PART II—
THEMATIC
Three—
The Body and the Mind, The Doctor and the Patient:
Negotiating Hysteria
Roy Porter
Diseases
A central aim of medical history must surely be to chart the history of disease, for without that, we will never fully gain a sense of people's health, sufferings, morbidity profiles, life expectations, and expectations out of life.[1] Some historians go so far as to claim that pathogens have perhaps been the most potent agents of sociopolitical change at large.[2] And without proper understanding of microbes and toxins, it has been contended, the history of hysteria will be misread. For according to Mary Matossian, what contemporaries and scholars alike have identified as eruptions of mass hysteria—the late medieval witch craze, religious revivals, la grande peur —ought properly to be read as the symptoms of ergotism.[3]
Yet, as is shown by scholarly scepticism toward such claims, identifying past diseases presents daunting challenges. With all our semiotic skills and modern clinical expertise, are we able to decode the medical texts, eyewitness accounts, and mortality records of bygone centuries and alien cultures, and trace the natural histories of diseases?[4] Was the "ague" of early modern England truly malaria, or "quinsey" a streptococcal infection? On the basis of Thucydides' description of the so-called "great plague" of Athens, scholars have come up with dozens of disease labels (though such is the debris of discarded identifications, that only fools should rush in).[5]
The hazards of retrospective diagnosis teach a salutary scepticism. After all, as epidemiologists know, microorganisms themselves mutate, following unpredictable evolutionary biogeographies. Perhaps the Athe-
nian plague, or the decimating "great sweat" of early-Tudor England, that mysterious disorder, were due to pathogens that came and went. And, in any case, our forebears may have reacted to this or that infection in ways foreign to modern symptomatologies—to the despair of the historical epidemiologist but the delight of the shameless relativist. The former expects disease to obey laws, regularly producing predictable effects; the latter may, by contrast, luxuriate in the heterogeneity of subjective experiences of affliction.[6] Medical historians must soldier on, using what evidence they can: skeletal remains, artifacts (paintings, photographs), and written testimony, though words may be false friends: what early moderns called "cholera" was certainly not the "Asiatic" cholera that swept Europe and North America in the nineteenth century, although its identity still baffles inquiry.[7]
So what of hysteria? Are historians to think of hysteria as a true disease, whose rise and fall can, in principle, be plotted down the centuries, so long as we exercise vigilance against anachronistic translation of archaic concepts? Or is it a veritable joker in the taxonomic pack, a promiscuous diagnostic fly-by-night, never faithfully wedded to an authentic malady—or worse, a wholly spurious entity, a fancy-free disease name, like Prester John, independent of any corresponding disease-thing, a cover-up for medical ignorance? Or, worse still, may hysteria truly have been the doctors' Waterloo: a real disorder, but, as Alan Krohn hints, one so "elusive" as to have slipped our nosological nets?[8]
For reasons clear to every reader of this book, "hysteria" inevitably induces doubts. Yet why shouldn't a history of hysteria be written? Not one expecting (in the manner of Professor Matossian) to unearth a microtoxin as vera causa , nor even one tracing progress from medical confusion to medical clarification. But a history of hysteria experiences, that is, of people labeled as hysterical, or identifying themselves as suffering from the condition, and embodying it in their behavior; one taking into account all the intricate negotiations, denials, and contestations bound to mediate such multifarious sickness presentations.[9]
Such a history could be written while judgment is suspended about hysteria's ontology. Scholars, after all, habitually trace the incidence of various fevers—low, spotted, and remitting—while remaining in the dark as to their etiology; "war fever" or "gold fever" are also discussed without obligation to specify the root cause of these drives. The embossing of hysteria—perhaps unlike spotted fever—with cultural meanings does not discredit such a project, but makes it all the more inviting.
We should expect not a single, unbroken narrative but scatters of occurrences: histories of hysterias, in fact. Yet the chronological epicenter
is bound to be the nineteenth century. As Helen King has shown in chapter 1, antiquity and medieval Europe had no need of the hysteria concept.[10] And—so runs G. S. Rousseau's discussion in the previous chapter—though from Renaissance to Enlightenment physicians developed the hysteria diagnosis, it remained largely subordinate to discourses about melancholy and the nerves.
It was during the nineteenth century that hysteria moved center-stage. It became the explicit theme of scores of medical texts.[11] Its investigation and treatment made the fame and fortunes of towering medical figures—Charcot, Breuer, Janet, and Freud. Hysteria came to be seen as the open sesame to impenetrable riddles of existence: religious ecstasy, sexual deviation, and, above all, that mystery of mysteries, woman.
Moreover, people began to suffer from hysteria, or (what amounts to the same thing) to be said to suffer from hysteria, in substantial numbers. In novels[12] and newspapers, police reports and social surveys, the predicaments of mass society, crowd behavior, street life, and social pathology were endlessly anatomized in the idiom of hysteria.[13] And—often in compound forms, such as hystero-epilepsy—hysteria became traded as a common currency between the sick, their families, their medical attendants, and the culture at large: witness the repeated illness episodes undergone in the 1830s by Ada Lovelace, Byron's daughter (needless to say, the word carried deeply divergent nuances for Ada, her mother, her husband, and her flock of medical attendants).[14]
Hysteria's clientele broadened. One senses that, in the eighteenth century, the term still circulated in rather confined, indeed, refined, circles. That changed. As may be seen from Charcot's practice, hysteria became, at least by the belle epoque , established as a disorder of males as well as females,[15] of sensitive and silly alike: perhaps none was wholly immune. In his discussion in chapter 5, Sander Gilman documents the extension of "hysterical" to certain ethnic types, notably Semites.[16]
Furthermore, as Edward Shorter has emphasized, a multitude of nineteenth-century records—police, hospital, and Poor Law—testify that the terminology of hysteria shed most of its class exclusiveness. Shop girls, seamstresses, servants, street walkers, engine drivers, navvies, wives, mothers, and husbands too, were now eligible for depiction as hysterical alongside their betters, and not merely (as in Restoration comedy) as mimicry à la mode.[17] The coming of mass society evidently democratized the disorder.
Institutional evidence attests this. In the mid-nineteenth century, Robert Carter alluded to hysteria epidemics in workhouses as though such outbreaks were common.[18] Victorian asylum records show patients
sectioned with hysteria written into their diagnosis or figuring in their case notes.[19] Establishments—hydros, spas, retreats, sanatoria, nursing homes—started catering to private patients suffering from hysteriform conditions.[20] Shorter has explored the procedures that filtered invalids of a certain class or income into superior institutions (with greater freedom and privileges), under choicer diagnostic verbiage. Considerable linguistic tact was requisite. Too psychiatric a diagnosis could suggest psychosis, or downright lunacy, with connotations unacceptable for the family. An overly physicalist term might come too near the bone by suggesting a tubercular condition or syphilis and its sequelae. Dexterity with diagnostic euphemisms was at a premium: this became the age of "neurasthenia."[21]
Finally, and to us, most famously, there was the string of clients climbing the stairs at Berggasse 19. If some were "hysterics" largely by virtue of being so designated by others, Freud's patients, it seems, mainly volunteered. Freud strenuously contested his patients' "denials," but none of them, not even Dora, seems to have denied that he or she was hysterical.[22]
One could thus trace the hysteria wave (or one might say craze, epidemic, or simply spread). Its cresting at that time seems perfectly amenable to explanation, without need to resort to crass reduction-ism (vulgar labeling or social control theory, or the medical dominance model). Cultures, groups, and individuals respond in different ways to life's pains and pressures; idioms of suffering and sickness can be more or less expressive; direct or indirect; emotional, verbal, or physical; articulated through inner feelings or outward gesture. Varied repertoires clearly register the tensions, prohibitions, and opportunities afforded by the culture (or subculture) at large, reacting to expectations of approval and disapproval, legitimation and shame, to prospects of primary penalty and secondary gain.[23]
Some societies legitimize psychological presentations of suffering, while others sanction somatic expression. Affluent New Yorkers are today allowed, even expected, to act out trauma psychologically. Mao's China, by contrast, apparently condemned such performances as lapses into inadmissible subjectivism and political deviancy. Hence "feeling bad" in the Republic had to be couched in terms of a physical debility or malfunction that escaped censure and solicited sympathy and relief.[24]
In this respect, the sickness culture of nineteenth-century Europe and North America seems to have borne some resemblance to modern China. In a fiercely competitive economic world, high performance was expected, with few safety nets for failures. There were intense pressures
toward inculcating self-control, self-discipline, and outward conformity (bourgeois respectability). Personal responsibility, probity, and piety were, furthermore, internalized through strict moral training, imparted via hallowed socialization agencies like the family, neighborhood, school, and chapel. Guilt, shame, and disapproval were always nigh. In such stringent force fields, feelings of distress or resentment, anxiety or anger, were inevitable but difficult to manage; they were commonly "repressed" or rerouted into one of the rare forms of expression that were legitimate: the presentation of physical illness. Being sick afforded respite and release to those who needed temporarily or permanently to opt out.[25] And the system was skewed so that some took the strain more than others. Women were disproportionately burdened, being more isolated and incurring intenser expectations of moral and sexual rectitude; ladies often had time for reflection without outlets for their talents.[26]
Such concatenations of circumstances—high pressures, few safety valves—seem almost tailor-made for hysteria, viewed (as, of course, many nineteenth-century physicians themselves viewed it) as a disorder whereby nonspecific distress was given somatic contours.
Symptom choice involves complex learning and imitative processes. Picking up hysteria was aided by the fact that nineteenth-century public life put on view an abundance of physical peculiarities: gait disorders, paralyses, limps, palsies, and other comparable handicaps. Such conditions were the effects of birth defects and inherited diseases, of syphilis, lead and mercurial poisons at the workplace, of overdosing with unsafe drugs, industrial accidents, and high levels of alcoholism with consequent delirium tremens . The visibility of real biomedical neurological disorders enticed and authenticated those seeking a sickness stylistics for expressing inner pains.
Shorter has further argued, as have many feminist scholars, that a certain rhyme and reason may be discerned in the symptom selection.[27] The gastric disorders men widely "adopted" were compatible with continuing an active life, and hence with a certain model of masculinity. Being a hysterical woman, by contrast, meant exhibiting a battery of incapacitating symptoms emblematic of helplessness, enfeeblement, and (with lower limb paralyses) immobilization, acting out thereby, through sickness pantomime, the sufferer's actual social condition. Hysteria was thus mock escape by self-mutilation (a male analogue finally emerged in the First World War with shell shock).
