during the four months after September 1, 1987, met only the new case definition.[13]
See John M. Karon, Timothy J. Dondero, Jr., and James W. Curran, "The Projected Incidence of AIDS and Estimated Prevalence of HIV Infection in the United States," Journal of Acquired Immune Deficiency Syndromes 1 (1988): 542-50.
What caused this disorder? With limited clinical data at hand, the CDC did a "quick and dirty" survey of 420 males attending venereal disease clinics in San Francisco, New York, and Atlanta, with the intention of finding cases with KS or PCP. The thirty-five cases culled from the sample (biased, since such patients are more active sexually than the general population) were interviewed on many subjects in the hope that a lead might be discovered.
The researchers found two patterns of behavior that "fell out": sex
and drugs. The cases, all homosexuals, had had many sexual partners in the past year (the median was eighty-seven) and had frequently used marijuana, cocaine, and amyl or butyl nitrite—inhalant sexual stimulants.[14]
Centers for Disease Control, Task Force on Kaposi's Sarcoma and Opportunistic Infections, "Epidemiologic Aspects of the Current Outbreak of Kaposi's Sarcoma and Opportunistic Infections," New England Journal of Medicine 306 (1982): 248 (hereafter cited as Task Force Report); see also Gerald Astor, The Disease Detectives (New York: New American Library, 1983), p. 56.
Were sex and drugs independent of each other, however? The rate of nitrite use, for example, was closely associated with the number of sexual partners, suggesting that nitrite inhalation might be associated with other hypothetical causal variables, including sexually transmitted diseases, the medications used to treat them, or types of sexual behavior.[15]Task Force Report, p. 252.
It was also possible that nitrite use was not an etiological factor, but appeared to be one because it was associated with a casual or "confounding" variable such as sex.Despite the dearth of evidence (the "quick and dirty" survey had found that 86.4 percent of homosexual or bisexual men, whether cases or not, had used nitrite in the previous five years), amyl nitrite (AN) did become one of the first hypothetical causal variables to be investigated.[16]
MMWR, pp. 4-5.
As a clue, amyl nitrite seemed worth pursuing. It appeared to be compatible with the gay life-style thesis posed by the MMWR and attractive to epidemiological researchers. Studies in which nitrite inhalant was a variable will be evaluated below.Scientific papers published in 1981 consisted mainly of case and surveillance reports, in which attempts were made to define the new syndromes and the patients—that is, to formulate what constituted a "case." By describing the population at risk in terms of person, place, and time, and by learning from physicians the clinical details of the disorder, epidemiologists could grope for etiological clues that they might use to design formal studies.
One of the first clinical clues pursued was the possibility that the new syndrome was caused by the cytomegalovirus (CMV), a microbe suspected of being both sexually transmitted and a cause of KS. In September the British medical journal The Lancet published a clinical study of KS in eight homosexual men in New York City; the investigation found that all four patients tested were positive for CMV.[17]
Kenneth B. Hymes et al., "Kaposi's Sarcoma in Homosexual Men—A Report on Eight Cases," Lancet 2 (1981): 598-600.
Three months later Michael Gottlieb and his colleagues reported that four previously healthy men with PCP were infected with CMV and also were suffering from a marked decrease in white blood cells, particularly of a kind known as T4 helper cells.[18]Michael S. Gottlieb et al., "Pneumocystis Carinii Pneumonia and Mucosal Candidiasis in Previously Healthy Homosexual Men," New England Journal of Medicine 305 (1981): 1430.
While acknowledging that CMV infection might result from T4-cell deficiency and the reactivation of a dormant infection, Gottlieb and his colleagues, basing their position on previous studies, preferred to hold CMV highly suspect.The CDC, in its year-end summary on the epidemic, also cited CMV
as one of three possible etiological agents.[19]
Task Force Report, pp. 251-52.
Other putative causes, perhaps more closely related to the life-style hypothesis, were amyl nitrite and opiate addiction. (A recent investigation in New York City of eleven immunocompromised men with PCP had found that seven of the patients, including five heterosexuals, were drug "abusers."[20]Henry Masur et al., "An Outbreak of Community-Acquired Pneumocystis Carinii Pneumonia," New England Journal of Medicine 305 (1981): 1431-38.
) Did any of these agents bear a relationship to any other? How did CMV fit into the life-style hypothesis? An editorial in the New England Journal of Medicine addressed these issues in December 1981.Ignoring the heterosexual cases of PCP and other opportunistic infections, the editorialist noted that "the question of cause is obviously central. What clue does the link with homosexuality provide?"[21]
David T. Durack, "Opportunistic Infections and Kaposi's Sarcoma in Homosexual Men," New England Journal of Medicine 305 (1981): 1466.
The answer was a high incidence of sexually transmitted diseases, including viral infections such as CMV and hepatitis B, that might cause immunosuppression and KS. But because neither homosexuality nor CMV is new, the author suggested that a new factor may have modified the host-agent relationship: recreational drugs, particularly amyl nitrite. On the basis of this reasoning, he postulated a possible multifactorial disease model.[22]A model can be defined as "a description, a collection of statistical data, or an analogy used to help visualize often in a simplified way something that cannot be directly observed"; see Webster's Third New International Dictionary of the English language Unabridged (1986), S.V. "model." According to Susser, a model is a system reduced to a set of related variables for the purpose of prediction or representation (Mervyn Susser, Causal Thinking in the Health Sciences [New York: Oxford University Press, 1973], p. 32). In the present essay the models discussed perform a representational function in that they "represent existing or postulated relationships in simplified form" (ibid., p. 33).
Specifically, he proposed that the joint effects of persistent, sexually transmitted viral infection (presumably from CMV) and a recreational drug such as amyl nitrite precipitated immunosuppression in genetically predisposed males. From this followed a clinical course that included minor illnesses, then KS or other neoplasms, and serious opportunisitic infections. In essence, the model was an elaboration of the hypothesis originally proposed in the editorial note appended to the first MMWR on the new disease.The Life-Style Hypothesis: Experimental Work
To refine hypotheses generated by case reports, "quick and dirty" surveys, and surveillance, researchers compared patients with the new syndrome to a group of healthy men possessing comparable sociodemographic characteristics, experiences, or behaviors. Such research designs, which begin with outcome (the disease) and attempt to discover factors retrospectively that can account for the different health status of the two groups, are known as case-control studies. The early case-control studies were meant, in part, to test whether suspected agents such as CMV or amyl nitrite might be causative factors.
One of the first such studies, by James Goedert and his colleagues at the National Institutes of Health (NIH) and the Uniformed Services
University of the Health Sciences, explored the relationship between KS and amyl nitrite.[23]
James J. Goedert et al., "Amyl Nitrite May Alter T Lymphocytes in Homosexual Men," Lancet 1 (1982): 412-16.
Goedert attempted to assess the new disorder (the outcome) by collecting clinical, virological, and immunological information on two male homosexuals with KS and fifteen healthy homosexual volunteers. The researchers hypothesized that CMV hyperinfection and/or the chronic use of amyl nitrite might be causal variables. In presenting their results and assessing the implications, the investigators suggested that amyl nitrite inhalation may predispose homosexual men to immune deficiency.This investigation had some serious limitations. The small number of subjects in the study, for example, deprived it of the power to find statistical significance if significance existed. Moreover, though amyl nitrite was correlated with immune defects, the researchers did not report controlling for the effects of possible "confounders"—that is, alternative causal variables, such as number of sexual partners or history of infectious diseases. Notwithstanding its defects, this study was cited by others as evidence for the plausibility of amyl nitrite as a causal variable, a tribute, in part, to the power of the life-style hypothesis.[24]
As a causal factor, nitrite continues to attract research attention. For a partial list of studies that tested the association of nitrites to AIDS, see Oppenheimer, "In the Eye of the Storm," note 34, p. 295.
Almost simultaneously with the investigation by Goedert and his colleagues in Bethesda, Michael Marmor and his colleagues in New York City interviewed twenty gay men with biopsy-confirmed KS and forty gay male controls, matched for age and race, eliciting information on sociodemographic characteristics, medical history, sexual practices, and drug consumption. The cases were twenty of the twenty-one males with KS, aged fifty-two or younger, admitted to New York University Medical Center between March 1979 and August 1981. Controls were selected from the private patients of a Manhattan physician. (Since one-third of those asked to be controls refused, it is possible that the control group was skewed in some indeterminate way.) Using multivariate analysis, the investigators found that, of all the study variables, only amyl nitrite and "promiscuity" (as measured by number of different sexual partners per month in the year before onset of disease) appeared to have an independent, statistically significant association with KS.[25]
Michael Marmor et al., "Risk Factors for Kaposi's Sarcoma in Homosexual Men," Lancet 1 (1982): 1083-87.
In October 1981, approximately when the Marmor study began, the CDC undertook a multisite case-control investigation to identify risk factors for KS and PCP in gay men who lacked presdisposing clinical factors for either.[26]
Harold W. Jaffe et al., "National Case-Control Study of Kaposi's Sarcoma and Pneumocystis Carinii Pneumonia in Homosexual Men: Part I, Epidemiologic Results," Annals of Internal Medicine 99 (1983): 145-51.
The CDC chose as controls male homosexuals without KS or PCP, matched to the cases by age, race, and area of residence. Mindful that private-practice controls might not be drawn from preciselythe same population as the cases, the researchers used, where possible, multiple controls—that is, patients from both private practice and STD clinics.
Published in August 1983, the study found that KS and PCP were associated with certain aspects of male homosexuality—in particular, numerous sexual partners per year. Other significant variables were attendance at bathhouses, a history of syphilis, the use of illicit drugs (except nitrites), and exposure to feces during sex. The strong implication was that a subgroup of the male homosexual population, those who were most sexually active, was at greatest risk for KS or PCP. Taking into account the fact that AIDS had by then appeared in other segments of the U.S. population, including hemophiliacs, the authors concluded that an infectious agent might be the necessary cause of the syndrome.
Nonetheless, the CDC was unwilling to dismiss the life-style hypothesis and to commit itself completely to a microbe theory. In the second part of the study report, the authors summarized that position: "Although the cause of the acquired immune deficiency syndrome in homosexual men remains unknown, the study presented here and in the companion paper has identified a distinctive lifestyle as an important risk factor."[27]
Martha F. Rogers et al., "National Case-Control Study of Kaposi's Sarcoma and Pneumocystis Carinii Pneumonia in Homosexual Men: Part 2, Laboratory Results," Annals of Internal Medicine 99 (1983): 151.
The first heterosexual patients, including the first woman, were reported by the CDC in August 1981.[28]
MMWR, pp. 4-5.
The first clinical descriptions of immunosuppression in heterosexual intravenous (IV) drug users appeared in December 1981.[29]Masur et al., "An Outbreak."
By June 1982 the MMWR reported that 22 percent of patients with KS and/or PCP were heterosexuals, the majority IV drug users.[30]MMWR, p. 10.
Almost one-third of the heterosexual patients were women. Despite the early appearance and growing number of heterosexual patients, epidemiological studies of this group were significantly underrepresented in the literature prior to 1984.[31]For the articles published prior to 1984 on HIV infection in drug users and women, see Oppenheimer, "In the Eye of the Storm," note 51, pp. 296-97.
Would investigations of heterosexual patients, paralleling those of gays, have offered a different cast to the life-style model? We will never know for certain. Perhaps chemical toxicity or the immunosuppressive power of heroin, nitrites, and other drugs might have had more significance, at least at the start. But inasmuch as women—some of whom were not IV drug users—were among the first cases, investigators might have hypothesized much earlier that a microbe was the direct cause of the new disorder in all affected groups.
Why, we might ask, were heterosexual intravenous drug users not studied? There is no simple answer. One reason, a structural one, is that
at the federal level the National Institute on Drug Abuse (NIDA) had principal responsibility for investigating issues related to intravenous drug use and had a staff of epidemiologists just for that purpose. NIDA's traditional focus, however, was only on drug abuse; it eschewed investigations of diseases such as hepatitis B and endocarditis, which were endemic or epidemic in its target population. The leadership of NIDA decided that AIDS would be treated like any other disease, thereby leaving the research initiative to other centers at NIH or the CDC.[32]
Don C. Des Jarlais, Ph.D., former coordinator for AIDS Research, New York State Division of Substance Abuse Services, personal communication, January 15, 1988. As exceptions to that decision, NIDA funded some internal biomedical work in 1983, the same year it made a single extramural award to New York State to study risk factors for AIDS in drug users. In 1985 NIDA reversed itself and began to fund AIDS research extensively.
Unfortunately, the CDC, lacking previous experience and expertise, shied away from studying the drug-using population, leaving a lacuna.[33]Stephen Schultz, personal communication, July 27, 1987.
Another reason drug users were not studied is that only a relatively small number of research subjects were available, particularly outside the New York metropolitan area.[34]
Don C. Des Jarlais, personal communication, January 15, 1988.
That problem was alleviated, however, by the development during the summer of 1984 of a blood test measuring antibodies to the HIV. The test created a much larger pool of potential research subjects by identifying individuals who were infected but who did not have AIDS or serious related illnesses.[35]Ibid.
A final answer to the question posed is that epidemiologists were unwilling to study this group.[36]
Stephen Schultz, personal communication, July 22, 1987.
Partly justified by the disinclination of addicts to cooperate in interviews and with follow-up, their unwillingness may also, in part, be explained by a feeling among many clinicians and researchers (in this respect reflecting the attitudes of the public at large) that addicts are of less social consequence than other patients.[37]Ibid.
In a striking reflection of that lack of interest, at all levels of government and in the universities few epidemiologists had expertise in drug addiction when the HIV epidemic began.Despite its appeal, the life-style hypothesis was eventually undercut as a sufficient explanation. During 1982 epidemiological surveillance and case reports clearly indicated that others besides homosexual males were at risk. As an article in the Journal of the American Medical Association (JAMA) observed in September of that year, "if lifestyle is the key, the question still remains: Why has AIDS also occurred in heterosexual men (84 cases so far), women (32 cases so far), mostly heterosexual Haitians, and hemophiliacs?"[38]
Catherine Macek, "Acquired Immunodeficiency Syndrome Cause(s) Still Elusive," Journal of the American Medical Association 248 (1982): 1426.
A new model was required.An Unknown Transmissible Agent
On March 4, 1983, after a year of suggestive data, a Public Health Service Inter-Agency Report (published in the MMWR ) marked a major
shift in the conceptualization of the disorder.[39]
MMWR, pp. 32-34.
That shift was caused in part by the kind of evidence cited by JAMA: case reports to and surveillance by the CDC made it clear that the disease was more than a syndrome of homosexual men and promiscuous life-style.On July 9, 1982, the CDC had reported that thirty-two Haitian immigrants to the United States, seven of them women, showed immunological, morbidity, and mortality patterns similar to those in homosexual men and intravenous drug users.[40]
Ibid., pp. 12-13.
Although the MMWR had previously published two general updates on the increased incidence of the new disease—updates that had included data on heterosexual patients—the article on Haitians constituted the first complete report focusing directly on persons outside the "homosexual" category.A week later, and again in December 1982, the MMWR alerted its readers that patients with hemophilia but no other underlying disease had contracted PCP.[41]
Ibid., pp. 14-15, 24-26.
What the hemophilia patients shared was a dependence on Factor VIII, the clotting substance they lacked, usually derived from the pooled blood of two thousand to nearly twenty thousand donors.[42]Ibid., p. 47.
The possibility of blood as a vector for AIDS was heightened by a CDC report of unexplained immunodeficiency and opportunistic infection in a twenty-month-old infant who had received multiple transfusions from a donor subsequently diagnosed with AIDS.[43]
Ibid., pp. 26-27.
The sibling of the infant was in good health, and his parents were described as "heterosexual non-Haitians" without a history of intravenous drug use.Summing up the new cases, the March 4 MMWR observed that, according to current epidemiological data, four groups were at increased risk of AIDS: homosexual men with multiple sexual partners, users of intravenous drugs, Haitians who had emigrated to the United States in the previous few years, and hemophiliacs. In addition, unexplained immunodeficiency and life-threatening opportunistic infections had occurred in the female sexual partners of bisexual or intravenous drug-using men and in the children born of their unions.
Instead of life-style, the report suggested that the cases shared exposure to a transmissible agent. Though the agent was unknown, the pattern of cases mimicked that of a known pathogen, one that epidemiology had studied and helped control in the years before AIDS.[44]
W. Thomas London and Baruch S. Blumberg, "Comments on the Role of Epidemiology in the Investigation of Hepatitis B Virus," Epidemiologic Reviews 7 (1985): 59-79.
The distribution of AIDS cases parallels that of hepatitis B virus infection, which is transmitted sexually and parenterally. Blood products or blood appear responsible for AIDS among hemophilia patients who require clotting factor replacement. The likelihood of blood transmission is supported by the
occurrence of AIDS among IV drug users. Many drug abusers share contaminated needles, exposing themselves to blood-borne agents, such as hepatitis B virus.[45]
MMWR, p. 33.
In adopting the hepatitis B analogy, epidemiologists posited an alternative organization of known variables, one that stressed a biological agent whose vector was blood and/or its constituents. Although lifestyle factors could be incorporated, they had lost some of their cachet. In the CDC national case-control study, for example, Harold W. Jaffe and his colleagues, reporting their results in August 1983, suggested that life-style factors are indirect causes of AIDS, with a microbe, probably a virus, as the direct cause.[46]
Jaffe et al., "National Case-Control Study," p. 149.
Although epidemiologists had not identified an agent, the model of hepatitis B supported the introduction of public health measures. That is, the model offered a putative point of intervention in the multifactorial "web of causes," even in the absence of a known pathogen. Applying recommendations developed for hepatitis B, the Public Health Service suggested that people avoid sexual contact with persons suspected or known to have AIDS. In addition, members of groups at risk were asked not to donate blood or plasma, and doctors were encouraged to recommend autologous transfusions to their patients. Finally, the Public Health Service called for the development of blood-screening procedures.