We need detailed a history "from below" of rank-and-file nineteenth-century hysterics, and not just of such "immortals" as Blanche Wittmann, Léonie B., and Anna O. It would enhance our grasp of the elec-
tive affinities between disease and culture, confirming the adage that every society gets the disorders it deserves. Alongside epidemiology, medical history needs to study the history of illness, that is, of sufferers' conditions, regardless of science's judgment upon their authenticity. Aside from metaphysical questions (is hysteria a real disease?), it is clear that our great grandparents suffered from hysteria, no less than Elizabethans underwent the "sweat" or we succumb to "depression," "stress," or low-back pain; it is the job of historians to explain how and why.[28]
This grass-roots history of hysterics, this social history of symptoms, should be high on the agenda. But it is not what the remainder of this chapter tackles. Instead, I shall explore the medical profession's attempts to resolve the hysteria mystery, a disorder enigmatic because it hovered elusively between the organic and the psychological, or (transvaluating that ambivalence) because it muddled the medical and the moral, or (put yet another way) because it was ever discrediting its own credentials (were sufferers sick or shamming?). In this, I have in mind several larger goals. I want to explore the opportunities hysteria offered, and the puzzles it posed, for the medical profession: was it to be their finest hour or their Waterloo? I shall probe how differential readings of hysteria suited diverse sectors of a profession increasingly specialized and divided. Not least, I wish to gauge hysteria's symbolic replay (parody even) of the interactions between doctors and patients, suggesting how, in psychoanalysis, it launched a wildly new and deeply aberrant script of doctor-patient interplay.
Hysteria/Mysteria
Nineteenth-century doctors habitually represented hysteria as a challenge, a tough nut to crack. Chameleonlike in its manifestations, and often aggravated by their ministrations, it did not fight by the Queens-bury Rules.
Medicine's flounderings suggest that hysteria proved something "other," the one that got away. Consensus never crystallized as to its nature and cause. In recent years, it has waltzed in and out of the Diagnostic and Statistical Manual , the English-speaking world's authoritative psychiatric handbook. Disgruntled doctors have often proposed conceptual slum clearance and a fresh terminological start: Josef Babinski wanted to rename it "psychasthenia" or "pithiatism," Janet suggested "psychasthenia," and certain contemporary physicians prefer "Briquet's syndrome,"[29] all in the, surely vain, hope that old confusions were but word deep. As the shrewd reassessments of Alec Roy, Harold Merskey, Alan
Krohn, and others have made clear, medicine today remains deeply divided as to whether hysteria is a skeleton in the cupboard or a ghost in the machine; a phantom like "the spleen," or a bona fide disorder. And if authentic, is it organic or mental? A disease that has largely died out or been cured, or one camouflaging itself in colors ever new?[30]
Such battles long since spilled over time's border into the terrain of history. A cast of heroes and villains from the past has been recruited to play key roles. Indeed, as Helen King established earlier in this volume, when Renaissance doctors first needed to develop the hysteria concept, high priority was given to manufacturing a pedigree going all the way back to Hippocrates.[31] Physicians have also turned to the past to exercise their skills in retrospective diagnosis: preferred readings of hysteria will, it is assumed, be vindicated if they lead to the identification of former outbreaks. After all (so argued nineteenth-century bio-medics), what is medical science if not an engine for discovering nature's universal laws, operating uniformly through time and space, in the past, present, and future? Thus Charcot declared in ringing tones that "L'Hystérie a toujours existé, en tous lieux et en tous temps."[32] In Les Demoniaques dans l'art (1887), jointly written with his colleague Antoine Richer, he contended that what benighted ages had mistaken for mystics and demoniacs were archetypically hysterics. By thus exposing the hysteria so long hidden from history, Charcot strengthened his claim to be, in the there-and-then as well as the here-and-now, the all-conquering "Napoleon of the neuroses." Further medical demystification of religious enthusiasm by D.-M. Bourneville and other intimates of the charcoterie helped mobilize the radical, anticlerical medical politics of the Third Republic.[33]
Psychiatrists such as Gregory Zilboorg subsequently developed these retrospective diagnoses of early modern demoniacs as sick people possessed, not by the devil, but by disease, as people fit, not for the flames, but for the couch. In propagating such views, analysts from Freud to present psychohistorians have presented themselves as pioneers of therapeutic methods and historical readings both enlightened and scientific.[34]
Historiography
And historians of hysteria have characteristically followed in their footsteps: it was no accident that the first substantial chronicles of hysteria were written by Charcotian protégés.[35] Such works have assumed that the annals of medical history, down the centuries and across the cul-
tures, point to outcrops of a disorder now identifiable as hysteria, and that the medical mission of understanding, classifying, and treating it can be recounted as a progression from superstition to science, ignorance to expertise, prejudice to psychoanalysis. The standard English-language history, Ilza Veith's Hysteria: The History of a Disease (1965), is wholly cast within this mold.[36]
As her title indicates, Veith's premise is that hysteria is an objective disease, the same the whole world over. It had been known to doctors—East and West—at least from 1800 B.C ., Veith contended, though it was the Greeks who had given it its name. Medieval Christendom's gestalt switch, treating psychosomatic symptoms as the stigmata of Satan, had entailed a gigantic regression.[37] Fortunately, far-sighted Renaissance physicians such as Johannes Weyer had recaptured hysteria from the theologians, seeing it as a disease, not a sin.
Even so, true understanding (and treatment) continued to be hamstrung by a fallacious medical materialism misconstruing hysteria as organic—standardly, an abnormality of the womb, or, in later centuries, of the nervous system and brain stem. Veith particularly deplored the "increasingly sterile and repetitive neurological basis that had emanated from Great Britain for nearly two hundred years," sparked, above all, by George Cheyne's "nervous" theory, whose "affectation and absurdities are such that it scarcely merits elaborate discussion"—even the Scottish iatromechanist's "references to his own distress," Veith uncharitably grumbled, "seem inconsequential."[38] Not least, she argued, somatic hypotheses had been marred by misogyny. Overall, such ideas were precisely the obstacles that, in Freud's view, had "so long stood in the way of [hysteria] being recognized as a psychical disorder."[39]
Fortunately, according to Veith, a counterinterpretation had emerged, albeit by fits and starts. Brave spirits such as Paracelsus, Edward Jorden, Thomas Sydenham, Franz Anton Mesmer, Philippe Pinel, Ernst von Feuchtersleben, and Robert Carter began to develop "an amazing amount of anticipation" of the insight—finally triumphant with Freud—that hysteria was psychogenic, the monster child of emotional trauma aggravated by bourgeois sexual repression, especially of females.[40] Thanks principally to Freud, this libidinal straitjacket had finally been flung off, leading to the disorder's demise in the present century: Veith's narration concluded with Freud.
It says something for the vitality of medical history that, twenty-five years later, Veith's recension appears hopelessly outdated. For one thing, hers was heroes-and-villains history, being particularly free with bouquets for those who "anticipated" Freud's psychosexual theory. Among these,
the mid-Victorian practitioner Robert Carter received her most fulsome floral tributes, for having effected "a greater stride forward" than "all the advances made since the beginning of its history."[41] This rosy interpretation of Carter grates, however, upon a modern generation primed on antipsychiatry and feminism. After all, it was precisely his judgment that hysteria was psychogenic that enabled Carter to indict hysterical women as not sick but swindlers, sunk in "moral obliquity," cynically exploiting the sick role to manipulate their families and getting perverse sexual kicks out of the repeated vaginal examinations they demanded. Carter, however, saw through their tricks and advocated subjecting them to ordeal by psychiatric exposure.[42] With Dora's case in mind, we might wryly agree with Veith that Carter did indeed "anticipate" Freud, but such a compliment would, of course, be backhanded, underlining that Freud too could be a misogynistic victim blamer and therapeutic bully. Faced with the deviousness of hysterics, Freud confided to Wilhelm Fliess his sympathy for the "harsh therapy of the witches' judges."[43]
More generally, Veith's "history of a disease"—indeed, of a "mental disease"[44] —conceived as a joust between benighted (somatic) theorists, who "retarded" comprehension, and their forward-looking psychological rivals, suffers from the stock shortcomings of wise-after-the-event Whiggism.[45] Past theorists are graded by the yardstick of Freud, whose theory is taken as the last word. With hindsight derived from the psychodynamic revolution, Veith organizes her history of hysteria around an essential tension between (wrong) somatogenic and (valid) psychogenic claims.
A radically different reading is offered by Thomas Szasz. For Szasz, hysteria is not a real disease, whose nature has been progressively cracked, but a myth forged by psychiatry for its own greater glory. Freud did not discover its secret; he manufactured its mythology.[46] Drawing upon varied intellectual traditions—logical positivism, Talcot Parsons's theory of the sick role, ethnomethodology, and the sociology of medical dominance—Szasz has made prominent, in his The Myth of Mental Illness ,[47] psychoanalysis's "conversion" of hysteria into a primary psychogenic "mental illness" marked by somatic conversion, the translation, as William R. D. Fairbairn put it, of a "personal problem" into a "bodily state."[48] "I was inclined," reflected Freud, "to look for a psychical origin for all symptoms in cases of hysteria."[49]
Exposing this as a strategy integral to a self-serving "manufacture of madness," Szasz counters with a corrosive philosophical critique. By thus privileging the psyche, Freud was in effect breathing new life into the
obsolete Cartesian dualism, resurrecting the old ghost in the machine, or rather, in the guise of the Unconscious, inventing the ghost in a ghost.[50] For Szasz, on the other hand, the expectation of finding the etiology of hysteria in body or mind, above all in some mental underworld, must be a lost cause, a dead end, a linguistic error, and an exercise in bad faith. For the "unconscious" is not a place or an organ but, at most, a metaphor; Freud stands arraigned of rather naively pictorializing the psyche in hydraulic and electrical terms, of reifying the fictive substance behind the substantive.[51]
Properly speaking, contends Szasz, hysteria is not a disease with origins to be excavated, but a behavior with meanings to be decoded. Social existence is a rule-governed game-playing ritual. The hysteric bends the rules and exploits their loopholes. Not illness but idiom (gestural more than verbal), hysteria pertains not to a Cartesian ontology but to a semiotics, being communication by complaints . Since the hysteric is engaged in social performances that follow certain expectations so as to defy others, the pertinent questions are not about the origins, but the conventions, of hysteria.[52]
Sidestepping mind/body dualisms, Szasz thus recasts hysteria as social performance, presenting problems of conduct, communication, and context. Freud believed mind/body dichotomies were real, though typically mystified, and attempted to crack them. Szasz dismisses these as questions mal posées , deriving (like Freud's "discovery" of the unconscious) from linguistic reification or bad faith, and he aims to reformulate them.
If idiosyncratic, Szasz's analysis is also a child of its time. Modern linguistic philosophy, behaviorism, and poststructuralism all depreciate the etiological quest: origins, authors, and intentions are discounted, systems, conventions, and meanings forefronted. Szasz does not, of course, expect that his paradigm-switch will magically switch off all the uncontrollable sobbing, fits, tantrums, and paralyses. But it offers alternative readings of such acts, while undermining expectations that tracking hysteria will lead to the source of the Nile, that is, the solution of the riddle of mind and body.[53]
Szasz's resolution of hysteria is bracing, but it is achieved at the cost of reducing its past to pantomime: his adoption of the language of game-playing turns everyone, sufferers and medics alike, into manipulative egoists. Illness is just a counter in a contest. So why embrace this dismissive, belittling view? It is because Szasz is at bottom an old-school medical materialist: disease is really disease only if it is organic.[54] Were hysteria—were any so-called mental illness—somatically based, it would have a real history (afflicting people, being investigated by physicians). Lacking organic "papers," its past, rather like those of transubstantiation
or of perpetual-motion engines, is a blot, a disgrace, a fiction, a tale of knaves and fools worthy of some philosophe's pen.