On March 4, 1983, for the first time in the MMWR , the CDC referred to high-risk groups, attesting to the spread of AIDS into multiple segments of the U.S. population and to the relationship between the concept of high-risk group and hepatitis B. High-risk groups were those whose members were at a greater risk of infection and of infecting others, carrying a microbe that was capable of spreading through sexual and blood-borne traffic. The MMWR underscored that "each group contains many persons who probably have little risk of acquiring AIDS."[47]
MMWR, p. 32.
Nonetheless, no calibration of degree of risk was introduced, so that no distinction could be drawn. Since no microbe had been isolated, risk designation was, in effect, regarded—even among scientists, not to speak of the news media and among the general public—as synonymous with carrier state.Some months later the CDC justified its use of risk groups, arguing that classification of individuals is intrinsic to any epidemiological investigation.[48]
Ibid., p. 45. Whatever the scientific basis for these high-risk groups, their existence was also open to negotiation. For a short discussion of the successful pressure applied by the Haitian government to have Haitians dropped as a risk group, see Dennis Altman, AIDS in the Mind of America (Garden City, N.Y.: Doubleday, 1986), pp. 71-73.
Classification should not be taken to mean, however, that groups at higher risk for AIDS could transmit the disease through nonintimate contact, since casual transmission was a view unsupported byavailable evidence. To use the likelihood of casual transmission as a basis for social and economic discrimination was unfair.
The apology of the CDC missed the point. Grouping individuals may be traditional in epidemiology, both as a means of intervention and as an analytic prerequisite. The political or social consequences of such grouping are rarely examined. In this instance, even if the fear of casual transmission could be eradicated, the groups identified would still be seen as bearing a strong negative relationship to the life-sustaining blood supply. They were created, qua groups, to signify their potential status as carriers of tainted blood and as contaminators. Moreover, the analogy with highly contagious hepatitis B reinforced the association of casual transmission, particularly for health care providers, because hepatitis B is a disease in which a virus is transmitted through close personal contact, through all secretions, and through wounds and lacerations.[49]
Abram S. Benenson, ed., Control of Communicable Diseases in Man, 12th ed. (Washington, D.C.: American Public Health Association, 1975).
A further consequence of creating high-risk groups was to reinforce the relationship between the disease and "marginal" members of the population. In the case of HIV, although each of the groups ostensibly threatened the remainder of the community through the medium of blood or sex, public health recommendations would inhibit such contamination. Consequently, the disorder could be contained at the boundaries, among people who were "different" from the majority but undifferentiated within each of the high-risk groups.
One of the dangers of a scientific classification of people based on stereotypes was that it defined the questions raised and thus answered. Such categorization created a procrustean mind-set that was evident from the beginning of the epidemic. For example, in early 1982 researchers, in an act of political and scientific oversimplification, designated the new disorder by the acronym GRID (gay-related immunodeficiency), even though the CDC and the New England Journal of Medicine had published reports of heterosexual IV drug users with the new syndrome. At a major conference Michael Gottlieb and his colleagues could report, in a paper entitled "Gay-Related Immunodeficiency (GRID) Syndrome: Clinical and Autopsy Observations," that of the ten adult males in the study with the syndrome, two were exclusively heterosexual.[50]
Michael S. Gottlieb et al., "Gay-Related Immunodeficiency (GRID) Syndrome: Clinical and Autopsy Observations," Clinical Research 30 (1982): 349A.
Ultimately, the hepatitis B metaphor assumed the existence of an infectious agent, probably a virus. Though some favored a new variant of the cytomegalovirus, others, including James W. Curran of the CDC Task Force, supported the notion of a new infections agent.[51]
Jean L. Marx, "A New Disease Baffles Medical Community," Science 217 (1982): 619; Robert C. Gallo, "The AIDS Virus," Scientific American 256 (1987): 48. James Curran was showing slides demonstrating the plausibility of a viral etiology at scientific meetings as early as February 1982 (Pauline Thomas, M.D., director of AIDS surveillance, New York City Department of Health, personal communication, July 28, 1987).
In thelong run, either hypothesis rested on the detection of a pathogen that had hitherto proved elusive.
Aids: "The Story Of A Virus"
From 1981 until the isolation of a new virus, epidemiology played a central role in the characterization of HIV infection. That discipline, using specific case definitions, surveillance, and case-control studies, identified high-risk groups and offered suggestive models and similes. Although epidemiology formulated the social context and morphology of the new disorder, it could not discover its microbial cause. That function was filled by virologists at the Pasteur Institute in Paris and in laboratories in the United States, at the National Cancer Institute (NCI) in particular.
In May of 1984 the journal Science published four reports authored by Robert C. Gallo of the NCI and his colleagues and a fifth by Luc Montagnier of the Pasteur Institute.[52]
Science 224 (1984): 497-508.
These reports established a strong case for a causal link between AIDS and a newly discovered retrovirus that the NCI called HTLV-III and the French called LAV. Later an international agreement was made to call the retrovirus human immunodeficiency virus (HIV).With the isolation of the HIV, the relative importance of epidemiology in the definition of the disease lessened. Epidemiologists continued to play an important, although somewhat more peripheral, role, providing supporting evidence for the viral hypothesis and developing information in areas outside the reach of microbiology and its techniques.
Increasingly, the "bench" scientists—virologists, immunologists, cancer researchers—determined the definition of HIV infection. In effect, they redefined AIDS as a set of biomedical problems open to a chemical resolution in the form of drugs and vaccines. These scientists removed the disorder to a considerable degree from the stigma of its original social matrix, placing it instead in a context resembling that of the supposedly more purely clinical crusades against cancer or polio.
The change in the types of professionals studying HIV infection and in their defined fields of observation and analysis effected a subtle shift in the characterization of the disorder. The disease was increasingly conceptualized in terms of the infections agent, the virus. Interest in cofactors or a multifactorial model diminished.
One marker of this shift was the title of a book published by the
Institute of Medicine and the National Academy of Sciences in 1986: Mobilizing against AIDS: The Unfinished Story of a Virus .[53]
Eve K. Nichols, Mobilizing against AIDS: The Unfinished Story of a Virus (Cambridge, Mass.: Harvard University Press, 1986).
Four years earlier, an article in JAMA had observed that "it seems unlikely that a virus alone is inducing AIDS."[54]Macek, "Acquired Immunodeficiency Syndrome Cause(s) Still Elusive," p. 1425.
Another marker was the dearth of studies of cofactors, of events or states independent of the virus but necessary to cause HIV infection in general or AIDS in particular. In early 1987 an article evaluating cofactors for HIV could cite only one published report on cofactors after 1984.[55]James J. Goedert et al., "Effect of T4 Count and Cofactors on the Incidence of AIDS in Homosexual Men Infected with Human Immunodeficiency Virus," Journal of the American Medical Association 257 (1987): 334.
A few months earlier, another volume by the Institute of Medicine and the National Academy of Sciences, although acknowledging the importance of cofactors, suggested that "there are no data to support the concept [of cofactors], with the possible exception of genital ulcers in Africa."[56]Institute of Medicine and National Academy of Sciences, Confronting AIDS (Washington, D.C.: National Academy Press, 1986), p. 45 (hereafter cited as Confronting AIDS).
The increasingly biological definition of the disease was reinforced by the successful development of serological procedures for the detection of antibodies to the virus. These tests—the enzyme-linked immunosorbent assay (ELISA) and the Western blot technique—allowed epidemiologists and other scientists to outline the biological boundaries of the new disorder.
IN July 1986 the CDC reported that epidemiologists, using the new blood tests, had confirmed that persons in the previously defined groups at higher risk of AIDS showed a greater prevalence of HTLV-III/LAV viral antibody.[57]
MMWR, p. 63.
Epidemiologists also found that AIDS and a number of less full-blown conditions, including lymphadenopathy and AIDS-related complex (ARC), had the same underlying viral cause. In addition, antibody tests demonstrated the existence of the virus in persons without clinical symptomatology, a not unusual pattern in infectious disease epidemiology. These data suggested to the CDC a wide spectrum of human response to the virus, requiring careful study.[58]Ibid.
Standardized blood tests thus initially provided a biological justification for the previously defined high-risk groups. At the same time, antibody testing could determine which individuals within the risk groups were seropositive and which were not. As a result, group membership and carrier status could theoretically be separated. Given the logic of the biological model, moreover, the concept of high-risk membership should actually have withered away, replaced by the notion of high-risk activities that made infection more likely. Despite logic, a shift in emphasis from "status" to "act" did not occur until "mainstream" heterosexuals were targeted as a population at risk.[59]
See, for example, Confronting AIDS, pp. viii-ix.
Since 1984 epidemiologists have also contributed to knowledge of the natural history and transmission of HIV infection. The particular strength
of epidemiology in these areas has derived in part from the "bench" scientists' inability to uncover suitable nonhuman animal models and in part from epidemiologists' technical ability to transcend the ethical limitations on human experimentation by studying disease patterns occurring in populations.
Overall, these epidemiological studies are attempting to enlarge our knowledge of the biological and clinical dimensions of HIV infection, but to develop that knowledge, wherever possible, within the social matrix or behavioral history of the populations involved. By so doing, epidemiologists are maintaining the vitality of a multifactorial, social conception of AIDS in the face of a narrower biological definition.
To date, some of the most important epidemiological studies have prospectively followed defined cohorts of individuals—at first cohorts of homosexual men, but more recently cohorts of hemophiliacs, intravenous drug users, women, and children.[60]
For recent results of cohort studies involving one or more of these groups, see papers presented at the Sixth International Conference on AIDS, San Francisco, June 20-24, 1990.
The purpose of these investigations has been to establish the risk factors for HIV infection; the rate of, and time required for, seroconversion; the progression of pathology in those infected; and the proportion of the infected who eventually develop AIDS. In addition to defining the natural history of the disorder, the researchers aim to find determinative variables that may be open to clinical or social intervention. Finally, epidemiologists continue to develop more extensive and sophisticated means to measure the incidence and prevalence of HIV infection across subgroups in the American population.For example, a number of studies that followed gay or bisexual men over time in New York City,[61]
Cladd E. Stevens et al., "Human T-Cell Lymphotropic Virus Type III Infection in a Cohort of Homosexual Men in New York City," Journal of the American Medical Association 255 (1986): 2167-72.
Holland,[62]Godfried J. P. van Griensven et al., "Risk Factors and Prevalence of HIV Antibodies in Homosexual Men in the Netherlands," American Journal of Epidemiology 125 (1987): 1048-57.
and San Francisco[63]Warren Winkelstein, Jr., et al., "Sexual Practices and Risk of Infection by the Human Immunodeficiency Virus," Journal of the American Medical Association 257 (1987): 321-25.
isolated several possible risk factors for HIV infection. These included sexual contact with a person known to have AIDS and participation as the receptive partner in anal intercourse,[64]Stevens et al., "Human T-Cell Lymphotropic Virus," p. 2169; Winkelstein et al., "Sexual Practices," p. 323.
a risk that increased with the number of persons with whom one acted as the anal receptive partner.[65]Van Griensven et al., "Risk Factors," p. 1055.
These behaviors heightened the chance of viral transmission. Implicated as well was a history of anal douche use.[66]Winkelstein et al., "Sexual Practices," p. 324. For problems with the early cohort studies, see Oppenheimer, "In the Eye of the Storm," p. 288 and note 95, p. 299.
In the population studied, therefore, HIV infection is an STD in which anal mucosa appears to be an inefficient barrier to infection, especially when traumatized by frequent contact. These results, consistent over many epidemiological studies, offered the possibility of behavior intervention strategies.When epidemiologists have researched the natural history of HIV-associated disorders in infected persons, they have provided information on incidence and prevalence rates and, in the main, on biological markers and disease status. Their attempts to isolate cofactors for HIV
infection and progression have yielded, at best, some suggestive leads that must be interpreted with great caution. In addition, these investigations, like those discussed above, suffer from design flaws and biases. For example, most studies cannot specify the dates of HIV infection in their subjects. Consequently, endpoints (lymphadenopathy, for example, or AIDS) cannot be linked to and measured from precisely defined initiatory events. This lacuna often inhibits comparisons of findings across studies and prediction of time-measured outcomes. Recently, however, investigators have attempted both, using as their point of departure the few cohorts (primarily patients infected by blood products) with known or well-estimated dates of seroconversion.[67]
Andrew R. Moss and Peter Bacchetti, "Natural History of HIV Infection," AIDS 3 (1989): 56.
One of the first epidemiological studies of the course of HIV infection was that of Harold Jaffe and his colleagues, which followed a cohort of 6,875 male homosexuals and bisexuals recruited originally between 1978 and 1980 from STD patients at San Francisco City Clinic.[68]
Harold Jaffe et al., "The Acquired Immunodeficiency Syndrome in a Cohort of Homosexual Men," Annals of Internal Medicine 103 (1985): 210-11.
The researchers found that, by 1984, 87.4 percent of a putative random sample[69]About one-third of the sample refused to participate.
of the cohort were seropositive. More recently investigators have estimated that 54 percent of those seropositive for at least ten years will progress to AIDS.[70]A. Lifson et al., "The Natural History of HIV Infection in a Cohort of Homosexual and Bisexual Men: Clinical Manifestations, 1978-1989," paper presented at the Fifth International Conference on AIDS, Montreal, June 4-9, 1989.
These results suggest that without effective treatment a majority of those infected with HIV will eventually develop the last, usually fatal, stage of the disease.B. Frank Polk and his colleagues, unlike Jaffe and his colleagues, attempted to define predictors of AIDS in seropositive men by studying a cohort of 1,835 male homosexual volunteers recruited by centers in four cities: Los Angeles, Chicago, Pittsburgh, and Washington/Baltimore.[71]
B. Frank Polk et al., "Predictions of the Acquired Immunodeficiency Syndrome Developing in a Cohort of Seropositive Homosexual Men," New England Journal of Medicine 316 (1987): 61-66.
When each of the fifty-nine AIDS cases (developing over a median of fifteen months) was matched to five seropositive controls from the same study center, the researchers found three independent predictors of AIDS: a decreased number of T helper cells, a low level of HIV antibody, and a history of sex with someone who subsequently developed the syndrome. The first two predictors, however, are probably biological markers of disease progression to AIDS rather than determinants or causes of that progression. The last predictor may in fact be a marker of an infection longstanding enough for AIDS to develop in both partners. More recent epidemiological investigations of HIV-infected homosexual men and men with hemophilia have identified additional laboratory markers of progression to AIDS.[72]Andrew R. Moss, "Predicting Who Will Progress to AIDS," British Medical Journal 297 (1988): 1067-68; Moss and Bacchetti, "Natural History," pp. 57-58.
Cohort studies have also provided the basis for estimates of the "latency period," the median time between an initial infection and frank AIDS. In seropositive homosexual men, transfusion recipients, and hemophiliacs,
the latency period is an estimated seven to eleven years; and half of those infected are free of AIDS for an indefinitely longer term.[73]
Andrew R. Moss et al., "Seropositivity for HIV and the Development of AIDS or AIDS Related Condition: Three Year Follow Up of the San Francisco General Hospital Cohort," British Medical Journal 296 (1988): 745-50; Moss and Bacchetti, "Natural History," pp. 56-57; Alvaro Munoz et al., "Acquired Immunodeficiency Syndrome (AIDS)-Free Time after Human Immunodefiency Virus Type 1 (HIV-1) Seroconversion in Homosexual Men," American Journal of Epidemiology 130 (1989): 530-39.
This highly variable latency period will probably be extended further, moreover, with the prophylactic administration of AZT.[74]Gina Kolata, "Strong Evidence Discovered That AZT Holds Off AIDS," New York Times, August 4, 1989, p. A1; Philip J. Hilts, "Drug Said to Help AIDS Cases with Virus but No Symptoms," New York Times, August 18, 1989, p. A1.
In fact, new evidence appears to show that for some individuals the period between HIV infection and the appearance of persistent antibodies to HIV may be even longer than previously suspected. For some years, the normal period was thought to be three months or less.[75]
Moss and Bacchetti, "Natural History," p. 55.
Investigators in Los Angeles, however, have recently reported multiple instances of delayed seroconversion.[76]David T. Imagawa et al., "Human Immunodeficiency Virus Type 1 Infection in Homosexual Men Who Remain Seronegative for Prolonged Periods," New England Journal of Medicine 320 (1989): 1458-62.
Although HIV was isolated from 31 of 133 homosexual men, 27 of the 31 had no antibodies to HIV during the next thirty-six months of follow-up when their sera were tested by the ELISA and Western blot methods. Confirming the results of previous investigations,[77]Steve Wolinsky et al., "Polymerase Chain Reaction (PCR) Detection of HIV Provirus before HIV Seroconversion," paper presented at Fourth International Conference on AIDS, Stockholm, June 12-16, 1988; M. Loche and B. Mach, "Identification of HIV-Infected Seronegative Individuals by a Direct Diagnostic Test Based on Hybridisation to Amplified Viral DNA," Lancet 2 (1988): 418-21.
this study suggests that for an unknown number of individuals a "silent HIV infection," undetectable by conventional blood assays, may be, in fact, part of the latency period.These recent results carry several further implications. They raise questions about the limitations of current serum antibody tests, particularly worrisome if those with "silent" HIV infection can still transmit the virus. On a more positive note, these results suggest that some infected individuals have immune systems that successfully suppress the replication of HIV indefinitely. This finding has potentially profound implications for future drug research and therapy.
Why does HIV disease have such a variable incubation period? This question intrigues researchers and has renewed their interest in cofactors—exogenous or endogenous exposures that might modulate the rate of HIV-induced immunodeficiency.[78]
Confronting AIDS, p. 193.
Investigators have also hypothesized that cofactors may promote initial HIV infection. For example, some have suspected that a history of microbial infections, leading to immunological alterations, may put individuals at greater risk of HIV infection and of disease progression.[79]Thomas C. Quinn et al., "Serologic and Immunologic Studies in Patients with AIDS in North America and Africa," Journal of the American Medical Association 257 (1987): 2617-21.
There is growing evidence that sexually transmissible infections—particularly those that produce genital ulcerations, which, like douching and enemas, facilitate invasion of HIV—may be important cofactors.[80]Peter Piot et al., "Serum Antibody to Haemophilus Ducreyi as a Risk Factor for HIV Infection in Africa, but Not in Europe"; Edward E. Telzak et al., "A Prospective Cohort Study of HIV-1 Seroconversion in Patients with Genital Ulcer Disease in New York City"; and Robert Cannon et al., "Syphilis Is Strongly Associated with HIV Infection in Baltimore STD Clinic Patients Independent of Risk Group"—all presented at Fifth International Conference on AIDS, Montreal, June 4-9, 1989. See also Jacques Pepin et al., "The Interaction of HIV Infection and Other Sexually Transmitted Diseases: An Opportunity for Intervention," AIDS 3 (1989): 3-9.
Evidence is also accumulating that, for reasons not yet understood, lack of circumcision in African men may be a cofactor for HIV infection.[81]Jean L. Marx, "Circumcision May Protect against the AIDS Virus," Science 245 (1989): 470-71; J. Bongaarts et al., "The Relationship between Male Circumcision and HIV Infection in African Populations," paper presented at the Fifth International Conference on AIDS, Montreal, 1989.
According to some researchers, the simultaneous existence of genital ulcers in HIV-infected women and lack of circumcision in their partners may potentiate female to male transmission of the virus.[82]D. William Cameron et al., "Female to Male Transmission of Human Immunodeficiency Virus Type 1: Risk Factor for Seroconversion in Men," Lancet 2 (1989): 403-7.
There are also epidemiological indications that age-related variables may be cofactors for disease progression, sinceinfants and older homosexual men have higher rates of disease progression than other groups.[83]
Angelos Hatzakis et al., "Age at Time of HIV Infection as Cofactor of Progression to Advanced Immune Dysfunction and AIDS," paper presented at the Fifth International Conference on AIDS, Montreal, 1989; J. Roy Robertson et al., "Progression to AIDS in Intravenous Drug Users, Cofactors and Survival," paper presented at the Sixth International Conference on AIDS, San Francisco, 1990.
The possible role of cofactors testifies to the terrible complexity of HIV infection and justifies the reluctance of epidemiologists to reduce AIDS and related conditions to an agent-host phenomenon. Epidemiological researchers have consistently held up the possibility of nonviral factors to the "bench" scientists. Since 1981 they have rooted biological or clinical events in the matrices of human behavior and social experience. In one study of the role of cofactors in HIV infection, the authors put the epidemiologists' position quite well.[84]
Quinn et al., "Serologic and Immunologic Studies," pp. 2617, 2620.
Citing the viral etiology common to all patients with AIDS, they stressed the multiple determinants probably responsible for HIV infection and disease progression, including cultural differences, the presence of other endemic illnesses, and host and viral genetic factors. Their position reaffirms the multifactorial model as central to an understanding of HIV infection and to its control.From Aids To Hiv Infection: Tracking The Epidemic
While investigating the natural history of HIV infection, epidemiologists have continued to hold responsibility for an apparently mundane task: systematic surveillance. Since 1981 the CDC has both constructed the surveillance case definitions of AIDS and served as the national registry for all cases reported by the states, the District of Columbia, and the U.S. territories.[85]
AIDS has been a reportable condition since 1983, when the Council of State and Territorial Epidemiologists passed a resolution to that effect.
These data are used to monitor the spread of AIDS, project its future incidence and prevalence,[86]James W. Curran et al., "Epidemiology of HIV Infection and AIDS in the United States," Science 239 (1988): 610-16; Karon, Dondero, and Curran, "Projected Incidence of AIDS."
and provide the basis for health service planning and health education.In recent years, however, the systematic surveillance of cases has grown more problematic. Sources within and outside the CDC have observed that the true number of AIDS cases in the United States has been underreported, thereby weakening the epidemiological and policy functions the data serve. In addition, once the HIV virus was isolated, epidemiologists sought strategies to capture population-based information on HIV seroprevalence in general, not only on AIDS, the last stage of the disease. Methods developed by epidemiologists—the CDC in particular—to survey HIV prevalence put them at odds with other quantitative research workers and, for the first time, threatened the monopoly previously enjoyed by epidemiologists over the population-based definition of the disease.
In an editorial note in the MMWR of August 18, 1989, the CDC admitted that its AIDS case count was subject to error: "Because of the combination of underdiagnosis and underreporting of AIDS cases and severe manifestations of HIV infection that do not meet the CDC AIDS surveillance case definition, reported AIDS cases underestimate the number of persons severely affected by HIV since 1981."[87]
MMWR 38 (1989): 562.
Since the completeness of the case count varied by geographical region and patient population, the CDC surveillance system had captured only 70 to 90 percent of HIV-related deaths.In a separate assessment of the CDC's system for reporting AIDS cases, the Committee on AIDS Research and the Behavioral, Social and Statistical Sciences of the National Research Council (NRC) highlighted two problems: only 85 to 90 percent of cases are reported within one year of diagnosis, with a further decline expected; and the reliability and validity with which the mode of transmission of infection is established in each case have not been evaluated.[88]
Charles F. Turner, Heather G. Miller, and Lincoln E. Moses, AIDS, Sexual Behavior and Intravenous Drug Use (Washington, D.C.: National Academy Press, 1989), pp. 32-33.
Flaws in the CDC's methodology for establishing mode of transmission could affect the degree to which subpopulations are over- or underrepresented in the national surveillance system; such misreporting might have serious implications for identifying or tracking shifts in the spread of infection.Indeed, in a recent study the sociologist E. O. Laumann and his colleagues concluded that some segments of the U.S. population are systematically underrepresented. Arguing that the national reporting system is subject to systematic distortions because of "overt manipulations by interested parties" and the stigmatizing nature of HIV infection itself,[89]
E. O. Laumann et al., "Monitoring the AIDS Epidemic in the United States: A Network Approach," Science 244 (1988): 1186. By "overt manipulations" the authors mean that the highly decentralized CDC reporting system allows individual physicians and hospitals considerable opportunities to hide cases of AIDS if they have an interest in doing so (John H. Gagnon, personal communication, August 31, 1990).
the investigators used instead the 1988 General Social Survey (GSS), a national household survey in which respondents were asked to identify all those within their network of acquaintances who had either been a victim of homicide or had AIDS. When the GSS results were compared with official national statistics on homicide, the two were congruent. When a similar comparison was made between GSS survey data and those of the CDC, the investigators found that the national surveillance system significantly underestimated the prevalence of AIDS in white middle-class populations and in those living in the Midwest, while overstating the prevalence of that disease in blacks and latinos and in those living in the East. The researchers called for more prevalence studies independent of the CDC's surveillance network, in order to ensure a more accurate assessment of the social epidemiology of AIDS.The most critical evaluation of the national AIDS surveillance system is that of the U.S. General Accounting Office (GAO).[90]
U.S. General Accounting Office, AIDS Forecasting: Undercount of Cases and Lack of Key Data Weaken Existing Estimates (Washington, D.C.: General Accounting Office, June 1989). A study published some months later, albeit based on the experience of only one state, found that only an estimated 60 percent of AIDS cases in South Carolina were reported to the state's registry in 1986 and 1987. See George A. Conway et al., "Underreporting of AIDS Cases in South Carolina, 1986 and 1987," Journal of the American Medical Association 262 (1989): 2859-63.
The GAO hasfound that the system substantially undercounts the number of AIDS cases in the United States. It attributes that problem to essentially four sources, some already identified above. In essence, these sources are (1) the CDC's surveillance definition, which specifies those illnesses that qualify a case as AIDS and thereby excludes a considerable number of fatal HIV-related cases—in particular, young intravenous drug users—who never contract the required diseases;[91]
Rand L. Stoneburner et al., "A Larger Spectrum of Severe HIV-1 Related Disease in Intravenous Drug Users in New York City," Science 242 (1988): 916-19.
(2) the CDC's test criterion, which excludes from the national surveillance system all cases of AIDS diagnosed without HIV test results—despite the fact that such presumptive diagnoses are not rare and are increasing as physicians become more experienced with AIDS and as patients insist that no test results be attached to their medical charts; (3) physician error, as a consequence of which AIDS cases go undiagnosed or are diagnosed late; and (4) surveillance system breakdown, in which diagnosed cases are never reported or are reported late.The GAO estimates that, because of these and other sources of error, the national surveillance system may have counted only two-thirds of the cases of AIDS and other HIV-related fatal illnesses in the United States—an estimate that is lower than the CDC's own estimate of 70 to 90 percent. Whatever the precise shortfall, the combined results of the GAO and other studies suggest that the current AIDS case count may be sufficiently flawed to affect health planning or estimates of future cases, particularly for subpopulations or specified regions of the country. Unfortunately, similar, though perhaps more profound, flaws may be vitiating the recent HIV surveillance projects.
The need to monitor HIV infection rather than only AIDS was clearly adumbrated by the Committee on AIDS Research and the Behavioral, Social and Statistical Sciences of the NRC:
Counts of AIDS cases are out-of-date indicators of the present state of the epidemic. There is a long, asymptomatic latency period between HIV infection and the development of AIDS (in most persons). Consequently, the statistics on new AIDS cases reflect old cases of HIV infection. … [In addition,] persons whose life spans are significantly shortened by HIV infection do not always manifest sufficient symptoms to be captured by the AIDS reporting system. … [Finally,] the future magnitude of the AIDS epidemic will be determined primarily by the current extent and future spread of HIV infection in the population.[92]
Turner, Miller, and Moses, AIDS, pp. 31-32.
The CDC recognized the need for HIV seroprevalence data quite early. In the fall of 1985, six months after the ELISA was licensed, the CDC proposed that selected "sentinel" hospitals across the country provide
sera for "blinded" seroprevalence surveys—surveys that use anonymous samples of blood and therefore do not require informed consent, so that they are relatively free of self-selection bias.[93]
Ronald Bayer, L. H. Lumey, and Lourdes Wan, "The American, British and Dutch Responses to Unlimited Anonymous HIV Seroprevalence Studies: An International Comparison," AIDS 4 (1990): 283-90.
Once initiated, this plan was followed by another, outlined in September 1987 and implemented thereafter,[94]
U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, Human Immunodeficiency Virus Infections in the United States: A Review of Current Knowledge and Plans for Expansion of the HIV Surveillance Activities, a Report to the Domestic Policy Council (Washington, D.C.: DHHS, November 30, 1987).
to develop a "comprehensive family of complementary HIV surveys" that would capture seroprevalence information on pregnant women, those at high risk of HIV infection, and selected subgroups within the general population.[95]Timothy J. Dondero, Jr., Marguerite Pappaioanou, and James W. Curran, "Monitoring the Levels and Trends of HIV Infection: The Public Health Service's HIV Surveillance Program," Public Health Reports 103 (1988): 213-20.
Specifically, the CDC agreed to provide technical and financial support to thirty large metropolitan areas across the United States.[96]Of the thirty large metropolitan areas, twenty are cities that report 75 percent of the current cases of AIDS; the remaining ten were selected from cities with moderate to low prevalence of AIDS.
In each of these urban areas, the federal government, in collaboration with state and local agencies, selected in a nonrandom fashion one or more of six types of health care institutions or groups: sentinel hospitals, newborn infants, tuberculosis clinics, STD clinics, drug treatment centers, and women's health centers. Only "blinded" surveys are conducted in the first three; "blinded" and "unblinded" studies in the last. (Such "unblinded" studies allow investigators to ask in-depth questions, but they require informed consent of the respondents and run the risk, as recent studies have shown, of self-selection bias—the nonrandom refusal of some, perhaps those at greatest risk, to participate.[97]Harry F. Hull et al., "Comparisons of HIV-Antibody Prevalence in Patients Consenting to and Declining HIV-Antibody Testing in an STD Clinic," Journal of the American Medical Association 260 (1988): 935-38.
) According to the CDC, the family of surveys is central to defining and managing the problems presented by HIV infection: "Information on current levels and trends of HIV infection is needed to follow the course of the epidemic, to help project future trends in AIDS incidence, and to target and evaluate the impact of AIDS/HIV preventive programs."[98]U.S. Centers for Disease Control and National Institute on Drug Abuse, "Proposal for Monitoring HIV Seroprevalence in Intravenous Drug Users in Treatment, National HIV Seroprevalence Surveys," CDC Protocol No. 840, 1988.
The CDC has elected to use health care institutions to capture prevalence information, a traditional epidemiological strategy. The types of facilities selected allow it to obtain seroprevalence data on those at greatest risk of infection: the sexually active (STD clinics), intravenous drug users (drug treatment and tuberculosis clinics), and childbearing or reproductive-age women in lower socioeconomic strata (newborn screening and women's health centers). The CDC admits that the survey design for each of these subpopulations is flawed. It hopes, however, to analyze and evaluate the biases in each design and to compensate for them statistically, so that it can provide accurate prevalence estimates.[99]
Karon, Dondero, and Curran, "Projected Incidence of AIDS," p. 547.
The Committee on AIDS Research and the Behavioral, Social and Statistical Sciences of the NRC, advised by a panel of statisticians and demographers, has examined the six surveys in depth. It found that, contrary to the CDC's expectations, the "comprehensive family of surveys" is sufficiently flawed in research design to prevent it from accurately
measuring, with knowable margins of error, the incidence or prevalence of HIV infection in the subpopulations of interest. Central to the committee's criticism is that the CDC is using nonrandom samples—samples of convenience—in all surveys except newborn screening.[100]
Turner, Miller, and Moses, AIDS, pp. 52-62.
The committee's subsequent conclusions are unequivocally critical of the CDC:The committee has listened with interest to arguments that population-based estimates of HIV incidence and prevalence are unnecessary from a public health perspective. Rather, it has been suggested that targeted samples of convenience could suffice to provide "sentinels" that could be used to guide the nation's response to the AIDS epidemic. The committee concludes that it would be a serious mistake for the Public Health Service to continue to "make do" with estimates derived from convenience samples . … Now is the time to prepare for the future, and good data will be indispensable in future efforts to control the epidemic. No postponement should be accepted.[101]
Ibid., pp. 68-70.
To meet its objections, the committee suggests that the CDC reconstitute each of the seroprevalence surveys as probability samples, despite the administrative, political, and financial difficulties involved. In reformulating the surveys, the committee urges the CDC to draw on the expertise of the National Center for Health Statistics (recently made a part of the CDC), which employs statisticians, demographers, and other social scientists.[102]
Ibid., p. 7.
The committee does not comment, however, on another significant limitation of the "comprehensive family of surveys." These surveys are limited to groups historically at risk of HIV infection and to a special subgroup, the hospitalized sick, which only in part includes those at low risk. The CDC's surveys do not, however, measure seroprevalence in the population at large and therefore cannot estimate, with known margins of error, the prevalence of HIV in the United States. In addition, the surveys cannot monitor the incidence of HIV in new, previously unknown, risk groups.[103]Other federal agencies measure seroprevalence in segments of the general population—for example, civilian applicants for military service, active-duty military personnel, and Job Corps entrants; but the results obtained are flawed by self-selection bias.
Responding to the need to measure HIV prevalence in the general population, the National Center for Health Statistics (NCHS) has sponsored a National Household Seroprevalence Survey (NHSS), contracting with a private research organization, the Triangle Research Institute (TRI), to conduct feasibility tests. The ultimate objective of the NHSS will be to survey 50,000 anonymous household respondents concerning factors that might put them at risk for HIV infection and to take a blood sample from each participant. These respondents are to be randomly selected on the basis of probability sampling; the result should
be an estimate of HIV prevalence in the total U.S. population. Before the government approves the survey, however, a pilot stage must successfully demonstrate that the study is feasible and can generate new and useful data.[104]
Research Triangle Institute, "National Household Seroprevalence Survey, Pilot Study Summary Report," Contract No. 200-88-0605, Research Triangle Park, N.C., April 1989, p. 1.
Specifically, the pilot involves a careful evaluation of all field procedures and research methodologies, including sampling strategies, protection of the respondents, blood collection methods, survey design, and development of community support.After an aborted start in Washington, D.C., where local officials and community groups rejected the project, TRI successfully piloted the NHSS in Allegheny County, Pennsylvania, in January 1989; it initiated a second study in Dallas in September of the same year. The results from Pennsylvania show that, of 308 randomly selected households with an eligible respondent (a civilian, permanent resident, eighteen to fifty-four years of age), 85 percent agreed to participate in the study.[105]
Ibid., p. 7.
In Dallas a survey of 1,715 eligible households, completed in December 1989, achieved an overall response rate of 84 percent (90 if one includes those who completed the questionnaire but refused to be bled). Reaching that number proved somewhat more difficult than anticipated, because the leading gay political and service organization in the city, the Dallas Gay Alliance, actively campaigned against the survey.[106]On the Dallas survey, see National Center for Health Statistics, "Report on the Dallas County Household HIV Survey," Hyattsville, Md., May 1990; and Bruce Lambert, "Dallas AIDS Survey Is Begun amid a Furor over Its Worth," New York Times, September 27, 1989, p. A1.