Thus, for equal but opposite reasons, Veith and Szasz both short-circuit hysteria's history. Veith (oddly like Charcot) feels obliged to trace it from the pharoahs to Freud; Szasz thinks the history of hysteria begins with Freud's psychodynamic empire building. Believing hysteria psychogenic, Veith recounts her "history of a disease" as the road to Freud. Believing disease must be somatic, Szasz paints hysteria's history as the pageant of a dream. Both approaches trivialize the intricate texture of hysteria down the ages, the true understanding of which must respect, not explain away, the enigmas of multifaceted, evanescent pain in a culture within which mind/body relations have been supercharged and devilishly problematic.
Yet Veith's and Szasz's polarized readings are, in their own way, highly exemplary, for they both highlight mind/body disputes in hysteria's etiology. Down the centuries, physicians long lamented how hysteria remained sphinxlike, because mind/body relations themselves proved a conundrum. Veith's desire to divide her protagonists into ("retarding") materialist and ("progressive") psychological camps is, however, misguided, for it freezes the rhetoric of the Freudian era and anachronistically backprojects it. Yet Szasz's mythic history, subserving his own debunking and liberating polemic, also cuts corners, above all by seemingly denying any significant developments before Freud. Many recent historians, especially Mark Micale,[55] have, by contrast, insisted on the enormous intricacy and indeterminacy of the story of hysteria. Above all, as will be explored below, it would be simplistic to imply that early theories were exclusively either somatogenic or psychogenic; most commonly they were attempts to dissect and plot the puzzling entente between the passions of the mind and the constitution of the body. Our story is thus not a matter of either/or but of both/and. And it is, above all, a history in which the very notions of mind and body, and the boundaries and bridges between them, were constantly being challenged and reconstituted.
Hence this chapter will focus on medical theorizings of mind/body pathologies. It will thus engage the metaphysics of hysteria, examining the theoretical underpinnings that made possible a succession of puzzles, problems, and solutions. The story of hysteria (I will argue) makes scant sense if restricted to internal, technical skirmishings over nerves and neurons, passions and pathogens. Far more was at stake, not least because, as Szasz has insisted, hysteria became an exemplary disease, the disorder that single-handedly launched psychoanalysis.
Small wonder this wider history is requisite, for the biomedical doc-
trines of body and brain, psyche and soma, have never been neutral post-mortem findings, hermetically sealed from the symbolic meanings accreting around sickness in daily experience, meanings of utmost significance for doctrines of human nature, gender relations, moral autonomy, legal responsibility, and the dignity of man.[56] Medicine's authority, its prized scientificity, may have rested upon its vaunted monopoly of expertise over the human organism, but its public appeal has equally hung upon its ability to attune its terms and tones to the popular ear. The historian of hysteria must, in short, bear in mind the wider determinants: changing ideas of man, morality and culture, and the politics of medicine in society.
Mind and Body: Medical Materialism and Hegemonic Idealism
I wish to explore a further dichotomy—Charcot's historical metaphysics juxtaposed against Freud's—to show its exemplary status for understanding the mind/body politics of hysteria.
To secure their credentials, many nineteenth-century medics proclaimed a powerful metahistory: Auguste Comte's scheme of the rise of thought, from the theological, via the metaphysical, up to the scientific plane.[57] As embraced by positivists, par excellence those in Charcot's circle, such a progressive schema implied that sickness had, at the dawn of civilization, been misattributed to otherworldly agencies (spirit possession, necromancy, etc.), subsequently being mystified into formulaic verbiage (humors, animal spirits, complexions) dissembling as explanations. Growing out of such mumbo jumbo, physicians had finally learned to ground their art in the nuts-and-bolts real-world of anatomy, physiology, and neurology.[58] Through abandoning myths for measurement, words for things, metaphysics for metabolism, medicine had at long last grasped the laws of nature, which would prove the prelude to effective therapeutics. According to Charcot (as will further be explored below), hysteria would be solved by pursuing the science of the body.
Freud, however, though Charcot's sometime student, cuts across the grain of this explanatory strategy—indeed, presents a case of ontogeny reversing phylogeny. The young Freud had been inducted into the Germanic school of neurophysiology, whose creed (paralleling the positivist) espoused the triple alliance of scientific method, medical materialism, and intellectual progress: explanations of the living had to be somatically grounded or they weren't science. Though initially endorsing this neurological idiom, Freud, in his own theorizings of neuroses and hysteria,
eventually adopted a thoroughgoing psychodynamic stance, eventually formulating a battery of mentalist neologisms—the unconscious, ego, id, super ego, death wish, and so on—which logical positivists have ever since derided as throwbacks to Comte's "metaphysical" stage.[59] In tandem, Freud's therapeutics moved from drugs (e.g., cocaine), through hands-on, pressure-point hypnosis, to the purely psychical (free speech associations).[60] Freud, some would say, was a kind of mental recidivist.
In thus privileging the mind as primum mobile , Freud challenged biomedicine's bottom line—and regarded himself as victimized for his pains, while energetically milking his self-image as a persecuted heretic.[61] Yet, by so doing, he has won a standing ovation from twentieth-century high culture, predisposed to believe that explanations of human behavior predicated upon the workings of the mind , however dark and devious, must be more profound, humane, insightful, true, and titillating even, than any formulated in biochemical or genetic categories.[62] As we have seen, Veith herself assumed that once Freud finally discovered hysteria to be psychogenic , the curtain could be brought down to rapturous applause. Psychoanalysis's "discovery of the unconscious,"[63] unlocking the secrets of human desires, both normal and pathological, remains one of the foundation myths of modernity.
In addressing the rival paradigms of fin de siècle hysteria, we thus find a cross fire—the one scientific, ratifying positivist laws of the organism; the other convinced that meaningful explanations of action must derive from an ontology of the psyche. This is an instructive dichotomy (biologism/mentalism), reproducing in a nutshell two clashing configurations of Western thought.
On the one hand, psychoanalysis's mentalism is underpinned by the pervasive and prestigious Idealism, philosophized by Platonism and the Cartesian cogito , long underwritten by Christian theology, and, in secular garb, still the informal metaphysical foundations of the humanities in C. P. Snow's "two cultures" dichotomy. Such hierarchical, dualistic models programmatically set mind over matter, thinking over being, nurture over nature, head over hand, as higher over lower, the mental being ontologically superior to the corporeal. Macrocosmically, brute matter was subordinate to the Divine Mind or Idea, acting through immaterial agencies; likewise, microcosmically, the achievement of mens sana in corpore sano required that mind, will, or spirit must command base flesh—and, as Theodor Adorno, Norbert Elias, Foucault, and others have argued, the civilizing process, that celebrated march of mind demanded by capitalism, long entailed the intensification of body-disciplining techniques.[64] Within this view, sickness is regarded (like crime, vice, or sin)
as the aftermath of reason losing control, either because the metabolism itself has been highjacked (for instance, in the delirium of fever), or when civil war erupts within the mind itself, leading to the "mind forg'd manacles" of mental illness.[65]
Freud torpedoed theology, wrestled with philosophy, but loved science. His views of the drives and the unconscious naturally could not countenance the Christian-Platonic divine-right monarchy of Pure Reason: it is, after all, the mission of psychoanalysis to debunk such illusions (purity indeed!) as projections, sublimations, and mystifications.[66] Nor could he accept at face value the doctrinaire distinctions between freedom and necessity, virtue and appetite, love and libido, and so on postulated by philosophical Idealism. These—like so many other values—were not eternal verities, gifts from the gods, but problematic, sublimated, even morbid, constructs ("defences"). Nevertheless, the thrust of Freudian psychodynamics—his point of departure from Wilhelm Brücke, Charcot, and Fliess, and then from some of his own epigoni such as Wilhelm Reich—lay in denying the sufficiency of biology or heredity to explain complexities of behavior, healthy or morbid. In the case of complexes, the body becomes the battleground for struggles masterminded elsewhere.[67]
Freud was deeply torn. Clinical experience led to his giving sovereignty to the psyche. Yet herein lay a profound irony, for he was also, as Peter Gay has aptly emphasized, a child of the old Enlightenment itch to smash Idealism, unveiling it as the secret agent of false consciousness, repression, and priestcraft.[68] He was, moreover, heir, by training and temper, to the crusading medical materialism and biophysics of his youthful heroes—Hermann Helmholtz, Theodor Meynert, and his mentor, Brücke, not to mention Charcot himself. For such luminaries, as for the Freud of the abandoned 1895 Project, doing science meant translating behavior into biology, consciousness into neurology, random experience into objective laws. And in pursuing such positivist approaches, nineteenth-century bioscientists were, as Lain Entralgo has stressed, further endorsing the disposition, from the Greeks onward, in what was significantly titled "physick," to enshrine the body as the ultimate "reality principle."[69]
The body provides sufficient explanation of its own behavior. Diseases are in and of the organism. They are caused by some fluid imbalance, physical lesion, internal dislocation, "seed" (or foreign body), excess, deficiency, or blockage; material therapeutics—drugs and surgery—will relieve or cure. Abandon such home truths, such professional articles of faith, and the autonomy and jurisdiction of biomedical science and clinical practice melt like May mist. Once it were admitted that
sickness could not be sufficiently explained in and through the body—unless it could be said, at some level, "in the beginning, was the body"—medicine would forfeit its title as a master discipline, grounded upon prized clinicoscientific expertise. Unless sickness is translatable into the lingo of lesions and laws, why should not anyone—priests, philosophers, charlatans, sufferers—treat it as well as a doctor? Herein lies the explanation of why scientific medicine committed itself, from the Renaissance, to evermore minute anatomical and physiological investigations, even though the therapeutic payoffs long remained unconvincing.
Yet this strategy for ratifying professional credentials through a science of the body naturally ran the risk of counterproductivity. For, in a culture-at-large in which Idealism was hegemonic, medicine thereby exposed itself to the charge that its incomparable organic expertise was purchased at the price of higher dignity: a liability perfectly summed up in Coleridge's damnation of the doctors for their debasing somatism: "They are shallow animals," judged the ardent Platonist, "having always employed their minds about Body and Gut, they imagine that in the whole system of things there is nothing but Gut and Body."[70]
The program widely, if tacitly, adopted by medicine since the scientific revolution of locating disease explanations within the body seemed unexceptionable when addressing conspicuous conditions—tumors or dropsy, for instance—involving physical abnormalities. It has proved more problematic, however, where pain flares seemingly independently of manifest external lesions: even today medicine is embarrassed when faced with common complaints such as nervous exhaustion, stress, or addiction. And medicine's claims encounter special strain in cases where disturbances are sporadic and seemingly irrational. It is in these borderland areas, the fields of so-called functional and nervous disorders where sickness experience wants secure somatic anchorage, that medical credit is least convincing. If suffering lacks lesions and localizations, why should it be medicine's province at all? After all, leading critics from within the profession, notably Thomas Szasz, have invoked medicine's cherished criteria (logical positivism and methodological materialism) to contend that, since physick's kingdom is the body, and medicine is thus definitionally organic (else it is a chimera), the very idea of primary mental illness should be struck off the register as a category error, a misleading metaphor—or, worse, a pious fraud, smacking of professional bad faith.[71] Medicine has jurisdiction over the somatic, but who authorized its writ to run one step beyond? As G. S. Rousseau's essay has shown, physicians long ago hoisted their flag over hysteria; but the terra incognita has ever proved remarkably resistant to assured colonization.