With the feasibility studies completed, the CDC, along with other federal bodies, must now decide whether a national seroprevalence survey is technically and politically possible. The fierce local controversies in Washington and Dallas make political considerations important; so, too, do actions in Congress, where in July 1989 conservative members of the House Appropriations Committee were able to delete the $11 million required to fund a Public Health Service survey of sexual behavior in the United States.[107]
Michael Specter, "Funds for Sex Survey Blocked by House Panel," Washington Post, July 26, 1989, p. A3.
However, the CDC reportedly has an antipathy to the NHSS that predates and is independent of these political considerations.[108]Privileged communication.
The epidemiologists of the Centers for Disease Control had argued early on that the study, requiring blood samples and a survey of sex- and drug-related behaviors, would be vitiated by nonresponse bias; it would be bad science. They also insisted that the NHSS was politically untenable, in that it needed substantial outreach in the face of community opposition. Finally, the NHSS would consume funds that were better spent on the family of surveys, which, with its use of "blinded" seroprevalence studies, was unbiased (good) science.The arguments raised by the CDC regarding the scientific and political feasibility of the NHSS are somewhat disingenuous, in that they hide a struggle on the part of the CDC to maintain the hegemony of its
own mission and culture over the HIV "territory."[109]
Privileged communication.
The CDC has dominated the population-based study of AIDS since 1981. It has defined the disease for surveillance purposes, directed the national AIDS-reporting system, and designed the "comprehensive family of surveys" to expand that system to the whole spectrum of HIV infection. That design was based on traditional medical epidemiology; to measure rates of disease, the CDC has used patient data captured within health care institutions. After almost a decade of work and achievement, "accomplished in the face of considerable adversity on a number of fronts—physical, diplomatic, political and administrative"[110]Turner, Miller, and Moses, AIDS, p. 70.
—it would be strange if the CDC did not feel that if "owns" to a large degree the population-based study of HIV (as does epidemiology, through it). It would be surprising for the CDC to easily relinquish its funding, political power, and high visibility.The CDC experiences as an incursion the criticism and critical work of quantitative social scientists, most of whom are relatively new to AIDS research. These social scientists' insistence on population probability sampling—the General Social Survey or the NHSS, for example—as the basis of good science at least temporarily excludes the CDC. The CDC has little experience with the methodologies involved, and the CDC staff in Atlanta includes no sampling statisticians and precious few quantitative social scientists on the Ph.D level.[111]
Ibid., p. 24.
To alter course now requires the CDC to change both corporate strategy and corporate culture and to allow non-epidemiologists, with their own mission and culture, to participate in the population-based definition of HIV. The CDC is loath to share this territory, and a certain degree of inflexibility, even dogmatism, has followed. For example, the leadership of the CDC has made its calculation of 1 to 1.5 million HIV seropositive individuals in the United States an article of faith, despite the fact that the figure is only an estimate, based on much-criticized parameters.[112]Privileged communication. In 1986 the CDC estimated that 1 to 1.5 million people in the United States were infected with the HIV, a range that it modified the next year to between 945,000 and 1.4 million; see Institute of Medicine and National Academy of Sciences, Confronting AIDS: Update 1988 (Washington, D.C.: National Academy Press, 1988), p. 51. Early in 1990 the CDC changed the estimate slightly to between 800,000 and 1.3 million.
The social scientists who criticize the manner in which the CDC defines cases or collects the data are demanding something more than greater methodological purity—although that is important. They are also frustrated by the dominant role played by the CDC and other epidemiologists in defining and managing the HIV epidemic. Their criticism of the CDC is only the most public expression of anger at the power and apparent insensitivity of epidemiologists, who are seen as excluding, devaluing, or co-opting social science methodologies and objectives. Social scientists argue there are sound reasons for multiple approaches to studying the epidemic. Such approaches would, for example,
enable researchers to analyze with greater sophistication the personal (particularly the sexual) behavior of individuals; to measure the unique, local configurations and manifestations of the HIV epidemic; and to develop models of the political economy of that epidemic.[113]
John H. Gagnon, personal communication, August 31, 1990.
In brief, social scientists want badly to broaden the theoretical and empirical basis for the study and management of the epidemic. Such a change, in which they would have a greater voice in defining public policy, would enhance the power and prestige of these professionals and might (although this is not certain) increase the amount of research dollars available to them.Is the role of epidemiology, of the CDC, in defining HIV infection coming to an end? Most certainly not. That role, however, may be undergoing a subtle shift—not so dramatic as when the HIV was discovered, but still a change of position to make room for the social scientists. The degree of that displacement will depend on a number of issues, not all in the epidemiologists' control. How will the CDC, for example, incorporate the statisticians and social scientists at NCHS into its HIV data collection projects? Will the CDC benefit from the reluctance of political conservatives to survey Americans in their homes about sex- and drug-related activities? Will the growing insistence by clinicians and some public health officials that all pregnant women, surgical patients, and hospital patients undergo "unblinded" serotesting politicize and undercut all seroprevalence studies? Only time, that most confounding of variables, will tell.
Conclusion
I have outlined how epidemiologists, drawing on the unique perspectives of their profession, reacted to the outbreak of a new disease of unknown origin. By responding early to the epidemic, epidemiologists defined the syndrome first—an act of scientific acumen and power. Over time, however, investigators using other techniques have challenged the primacy of the epidemiologists' construction of the disorder, both of the disease itself and of the hypothetically infected population. To the extent that these challenges were successful, the definition of the disorder has changed, and with it the relative standing of epidemiologists (the CDC in particular). The history of the epidemic demonstrates that the construction of HIV infection was and is a dynamic process in which different scientific specialties negotiated definitions that, to a degree, reflected their relative power.
In the process, the legacy of epidemiologists remains significant. From the beginning of the epidemic, epidemiologists conceptualized HIV infection as a complex social phenomenon, with dimensions that derived from the social relations, behavioral patterns, and past experiences of the population at risk. On the one hand, the epidemiologists' approach may have skewed the choice of models and the hypotheses pursued and may have offered some justification for homophobia. On the other, by defining HIV infection as a multifactorial phenomenon, with both behavioral and microbial determinants, epidemiologists offered the possibility of primary prevention, a traditional epidemiological response to infectious and chronic diseases. Epidemiologists, in effect, established the basis for an effective public health campaign and—through publications, conferences, and the continuous collection of surveillance data—helped make AIDS a concern of policymakers and the public.
Primary prevention—including blood screening, health education, and behavior modification—is currently the only effective social response to the spread of HIV infection. Evidence from several sites indicates that the rate of HIV infection among some groups of homosexual males and IV drug users has begun to decline, possibly because of a reduction in high-risk activities.[114]
Marshall A. Becker and Jill G. Joseph, "AIDS and Behavioral Change to Reduce Risk: A Review," American Journal of Public Health 78 (1988): 394-410; Andrew Moss et al., "Seroconversion for HIV in Intravenous Drug Users in Treatment in San Francisco, 1985-1990," paper presented at the Sixth International Conference on AIDS, San Francisco, 1990.
These results, hopeful signs, have not yet been linked to a decrease in HIV-associated mortality. They may presage, however, a parallel between HIV and past infectious disease experiences.Historical epidemiology has shown that medical interventions, both chemotherapeutic and prophylactic, have had little impact on the overall decline in infectious disease mortality in this century. For example, John and Sonja McKinlay found that since 1900 new medical measures have had almost no detectable effect on U.S. disease-specific mortality rates, because such measures usually occurred some decades after significant declines in death rates had already set in.[115]
John B. McKinlay and Sonja M. McKinlay, "The Questionable Contribution of Medical Measures to the Decline of Mortality in the United States in the Twentieth Century," Milbank Memorial Fund Quarterly 55 (1977): 425.
Thomas McKeown and his colleagues obtained similar results in a study of the mortality trends in England and Wales. According to McKeown, the observed secular decline was mainly attributable to community factors, particularly better nutrition and hygiene.[116]Thomas McKeown et al., "An Interpretation of the Decline of Mortality in England and Wales during the Twentieth Century," Population Studies 29 (1975): 391-422.
It remains to be seen whether HIV-related mortality will also decline as a result of community-directed hygiene (condoms, clean needles, blood screening) before a vaccine or new chemotherapy can be introduced. If it does, the history of HIV infection will offer a powerful vindication of the epidemiologists' multifactorial social definition of disease and of the public health actions that followed from it.The Mass-Mediated Epidemic:
The Politics of AIDS on the Nightly Network News
Timothy E. Cook
David C. Colby
In June 1981 a rare assortment of opportunistic diseases was first noticed among otherwise healthy gay men. Now, ten years later, the epidemic known as acquired immune deficiency syndrome is one of the leading political and social dilemmas facing the United States and the world. Privately experienced illness became not only a public phenomenon but also, as political actors slowly agreed that it demanded public response, a public problem.[1]
On public problems see Joseph R. Gusfield, The Culture of Public Problems: Drinking-Driving and the Symbolic Order (Chicago: University of Chicago Press, 1981), and John W. Kingdon, Agendas, Alternatives and Public Policies (Boston: Little, Brown, 1985). Our perspective has been heavily influenced by the literature on construction of social problems; for an overview see Joseph W. Schneider, "Social Problems Theory: The Constructionist View," Annual Review of Sociology 11 (1985): 209-29.
How did this happen? We nominate one key actor: the news media. If Vietnam was the first "living-room war," with images broadcast directly into American homes, then AIDS may well be the first "living-room epidemic." As early as June 1983, when the first public opinion polls on AIDS were taken, virtually all of those surveyed were aware of it, even though scarcely 3 percent of them actually reported knowing a person with AIDS.[2]These and other data through 1986 are reported in Eleanor Singer, Theresa F. Rogers, and Mary Corcoran, "The Polls—A Report: AIDS," Public Opinion Quarterly 51 (1987): 580-95. See also James W. Dearing, "Setting the Polling Agenda for the Issue of AIDS," Public Opinion Quarterly 53 (1989): 309-29.
After all, the media help to determine which private matters, such as disease, become defined as public events, such as epidemics. Since the reach, scope, and gravity of problems cannot be fully judged in one's immediate environment, the media construct the public reality, a reality distinct from the private world that we inhabit, and provide "resources for discourse in public matters."[3]Harvey Molotch and Marilyn Lester, "News on Purposive Behavior: On the Strategic Use of Routine Events, Accidents and Scandals," American Sociological Review 39 (1974): 101-12, at p. 103.
But the process by which AIDS became an epidemic of public proportions is far from value free. Though journalists may claim to reflect outside reality, news cannot report everything that has occurred in a given day. News is invariably selective. Not all issues and individuals seeking to make news are equally favored in the process of determining
Earlier versions of this essay were presented at the annual meetings of the American Political Science Association, Chicago, September 1987, and the International Communication Association, San Francisco, May 1989. Portions of this essay appeared in the Journal of Health Policy, Politics and Law (16 [1991]) and are reprinted with permission of Duke University. We are indebted to many individuals, whom we will thank personally for advice and suggestions; but particular thanks go to Timothy Murray for his exemplary research assistance and coauthorship of the earliest version; Martha Roark for additional research assistance; Michael Kolakowski for advice and suggestions on poll data; Brenda Laribee for helping to process the charts; Williams College for several Division II grants and the University of Maryland Baltimore County for financial support; the Vanderbilt University Television News Archives for its excellent services; and Edward Brandt, Ellen Hume, Jim Lederman, and Keith Mueller for detailed critiques of earlier drafts.
newsworthiness.[4]
The most important studies of the processes of newsmaking in national media include Edward J. Epstein, News from Nowhere: Television and the News (New York: Random House, 1973); Leon V. Sigal, Reporters and Officials (Lexington, Mass.: Heath, 1973); Gaye Tuchman, Making News (New York: Free Press, 1978); and Herbert J. Gans, Deciding What's News (New York: Vintage, 1979).
Nobody really knows what news is, but journalists still have to produce a certain amount of this highly perishable commodity every day. They must develop ways to "routinize the unexpected," which push them toward recurring news sources, stories, and concerns. But, unlike most news, AIDS was unforeseen and unintentional. It thus provides unusual insight into the processes of negotiation by which events become structured as news.[5]"We take accidents to constitute a crucial resource for the empirical study of event-structuring processes" (Molotch and Lester, "News as Purposive Behavior," p. 103).
The media's identification and definition of public problems work not only on mass audiences but also on policymakers, who are highly attentive to news coverage. They are most likely to respond to highly salient issues, even those that provoke considerable conflict, but largely in the context of the initial frame that the media have provided.[6]
For a fuller discussion of the media's role in elite agenda setting, see Timothy E. Cook, Making Laws and Making News: Media Strategies in the U.S. House of Representatives (Washington, D.C.: Brookings Institution, 1989), chap. 6.
The construction of AIDS as a social and political problem thus has influenced not merely our reaction as individuals but also our response as a society and a polity.Finally, though most attention has separated the scientific study of AIDS from "its metaphors,"[7]
For example, Susan Sontag's influential and thought-provoking books Illness as Metaphor (New York: Farrar, Straus and Giroux, 1978) and AIDS and Its Metaphors (New York: Farrar, Straus and Giroux, 1989) tend to adopt a positivist approach that separates scientific discourse from its literary versions.
the very process of science is affected by the media. Because publicity can influence the allocation of the grants, profits, and prizes that enhance physicians' and scientists' careers, they have incentives to present findings that the media will cover, a situation leading to what has been called "science by press conference."[8]Jay A. Winsten, "Science and the Media: The Boundaries of Truth," Health Affairs 4 (1985): 15. For a fuller account see Sharon M. Friedman, Sharon Dunwoody, and Carol L. Rogers, eds., Scientists and Journalists: Reporting Science as News (New York: Free Press, 1986), and Dorothy Nelkin, Selling Science: How the Press Covers Science and Technology (New York: W. H. Freeman, 1986).
Moreover, since scientific results are fundamentally products of the questions asked, the media's priorities can push medical inquiries in certain directions. Even the answers may be affected by patients' quickness to report those symptoms and behaviors that have been the subject of media coverage.In short, the media may have played (and may continue to play) a critical role in the public perception of the epidemic and the range of possible social and political responses to it. By their ability to transform occurences into news, the media exert power. After all, "one dimension of power can be construed as the ability to have one's account become the perceived reality of others. Put slightly differently, a crucial dimension of power is the ability to create public events."[9]
Harvey Molotch and Marilyn Lester, "Accidental News: The Great Oil Spill as Local Occurrence and National Event," American Journal of Sociology 81 (1975): 235-60 (quoted passage, p. 237).
We suggest that the addition of AIDS to the political agenda was slow because of the way the problem was defined and the epidemic framed. Many observers have suggested that because the group initially most affected included gay men, the media delayed reporting AIDS, consequently postponing and distorting the governmental response.[10]
See for example, Dennis Altman, AIDS in the Mind of America (Garden City, N.Y.: Doubleday, 1986), pp. 16-21.
Although AIDS had entered public awareness by mid-1983, public opinion polls at that time showed relatively little concern that AIDS
would reach epidemic proportions. The issue had been seemingly contained, defined as a distant, not an immediate, threat. Only after the summer of 1985 did a large percentage of the public begin to conceive of the disease as likely to affect their world—and only then was there much pressure on the government to do something about the epidemic.[11]
In addition to the results presented by Singer et al., "The Polls—A Report: AIDS," this conclusion is based on Gallup poll data from the releases of July 7, 1983, and August 18, 1985; Newsweek, August 8, 1983, p. 33; Newsweek, August 12, 1985, p. 23; New York Times, September 12, 1985, p. B11; and the Harris poll released September 19, 1985.
Even then, political response was muted and often confused. AIDS did not become an agreed-upon issue until President Reagan and Vice-President Bush gave their first speeches on the epidemic in 1987, six years after the initial reports.Systematic studies of media coverage of AIDS have been largely limited to print media, such as newspapers and newsmagazines.[12]
The central systematic studies of news content in print media published thus far include Edward Albert, "Illness and Deviance: The Response of the Press to AIDS," and Andrea Baker, "The Portrayal of AIDS in the Media: An Analysis of Articles in the New York Times," both in The Social Dimension of AIDS: Method and Theory, ed. Douglas A. Feldman and Thomas M. Johnson (New York: Praeger, 1986), pp. 163-94; Edward Albert, "Acquired Immune Deficiency Syndrome: The Victim and the Press," Studies in Communications 3 (1986): 135-58; William A. Check, "Beyond the Political Model of Reporting: Nonspecific Symptoms in Media Communication about AIDS," Reviews of Infectious Diseases 9 (1987): 987-1000; and Sandra Panem, The AIDS Bureaucracy (Cambridge, Mass.: Harvard University Press, 1988), chap. 8. On journalists covering the AIDS beat, see James Kinsella, Covering the Plague: AIDS and the American Media (New Brunswick, N.J.: Rutgers University Press, 1989). The only examination to our knowledge of television news coverage of AIDS is Everett M. Rogers, James W. Dearing, and Soonbum Chang, "Media Coverage of the Issue of AIDS," a paper submitted to the Media Studies Project of the Wilson Center, Washington, D.C., 1989, but its primary concern is with the timing of stories rather than the interpretive frameworks provided therein.
Most imply that AIDS was initially ignored because it was regarded as a "gay disease"; but once the possibility of a large-scale epidemic became clear, AIDS evolved into a subject inviting metaphorical and sensationalized treatment. Dennis Altman has conjectured that "from mid-1983 on, AIDS had entered the popular consciousness and was widely discussed. Nor did press attention go away. … Medical stories are particularly attractive to the media, and where they can be linked to both high fatalities and stigmatized sexuality, we have all the ingredients for banner headlines."[13]Altman, AIDS in the Mind of America, p. 19. See also Warren Burkett, News Reporting: Science, Medicine, and High Technology (Ames: Iowa State University Press, 1986), p. 145: "The story of AIDS contained all elements necessary for sensational reporting: sex, threat to health, mystery, and high probability of death."
But print coverage was far from consistent. The volatility of the AIDS story is curious, give Edward Albert's claim that "acquired immune deficiency syndrome seemed tailor-made to the who, what, where and when ideology that often accounts for the content of stories which appear as the 'news.'"[14]Albert, "Acquired Immune Deficiency Syndrome," p. 136.
The opportunities for sensation, drama, and moralizing notwithstanding, AIDS presented numerous dilemmas for journalism as an institution.[15]
Kinsella, in Covering the Plague, presents numerous portraits of individual journalists and shows how their individual perspectives and experiences shaped their approach to the epidemic, but he neglects the impact of standard practices of journalism as a whole. As we shall argue here, the high points and valleys of AIDS coverage was due to more than individual journalists' attributes or failings.
First, the earliest identified group at highest risk comprised gay men. The media would have to deal with individuals who had not attained journalistic standards for newsworthiness prior to 1981. Particularly in television, reporters emphasize issues that are thought to affect the majority of their audiences. With the exception of a few event-driven stories—such as the 1975 discharge of Leonard Matlovich from the Air Force for homosexuality, the 1977 referendum organized by Anita Bryant to repeal the Dade County (Florida) gay rights ordinance, and the 1978 assassination of gay San Francisco County supervisor Harvey Milk—homosexuality and homosexuals had not become a news topic of continuing concern.[16]Ransdall Pierson, "Uptight about Gay News," Columbia Journalism Review, March-April 1982, pp. 25-33; Timothy E. Cook, "Setting the Record Straight: The Construction of Homosexuality on Television News," paper presented to the Inside/Outside conference of the Lesbian and Gay Studies Center at Yale University, New Haven, October 1989.
Reporters on the AIDS newsbeat, whether gay or straight, dealt with a group that mainstream news had neglected.Second, the subject matter of AIDs, mixing as it does references to blood, semen, sexuality, and death, defied traditional notions of "taste."
As Herbert Gans has noted, journalists take the audience into account by considering norms of taste, especially during the dinner hour of the nightly network news.[17]
Gans, Deciding What's News, pp. 242-46. He notes three other considerations for journalists seeking to protect their audience: shock, panic, and copycat behavior.
This audience is viewed as a collection of middle-class families. Av Westin, who has been an executive news producer at ABC and CBS, revealed the networks' logic: "I developed a series of questions to determine what should go into a broadcast and what should be left out. Is my world safe? Are my city and home safe? If my wife, children and loved ones are safe, then what has happened in the past twenty-four hours to shock them, amuse them or make them better off than they were? The audience wants these questions answered quickly and with just enough detail to satisfy an attention span that is being interrupted by clattering dishes, dinner conversation or the fatigue of the end of the working day."[18]Av Westin, Newswatch: How TV Decides the News (New York: Simon and Schuster, 1982), p. 62.
By making such choices, newspersons may inadvertently censor themselves; issues are thereby avoided or euphemized.Finally, and perhaps most important, the media were in the unenviable position of seeking to raise public awareness without creating public panic. While the media take seriously their perceived role of educating and alerting, reporters sense that they must also avoid being inflammatory.[19]
See, for example, David Paletz and Robert Dunn, "Press Coverage of Civil Disorders: A Case Study of Winston-Salem, 1967," Public Opinion Quarterly 33 (1969): 328-45.
The reason is simple. Because they believe that they should reflect politics rather than shape it, they are reluctant to appear to be interfering with the natural unfolding of the political process. Reporters attempt to ignore the consequences of their work lest they be in the paralyzing role of having constantly to predict the future impact of their reporting. They prefer either to avoid topics that could touch off panic or to report such topics in a reassuring way. Indeed, the media periodically examine their coverage of AIDS; and, as we shall see, the network news reports often disclose considerable discomfort as they perform the balancing act between education and instilling "AIDS hysteria."[20]For example, Don Colburn, "Pursuing the Disease of the Moment," Washington Post, February 10, 1987, Health Section, p. 7; Eleanor Randolph, "AIDS Reporters' Challenge: To Educate, Not Panic, the Public," Washington Post, June 5, 1987, p. D1.
We focus here on television news. Television is perhaps, in Tom Brokaw's curious but pungent phrase, "the most mass of the mass media." Although it is commonly reported that citizens receive the bulk of their information from television news, most Americans do not attend systematically to any single medium but, instead, assemble information in haphazard and casual ways. Television news is only one part of the news environment to which individuals react.[21]
Doris A. Graber, Processing the News (New York: Longmans, 1984); John Robinson and Mark Levy, The Main Source: Learning from Television News (Beverly Hills, Calif.: Sage, 1986).
Nonetheless, it is a central part of that environment and has become important in its own right as an agenda setter. Daily newspapers have become more analytic as television takes over the role of headline services for breaking news.And public officials, although they may not often watch the network news for new information, attend to television "to find out what the rest of the nation is finding out."[22]
Michael J. Robinson and Maura Clancey, "King of the Hill," Washington Journalism Review 5, no. 6 (July-August 1983): 49.
Studying television as well as print is also crucial because the two versions often diverge and because audiences learn differently from television accounts than from newspaper stories, as recent studies of information about AIDS have confirmed.[23]
A survey in Washington, D.C., comparing television-reliant and newspaper-reliant citizens, and an experimental study in New England, estimating learning from television, magazine, and newspaper accounts, both point to significantly lower amounts of information about AIDS among television viewers. See Carolyn A. Stroman and Richard Seltzer, "Mass Media Use and Knowledge of AIDS," Journalism Quarterly 66 (1989): 881-87; and W. Russell Neuman, Marion Just, and Ann Crigler, "Knowledge, Opinion, and the News: The Calculus of Political Learning," paper prepared for delivery at the annual meeting of the American Political Science Association, Washington, D.C., September 1988.
In each medium the process of newsmaking is essentially the same: go where news is expected to happen, consult individuals who are agreed-upon authoritative sources, and rework these recorded observations into a coherent account that takes advantage of widely shared cultural scripts and storylines. But the product differs. Television presents different kinds of information. Visual images provide more personalized, vivid, and memorable messages, which may differ from those set forth in print.All newsmaking assembles stories around a particular angle, but newspapers typically conceal this process by the inverted pyramid form, where each succeeding paragraph becomes progressively less essential, so that editors can cut at will. In television, the imperative is to keep the audience tuned in, or at least to ensure that they don't switch channels. Consequently, television news programs are thematic, attempting to flow both between and within stories. Similar subject matters are clustered together, and the half-hour moves gradually from important and serious "hard news" to more contemplative or upbeat feature stories. The reports themselves are miniature narratives, with the anchor's introduction, the correspondent's lead, and a closer that functions as the moral of the story. These stories introduce conflict that is either resolved or left hanging to bring viewers back for more the next day.
As Daniel Hallin has insightfully noted, "Because of their different audiences, then, and because of television's special need for drama, TV and the prestige press perform very different political functions. The prestige press provides information to a politically interested audience; it therefore deals with issues . Television provides not just 'headlines' … nor just entertainment, but ideological guidance and reassurance for the mass public. It therefore deals not so much with issues as with symbols that represent the basic values of the established political culture."[24]
Daniel C. Hallin, The "Uncensored War": The Media and Vietnam (New York: Oxford University Press, 1986), p. 125. Emphasis in original.
Of course, the symbolic presentation favored by television news may serve either to reassure or to mobilize.[25]The best statement on symbolic presentations continues to be Murray Edelman, Politics as Symbolic Action: Mass Arousal and Quiescence (New York: Academic Press, 1971).
Which symbols and which visuals are chosen can have a considerable influence on the public construction of the epidemic.We begin our investigation of AIDS coverage with the nightly news broadcasts by the three major commercial networks. Despite the proliferation of news into the morning and nighttime hours, the nightly news remains the flagships of the three major networks, ABC, CBS, and NBC. Moreover, since 1968 these broadcasts have been videotaped, archived, and indexed by Vanderbilt University's Television News Archive. For our analysis we made a search of all AIDS news stories listed in the archive's abstracts and indexes through December 1989. We then viewed and analyzed all stories from January 1981 through April 1, 1987, when President Reagan made his first major speech about the epidemic.
The Aids "Attention Cycle"
First of all, we should establish a benchmark against which to measure television coverage. In this case there is an easy comparison with empirical measures of the increasing severity of the epidemic. The medical community recognized the first cases in 1981. The number of new cases of AIDS per year, as estimated by the Centers for Disease Control (CDC), rose—at first exponentially and then more gradually (see fig. 1). As for medical attention, a count of articles on AIDS and related subjects in Index Medicus shows similar growth, with a slight drop in 1986, from twenty articles on AIDS in 1981; the medical community sustained regularly increasing interest in the problem (see fig. 2). If the media were merely reflecting either a growing problem or a professional concern, the trajectory of television coverage would follow similar lines as the exponential increase in morbidity rates.
Such was not the case (see fig. 3). There were few stories on AIDS as long as it was identified as a disease that affected only gay men. The CDC had first reported evidence of the disease in June 1981, and the New England Journal of Medicine carried three original articles and an editorial on AIDS in its December 10, 1981, issue. Although major newspapers did report this news,[26]
For example, the New York Times carried stories on July 3, July 5, and August 29; the Chicago Tribune, on July 4; the Washington Post. on August 30 and December 11; the Los Angeles Times, on June 5, July 3, and December 10; and the San Francisco Chronicle, on June 6 and August 29.
there was no nightly news coverage in 1981 and only six stories in 1982. With the exception of the three initial stories about the disease that attacked gay men, the nightly news did not cover AIDS until it spread beyond groups that could be held complicitous in their own illness—gay men and ntravenous drug users.[27]The initial indications of AIDS among heterosexual intravenous drug users appeared in early 1982; the CDC first reported AIDS infections among Haitians in July 1982.
As the risk groups proliferated, the amount of news time devoted to AIDS rose in 1983 but declined in 1984 and early 1985, even as the morbidity rate dramatically rose, until Rock Hudson's trip to Paris to receive an experimental treatment against AIDS. Hudson's illness revitalized
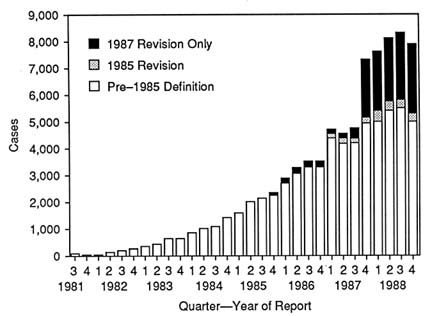
1. AIDS Cases (by quarter of report and case definition)—United States, 1981–1988
SOURCE : Morbidity and Mortality Weekly Report 38, no. 14 (April 14, 1989): 230.
and legitimized the media's interest in ways we shall shortly describe, but again the attention slackened off after Hudson's death in October, only to rise to a new height in 1987 with increasing attention to the possible heterosexual transmission of the human immunodeficiency virus (HIV)[28]
Although the virus was named differently at different times, we choose to call it by the terminology agreed upon in 1987.
and with Reagan's and Bush's first pronouncements on AIDS. Since that peak AIDS has become routinely reported news, with especially heavy concentration on the International AIDS Conferences that have been held generally in June.What accounts for this remarkably variable interest of network news programs in AIDS? In particular, how can we understand that their coverage actually declined at the same time that the severity of the epidemic continued to rise and as medical interest increased? One possibility is provided by Anthony Downs's famous "issue-attention cycle."[29]
Anthony Downs, "Up and Down with Ecology: The Issue-Attention Cycle," Public Interest 28 (1972): 38-50.
In the first stage of the cycle, the condition exists but is not constructed as a social problem; in the second stage an event triggers awareness of the problem and the public's demand that it be solved; in the third stage the public discovers the political and/or economic costs of solving the problem; and, finally, the revelation of these costs forces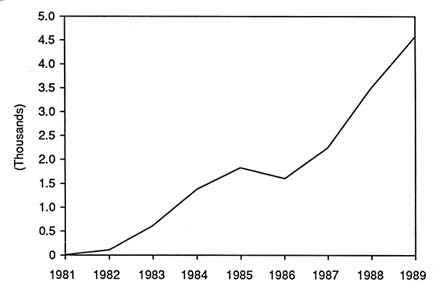
2. Number of Medical Articles on AIDS, 1981–1989
a decline in public interest. But Downs recognized that not all problems are likely to go through a cycle, and there is no evidence that the public beginning in late 1983 saw any costs to doing something about AIDS.
Another possible explanation has to do less with the public than with institutional dynamics of journalism. In particular, while some argue that AIDS was a perfect subject for newspersons, we contend that the epidemic caused newspersons less to sensationalize than to reassure, particularly following their apparent realization that their initial reporting had touched off "an epidemic of fear." News organizations therefore decreased their attention to the disease, which was, in any event, rapidly becoming so familiar that it was "old news." Thus, beginning in late 1983, coverage was sporadic, dictated more by events than by topics. Yet the cycle could begin again if it were refreshed by dramatic new developments that synopsized the reach and extent of the epidemic—and such were the effects of the disclosure of Rock Hudson's illness in July of 1985 and later of the evidence from abroad, particularly Africa, of a heterosexual epidemic.
Phases Of The Cycle
The dynamics of the media's attention to AIDS are further revealed in the themes that characterized the coverage. From 1981 to 1985 the
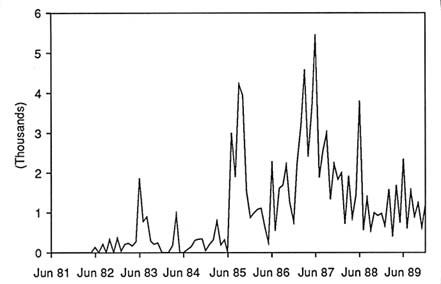
3. Seconds of Nightly News Time on AIDS, June 1981–December 1989
nightly news developed, in sequence, five major clusters of themes on AIDS. The first saw AIDS as largely a gay disease, implicitly blaming gay men and their "life-styles" for the disease. This "mysterious" disease became "deadly" only when it went beyond the initial risk populations, but the media then bypassed openly gay persons with AIDS while pursuing other angles and only eventually legitimized gay spokes-persons as accepted authorities. The spread of AIDS beyond the originally demarcated risk groups was the second theme. The "epidemic of fear" about AIDS provided a third theme. The fourth sought scientific breakthroughs and potential cures that provided hope along with hype—reassurance to calm the fears resulting from the reports of the spread of the disease. The fifth theme, news about the most famous AIDS patient, Rock Hudson, provided a new legitimacy for the issue.
Although these themes do not fall into distinctly separable phases, there is a recognizable time sequence to their initial development. The gay stories appeared at the outset in 1982. They were quickly followed by the stories emphasizing the spread beyond gay men, focusing in particular on hemophiliacs, children, and recipients of blood transfusion.[30]
It is worth noting that until very recently intravenous drug users have been mentioned only in passing as a high-risk group.
In May 1983, following Dr. Anthony Fauci's speculation that HIV might be transmitted by recurring personal contact, the news began to battle the "epidemic of fear," a phase that overlapped with the search on thepart of the media to locate scientific breakthroughs. At this point attention was paid to the isolation of HIV and the development of blood-screening tests, and only occasionally to angles that diverged from the media's stereotype of an illness affecting gay men in New York and San Francisco. Interest declined until the illness of Rock Hudson, which, in effect, certified the newsworthiness of the disease and provided an opportunity for the networks to investigate other aspects of AIDS. And the cycle began anew.
The Mysterious Disease
Scientists at the National Center for Disease Control in Atlanta today released the results of a study that shows that the life-style of some male homosexuals has triggered an epidemic of a rare form of cancer.
NBC, June 17, 1982
Anchor Tom Brokaw's lead-in to Robert Bazell's report in June 1982 introduced a new topic to nightly network news audiences. Both stressed the possibility that gay men's behaviors were directly responsible for the disease. Bazell noted, "Investigators have examined the habits of homosexuals, looking for clues," and then switched to a clip of a gay man, Bobbi Campbell, saying, "I was in the fast lane at one time in terms of the way that I lived my life. And now I'm not." After soliciting a comment from another gay man, Billy Wilder, that the disease itself was worse than dying, Bazell ended on a pessimistic note: "Researchers are now studying blood and other samples from the victims, trying to learn what causes the disease. So far they have had no luck."
A similar angle characterized ABC's first report, on October 18, 1982. George Strait began with a profile of a gay man, Phil Lanzaratta, who had been hospitalized several times in the previous months and who said, "I was walking around like a time bomb." In introducing the report, anchor Max Robinson had referred simply to "a mysterious disease," and the signals that Strait gave on the gravity of the disease were also mixed. After showing graphic photographs of lesions from Kaposi's sarcoma (KS) and emphasizing that it was spreading at "an alarming rate," the worst epidemic since polio in the 1950s, he also noted that Lanzaratta's doctors thought he would likely survive. Most prominent was the link of the epidemic to gay men and then to their sexual practices. Indeed, Lanzaratta's body became a signifier for the
disease; a shot on the left half of the screen of him walking down the street—with close-cropped hair, mustache, tight-fitting jeans, and cowboy boots—was juxtaposed with the words "acquired immune deficiency syndrome" on the right. And after listing the established high-risk groups, Strait returned to the connection between sexuality and disease: "Hotlines in New York and other cities are handling up to fifty calls a day from homosexuals who fear their sexual intimacy may make them especially vulnerable to immune deficiency syndrome." Yet, although his report was more vivid than Bazell's initial report, complete with graphics of the states affected and lists of the diseases that affected individuals contracted, Strait ended with a reassuring touch, noting that medicine and government were both hard at work trying to figure out the syndrome.