Thus ours has been a civilization in which, in an ideological shadow
play of the sociopolitical order, hegemonic Idealism has traditionally enthroned mind over what theology denigrated as the "flesh," forever too, too solid and sullied.[72] At the same time, medicine, by embracing (proto)-positivist notions of science and professional territorial imperatives, has espoused a praxis affording it control over the organic. Superficially it might seem that these two drives—enshrining spirit, yet making matter the foundation stone of science—are radically incommensurable. Yet doctors live in the world and medicine needs to be credit-worthy; or, in other words, accommodations have ever been reached, or ensure that cultural idealism and medical materialism work in broad harmony, rather than on a collision course.[73]
Medicine, philosophy, and theology developed thought-packages designed to demarcate the domains and specify the pathways of mind and matter. Thus, so ran long-standing prescriptions, the rules of health required that mind must be in the saddle, enacting the precepts of philosophers and preachers. Whenever the reign of reason is challenged, when brute flesh mutinies, the resultant state is sickness, and then the mentor makes way for the doctor. In any case, and giving the lie to Coleridge's slur, physicians themselves, time out of mind, have prescribed. liberal doses of willpower as the recipe for "whole person" well-being: be healthy-minded, think positive, exercise self-control. As Michael Clark has brilliantly shown, late Victorian doctors characterized the sound, responsible person as one who tempered the will and disciplined the body, channeling the energies, like a true Aristotelian, into healthy public activity. By contrast, the hypochondriac or degenerate was trapped in morbid introspection, prisoner, in Henry Maudsley's graphic phrase, of the "tyranny of organization."[74]
So cultural Idealism and medical materialism, though perhaps worlds apart, have rarely been daggers drawn. Each assigned roles to the other within its own play. Even medical materialists such as Julien de La Mettrie recognized that, taken to extremes, to reduce man to nothing but l'homme machine would be self-disconfirming, while no less an idealist than Bishop George Berkeley did not hesitate to tout tar-water as a panacea.[75] Thus cultural Platonism and medical materialism are best regarded as uncomfortable matrimonial partners, who have engaged in partial cooperation to frame images of the constitution of man, the dance of soma and psyche, the triangle of sanity, salubrity, and sickness, and, not least, of the politics of the moral/physical interface.[76]
For doctors have to operate in the public domain, jostling with rivals in expertise and authority, and their services ultimately have to please paying patients. So medicine cannot afford to bury itself in sprains and pains but must engage with wider issues—religious, ethical, social, and
cultural. The public wants from doctors explanations no less than medications; society looks to the profession for exhortation and excuses. Medicine is called upon to supply stories about the nature of man and the order of things. Moreover, because medicine has never enjoyed monopoly—nor has it been monolithic; it has been divided within itself—it has developed multiple strategies for securing its place in the sun.
It would, in fine, be myopic to treat medicine as a limited technical enterprise. This is especially so when we are faced with interpreting the peculiarities of hysteria, a disorder that, as indicated, dramatically rose and fell between the Renaissance and the First World War, a trajectory indubitably linked to larger cultural determinants affecting patients and practitioners alike.
Hysteria presented doctors with a tease, a trial, and a break. The hysteria diagnosis, critics griped, was the most egregious medical hocus-pocus, attached to symptom clusters physicians could not impute to some more regular cause. The symptoms were heterogeneous, bizarre, and unpredictable: pains in the genitals and abdomen, shooting top to toe, or rising into the thorax and producing constrictions around the throat (globus hystericus ); breathing irregularities; twitchings, tics, and spasms; mounting anxiety and emotional outbursts, breathlessness, and floods of tears; more acute seizures, paralyses, convulsions, hemiplagias, or catalepsy—any or all of which might ring the changes in dizzying succession and often with no obvious organic source. Faced with such symptoms, what was to be done? The mystery condition (spake the cynics) was wrapped up as "hysteria." Such, according to the mid-seventeenth-century neurologist Thomas Willis, was the physicians' fig leaf worn to hide their cognitive shame:
[W]hen at any time a sickness happens in a Woman's Body, of an unusual manner, or more occult original, so that its causes lie hid, and a Curatory indication is altogether uncertain. . . . we declare it to be something hysterical . . . which oftentimes is only the subterfuge of ignorance.[77]
Evidently, things did not improve. A full century later, William Buchan still felt obliged to dub hysteria the "reproach of medicine," since the "physician . . . is at a loss to account for the symptom."[78] Was hysteria then just a will-o'-the-wisp, a fabulous beast or phantom? Or was it an authentic malady, whose essence lay in having no essence, being prodigiously protean, the masquerading malady, mimicking all others?[79] And if hysteria were such a desperado, was it truly not a disease at all, but some kind of Frankenstein's monster, a brain-child of the medical imagination finally turned upon its own creators?
In the light of these grander issues—the problems of medicine's continued attempt to confirm its place within the wider culture, the mind/body ambivalence of hysteria, the brevity of hysteria's heyday, and the construal of hysteria as an anomalous monster disease—it can hardly be illuminating to write, as did Veith, about the "history of a disease" in the same manner that one might sensibly survey smallpox and its medical eradication. It would be doubly misleading to imply that medical advances successively laid bare the true roles played in the etiology of hysteria by mind and body; for, as just suggested, mind and body are not themselves cast-iron categories, but best seen as representations negotiated between culture, medicine, and society.[80] Hence, in the remainder of this chapter, I shall explore some different meanings successively assumed by hysteria, in a world in which medicine was battling to extend its sway.
My account will emphasize the initiatives of medicine. Not because I believe that doctors had unique special insight into the condition,[81] or, contrariwise, that hysteria was cynically manufactured by a malign medical mafia. I do so, rather, believing that, like invisible ink when heat is applied, hysteria was a condition chiefly rendered visible by the medical presence. Without the calling of medical witnesses to witch trials, early modern physicians would rarely have pronounced upon these bizarre behaviors. Without the leisured sufferer whose purse spelled good times for private practice, Enlightenment physicians would not have had a tale to tell of nervousness. Without confinement in the Salpêtrière hospital in the proximity of epileptics, and, above all, without the electric atmosphere of Charcot's clinic, Blanche Wittmann and other stars of hysteria would have wasted their swoonings on the desert air.[82] Robert Carter, who was cynical about those "actresses," reflected that nature knew no such being as a solitary hysteric: hysteria was a public complaint presupposing an audience—mass hysteria definitionally so.[83] Was hysteria, then, purely iatrogenic, or, at least, as Eliot Slater would put it, "a disorder of the doctor-patient relationship"?[84] Maybe, though it would be more judicious to say that the nineteenth century was hysteria's golden age precisely because it was then that the moral presence of the doctor became normative as never before in regulating intimate lives.
Continuities: Toward Nineteenth-Century Nervousness
As Rousseau showed in the previous chapter, Enlightenment sensibilities were confronted with actions and sufferings not easily compatible with
vaunted paradigms of conduct or classifications of disease. The appearance of such alienation and irrationality has commonly been blamed, by modern countercultural critics, upon the dualistic doctrine of man proclaimed by the new philosophy, above all the Cartesian severed head and divided self, derived from the absolute rule of the cogito in the age of reason.[85] It is possible to take a view more sympathetic to eighteenth-century structures of feeling. The new availability of a plurality of models of living (Christian, civic humanist, individualist, scientific, and so forth) perhaps afforded welcome psychological Lebensraum to those—for instance, members of the newly emergent intelligentsia—who did not fit easily into rigid prescriptions. Dualistic models and multiple prototypes allowed a certain indeterminacy, or psychological je ne sais quoi , to be built into the makeup of modern man, allowing the accommodation of eccentricity and difference.[86]
Such margins of tolerance were sorely needed. For, as the Enlightenment era relaxed religious requirements, it was also applying intenser personal strains. Its exhausting commitment to the life of intelligence, its demand for politeness, and its relentless pressures for self-awareness and-realization, spelled more stressful standards of behavior, and hence highlighted their obverse: abnormality. In the rarefied atmospheres of sophisticated courtliness and brilliant urbanity, the body was required to be disciplined and drilled, yet also displayed. Inner sensibilities had to find expression at the tea table or in the salon through refined, subtle, and often veiled codes of etiquette, revealing but concealing through actions compelled to speak louder than words. The lingua franca for negotiating such repression-expression tensions lay in nervousness, a body language ultra flexible, nuanced, and ambivalent, yet brittle and fitful.
For life lived through the idioms of nervous sensibility carried high risks. Want of nerve betrayed effeminacy; want of nerves , by contrast, exposed plebeian dullness; yet volatile excitability could be too much of a good thing, a lapse of tact, culminating in hysterical crises. A golden mean—poised decorum spiced with idiosyncratic difference—was the goal. Achievement of this hazardous role adjustment, this accommodation between the hypervisible narcissistic individual and a society demanding Chesterfieldian conformism, was perhaps facilitated by precisely that divided Cartesian self so often berated by modern critics. Such a dualism—the man-behind-the-mask playing out the ontology, of the ghost in the machine—allowed a certain distance, a disowning, a usable tension between self and body. Diderot, Sterne, Casanova, and Rousseau all demonstrated, through their lives and writings, the rich potential for
dramatic self-expression afforded to the "new person" by the novel polysemic idioms of impulse, feeling, imagination, nerves, and, ultimately, hysteria.[87]
Enlightenment thinkers professed bafflement at the Sphinxian riddles of psyche/soma affinities. "The action of the mind on the body, and of the body on the mind," noted a leading authority on madness, "after all that has been written, is as little understood, as it is universally felt."[88] This ontological equivocation, this suspension of judgment, surely enhanced that respect with which the post-Sydenham hysteric was treated in a private practice milieu in which, as Nicholas Jewson has stressed, some rough-and-ready parity governed patient/practitioner relationships.[89] Thus, that great clinician, William Heberden, a man utterly au fait with the symptoms, saw hysteria as a condition all too readily provoked by the "slightest affection of the sense or fancy, beginning with some uneasiness of the stomach or bowels." "Hypochondriac men and hysteric women" suffered acidities, wind, and choking, leading to "giddiness, confusion, stupidity, inattention, forgetfulness, and irresolution," all proof that the "animal functions are no longer under proper command."[90] But, a man of his time, he was loath to dogmatize as to the root cause. For,
our great ignorance of the connexion and sympathies of body and mind, and also of the animal powers, which are exerted in a manner not to be explained by the common laws of inanimate matter, makes a great difficulty in the history of all distempers, and particularly of this. For hypochondriac and hysteric complaints seem to belong wholly to these unknown parts of the human composition.[91]
Like most contemporary clinicians, Heberden was prepared to live with the mystery visitor. "I would by no means be understood, by any thing which I have said, to represent the sufferings of hypochondriac and hysteric patients as imaginary; for I doubt not their arising from as real a cause as any other distemper."[92]
In other words, the historical sociology of Enlightenment hysteria is defined by the clinical encounter between the sensitive patient and the sympathetic physician. The ambience was elitist, and it was, in principle at least, unisex. Ridiculing uterine theories of hysteria as anatomical moonshine, Richard Blackmore had concluded that "the Symptoms that disturb the Operations of the Mind and Imagination in Hysterick Women"—and by these symptoms he meant "Fluctuations of Judgment, and swift Turns in forming and reversing of Opinions and Resolutions, Inconstancy, Timidity, Absence of Mind, want of self-determining
power, Inattention, Incogitancy, Diffidence, Suspicion, and an Aptness to take well-meant Things amiss"—these, he insisted, "are the same with those in Hypochondriacal Men."[93] How could an age nailing its colors to the mast of universal reason, a culture whose moral vocabulary turned upon sense and sensibility, define hysteria as the malaise of the mucous membrane?