The first AIDS story on CBS, by Barry Petersen on August 2, 1982, diverged in many ways from Bazell's and Strait's reports. Unlike its counterparts, CBS did not initially entrust AIDS coverage to its medical or science correspondents and consequently presented a more overtly political report. Petersen paid less attention to the life-style hypotheses circulated by epidemiologists; instead, he was the most critical of the government's slow response and treated the men who had been diagnosed with the disease as tragic figures, fighting nobly against the odds, rather than as pathetic, helpless victims. Starting with a filmed quote from, again, Bobbi Campbell about his "devastation," the report featured gay activist Larry Kramer complaining that Kaposi's sarcoma was unknown because it was a "gay cancer"; it also included sound bites from physicians such as James Curran and Marcus Conant, who noted that spending on KS could also lead to an increased understanding of cancer. The report closed, "For Bobbi Campbell, it is a race against time. How long before he and others who have this disease finally have answers, finally have the hope for a cure?" But even here, Petersen seemed to be less concerned about its initial outbreak than about its spread: "It appeared a year ago in New York's gay community, then in the gay communities of San Francisco and Los Angeles. Now it's been detected in Haitian refugees. No one knows why." He continued to list its presence among hemophiliacs and intravenous drug users, again asking why; but, tellingly, he never asked why KS appeared among gay men. Even the angriest and least judgmental of these three reports did not find the first identification of the epidemic among gay men to be a puzzle.
All three reports—by starting with the experiences of Campbell, Wilder, and Lanzaratta and then broadening out—followed the networks'
tradition of placing disaster in its human-interest context,[31]
Av Westin, in a memo to ABC News correspondents, suggested, "If we are covering a hurricane, begin by concentrating on some wind-swept birds ('the gulls knew Clara was due. They felt the wind early. ...'), then move on to the general panorama of impending disaster." Westin explained his logic as follows: "[A] viewer has to grasp the main points of a story quickly before they are embellished with supporting elements. Starting 'small' and then broadening out helps maintain clarity in the short time usually available" (Newswatch, p. 44).
but they referred to the outbreak simply as "mysterious" and "fascinating." Only later would it turn "deadly." Implicitly, these reports characterized gay men—because of their "habits" or their "sexual intimacy"—as responsible for their illness.These themes were not surprising. Much of the early speculation by scientists came from epidemiology, which studied stereotyped social behaviors thought prevalent among the initially affected group—behaviors such as the use of poppers (the drug amyl nitrite), multiple sexual partners, and the like.[32]
Gerald M. Oppenheimer, "In the Eye of the Storm: The Epidemiological Construction of AIDS," in AIDS: The Burdens of History, ed. Elizabeth Fee and Daniel Fox (Berkeley: University of California Press, 1988), pp. 267-300; Meyrick Horton and Peter Aggleton, "Perverts, Inverts and Experts: The Cultural Production of an AIDS Research Paradigm," in AIDS: Social Representations, Social Practices, ed. Peter Aggleton, Graham Hart, and Peter Davies (New York: Falmer Press, 1989), pp. 74-100.
Defined primarily as a venereal disease, AIDS drew on an old and familiar stigma in American culture.[33]Allan Brandt, No Magic Bullet: A Social History of Venereal Disease in the United States since 1880 (New York: Oxford University Press, 1987). Horton and Aggleton, in "Perverts, Inverts and Experts," note that a blood-borne disease, such as hepatitis B, is actually a more accurate comparison for AIDS than venereal diseases such as syphilis, let alone leprosy and plague.
Even when a gay man with AIDS was interviewed in respectful terms, shot in the close-up "touching distance" favored by human-interest stories that personalize and individualize the subjects, some images stressed the "otherness" of the group. Strait's report showed two men walking to the camera's right shot from above, so that the viewer can see only their legs. As the men pass the camera, it pans up when their faces cannot be seen, while the voiceover tells us, "The only clue to this disease are the types of people caught in this epidemic." The New York location, the shots from above and the back, and the shoulder bag of one man provide a visual shorthand that would be repeated in later reports as a symbol of the anonymous, potentially dangerous urban gay man.But the most striking aspect of this first phase is how short-lived it was. In contrast to the thorough popular-magazine coverage at this time, the initial network reports on AIDS were the only stories to emphasize the "gay plague." In their next stories all three networks concentrated on the spread beyond gay men, "needle-using drug addicts," and Haitians to hemophiliacs, children, and recipients of blood transfusions. Yet the early framing did not disappear. Instead, by stating in each story that the syndrome was first seen among homosexuals—and by often accompanying such a statement with stock footage of gay-pride marches shot from above[34]
For example, ABC, December 10, 1982.
or a gay couple from the back[35]For example, ABC, March 3, 1983.
—the media reinforced the portrayal of AIDS as something emanating from the anonymous gay "other" and striking "innocent victims." And no other persons with AIDS were depicted in such an advanced state of the disease as were gay men. In its grisliest version, an NBC report on April 29, 1983, showed a skeletal man in a hospital bed lamely saying, "Dying at thirty-five isn't so bad. Maybe I'm being given a break," with the voiceover informing us that shortly after this was filmed, the man did indeed die.Many stories blamed the sick in subtle ways. The first story on the AIDS "Haitian connection" (shown on NBC, June 21, 1983) concluded that AIDS cannot be blamed on Haitians but "is transmitted among Haitians just as it is in the United States." The narration tells us that poverty, poor health practices, and prostitution are related to the transmission. But then the reporter takes the viewer via a hidden camera into a Haitian bar that caters to foreign gay men—with the implication that AIDS came to the United States from Haiti via an infected gay man who had sex with a Haitian "boy prostitute." The Haitian connection thus became subsumed under the already existing storyline of gay responsibility for the disease. The tendency to blame gay men was apparent even years later. On May 6, 1985, for example, when NBC reported on a hemophiliac who gave AIDS to his wife and child, the anchor referred to this family's plight as a "tragedy that goes beyond numbers," and noted that these people "live in a mobile home in central Pennsylvania, far from the gay bars in New York and San Francisco." The tragedy of those who live near the gay bars in those cities—for, as this report also noted, three-quarters of all persons diagnosed with AIDS were gay men—was ignored, since their disease was no longer news.
In short, gay men were shown more often as carriers than as victims. Yet at the same time, gay spokespersons were occasionally identified as authoritative sources, if only where they reacted to events initiated by others.[36]
The analysis in this section is based on the following broadcasts: (1) ABC: October 18, 1982; March 2 and June 26, 1983; October 23 and November 23, 1984; March 2, July 28, September 16, October 2, and October 21, 1985. (2) CBS: August 2, 1982; March 23, June 26, and August 6, 1983; April 23 and October 9, 1984; March 2, August 27, September 18, September 19, September 24, October 2, October 15, November 7, and December 12, 1985. (3) NBC: June 17, 1982; June 21, June 26, and October 13, 1983; March 15, August 17, and October 9, 1984; March 2, May 6, July 25, September 18, and October 2, 1985. The first network story that was clearly pegged to a media event by a gay group was CBS's coverage of an ACT UP demonstration on Wall Street on March 24, 1987.
Thus, a March 2, 1983, ABC report on proposals to exclude all gay men from giving blood quoted Virginia Apuzzo of the National Gay Task Force protesting such a move and urging that more attention be paid to research. Gay spokespersons could also be included if they participated in an official event that intersected with already established newsbeats and legitimated the networks' use of their comments. Thus, on August 1, 1983, two networks, ABC and CBS, reported on congressional hearings with numerous gay witnesses; both included Roger Lyon's quote, "I came here today to hope that my epitaph would not read that I died of red tape." In the first several years of coverage, gay men were asked to talk about discrimination; gay health issues; and, to a lesser extent, other gay problems, such as being closeted. By 1985 gay spokespersons were quoted on screen fifteen times in the network news—far less frequently than the ninety-five times that non-gay authoritative sources, such as politicians and doctors, were quoted but more often than the initially negative portrayal would have predicted.[37]Baker, "Portrayal of AIDS in the Media," finds a similar pattern in 1983 in the New York Times. We should be cautious about interpreting these figures too literally, however, since the gay movement may have sought out non-gay individuals (such as Mathilde Krim, researcher from Sloan Kettering Cancer Center) to serve as authoritative sources. The most important conclusion we can derive is that until mid-1985 the gay movement was not a salient aspect of television coverage.
How do we explain this turning to gay sources for comments in the midst of often negative reporting? One clue is provided by earlier television news coverage of homosexuality, which tended to be respectful
as long as the subject matter concerned individual gay men or (much more rarely) individual lesbians. But in the initial stages of the epidemic, when gay men were categorized as a high-risk group , the ambivalence of the media toward homosexuality as a social phenomenon became clear.[38]
See Cook, "Setting the Record Straight," for a further discussion.
Only when the individualistic emphasis could return would the media's assessment be less condemning. Second, because the gay movement was well organized and, once AIDS first hit, its members became convinced that the news media had to be pursued, reporters were provided with willing and easily accessible sources.[39]Altman, in AIDS in the Mind of America, points out that the governmental response to AIDS probably would have been even slower if AIDS had been first identified in less organized groups, such as Haitians or intravenous drug users. Social movements face difficulty in making news, not only because of reporters' doubts about their authority (and hence their newsworthiness) but also because they are often either insufficiently organized to constitute a newsbeat or are ambivalent about the priority of making news. See especially Edie N. Goldenberg, Making the Papers: The Access of Resource-Poor Groups to the Metropolitan Press (Lexington, Mass.: Heath, 1975). Presumably, the professionalization within AIDS activism—what Cindy Patton has termed the move from grass roots to business suits—has contributed to a greater willingness on the media's part to rely on sources within the gay movement. For a good study of this shift, see Donald B. Rosenthal, "Dilemmas in the Institutionalization of AIDS Service Organizations in Upstate New York," paper presented at the annual meeting of the American Political Science Association, San Francisco, August 1990.
These sources, of course, may have unwittingly enabled the media to frame AIDS as a largely gay disease.[40]The media attention may have been a double-edged sword for the gay movement in the early stages; even if negative, it alerted audiences both to the importance of the disease and to the presence of gay organizations. John D'Emilio, in Sexual Politics, Sexual Communities: The Making of a Homosexual Minority in the United States (Chicago: University of Chicago Press, 1983), notes that, paradoxically, even negative reporting in the 1950s and 1960s spurred the development of a gay minority by alerting audiences to the presence of a community they had not known existed before.
But at a later point, once the threat to the innocent was downplayed, gay men moved from being persons responsible for the spread of the illness to "owners" of the problem, legitimate authorities to be interviewed. As Altman has noted, the gay movement may have thereby attained legitimacy, but at a terrible price.[41]Dennis Altman, "Legitimation through Disaster: AIDS and the Gay Movement," in AIDS: The Burdens of History, ed. Fee and Fox, pp. 301-15. On owning a problem, see Gusfield, Culture of Public Problems.
The Threat To The Innocent
An unknown and mysterious disease is spreading. It has killed more people than toxic shock syndrome and legionnaires' disease combined. It first struck homosexual men; but, as Robert Bazell reports, others are getting it.
NBC, October 6, 1982
After the intermittent coverage when gay men and other minorities were deemed the sole persons with AIDS, the media dramatically reported the spread to the "general public."[42]
The analysis in this section is based on the following reports: (1) ABC: December 10, 1982; March 2, July 14, and September 7, 1983; August 16, August 29, September 5, September 11, September 19, October 21, November 13, and November 14, 1985. (2) CBS: December 10, 1982; February 26, March 23, July 26, August 30, and November 9, 1983; April 26, August 2, September 1, November 23, and November 29, 1984; July 29, July 30, July 31, August 27, September 5, September 11, September 18, November 14, December 12, and December 13, 1985. (3) NBC: October 6 and December 10, 1982; March 1, July 14, August 22, August 30, and November 2, 1983; October 9, October 10, November 9, and November 29, 1984; February 27, March 15, April 26, May 6, May 7, July 30, August 15, August 16, August 29, August 30, September 5, September 11, September 19, October 17, November 7, November 8, November 13, November 14, November 21, December 5, and December 8, 1985.
In July 1982 the CDC had noted thirty-four Haitians with opportunistic infections similar to those discovered in gay men, but the networks did not emphasize the spread until the CDC reported AIDS in hemophiliacs and infants. The December 10, 1982, reports of all three networks emphasized the spread of AIDS by blood transfusions, with two noting the CDC's recommendations that those in the high-risk groups not give blood. Two reports fed the fears about the spread. ABC ominously concluded, in an invasion-of-the-body-snatchers tone, that "blood banks cannot know who to look out for if they cannot know what to look out for." CBS suggested that the virus also might be transmitted by saliva, sperm, and mucus in addition to blood. Stories about transmission by blood continued throughout the period under study and were pushed farther forward in the broadcast, even well after the development of the blood test. Otherpotential transmission modes—such as saliva, tears, mucus, urine, dirty needles, and even close contact—were alluded to, though with lesser frequency than blood. These stories, unlike their predecessors, could have proved alarming to viewers. For one, they could easily slip from the conditional "could" to the more inevitable "would." And, among those infected, gays were shown in ways that emphasized their roles as patients or as others, whereas hemophiliacs and children were portrayed as ordinary individuals who happened to be in the wrong place at the wrong time. The gay men interviewed in the first three reports, for instance, were shown alone, either in public places such as parks and cafes or in doctors' offices. In contrast, the hemophiliacs appeared at home surrounded by family members. The reports stressed the fact that hemophiliacs could not adjust their behavior to avoid exposure to AIDS—thereby implying that gay men could adjust their behavior.
Typical in this regard was a CBS story from February 26, 1983. Anchor Bob Schieffer began by noting, "Some doctors suspect that blood banks and plasma centers may be spreading a new and mysterious disease called AIDS." The report dealt with hemophiliacs, which the correspondent, David Dow, labeled a "small but vulnerable part of the population." The networks never reported on gay men in similar terms, though those terms would have been accurate. In the CBS report Dow interviewed one hemophiliac:
DOW :
The unaffected are beginning to worry. … For college professor Charles Bell and many other hemophilia patients, the plasma concentrate they can store at home and inject themselves is not just a lifeline; it is their key to an active, somewhat normal life.
BELL :
I really don't have an option. I really have to continue using the plasma, or the concentrate as it's called. The thought of abandoning the kind of life I have as a result of the concentrate is almost unthinkable. …
DOW :
For now, no one is flatly declaring that the nation's blood supply is in danger. Too little is known about AIDS itself—what it is and how it spreads. But until those questions are answered, other questions will persist among those Americans who depend on the blood of others for their own life and health.
The demarcation between "innocent victims" on one hand and the gay men and IV drug users on the other, which implicitly characterized early AIDS reporting on television, became explicit later on, when virology took over from epidemiology and the stress on behaviors became downplayed. On September 18, 1985, in a revealing passage during the Rock Hudson saga, CBS anchor Dan Rather introduced one sequence:
"It's not at all what people first thought—a mysterious killer that seemed to strike beyond the bounds of respectable society. People thought AIDS was something you caught in alleyways from a dirty needle or picked up in gay haunts doing things most people don't do. But now science knows it is a deadly virus that makes no moral or sexual distinctions. And it's making its way very slowly toward Main Street."
The networks could find little assurance in the statistics about the spread, with the exception of the decreases in syphilis infection rates among gay men.[43]
For example, NBC, June 13, 1983.
At the outset all that reporters could do was to draw some reassurance from their setting—usually a hospital laboratory or, as in George Strait's first report, the Capitol building. Posing in front of the Capitol, Strait closed his report with these words: "In Phoenix and in labs around the country, researchers are trying to solve the mystery around AIDS and the disease it causes. To help, Congress has just appropriated a half a million dollars for more research, reflecting the growing national concern about the spread of this immune deficiency syndrome" (ABC, October 18, 1982). In contrast to Bazell's downbeat presentation in the first report on NBC, later reports sought to depict people hard at work unraveling the mysteries of the mysterious and now "deadly" disease.The "Epidemic Of Fear"
Fighting the fear of AIDS, it seems, is as important as fighting the disease itself. … As researchers attempt to conquer this disease called AIDS, public officials attempt to conquer the epidemic of fear. … It is a delicate balancing act, raising the level of concern for the disease on the one hand, while reducing the level of panic on the other.
ABC, June 20, 1983
Anchor Max Robinson's lead-in and Ken Kashiwahara's voiceover adroitly captured the dilemma for journalists covering AIDS. Already, in noting the spread beyond gay men, they had fallen into a typical approach to a potential disaster, best indicated by a study of how newspapers covered (and how the population responded to) predictions of earthquakes after the discovery of the Palmdale bulge north of Los Angeles. News fell into "an alarm-and-reassurance pattern. … [S]tories began with dramaticized accounts of worst-possible scenarios, as though to shake readers out of their lethargy, and concluded with reassurances
about the seismic resistivity of most local construction … as though to quiet the alarm so deliberately generated."[44]
Ralph H. Turner, Joanne M. Nigg, and Denise Heller Paz, Waiting for Disaster: Earthquake Watch in California (Berkeley: University of California Press, 1986), pp. 58-59.
As these authors note, such a pattern, derived from journalists' attempts to show two sides to an issue, could easily leave audiences confused or able to read in their own (possibly incorrect) conclusion. In television, alarm could easily dominate, even when the final tagline attempted to reassure.For newspapers AIDS became front-page news in May 1983, after Dr. Anthony Fauci's editorial in the Journal of the American Medical Association noting cases of children with AIDS and raising the hypothesis that recurring household contact could be a mode of transmission. The networks did not initially rush to cover this new story. Indeed, only ABC, in a twenty-second throwaway, made any mention of it at all. However, the potential of contamination by casual contact provoked fearful responses, which, in turn, were ambiguously covered by reporters, who partially condemned the "hysteria" but also instilled fears about the potential for a pandemic.[45]
The analysis in this section is based on the following reports: (1) ABC: June 20, 1983; August 2, August 26, September 9, September 13, and September 25, 1985. (2) CBS: May 18, June 19, August 6, and August 11, 1983; March 2, August 9, August 25, August 30, September 9, September 10, September 11, September 12, September 18, September 19, October 3, and November 7, 1985. (3) NBC: May 24, June 20, July 14, September 4, and October 13, 1983; August 26, September 9, and September 12, 1985.