This clinical rapport forged in the century after Sydenham between fashionable doctor and his moneyed patients did not cease in 1800: far from it. Nineteenth-century medicine presents a Frithian panorama of well-to-do, time-to-kill, twitchy types of both sexes being diagnosed as hysterical, or perhaps by one of its increasingly used euphemistic aliases, such as "neurasthenic,"[94] and being treated, by general practitioners and specialist nerve doctors alike, with a cornucopia of drugs and tonics, moral and behavioral support, indulgence, rest, regimen, and what-you-will—in ways that surely would have won the imprimatur of Samuel Tissot, Theodore Tronchin, or Heberden.[95] Such continuity may show that Victorian medicine failed in its quest for the promised specific for hysteria. But it would be more to the point to emphasize that, from Giorgio Baglivi to George Beard, the canny clinician knew that the hysteric's prime needs were for attention, escape, protection, rest, recuperation, reinforcement—physical, moral, and mental alike. The least plausible indictment against either Mandeville or Weir Mitchell is that they tried to force hysteria onto some Procrustean bed. For them, the protean language of nerves permitted the sufferer to bespeak his or her own hysteria diagnosis as a nonstigmatizing cloak of disorder. It was Mitchell who was wont to speak of "mysteria."[96]
In the nineteenth century, the rest home, clinic, and sanatorium supplemented the spa-resort to provide new recuperative sites for the familiar nervous complaints of the rich. Their therapeutic rationale, however, was old wine in new bottles. Nerve doctors continued to emphasize the force field of the physical, emotional, and intellectual in precipitating hysteria (or, later, neuropathy, neurasthenia, etc.); they defined hysteria, formally at least, as gender nonspecific, independent of gynecological etiology. There was life still in the old Enlightenment idiom of the nerves. Above all, by cushioning neurasthenic patients within a somatizing diagnostics of nervous collapse, nervous debility, gastric weakness, dyspepsia, atonicity, spinal inflammation, migraine, and so forth, fashionable doctors could forestall suspicions that their respectable patients were either half mad or malingering sociopaths.[97]
Not least, "nerves" precluded moral blame, by hinting at a pathology not even primarily personal, but social, a Zeitgeist disease. Eighteenth-
century nerve doctors tended to indict cultural volatility: salon sophisticates were victims of exquisitely vertiginous life-styles that sapped the nerves. By contrast, in later recensions of the diseases of civilization, High Victorian therapists on both sides of the Atlantic pointed accusing fingers at the pitiless competition of market society. As Francis Gosling has shown, George Beard and Weir Mitchell argued that career strains in the business rat race devitalized young achievers; brain-fagged by stress and tension in the cockpit of commerce, they ended up nervous wrecks, their psychological capital overtaxed. Cerebral circuits suffered overload, mental machinery blew fuses, batteries ran down, brains were bankrupted: such metaphors, borrowed from physics and engineering, were reminders that disorders were physical, offering convincing explanations why go-getting all-American Yale graduates like Clifford Beers should suffer nervous breakdowns no less than their delicate and devoted sisters.[98]
Such decorous somatizing also permitted physicians to exhibit dazzling therapeutic machineries, targeted at bodily recuperation: baths and douches, passive "exercise," massage, custom-built diets programmed to make weight, fat, and blood; regimes of walking, games, and gym; occupational therapy, water treatments, electrical stimuli, relaxation, routine, and so forth. This paraphernalia of remedial technologies obviously spelled good business for residential clinical directors. Strategically, such routines were said to benefit patients by deflecting them from morbid self-awareness, training attention more beneficially elsewhere.
For nineteenth-century physicians began to voice fears of morbid introspection, that hysterical spiral arising from patients dwelling upon their disorders.[99] Precepts for healthy living widely canvassed—by sages such as John Stuart Mill and Thomas Carlyle no less than medical gurus—deplored egoistic preoccupation as the road to ruin, to suicide even, and advised consciousness-obliterating, outgoing activity.[100] For the hysteric was typically regarded as the narcissist or introvert. From her Freudian viewpoint, Veith has blamed Weir Mitchell for not encouraging his rest-cure convalescents to talk their psychosexual problems through, implying that this silence may have been due to prudery. One suspects, in truth, the doctor's reticence reflects neither puritanism nor shallowness, but savvy: a conviction that some matters were better left latent, lest they inflame morbid tendencies.[101]
"Only when bodily functions are deranged," warned the mid-Victorian British physician Bevan Lewis, do "we become . . . conscious of the existence of our organs."[102] In his caution about consciousness, Lewis was of a mind with the leaders of British practice—Charles Mercier,
David Skae, Henry Maudsley, and Thomas Clouston—who saw hysteria as the penalty for excessive introspection, especially when accompanied by a- or anti-social dispositions and, worse still, by auto-erotism.[103] It was, consequentially, dangerous to discuss such dispositions freely with patients, lest this encourage further morbid egoism and attention-seeking, and all the attendant train of self-absorption, daydreaming, reverie, and solitary and sedentary habits. Prompted to dwell upon herself, Maudsley feared, the hysteric would most likely sink into solipsistic moral insanity or imbecility;[104] for, as the patient progressively abandoned her power of will—"a characteristic symptom of hysteria in all its protean forms"—she would fall into "moral perversion," losing
more and more of her energy and self-control, becoming capriciously fanciful about her health, imagining or feigning strange diseases, and keeping up the delusion or the imposture with a pertinacity that might seem incredible, getting more and more impatient of the advice and interference of others, and indifferent to the interests and duties of her position.[105]
For their own sakes, therefore, patients must be taken "out of themselves"—through therapeutic hobbies, exercise, and sociability. Thus Sir William Bradshaw, the society physician in Virginia Woolf's Mrs. Dalloway , notoriously instructs the shell-shocked war victim Septimus Smith to pull himself together and cultivate a sense of proportion. Through the caricature of this pompous ass, Woolf expressed her contempt for such London physicians as Sir George Savage and Maurice Craig, who treated her own nervous collapses with the moral anodyne of the rest cure. Yet Woolf herself was no less scathing, in a terribly English way, about the asininities of sex-on-the-brain Germanic psychiatrists. There is no sign that she favored having Freudian "mind doctors" open Freud-ian windows onto her psyche.[106]
In short, powerful currents through the nineteenth century and beyond continued to class hysteria as a disease of nervous organization. Doctors fixed upon physical symptoms, and treated them with physical means, steering clear of too much skirmishing with, or stirring up, the mind. If blinkered and complacent, such approaches were not necessarily obtuse. The contrasting protocols of Charcot's Tuesday Clinic[107] and the Freudian couch arguably hysterized hysteria, as one might douse a fire with gasoline. Yet if continuities with the Enlightenment may be seen, there are gear shifts too; above all, perhaps, a certain waning of medical sympathy for the nervous hysteric in the generations after 1800, thanks to a sterner Evangelical prizing of self-reliance.[108] If the Enlightenment indulged a certain fascination for idiosyncracy, Victorian
mores took their stand against the egoistic sociopath. To these sociopaths we turn.
Change: Women, Body, and Scientific Medicine
Concentrating on continuities with the past risks skewing nineteenth-century outlooks on hysteria. It was, all agree, hysteria's belle epoque , thanks above all to the startling emergence and convergence of mutually reinforcing conditions: a profound accentuation of the "woman question," coterminous with an evidently not unrelated expansion in organized medicine.
As Elaine Showalter fully explores in chapter 4, the question of feminine nature became a burning issue. Romanticism rang the changes on the paradoxes: wife and whore, femme fragile and femme fatale , weak but wanton—woman, it seemed, was an appallingly irresistible cocktail of innocence and morbid sexuality.[109] Bram Dijkstra, among others, has traced the sensationalization of that mythology toward the turn of the century.[110] In the shadow of such stereotypes, women experienced profound conflicts over rival ideals and expectations.[111] To hook a husband, a woman had to be childlike and dependent, yet also a tower of strength as the household manager of that great moral engine, the family, and robust enough to survive innumerable pregnancies. Wives had to be pure, yet pleasing, or risk being supplanted by the "other woman." Hence they had to develop their talents, yet intellectual aspirations were censured as unnatural, imperiling their manifest biological destiny as willing wombs. And if, stupefied by such pressures, paradoxes, and prohibitions, women showed signs of bewilderment or bridling, what did this prove but that they were spoiled, difficult, and capricious, further proof of the necessity for male and medical control? When proto-feminist protest mounted, it gave further evidence to those who saw hysteria as the root of all female activism. History, anatomy, destiny, evolution—all were conscripted to clamp women in their place.[112]
And so, of course, as fine feminist scholarship has shown, was medicine.[113] Yet the medical profession itself was in the toils of traumatic transformation. Space limits here preclude any adequate exploration of the upheavals in the internal organization and public facade of medicine during the nineteenth century, but a few developments must be mentioned, playing as they did key parts in reshaping hysteria.
Amid the throng of professional groups competing for recognition and rewards, medicine contributed noisily to the clangor, frantically asserting its own unique vocation. Doctors sought fighter professional orga-
nization and public privileges. Teaching and research assumed greater institutionalization in university and laboratory. And, thanks to such developments, medical discourse became increasingly directed to professional peers. With new ladders of advancement, and the expansion of research schools and scientific circles, professional esprit de corps grew commensurably, entailing a certain displacement of the patient, who was increasingly downgraded to an object of "the medical gaze." All such changes had, as we shall see, profound implications for the hysteric.[114]
Overpopulated, insecure, but ambitious, medicine fractured into a proliferation of subdisciplines, with new specialties multiplying and vying for funds and fame. As Ornella Moscucci has demonstrated, obstetrics and gynecology pioneered identities of their own, staking out the new terrain of women's medicine. Neurology took shape as a specialty; Russell Maulitz has traced the rise of pathology. Public health came of age, and alliances between the social sciences and the emergent specialties of organic chemistry and bacteriology helped to forge modern epidemiology. Psychiatry blossomed, colonizing its own locations, above all, the asylum and the university polyclinic.[115]
And all such heightened division of labor led to different schools, national groups, and subspecialisms vaunting their own cognitive claims: in some cases, basic science, in others, clinical experience or laboratory experimentation, keyed to the microscope. L. S. Jacyna has stressed the espousal by professional medics of ideologies of scientific naturalism, centered on the laws of life.[116]
Nineteenth-century medicine reoriented itself beyond the sickbed into the clinic: the vast, investigative teaching hospital, equipped with advanced patho-anatomical facilities and a never-failing supply of experimental subjects. At the same time, with the emergence of the industrial state, medicine also found itself enjoying greater interaction with sociopolitical institutions. Examining vast disease populations in their new public capacity, physicians had to confront fresh questions: latency, disposition, contagion, diathesis, constitution, and inheritance.[117]
In short, scientific medicine flexed its muscles and spread its wings. It was courted by the public; it craved official authorization. Hence, doctors made bold to become scientific policymakers for the new age. The questions they addressed—matters of hygiene, efficiency, sanity, race, sexuality, morality, criminal liability, and so forth—were inevitably morally charged; many physicians claimed medicine as the very cornerstone of public morals. And so physicians shouldered an ever greater regulatory role, acting as brokers and adjudicators for state, judiciary, and the family. Turning technical expertise into social and moral directives,
medicine spoke out upon social order and social pathology, progress, and degeneration. As will now be seen, new medical specialties claimed jurisdiction over hysteria, and made it yield moral messages to slake, or stoke, Victorian anxieties.[118]
Problem Women: Gynecology and Hysteria
As Thomas Laqueur has contended, research in the late eighteenth and early nineteenth centuries into human sexuality did not resolve the mystery of woman, but deepened it. The more that was discovered, however tentatively and tardily, about menstruation and conception, the more medical science confirmed the truth that hegemonic male culture was independently affirming: women were different .[119] Traditional Greek-derived biomedical teachings had represented the female reproductive apparatus as an inferior, imperfect inversion of the male. But during the eighteenth century and beyond, medicine and culture were abandoning that view and combining to reconstruct women as radically other .[120] And not merely other, but bizarre.
It had become acknowledged that, contradicting medical teachings going back to Hippocrates, female orgasm was unnecessary for conception. Investigations into ovulation also appeared to show that menstruation in women, unlike other mammals, occurred independently of libidinal excitation. In short, the relationship between erotic stimulus on the one hand, and conception on the other, became utterly (and uniquely) problematic. Female sexuality thus seemed, from the viewpoint of research into generation, a mystery, apparently biologically superfluous, and perhaps even pathological.[121]
Pontificating upon the riddles of female sexuality became the stock-in-trade of emergent gynecology. Elbowing aside "ignorant midwives" and the much-mocked accoucheurs , specialist surgeon-gynecologists made their bid to pass themselves off as more than mere operators: being rather experts, qualified to hold forth on the overpowering role of reproduction in determining female life patterns, in a set of scientific discourses in which womb became a synecdoche for woman.[122] Nineteenth-century medicine, claimed Foucault, forged a new hysterization of women's bodies. This was precisely the achievement of gynecology, largely backed by the equally junior disciplines of sexology and psychological medicine, against the backdrop, just sketched, of the establishment of specialized, scientific medicine.[123]
In a context of patriarchal values ultra-suspicious of female sexuality,[124] gynecologists set about designating the physiology and pathology
of this perplexing being. Once the chasm between arousal and conception had been established, female libido—so volatile, capricious, even rampaging—was revealed as inherently dysfunctional, dangerous even. So why the peculiar sensitivities of clitoris and vagina, all too susceptible to physiological and emotional disturbance? Was not even the uterus itself troublesome beyond the demands of childbearing? Were not women enslaved by their generative organs? And if so, what was to be done? Confronted with streams of female patients—many tortured with internal pain, others dejected, still others "delinquent"—these were the problems upon which the growing corps of women's disease specialists built their platform.
The answers offered by emergent gynecology portrayed women's health as desperately womb-dependent. Since the very raison d'être of the female lay in procreation,[125] properly directed thereto, erotic arousal had a certain value, within the walled garden of matrimony. Yet what of the risk of arousal among adolescent girls, spinsters, and widows? Abstinence was socially expected, yet continence had its quandaries, leading to chlorosis, wasting conditions, and emotional waywardness.[126] Frustration fueled fantasies and could lead to masturbation, an activity imperiling health—physical, moral, and mental.[127] In short, the female reproductive system was so precariously poised that almost any irregularity, whether excitation or repression, was sure to provoke hysteriform disorders.
Hysteria had ever been regarded as the charade of disease.[128] Now doctors feared it as eros in disguise. Its swoonings, jerks, convulsions, and panting blatantly simulated sexuality, affording surrogate outlets and relief, while the sufferer escaped the stigma of lubricity. Not least, in the throes of a fit, the hysteric was bound to be touched, pampered, and subjected to medical examination and treatment, all of which nineteenth-century doctors regarded as erotically gratifying.[129]
Gynecology and psychophysiology thus joined forces to make female sexuality problematic, highlighting the role of the sexual organs in provoking hysterical conditions widely believed to precipitate moral insanity. "Convulsions . . . in early life," judged the top late Victorian psychiatrist, Henry Maudsley, were indices of the "insane temperament," even in subjects not yet actually insane.[130] Such precocious, displaced eroticism could trigger long-term disturbances.
Early in the century, psychiatrists had pinpointed the links between menstrual abnormalities and hysteria. John Haslam, apothecary at Bethlem Hospital, observed that in "females who become insane, the disease is often connected with the peculiarities of their sex."[131] In a similar
vein, the influential psychiatric spokesman, George Man Burrows, drew attention to "various sanguiferous discharges, whether periodical, occasional, or accidental," all of which "greatly influence the functions of the mind."[132] Herein, argued Burrows, lay the key to female troubles, for "every body of the least experience must be sensible of the influence of menstruation on the operations of the mind"—it was, he judged, no less than the "moral and physical barometer of the female constitution."[133] Burrows tendered a physiological explanation based upon "the due equilibrium of the vascular and nervous systems":
If the balance be disturbed, so likewise will be the uterine action and periodical discharge; though it does not follow that the mind always sympathises with its irregularities so as to disturb the cerebral functions. Yet the functions of the brain are so intimately connected with the uterine system, that the interruption of any one process which the latter has to perform in the human economy may implicate the former.[134]
Ripeness for childbearing was the mark of the healthy woman. Hence, Burrows emphasized, were menstruation interrupted, "the seeds of various disorders are sown; and especially where any predisposition obtains, the hazard of insanity is imminent."[135]
Equally, he judged, local genital and uterine irritations would generate "those phantasies called longings, which are decided perversions or aberrations of the judgment, though perhaps the simplest modifications of intellectual derangement."[136] What was the explanation?
These anomalous feelings have been referred to uterine irritation from mere gravitation, and so they may be; but they first induce a greater determination of blood to the uterus and its contents, and then to the brain, through the reciprocal connexion and action existing between the two organs.[137]
It was two-way traffic. Amenorrhea was sometimes "a cause of insanity,"[138] but, reciprocally, "cerebral disturbance" could itself cause "menstrual obstruction,"[139] further exacerbating mental disorder, for "terror, the sudden application of cold, etc., have occasioned the instant cessation of the menses, upon which severe cerebral affections, or instant insanity, has supervened."[140]
In line with the times, Burrows also blamed menopause for severe female disturbance. Once again, he emphasized, the primary change was physiological:
The whole economy of the constitution at that epoch again undergoes a revolution. . . . There is neither so much vital nor mental energy to resist
the effects of the various adverse circumstances which it is the lot of most to meet with in the interval between puberty and the critical period.[141]
Yet, in the opinion of the less-than-gallant Burrows, sociopsychological forces were also at work:
The age of pleasing in all females is then past, though in many the desire to please is not the less lively. The exterior alone loses its attractions, but vanity preserves its pretensions. It is now especially that jealousy exerts its empire, and becomes very often a cause of delirium. Many, too, at this epoch imbibe very enthusiastic religious notions; but more have recourse to the stimulus of strong cordials to allay the uneasy and nervous sensations peculiar to this time of life, and thus produce a degree of excitation equally dangerous to the equanimity of the moral feelings and mental faculties.[142]
Double jeopardy surrounded the menopausal crisis.
Overall, Burrows judged hysteria intrinsic to the female sexual constitution: "Nervous susceptible women between puberty and thirty years of age, and clearly the single more so than the married, are most frequently visited by hysteria."[143] Its root, he emphasized, was organic: "Such constitutions have always a greater aptitude to strong mental emotions, which, on repetition, will superinduce mental derangement, or perhaps epilepsy."[144]
Unlike Enlightenment physicians, though prefiguring later Victorian opinion, Burrows feared hysteria, because it was always liable to flare into a dangerous, even incurable, condition. "Delirium is a common symptom of hysteria," he warned, "and this symptom is prolonged some-times beyond the removal of the spasm of paroxysm."[145] Thus, in the event of a repetition of hysterical fits, "the brain at length retained the morbid action, and insanity is developed." Indeed, because "hysteria is of that class of maladies which, wherever it is manifested, betrays a maniacal diathesis," it followed that "habitual hysteria clearly approximates to insanity."[146]
This prognosis (uterine disturbances lead to hysterical conditions that precipitate insanity proper) became standard to nineteenth-century medicine. "The reproductive organs . . . when unduly, unseasonably, or exorbitantly excited," argued Alfred Beaumont Maddock, are not only "necessarily subject to the usual advent of those physical diseases which are the inheritance of frail humanity, but are also closely interwoven with erratic and disordered intellectual, as well as moral, manifestations."[147] Such female disorders were, Maddock judged, the direct result of "the peculiar destiny that [woman] is intended by nature to fulfil, as
the future mother of the human race."[148] Others concurred. "Mental derangement frequently occurs in young females from Amenorrhoea," argued John Millar, "especially in those who have any strong hereditary predisposition to insanity."[149]
This "Hysteric's Progress," arcing almost literally from womb to tomb, was evoked most vividly by that gloomy giant of late Victorian psychiatry, Henry Maudsley. Maudsley traced the slippery slope from hysteria to "hysterical insanity," a "special variety" of the complaint connoting
an attack of acute maniacal excitement, with great restlessness, rapid and disconnected but not entirely incoherent conversation, sometimes tending to the erotic or obscene, evidently without abolition of consciousness; [and also] laughing, singing, or rhyming, and perverseness of conduct, which is still more or less coherent and seemingly wilful.[150]
Such disturbances "may occur in connection with, or instead of, the usual hysterical convulsions," although, Maudsley warned, "the ordinary hysterical symptoms may pass by degrees into chronic insanity."[151] Gynecological and psychiatric causes were virtually inseparable: "Outbursts of temper become almost outbreaks of mania, particularly at the menstrual periods. An erotic tinge may be observable in her manner of behaviour; and occasionally there are quasi-ecstatic or cataleptic states."[152]
Such conditions, emphasized the highly materialist Maudsley, were "the effect of some condition of the reproductive organs on the brain." Their cerebral fibers warped, sufferers would not hesitate to exploit their self-dramatizing potential, Maudsley admonished, pointing to the "extreme moral perversion shown by such hysterical young women of a nervous temperament as imagine that their limbs are paralysed and lie in bed or on a couch day after day."[153] There was, however, a moral sting in the tail of Maudsley's materialism. Like most of his cloth, he judged that the optimum treatment for young ladies in this "extremely perverted moral state" was moral, requiring that "the patient be removed in time from the anxious but hurtful sympathies and attentions of her family, and placed under good moral control." If, instead, "it be allowed to go on unchecked, it will end in dementia, and it is especially apt to do so when there is a marked hereditary predisposition."[154] Not surprisingly, Maudsley linked hysterical insanity to nymphomania, both following from "the irritation of the ovaries or uterus."[155]
Such anxiety-making, misogynistic views—singling out women and blaming the uterus—were no peculiarity of the English. The eminent German psychiatrist Wilhelm Griesinger identified hysteria as symptomatic of local disorders of the uterus, ovaries, and vagina.[156] Like his
English counterparts, Griesinger espoused a doctrinaire medical materialism in which bio-reality was definitionally somatic, and phenomena apparently without bodily correlates were to be presumed imaginary. Female hysteria, he disclosed in his Mental Pathology and Therapeutics (1845), was thus either the product of genital disease or a work of art. Authentic hysteria was somatic, involving the "morbid action of . . . the brain,"[157] generally provoked by vaginally seated erotic stimulus, itself in turn sparked by menstrual pain and irregularities, constrictions and stoppages, and exacerbated by habitual masturbation. But hysteria was often faked—a characteristic foible of a sex whose entire demeanor was pockmarked by dishonesty, deceitfulness, and emotional waywardness. Griesinger's "reversion to a somatic explanation for hysterical disturbances," judged Veith, "must be looked upon as a regression from the psychiatric concepts of Pinel and Feuchtersleben," above all because he had a "blind spot" for women's sexual frustration.[158]
Thus the new sciences of gynecology and psychological medicine provided twin pillars supporting the rehabilitation of uterine theories of hysteria that became so prominent throughout the nineteenth century. These led in turn, with growing frequency, as Jeffrey Masson has amply documented, to surgical interventions, including the practice of hysterectomy and ovariectomy and the occasional resort to clitoridectomy or cauterization by figures such as Baker Brown and Alfred Hegar, touted as radical solutions to mental disorders no less than to local infections. It was not unknown, Ornella Moscucci has shown, for English surgeons to recommend genital operations for preventive psychiatric purposes.[159] Against the backdrop of the "woman problem," aggressive medicalization thus reinstated, in new guise, the uterine pathology theory, both regendering and re-eroticizing the condition.