CBS reported the first epidemic-of-fear story on May 18, 1983. Dan Rather introduced the segment, which was placed early in the broadcast to signal its importance,[46]
This story appeared six minutes after the broadcast began; it was the first story after the first commercial break. By contrast, the three original stories appeared after twenty-two (NBC), fifteen (CBS), and fourteen (ABC) minutes.
with an overview of the exponential climb in AIDS cases. He continued: "Those of course are frightening figures, and Barry Petersen tonight reports that in some places fear of the disease is itself becoming epidemic." In the report San Francisco police officers were shown demanding special masks and gloves; health care and sanitation workers were shown, concerned about contamination; and blood banks were shown turning away donors whose "life-style fits that of AIDS victims." Yet, in his closing words, Petersen left open the possibility that such fear was warranted: "Doctors say they do not yet know how far and how fast the disease could spread."Petersen's report on fear of AIDS was perhaps the most alarming. Later reports, starting with NBC's May 24 story, explicitly attempted to calm these fears. In mid-June all three networks aired lengthy stories about "AIDS hysteria" within a day of each other. The news had piqued interest in the spread of the disease, which had gone from being "mysterious" to being "deadly." Now the attention shifted from the threat to would-be innocent bystanders caught by circumstance to social institutions. Most prominent among these institutions were, of course, blood banks and hospitals; but prisons, the military, and schools were all shown as undergoing considerable anxiety, with the possibility of infected or exposed inmates, soldiers, or schoolchildren. Such locales often provided, whether advertently or not, an opportunity to spread
misinformation as frightened individuals made emotional statements.
Take CBS's prison story from June 19, 1983. Anchor Morton Dean introduced the lengthy story by quoting Edward Brandt, assistant secretary of the Department of Health and Human Services, to calm concerns with factual information about the only known modes of transmission. But the report had other effects. Reporter Joan Snyder said that AIDS was probably not spreading rapidly in prison: "But what has spread rapidly is fear." She illustrated this statement by showing an emotional correctional officer shot in dramatic close range and yelling, "Get these people out of the jails! It's gonna cost people's lives one way or another. Either we're going to die of AIDS or these people are going to kill us or something. Get 'em out of the jails! That's the answer." Snyder could not counteract this vivid quote with a bland statement from what she termed "a correctional officer at a meeting called by state prison officials to try to relieve anxiety among prison workers with medical information." Her indication of no evidence for transmission by casual contact was again counterbalanced by inmate liaison Pedro Soto arguing, "Once you have AIDS, you're gonna die. … There is no way that they can tell you how to catch AIDS. They have ideas. They're checking 'em out. But they cannot say," followed by an inmate endorsing the idea of quarantine.
These stories often showed persons-in-the-street commenting in ways that defied scientific understanding, even at that time, of how the disease would spread, or expressing doubts that one could be absolutely sure. Reporters, hewing to the strategic ritual of objectivity, never specifically rebutted these misleading statements, apparently considering it sufficient to mix alarm with reassurance from public officials.[47]
Kashiwahara's June 20, 1983, story on ABC, for example, followed images of discrimination with the statement "Politicians and health officials have declared war on AIDS hysteria," with sound bites by New York mayor Edward Koch, CDC scientist James Curran, and Health and Human Services secretary Margaret Heckler.
The report could then inadvertently reinforce and authenticate the viewers' doubts.Ironically, although journalists sided with those who were trying to calm the fear, their reports about it may have served not to exorcise but to heighten it. The emotionally charged quotes from upset individuals would in all likelihood have overriden the cool statistics proffered by the authorities. Other vivid film excerpts portrayed reactions that may have (incorrectly) seemed legitimate: police officers donning surgical gloves and masks, prison guards putting on futuristic "special protective outfits should they have to subdue a prisoner with AIDS," and television technicians refusing to fit a microphone on a person with AIDS.[48]
See ABC, June 20, 1983; CBS, June 19, 1983; NBC, June 20, 1983.
In later stories the news would recount the various impacts of fear:
discrimination against AIDS patients; discrimination and violence against gay men; shortage of blood supplies after incorrect rumors that people could contract AIDS by donating blood; anxiety among health care workers, police, and prison guards; refusals to adopt AIDS children; and, most frequently of all, the attempts to keep children with AIDS out of public schools. Only a few stories presented segments showing cool, deliberate reactions from the public: the townspeople who allowed a child with AIDS to attend school without protests; the young playmates of an HIV-positive child.[49]
ABC, September 13, 1985; CBS, January 22, 1986.
Vividness alone does not explain this preference. Witness a moving NBC story of a teacher with AIDS who had been transferred out of his classroom for the hearing-impaired and who won a suit that returned him there; his press conference in the school library was interrupted by several beaming students who embraced him (November 23, 1987). But such a story evaded the usual priority of television media for setting forth an easily reported either-or conflict, preferably in continuing sagas, such as those of schoolchildren struggling to stay in school: Ryan White in Kokomo, Indiana, in 1985; or the Ray brothers in Arcadia, Florida, in 1987. In search of the balance between being informative and being interesting, network news tended to offset the bland reassurances of government health officials with the dramatic emotions of those who feared the worst. The epidemic of fear was far from stemmed.Faced with an impossible balancing act, the news media seem to have decided to turn their attention elsewhere. As long as a story had to involve two distinct sides that often talked past each other and were rarely directly rebutted by reporters, calling attention to the potential gravity of AIDS provoked fearful responses, whose coverage simply made matters worse. The epidemic had not played itself out, but the topic as a news story had, and journalists would now await authoritive scientific and political sources to let them know when news on AIDS would happen.
The Search For The Breakthrough
There may be a dramatic breakthrough in the treatment of AIDS tonight. Maybe. Everybody is anxious for some encouraging news.
NBC, October 29, 1985
Tom Brokaw, in his lead to a story about the promising effects of Cyclosporin A, typifies reports on scientific research and treatments for
AIDS. After emphasizing the spread of this disease to "innocent" victims and the consequent fearful reaction, the networks proceeded, beginning in 1983, to express cautious hope, reassuring the audience that scientists were inexorably progressing toward a treatment, cure, or vaccine.[50]
The following broadcasts are examined in this section: (1) ABC: July 12, August 1, and October 26, 1983; April 4 and April 23, 1984; January 10, January 11, March 2, and July 26, 1985. (2) NBC: January 14, April 29, July 8, and July 12, 1983; March 15, August 17, and December 14, 1984; January 17, February 8, March 2, July 24, July 26, October 29, and November 11, 1985. (3) CBS: July 12, 1983; March 1, April 4, April 19, April 20, and April 23, 1984; January 5, January 10, February 20, March 1, March 2, May 5, May 6, May 10, July 25, September 4, September 12, September 18, November 14, and December 13, 1985.
As with newsmagazines, the focus of coverage shifted from a preoccupation with life-style and contagion to reports on science and medicine.[51]Albert, in "Acquired Immune Deficiency Syndrome: The Victim and the Press," notes that life-style/contagion stories in newsmagazines peaked in May-July 1983 and fell behind science/medicine stories in May-July 1984.
Such attempts to reassure had been evident in news reporting since Strait's October 1982 ABC story, but the search for a breakthrough began in earnest in mid-1983. For example, on April 29, 1983, NBC reported that the isolation of a virus was the "best lead yet" and, three months later (on July 12, 1983), that research on Interleukin-2 provided "encouraging news tonight—not enough to call it a breakthrough, but encouraging news nonetheless."This phase differed from the preceding ones. Coverage was no longer topic-driven, whereby enterprising reporters dug up new aspects of a continuing story. Instead, it was event-driven; that is, reporters routinely awaited event summaries or pseudo-events, such as news conferences or demonstrations, to discuss the otherwise less than newsworthy subject.[52]
For discussion of these issues, see G. Ray Funkhouser, "The Issues of the Sixties: An Exploratory Study of the Dynamics of Public Opinion," Public Opinion Quarterly 37 (1973): 62-75. This split is similar to the contrast between enterprise and routine journalism provided by Sigal, in Reporters and Officials.
Reporters consequently became even more dependent on authoritative sources, such as political officials, prestigious doctors, or drug companies' spokespersons, to create such events and allow an opportunity to cover the issue. In the absence of new developments announced by these sources, the only news about AIDS that would develop were occasional odd angles, such as the death of a great-grandmother from AIDS (NBC, February 27, 1985).Such authoritative sources also had reason to look for a breakthrough and to provide reassurance. At the very least, governmental officials and scientists were more likely to call a press conference when progress and promising news would occur.[53]
A recent example occurred in 1989, when HHS secretary Louis Sullivan appeared before the news media to announce the government's finding that the drug AZT worked to slow the reproduction of HIV among infected asymptomatic individuals. According to Sullivan's spokesman, had the news not been so upbeat, his boss would likely not have appeared (Robert Schmermund, comments in panel "NIH Announces AZT," at the Harvard School of Public Health, April 1990).
Moreover, the Reagan administration was eager to limit the damage near an election year. Thus, in a July 12, 1983, story on Interleukin-2, NBC quoted Health and Human Services secretary Margaret Heckler: "It's the first glimmer of light. It's not the whole answer, but it is promising." The most notable example of the media's being misled was Heckler's prediction that, with the isolation of the virus, a vaccine was only a few years away. The reporters added some caution, but the optimism of the authoritative source dominated the reports. Meanwhile, scientists downplayed dead ends and stressed advances—findings that the news media would cover and that would boost the scientists' credibility and their careers. Given the interest on the part of both political officials and scientists to callattention only to progress, if not breakthroughs, much reporting on AIDS went from alarming to soothing.
To be sure, many reports on cures were often interwoven with stark data on the spread of the disease. In an August 17, 1984, report on the isolation of the virus by San Francisco scientists, NBC introduced the story with the following statement: "No one knows for sure what causes AIDS. But what both scientists and researchers know is that it attacks homosexuals mostly and that invariably it kills. Tonight Robert Bazell tells of one more step in the search for clues to the disease and a new and sinister element in the AIDS equation." As with many of the stories, NBC first alarmed and then assured the audience—by raising anxieties that can be resolved. Thus, the media created a "strong" science story that reaches the "boundaries of truth."[54]
Winsten, "Science and the Media", pp. 11, 9.
Sometimes they offered only faint hope, but virtually no reports were as downbeat as Bazell's original story in 1982. On March 1, 1984, in one of its several reports on simian AIDS, CBS interviewed a researcher who described his findings as follows: "There is no immediate significance, in terms of therapy. However, there is great significance in terms of hope." Most stories carried caveats, such as "Officials warn against premature expectations of a quick cure"; "Scientists caution that even when they are certain of the cause of AIDS, it will probably take years of more research before they develop a vaccine"; and "The next step: a vaccine. But that's a big step, and researchers say that it could take years."[55]
Respectively, NBC, July 12, 1983; NBC, March 15, 1984; CBS, April 20, 1984.
This tendency from mid-1983 until mid-1985 is important because dead ends in research were not considered newsworthy by any of the actors involved in making news—neither the sources (whether politicians or physicians) nor the journalists—even though gay spokespersons were then vocal in their denunciation of government inaction. And even more than most sources, the networks stretched to the boundary of truth, looking for a breakthrough that would reassure. Reports on tongue sores, a plant fungus, feline AIDS, and experimental drug treatments provide examples.
This attempt to be the first to report a breakthrough is, of course, common to many science stories, as the flap over "cold fusion" in 1989 clearly illustrates. But not only does this penchant exaggerate preliminary or mixed results; it also leads to omissions, so that certain stories (or parts of stories) are not covered.[56]
In the story of Baby Jane Doe, an infant with multiple birth defects, the major distortion, according to Klaidman and Beauchamp, was not inaccuracies but incomplete reporting. See Stephen Klaidman and Tom L. Beauchamp, "Baby Jane Doe in the Media," Journal of Health Politics, Policy and Law 11 (1986): 271-84.
Breakthroughs are key, because if events are not perceived to move the process along, then by definition news did not occur.[57]Mark Fishman, in Manufacturing the News (Austin: University of Texas Press, 1980), has suggested that reporters at a governmental newsbeat decide what to cover by referring to a "phase structure," or an idealized version of how that institution's process unfolds; newsworthy points occur when the process moves from one phase to the next. The same may be true of science correspondents, but here the idealized process may well be science marching on.
We have already noted that television failed toreport the AIDS story until more than a year after the disease was first noted. And when it did cover the AIDS story, it overlooked a number of significant events: the development of a clinical case definition of AIDS in September 1982; the voluntary guidelines developed by the American Red Cross and others advising against accepting blood from high-risk groups in January 1983;[58]
NBC briefly mentioned this, but ABC and CBS did not.
the discovery in May 1983 by scientists from Harvard, the Pasteur Institute, and NIH that HIV infected at least some AIDS patients; Interleukin-2 clinical testing that began in March 1984; the First International Conference on AIDS in Atlanta in April 1985; and the May 1985 NIH study showing that health care workers have a low risk of contracting HIV.The event-driven storyline not only tended to discourage access of gay spokespersons to the media, who could not point out the lack of progress that they perceived; it also meant that the story of how the gay community was responding to the crisis went almost unreported. From mid-1983 to mid-1985, most events concerning AIDS were not included in the news, and larger assessments of the epidemic and the responses to it were all but nonexistent. In this event-driven phase of routine journalism, the news media may have continued intermittently to sound the alarm, but the alarm was now at least equally balanced by reassurance. Consequently, AIDS stories not only declined in number but also became less urgent and tended to imply that the situation, however grave, was largely under control.
Rock Hudson And The Legitimation Of Aids
Hudson's condition has brought AIDS back into the headlines, but after all it is an ongoing emergency.
NBC, July 24, 1985
The illness and death of a famous actor with a masculine image, "the most well-known victim yet" (CBS, July 25, 1985), legitimized the media's attention to this disease as a continuing story instead of sporadic breaking news. Indeed, it would not be too far-fetched to describe AIDS coverage in television as falling into two phases: before and after Rock Hudson. Some of this new attention can be attributed to Rock Hudson's status as a celebrity. But the replayed visuals of his scenes with Doris Day, Elizabeth Taylor, or Linda Evans tended to reinforce Hudson's powerful image as the epitome of heterosexuality—an image that
the networks, presumably concerned about privacy, did not contest, since they kept largely silent about Hudson's sexual preferences in real life. Little wonder that the new image of AIDS was that it was at last hitting home.
Yet what is most striking about this phase of reporting is the new legitimacy accorded to topic-driven stories about AIDS and to sources, notably in the gay movement, that had been absent in the preceding several months. This new concentration also provoked agencies, such as the National Institutes of Health, to be more proactive than reactive.[59]
According to Ann Thomas, director of public information at NIH, "After Rock Hudson, instead of responding to reporters, we were so nicked by the criticism why weren't we doing more that we decided to give more backgrounders and sent out more press releases." At this point Fauci was designated as the principal source for reporters (Thomas, comments on panel "NIH Announces AZT," Harvard School of Public Health, April 1990).
Not only did the new legitimacy allow the networks to develop longer stories and special segments on AIDS; it also pushed AIDS stories earlier in the broadcast, thus according them more importance, and allowed the "old news" story of gay men with the disease to reappear.The initial reports, on July 23, 1985, described Hudson's hospitalization in Paris and reported speculation of his having AIDS. On the second day of this story, two networks, in rare lead stories, not only confirmed reports that he had AIDS but also used the opportunity to report broader aspects of the AIDS story.[60]
CBS, July 24, 1985; NBC, July 24, 1985.
CBS developed the story of experimental drugs, using, as the rationale, Hudson's attempt to be treated in Paris with HPA-23. NBC further broadened the story by presenting an extensive report on the stress experienced by health care workers and AIDS patients in the clinic at San Francisco General Hospital. For the first time in months, instead of reporting primarily on hemophiliacs or other people with AIDS from atypical locales or groups, the networks showed gay people with AIDS—and treated them with respect. On July 25 all three networks led with the news confirming Hudson's diagnosis of AIDS and also examined other aspects of the AIDS story: ABC reported on the development of experimental treatments; this report was followed by a lengthy question-and-answer session between anchor Peter Jennings and medical editor Timothy Johnson on the transmission of AIDS. CBS reported on the development of experimental treatments. NBC reported on fund-raising efforts in Hollywood, and Tom Brokaw interviewed Dr. Paul Volberding, the AIDS clinic director at San Francisco General Hospital, on AIDS transmission. On July 26, after perfunctory reports on Hudson's condition, ABC described the AIDS clinic at San Francisco General Hospital, and NBC recounted the development of experimental drugs. Then, on July 28, ABC described fund-raising efforts such as a ten-kilometer walkathon in Hollywood. In late September ABC presented a week-long series of reports on theorigins, extent, transmission, cures, and treatments of AIDS and, even more unexpectedly, on AIDS-related complex (ARC), which had been previously unmentioned by the networks.[61]
September 23, 24, 25, 26, and 27, 1985.
Even on the day of Rock Hudson's death, October 2, NBC recapitulated general information about AIDS.To be sure, in many ways coverage merely revived a wealth of familiar storylines. CBS's Dan Rather resuscitated "an epidemic of fear that seems to be spreading faster than the disease."[62]
September 9, 1985.