Neurology and Hysteria
Enlightenment scientific medicine classed as "nervous" those protean behavioral disorders, floating free of determinate lesions, which it termed the vapors and spleen, hysteria, hypochondria, and melancholy. Assimilating hysteria by this verbal sleight of hand to one of the major organic systems proved strategically adroit, allowing the incorporation of the anomalous within prestigious, systematizing, and bodily anchored disease schemata.
Neurological models proved equally fruitful in the nineteenth century, in context of the special diagnostic and bureaucratic needs of the public hospital and the mammoth mental asylum.[160] Institutional medi-
cine had the burden of processing—and the benefit of studying—an infinitely wider range of morbid conditions than ever before encountered close up and en masse: chronic, progressive, and degenerative disorders, above all. Hospital medicine, on the Paris model, took advantage of the unique availability of poor patients for observation, experiment, and postmortem investigation. Diagnostic acumen, therapeutic nihilism, and patho-anatomical expertise combined to lay bare a host of degenerative disorders.[161] The asylum likewise provided unparalleled opportunities for long-term surveillance (and subsequent autopsy) of epilepsy, dementia, general paresis, speech and gait defects; of what would eventually be identified as multiple sclerosis; of Parkinson's disease, Huntingdon's chorea, cerebral palsy, and a host of other hitherto little-tracked sensorimotor disturbances. Such conditions, many feared, were spreading; they certainly afflicted a hard core of patients in nineteenth-century public institutions, workhouses, and infirmaries, and the "back wards" and chronic and incurable wings of Europe's and North America's mush-rooming lunatic asylums.
Though typically defying not just cure but even anatomical localization, such conditions at least squared with a popular and plausible comprehensive sickness scenario, whose parameters were nature and history: degeneration.[162] Disorders otherwise baffling to science were increasingly normalized by being termed constitutional, hereditary, and degenerative. In the absence of tangible lesions, even postmortem, the individual's pedigree, the family history, became, as it were, a display of lesions dredged up from the past: the generational deterioration, for instance, from alcoholic great grandparents, through a nymphomaniacal prostitute of a grandmother, to a hysterical mother, and finally perhaps to an epileptic child. Such genealogical declensions apparently laid the disease affinities bare.
It is against this wider degenerationist backdrop, and in context of the drive to translate intractable disorders into neurology through deploying the patho-anatomical methods pioneered in the clinic, that the career of Jean-Martin Charcot assumes such monumental importance in framing yet another paradigm of hysteria. Historians have rightly drawn attention to the great professor's exercise of Svengalian authority over his female patients.[163] Yet something far more complex was going on. The hysteria that Charcot studied—or, better perhaps, that he and his patients co-produced—was a palimpsest of a performance, many layered with meanings. It bespeaks the utter docility of the body, under the charismatic authority of mind (above all, the robot behavior of the hypnotized). It marks deflected, oblique protest—a resistance that, incapa-
ble of verbalization, was converted into somatic signals of violence and burlesque.[164] It may also be read as duplicitous seduction: were not the patients, or their diseases, duping the scientistic, voyeuristic doctors, thereby ironically confirming—had Charcot only known!—fin de siècle medicine's conviction of the pathognomy of the feminine, and insensibly ratifying male phobias about woman as the femme fatale?
These are just some of the facets of gender politics in Charcotian hysteria, further dissected in chapter 4 by Elaine Showalter. Against such a background, a different aspect also deserves emphasis: Charcot's burning desire to make hysteria reputable, distinguished even, within the somatizing enterprise of scientific medicine. As Trillat and Micale have emphasized, despite his location at the Salpêtrière, Charcot never was, nor aspired to be, a psychiatrist or alienist in the great tradition of Pinel and Esquirol.[165] He was an ardent neurologist, committed to the techniques of pathological anatomy, proud to hold a Clinical Chair of the Nervous System. He aimed to reduce neurological chaos, hysteria included, to order. He was faced with fiendishly complex symptom clusters. Such conditions as "epilepsy, hysteria, even the most inveterate cases, chorea, and many other morbid states . . . come to us like so many Sphynx," he confessed, defying "the most penetrating anatomical investigations." For precisely that reason, he observed, sceptics urged that hysteria "should be banished to the category of the unknown."[166] Not so! His ambition, initially at least, was to pin down nervous phenomena to organic lesions, and thereby to bring regular system to general paralysis, neuralgias, seizures, epileptiform fits, spastic symptoms, tabes dorsalis, and, not least, hysteria.[167]
And in attempting this Herculean labor, far from focusing exclusively upon a troupe of star hysterics, Charcot aimed to show that hysteria partook of the characteristics of neurological disorders as a whole, dispersed among the community at large. He thus took pride in his demonstrations that hysteria visited males as well as females, parents and children alike, a galaxy of ethnic groups, and, above all, the whole social spectrum.[168] With hysteria, the more it was universal, the surer the grounding for its "scientificity."
Addressing thus the range of its manifestations, Charcot's project was committed to massive clinical scrutiny of hysterical pathology—motor and sensory symptoms, bizarre visual abnormalities, tics, migraine, epileptiform seizures, somnambulism, hallucinations, word blindness, alexia, aphasia, mutism, contractures, hyperaesthesias, and numerous other deficits—devising critical experiments (e.g., upon eyesight and hearing peculiarities), refining comparison and measurement, and com-
piling lavish and multigenerational patient histories.[169] The contented positivist could leave no variable unturned.
Charcot had some measure of success in mapping hysteria onto the body. He was delighted to discover, for instance, hysterogenic points, zones of hypersensitivity which, when fingered, provoked an attack, analogous perhaps to the pressing of an electric light switch. Such a discovery confirmed his conviction of the reality of "latent hysteria."[170] Yet his early faith that scientific investigation into hysteria would systematically reveal demonstrable neurological substrates increasingly proved a forlorn—or, at least, a premature—hope.
By consequence, Charcot found he needed to satisfy himself with an epiphenomenalist account of the regularities and laws of hysteria, derived from its manifestations. Characteristically, he couched his praise for his predecessor, Pierre Briquet, in just these terms; Briquet's achievement lay in having shown that "hysteria is governed, in the same way as other morbid conditions, by rule and laws, which attentive and sufficiently numerous observations always permit us to establish."[171] Building thereupon, Charcot thus claimed to have established the series or stages of manifestations, from petite hystérie through hystérie ordinaire up to the grande attaque d'hystéro-epileptique . In this way clinical observations permitted the uncovering, he claimed, of the natural histories of extended families of related deficits: hemilateral anesthesias, pharyngeal anesthesias, grandes paroxysmes , palpitations, chorea, Saint Vitus dance, tertiary neurosyphilitic infections, and temporal lobe epilepsy. If Sydenham had seen hysteria as the exception to the natural history of diseases, the positivist Charcot, by contrast, believed he could incorporate it within such a taxonomy. "These diseases," he insisted, "do not form, in pathology, a class apart, governed by other physiological laws than the common ones."[172]
It is this passion to illuminate hysteria's hidden disposition, its diatheses and frequencies, that explains Charcot's lasting passion for hypnosis and his brief encounter with metalloscopy. Hypnosis served Char-cot as a kind of litmus test. It became an article of faith with him that the capacity to be hypnotized was a crucial experimental demonstration of underlying, organic, hysterical pathology. Hypnosis was the dowser's twig, pointing to the reservoir of the pathological; hence his eagerness to discredit Hippolyte Bernheim's view that hypnotic states were normal and potentially universal. For Charcot, hypnotizability was the giveaway of the pathological.[173]
For similar reasons, as Anne Harrington has demonstrated, Char-cot's circle became fascinated by Victor Jean-Marie Burq's metalloscopic
experiments. Burq claimed that distinct metals, each possessed of its own force neurique , had the power, when brought close to a subject, to modify behavior. Indeed, the bio-magnetist Burq even appeared to have the capacity, through deploying rods of diverse alloys, to transfer hypnotic and hysteric conditions from organ to organ, and from individual to individual, depending upon their "metallic personality." Burq's neo-Mesmeric use of rods offered further confirmation to the credulous Charcot (in a manner echoing Mesmer himself) that hysteria and its kindred nervous conditions derived from authentic, if ill-understood, organic substrates, being subject to the universal physical laws governing the atomic structures of different metals. Manipulation of mood by the manipulation of metals showed the very laws of cause and effect at work, no less clearly than using magnets to make iron filings dance. In drawing upon Burq, the charcoterie (group of disciples of Charcot) thus further hitched its wagon to the rising star of late-nineteenth-century physics, with its prestigious doctrines of ethers and quasi-occult energy sources.[174]
How then do we appraise Charcot's characterization of hysteria? It was clearly in part the product of the interprofessional rivalries of medicoscientific specialisms discussed earlier. In championing physiological methods to plot hysteria onto the body, Charcot was planting patho-anatomy's flag on a condition contested by alienists and clinicians, gynecologists and obstetricians. Charcot never approached hysterical patients from the standpoints of psychiatry or psychology. His investigative techniques remained largely indifferent to the probing of their consciousness.[175] Why?