The principal stories were related to schoolchildren with AIDS: an unidentified second-grader in Queens and, what was better for the news, the ongoing saga of Ryan White.[63]The first Ryan White story appeared on CBS on July 31, followed by ABC on August 2 and NBC on August 16. All three covered the first day of school in Kokomo on August 26.
But coverage of fear also included people with AIDS who were barred from nursing homes; unwanted and thus unadoptable foster children of AIDS-afflicted mothers; and even extraordinary precautions at the Rajneeshpuram community in Oregon.[64]Respectively, ABC, August 2, 1985; CBS, August 2, 1985; ABC, September 5, 1985.
But the epidemic-of-fear story now concentrated less on frightened heterosexuals, particularly parents pulling their children out of school, than on gay men who were subjected to discrimination and violence. Thus, in one report CBS not only showed conventional incidents of fear—Houston police wearing rubber gloves when frisking gay suspects, a school board meeting in New Jersey—but also interviewed a man with AIDS who was suing to regain his job as a budget analyst in Florida.[65]
October 7, 1985.
In an NBC story gay men in Colorado expressed their concern about losing insurance coverage after a law was passed requiring blood banks and doctors to report HIV-positive individuals by name; and a CBS story reported discrimination against gay actors in Hollywood in the wake of Hudson's illness.[66]NBC, September 18, 1985; CBS, September 19, 1985.
ABC broadcast a "special segment" on violence against gay men and lesbians, with Jennings noting, "There's always been prejudice and violence against homosexuals and lesbians [sic] . But the public concern about AIDS and its connection to homosexuals has made it a more serious problem."[67]October 21, 1985.
The illness of Rock Hudson recertified AIDS as a newsworthy topic suitable for stories beyond breaking news. The authoritative sources that had dominated the coverage of AIDS prior to the revelation of Hudson's illness no longer held the upper hand, and the reappearance of AIDS as a newsworthy issue allowed gay spokespersons to add their perspective. But instead of maintaining a continuing high attention, the networks' interest again would decline in late 1985 and early 1986. In effect, the cycle may have begun again. After Hudson's death AIDS became old news, and reporters relapsed to an event-driven mode. Although
Hudson's illness ushered in a new phase of AIDS reporting, notable for its thoroughness and for its new sympathy to both gay persons with AIDS and gay-movement spokespersons, it did not last.
The Cycle Again, But With A Difference
Hope and despair. Those are the conflicting emotions evoked by two stories tonight.
CBS, September 18, 1986
Anchor Dan Rather's lead-in to two stories, one about the drug AZT and the other about the epidemic in Africa, shows how the AIDS attention cycle replayed itself with a difference. Already, in the fall of 1985, there had been a spate of epidemic-of-fear stories, but by the beginning of 1986, the topic-driven coverage provoked by Rock Hudson's illness had once again been replaced by a largely event-driven routine approach. And once again, news organizations relied on political officials and authoritative medical and scientific sources to indicate when an AIDS story was newsworthy.
But five linked characteristics distinguished the post-Hudson coverage. First, although the number of stories declined from the 1985 level, they were presented earlier in the news flow, and items were placed among the top stories—a status that had rarely occurred prior to the revelations about Rock Hudson.[68]
Indeed, during 1986, when the number of stories dipped, AIDS was the top story on NBC on June 12 (announcing federal forecasts of 170,000 cases). It was also the top story on ABC on June 23 (reporting the Justice Department's announcement that laws barring discrimination against the handicapped did not extend to HIV-positive individuals—this announcement occurring on the same day that the international AIDS conference was held in Paris). Finally, AIDS was the top story on ABC and NBC on October 29 (quoting a National Academy of Sciences report, which charged that the response to AIDS was "woefully inadequate").
More telling, the networks' complete neglect of AIDS as recently as the month before Hudson flew to Paris would never be repeated. Second, as AIDS became more generally recognized as newsworthy, more approaches were brought to bear; thus, stories in 1986 were covered not only by medical and science correspondents but increasingly by law reporters, political reporters (both foreign and domestic), and regional stringers who sought new angles and spoke to new sources. Third, there was thus less consensus about how best to cover the epidemic. The medicalization of the epidemic was no longer complete. The networks' confusion is best revealed by the contrasting logos placed behind the anchor announcing the story—ABC using two overlapping faces of uncertain gender in 1986 and, beginning in March 1987, the word AIDS against two crumbling male and female symbols; CBS using the medical symbol to replace the "I" in AIDS; and NBC varying the graphic for medical stories (e.g., a hand holding a test tube of blood) or for items emphasizing social ramifications (e.g., a man and a woman silhouetted against the letters AIDS). Fourth, this lack ofconsensus meant that a variety of storylines would be revived—the continuing preoccupation with the safety of the blood supply, or the Rock Hudson angle applied to other famous people with AIDS, such as pro football star Jerry Smith—and would continue to reinvigorate the media's attention to the epidemic on a variety of dimensions.[69]
Rogers, Dearing, and Chang, in "Media Coverage of the Issue of AIDS," identify thirteen "sub-issues" of AIDS, whose individual ebb and flow actually allowed the epidemic to continue to be in the news on a regular basis.
Fifth and most important, the increased prominence of AIDS and the new variety of approaches allowed more authoritative sources to be heard. And now these sources were in disagreement, whereas from late 1983 to mid-1985 they had converged on a storyline that reassuringly noted science doggedly at work to master the epidemic. Although the First International AIDS Conference in Atlanta in 1985 went unnoticed by the networks, its 1986 counterpart in Paris became the first of periodically recurring events that attracted enormous coverage.As the number of cases in Europe and Africa grew, sources outside the United States—at an international conference on AIDS in Africa held in Brussels in November 1985, at the Paris conference in June 1986, and later at the World Health Organization—began providing information. Significantly, these sources, drawing from African data, were more likely than their American counterparts to raise the possibility of an epidemic among heterosexuals. As AIDS gained attention, scientists and physicians who were not directly involved in research or treatment spoke out. These sources, instead of talking primarily about progress and breakthroughs, pointed to the rising number of cases and to what became a lead story on both ABC and NBC—the National Academy of Sciences report of a "woefully inadequate" response. Within the Reagan administration, too, there was disagreement; in addition to confusion in the Justice Department over the reach of antidiscrimination laws to people with AIDS and HIV-positive individuals, the outwardly united front was publicly broken by Surgeon General C. Everett Koop, who tersely called for massive education of adults and children with the words "We're talking about death because of our reticence. … This silence must end" (ABC, October 22, 1986).
Early in 1986 the networks were still trying to maintain a balance between alarm and reassurance. In February, for example, Dan Rather announced new evidence about "how the AIDS virus works with terrifying speed," and science reporter Susan Spencer used this evidence to add a more upbeat closer: "A major development in basic science does not mean that a cure for AIDS is around the corner. But the virus has given up another secret and scientists have a new weapon in the fight against it" (CBS, February 12, 1986).
But as the sources expanded, even the most reassuring of journalists, such as ABC's George Strait, changed tone. Strait was the first to report about the potential for the drug AZT as an area where "great progress is being made," with footage of AIDS patient John Solomon in what Strait termed "the midst of a remarkable recovery."[70]
ABC, March 13, 1986. Strait was then still searching for the breakthrough, as an interview with Samuel Broder revealed. Strait, with urgency in his voice, asked Dr. Broder, "Is this a breakthrough?" and Broder cautiously responded, "It's not a breakthrough, but it's a dent."
But, along with his colleagues, he too would note "the latest disturbing news about the spread of the disease" from the Paris conference in June.[71]ABC, June 23, 1986. On CBS Dan Rather noted, "Just how shocking and widespread is the disease is the subject of Susan Spencer's report" (June 25, 1986); on NBC anchor Chris Wallace pointed to "the alarming spread announced in Paris" (June 22, 1986).
By the spring of 1987, when governmental sources began suggesting testing for those in high-risk categories (including recipients of blood transfusions), Strait showed clinics with heterosexuals seeking to be tested. Then, segueing from a shot of a New York street scene to one of a man and a woman in a rural field, walking and nuzzling, he added, "For most people, the likelihood is low, but even small-town America is not completely safe." The woman in this story had AIDS. After running a quote from her, in which she wondered how many people might be infected without being aware of it, the report froze the frame, and Strait noted, "Last January, two years after these pictures were taken, Amy Sloan died" (ABC, March 19, 1987).Even with the September 1986 announcement of the dramatic results of AZT, the first effective treatment against AIDS, and with the lead stories allocated to the Food and Drug Administration's approval of AZT in March 1987, the networks balanced only muted reassurance with alarm, either noting the toxicity and uncertain duration of AZT's effect or pointing to areas where AIDS was seemingly out of control. Similar storylines emerged once more. Blaming the victims occurred in curious ways. An otherwise bland ABC report on anonymous tests by the CDC to gauge the spread of HIV shifted its visuals from CDC head-quarters to a back shot of two jeans-clad men holding hands when Mike von Fremd intoned his close: "Those testing positive cannot and will not be told" (January 10,1987).
But the stories now used less file footage of the Castro district and more of New York telephoto street scenes or of heterosexual couples shot from behind as they walked down the streets. Some of the reports emanated from bars frequented by single heterosexuals, who now responded with the same caution about multiple partners that the networks had elicited from gay men in 1983.[72]
For example, ABC, March 11, 1987.
The epidemic-of-fear stories—noting again that "the AIDS virus is spreading rapidly, but even more contagious are the fears of the worried well" (NBC, March 17, 1987)—began to fuel not just reaction against high-risk groups and people with AIDS but also a seemingly growing concern from that general populationitself that it, too, might be infected. The epidemic, as far as the nightly news was concerned, had been heterosexualized.
The increased diversity of newsbeats, journalists, and sources brought to bear on the AIDS epidemic after Rock Hudson's death was responsible for the upward spiral of stories that peaked in the spring of 1987. When President Reagan finally delivered a major address on AIDS on April 1, 1987, before the College of Physicians in Philadelphia, he briefly halted this climb, since there was a hiatus of several days on each network before they reported another AIDS story. But in the process the president also guaranteed that all authoritative sources now agreed about the place of the epidemic on the political agenda.
Conclusion
We cannot agree that "media response to AIDS has generally been irrational."[73]
Albert, "Acquired Immune Deficiency Syndrome: The Victim and the Press," p. 155.
The ebb and flow of AIDS reporting reflects considerable rationality, but by the standards of "media logic ." After all, journalists used authoritative sources, presented ostensibly balanced reports (which, as we have seen, may not have been so evenly balanced as the reporters thought), moved away from stories seen as repetitive "old news," and sought to avoid subjects that present too many complexities for the audience. Each of these strategies represents a journalist's rational adaptation to the uncertainty and vulnerability of trying to figure out what's news. Merely arguing that the media should be more objective or more rational overlooks the possibility that objectivity and rationality led us to the inadequate picture of AIDS that television presented.Our evidence supports the conclusion that the media did not merely reflect outside events but, instead, profoundly recast the epidemic for both public and governmental audiences. The media played a crucial role in agenda setting on AIDS, particularly at the time of problem definition. First, the lag time between the first identification of the syndrome and the earliest television reports may have caused or allowed delay on the part of government officials, who could overlook the gravity of the epidemic. More important, the evidence from television network news suggests that—in contrast to the expectation that coverage of AIDS would tend to be sensational—the networks attempted to reassure at least as much as they played up the story. After they discovered the "epidemic of fear" set off by reports of AIDS in mid-1983, the networks quickly searched for a breakthrough, particularly in progress toward the development of a vaccine, and turned away from AIDS stories
unless government officials and high-ranking doctors presented them with breaking news, which itself was likely to be taken as an indication of progress against the disease. In short, the media did not maintain consistent pressure after AIDS was brought to public attention in the summer of 1983. The access of the gay movement was highly conditional and was low during the period before Rock Hudson's illness became known. When the media did cover the issue, they defined the problem not as the lack of a cure for those already afflicted but as the lack of a vaccine that would control the spread to the "general population." Overall, media coverage was more inclined to reassure than to criticize.
The initial coverage, with its emphasis on gay life-styles and "innocent victims," made AIDS a much more controversial matter than it would have been if the initial coverage had addressed purely medical problems. As Barbara Nelson has noted, only when child abuse was packaged as a medical question rather than a moral question did government action proceed.[74]
Barbara J. Nelson, Making an Issue of Child Abuse: Political Agenda Setting for Social Problems (Chicago: University of Chicago Press, 1984).
A similar conclusion could emerge from the evidence on AIDS.Even here, television did not do a stellar job, partially because of its squeamishness not only about disease but about sexuality in general and homosexuality in particular.
But AIDS reporting was primarily shaped by a routine that was, on its face, neutral. The epidemic hit first and hardest a stigmatized group that the media considered to be distinct from their audience at large. As long as AIDS was defined as a disease that largely affected gay men—who were depicted as anonymous, often foreboding, carriers of the illness—media attention was marginal. As NBC's Robert Bazell admitted in February 1983, "It would be dishonest not to say we couldn't sell the AIDS story early on because it was about gays."[75]
Quoted in Altman, AIDS in the Mind of America, p. 16.
Moreover, the access of gay-movement spokespersons to television news was lower than that of scientific or political authorities, whose "event needs" favored reassurance about the progress to a breakthrough. Television news, if it were to find a way to cover AIDS, had to sell the story to the general public—hence the early focus on hemophiliacs and children—in ways that enlightened without panicking and that violated none of the taste taboos prominent in television. This was, as it turns out, an almost impossible task; little wonder that after each of the upswings in 1983, 1985, and 1987, the networks receded from covering it.In 1985 television would eventually accord AIDS the ultimate status of a social problem—a made-for-TV movie, NBC's acclaimed An Early
Frost . As with network news, the producers faced considerable difficulty in selling the story to the network's broadcast standards department. One source pointed out, "The NBC censor said to the producer, 'I thought we were doing a film about AIDS, not about homosexuality.' And the producer said to him, 'What planet have you been living on?' If this were a heterosexual AIDS movie, there would have been no problems at all."[76]
Stephen Farber, "A Drama of Family Loyalty, Acceptance and AIDS," New York Times, August 19, 1985, p. 23.
This temptation to make a movie about AIDS without making a movie about homosexuality is much the same as the temptation to ignore AIDS as legitimate news when it appeared to affect only homosexuals. The consequences to us seem far-reaching indeed.Postscript: The Hiv Epidemic And The Networks In The 1990s
By mid-1987 President Reagan and Vice-President Bush broke their silence on the epidemic, and AIDS entered the political agenda not as a sporadically recurring problem but as a permanent matter, to which politicians would be expected to respond. Indeed, the cycles of television coverage that followed after the three peaks—in June 1983, with the first concentration on the epidemic reaching beyond the four risk groups then classified; in September 1985, with a gay actor's illness symbolizing, paradoxically, the long reach of AIDS; and in the spring of 1987, with the warnings about a heterosexually transmitted epidemic—may well have played themselves out in the absence of new evidence of a more rapid or widespread expansion of the epidemic that challenges the current understanding. AIDS has become a routinely reported matter, no longer subject to fluctuations inherent in crisis reporting.
As with prior periods following the peaks, reporting since mid-1987 has slackened off.[77]
A search of the Nexis data base showed that the number of stories was halved between 1987 and 1989. See Larry Thompson, "Commentary: With No Magic Cure in Sight, Dramatic Epidemic Loses Luster as News Story," Washington Post Health, June 13, 1989, p. 7.
Once again, it has become event-driven, focusing above all on occasions that can be planned for well in advance, especially the annual international AIDS conferences. But in contrast to the earlier phases, in which spokespersons for the gay movement or for people with AIDS were consulted only when stories were cued by scientists or by politicians, the post-1987 coverage has been shaped by the routine ability of these sources to make news on their own, particularly as they anticipate and plan for just such long-scheduled events. These sources have hailed not only from more mainstreamed groups such as the National Lesbian and Gay Task Force or the Names Project but also from confrontational organizations such as the AIDS Coalition toUnleash Power (ACT UP). ACT UP, particularly in its earliest stages, often received respectful coverage, which is striking given its members' penchant for disrupting speeches, conducting sit-ins (or "die-ins"), and getting arrested. But ACT UP's more radical and far-reaching critique that science and medicine were inherently political may have been blunted. Though ACT UP received air time, journalists either framed its agenda as reformism favoring anti-bureaucratic, clear-cut good-government solutions or reported the demonstrations as political theater in, of, and for itself.[78]
Future scholars will want to study the development of ACT UP as it interacted with the news media, since those interactions seem to be subject to the same dynamics that Todd Gitlin identified for the New Left in The Whole World Is Watching: The Mass Media in the Making and Unmaking of the New Left (Berkeley: University of California Press, 1980).
In the 1990s, then, the coverage of the HIV epidemic, though avoiding the extraordinary focuses of its peaks in 1983, 1985, and 1987, should continue to be a routine and relatively constant news item. There are, to be sure, some drawbacks to routine coverage, insofar as saturation of the airwaves may be necessary to keep individuals vigilant about proper prevention, such as safer sex. But it avoids the on-again, off-again cycle of alarm and reassurance that proved debilitating in the first years of the epidemic.
Yet the future coverage of the epidemic will be far from problem free. The network news lagged in realizing that the epidemic has slowed among the initial high-risk group of gay men but continues to rage within the population of intravenous drug users, and primarily through them into urban minority communities and to women. Such sectors are even less organized and less legitimated to speak for themselves than were gay men in the early 1980s, and their ability to influence the future progress of the epidemic may be seriously harmed. If journalists are to play a virtuous part in stemming the HIV epidemic, they must take care to reflect a democratic variety of voices, whether or not these voices are connected to the usual authoritative sources and whether or not their concerns can be linked to the supposed "general population." But given the constraints on journalism that push it toward elite sources and away from democratized news, we cannot be optimistic that such reporting will indeed occur.