Institutional ensconcement in the "living pathological museum" of the Salpêtrière[176] and staunch Third Republic positivism confirmed in Char-cot a concept of science which gave priority to establishing the laws of life, grounded in the totality of the living organism. Hence he set consciousness to one side as essentially secondary. Of course, he had no doubt that hysteria attacks were commonly sparked by mental and emotional trauma, albeit, naturally, in individuals already endowed with a hysterical constitutional diathesis. And, equally, he had to put his patients' minds to the test in critical experiments, to winkle out malingerers and self-publicists: his pneumograph machine, for example, gave graphic proof that, unlike a genuine cataleptic, a bogus cataleptic will register fatigue. Hindsight reveals the deep pathos in Charcot's boast that the "province of the physician" is "to dissipate chicanery."[177]
But overall, Charcot—unlike certain of his protégés such as Janet[178] —showed scant professional interest in what were then being called the
psychology or psychodynamics of the patients he used for experimental and pedagogical purposes. This was partly the result of circumstances. It is likely, after all, that Charcot's main face-to-face contact with such patients lay in clinical demonstrations, his assistants and students having been delegated to subject them to prior personal examination. Charcot was thereby probably the unwitting victim of both doctor and patient compliance, yes-people all in his Napoleonic empire. In any case, his Tuesday Clinic subjects were but working-class Parisian girls. Would a Charcot consider it scientifically fruitful to interrogate such riffraff personally? (For the sake of his illusions, it was perhaps just as well that he didn't.) One wonders whether Charcot used identical, that is, neurological, approaches on his private patients: it was certainly his contention that, in hysteria, "everything follows definite rules—always the same, whether the case is met with in private or hospital practice."[179] Charcot the public figure, the institutional man, and champion of the discipline of neuropathology, was wholly wedded to the positive scientific pursuit of hysteria as a pathology of the constitution. We know all too little of how far the public Charcot also had a double, one prepared to elaborate on the more psychological perspectives implied by his notorious aside, "C'est toujours la chose génitale "—a remark reestablishing precisely that link between hysteria and lubricity which he habitually denied.[180]
Charcot played the scientist, an epiphenomenalist insistent that hysteria was a function of the body. Science's point of entry lay not in psychology but in physiological stigmata, reinforced by degenerationist neuropathy ("contracture diathesis" or "latent hysteria"). "Neuropathic heredity," he believed, "figures conspicuously in the etiology of hysteria,"[181] for "hysteria is often hereditary."[182] Hysteria, of course, had its emotional correlates (attention seeking, coquettishness, lying), but these were chiefly by-products, symptomatic of more basic psychophysiological defects embedded in bodies over the generations.[183]
Hysteria, Psychiatry, and the Clinical Encounter
Nineteenth-century transformations in medicine and society produced their reconceptualizations of hysteria. Gynecology and psychological medicine interacted to represent hysteria as a woman's disease, stemming from the reproductive system and generating an emotional pathology. By contrast, the patho-anatomical gaze of hospital medicine imagined a hysteria that was unisex and indexed by multiple behavioral irregularities that were deemed ultimately neuro-physiological. In this
highly schematic account, a third and final initiative remains to be discussed: the development of a psychological theory of hysteria.
The intellectual roots of this approach lie in lunatic asylum reform around the turn of the nineteenth century. Leading asylum superintendents, particularly Chiarugi, Pinel, Johann Reil, and the Tukes (William and Samuel), repudiated traditional organic nosologies and medical therapeutics as misconceived and inefficacious, urging instead techniques of moral management and moral therapy. Within their theories, insanity was redefined as springing from consciousness—the intellect and the passions—thus necessitating treatment on psychological principles, by appeals to reason, humanity, and the feelings (fear and esteem, pleasure and pain, etc.). Herein lay the founding of psychiatry. Being chiefly concerned with desperate asylum cases, such authors naturally had rather little to say about hysteria per se. But their vision of an authentic secular psychopathology later proved a source of inspiration and authority.[184]
Psychological theories of hysteria were developed by doctors active in bourgeois private practice. This should come as no surprise. Such practices necessitated protracted and intimate contact with patients, women above all, who—whatever their actual medical histories—were utterly au fait with the power possessed by sickness and invalidism to secure respite or leverage within the politics of the family. The culture of sensibility, particularly among those on whose hands time hung heavily, encouraged hypersensitivity to malaise. Bourgeois sufferers were both introspective and vocal in their complaints, rationalizations, and demands. Little wonder that the affinity between hysterical symptoms and the outpourings of consciousness might be thought to stare physicians in the face.
I have argued earlier that doctors typically refused this association. Theirs was a mental set which, by professional article of faith, and almost by way of reflex, equated sickness with the somatic. Many chose, as suggested above, for their patients' peace of mind, surreptitiously to translate complaints into somatic ailments (nervous stomach, and so forth), believing this recourse optimal, for all concerned, for negotiating tricky conditions. A few, however, broke out of this convention, perhaps this pious fraud. Why this happened in the particular case is generally impossible to decipher. The consequences were, however, quite radical: translating hysteria into a malady of the mind drastically changed the rules of the game. It typically reduced hysteria from a disease into a deceit; exculpation turned to indictment; and a darker psychopathology emerged of the pretend hysteric, almost without exception female. Hys-
teria as the disease-mimicking disease made way for the hysteric as the woman (or the woman's unconscious ) pretending to be ill.
These moves appear most starkly in the writings of Robert Carter, a man praised by Veith for his "clear insight into the psychopathology of hysteria" and his "advanced" discovery of sexual etiology.[185] Carter was a young general practitioner in the leafy London suburb of Leytonstone when he published his On the Pathology and Treatment of Hysteria in 1853.[186] In it, he reviewed all available somatic theories of the condition—Cullen's and Pinel's view that it was a morbid condition of the uterine nerves; Cheyne's and Caleb Parry's indictment of the stomach; Highmore's claim that it was consequent upon lung and heart congestion; the notion, associated with Whytt, Tissot, Boerhaave, and Boissier de Sauvages, that it was a disease of the nervous system; Willis's theory, revived by Etienne Georget, that it was a morbid condition of the brain; Gerard Van Swieten's "morbid condition of the spinal cord," and so forth. All without exception he judged as lacking authenticated foundation; for "the disease itself is too shifting and variable to depend upon any definite change in any individual organ."[187] Above all, attempts to ground hysteria in "irritation of the uterus and ovaria [were] . . . utterly untenable"—indeed, merely circular.[188] Hysteria, in short, was not somatic at all, but psychological: "The emotional doctrine affords an easy and complete solution of the difficulty." Indeed, its etiology lay specifically in "the sexual feelings," these being "both more universal and more constantly concealed than any others."[189]
What was the mechanism of the psychological theory of hysteria? Drawing upon the writings of W. B. Carpenter, Thomas Laycock, and other British psychophysiologists, he explained that, within the regular self-adjusting system of the metabolism, strong emotions (fear, joy, etc.) should properly find healthy outlet in physical release such as tears, laughter, flight, and so on. Obviously, central among the emotions were the sexual passions. Ideally these found natural fulfillment in erotic activity, ultimately in orgasm. Discharging such desires rarely posed problems for males.[190]
In modern civilization, however, the double standard commonly denied such relief to women—a result of high moral expectations and the "habitual restraint" imposed upon ladies by respectability. Denied the "safety valve"[191] of such direct, physiological outlets, women were forced to bottle up their amatory longings and suffer what Carter called repression. Intense personal crises (e.g., a broken engagement) could easily cause that dam to burst, however, whereupon indirect tension release was unintentionally gained in hysteria—expressed in outbreaks of un-
controllable sobbing, shaking, fits, temper, and the like. Such hysteria—"a disease starting with a convulsive paroxysm"[192] —Carter called "primary"; it was, in a sense, a spontaneous compensatory mechanism designed to make the best of a bad situation. Some salutary tension-discharge was at least achieved, and eventually the sobbing or tantrum would play itself out and calm would be restored. Primary hysteria of this kind did not require the physician's services.
Hysteria did not stop there, however. For unfortunately, "the suggested or spontaneous remembrance of the emotions"[193] attending the primary fit could easily provoke further attacks, which Carter dubbed "secondary hysteria." Sufferers, relatives, and doctors alike could help forestall such secondary attacks by providing appropriate distractions. Such prevention was prudent, for patients quickly habituated themselves to secondary hysteria, finding it provided them with compensatory pleasures—not least, attention.
Worse, such indirect gratifications readily deteriorated into "tertiary hysteria," which Carter defined as a condition "designedly excited by the patient herself through the instrumentality of voluntary recollection, and with perfect knowledge of her own power to produce them."[194] In short, tertiary hysteria—Carter's prime concern—was an ego-trip, mobilized by the patient's will, for tyrannizing others. The tertiary hysteric, in Carter's view, had thus sunk to appalling depths of moral depravity, contriving to manipulate all around her, so as to gratify her whims and domineering spirit, and enable her to bask in the "fuss and parade of illness."[195] Because this exercise of will was wholly camouflaged in somatic expressions, it naturally compelled sympathy (the patient, after all, appeared dramatically sick), without risking suspicions of shamming. The greater the sympathy it won, the more tyrannical it became. Hysterics grew expert in their art. Thus, to create an effect, Carter noted, "hair will often be so fastened as to fall at the slightest touch," and other histrionic effects would testify to the "ingenuity of the performer.[196]
Such a minx, manipulating a "self-produced disease" in which the patient herself had full "power over the paroxysm,"[197] could be overcome only by a battle royal engaged by the physician, willing to enter into a war of wills. Defeating the "tricks" of such a monster of "selfishness and deceptivity," possessed of a "mendacity that verges on the sublime,"[198] was not, however, an easy matter; for the symptoms of physical illness (including in the extreme case the tacit threat of fasting unto death) were powerful weapons to have in one's armory. Carter knew medical means were utterly irrelevant (no Mesmeric magnets for him). Psychological warfare was needed to defeat "the ends which she proposes to
herself for attainment."[199] First, the hysteric had to be separated from her parents and friends and incarcerated in the physician's home. Once there, under no circumstances should the doctor "minister to the hysterical desire."[200] Every bid of the patient to use hysterical tantrums to command attention had to be steadfastly ignored and thus proven futile: no notice was to be taken of convulsions, self-starving, or acts of self-mutilation; above all, the hysteric's cravings for surrogate sexual gratification, especially through demands for vaginal examinations with a speculum, had to be resisted.[201] Normal, sociable behavior was, by contrast, to be encouraged and rewarded.
No holds were barred. The hysteric was mistress of duplicity, and, in response, the physician would often find it necessary to "completely deceive her."[202] His most difficult task was to find tactful ways of communicating to the hysteric that her wiles had been rumbled and the game was up. Diplomatically done, this would afford her the opportunity to surrender with honor, and put herself "completely in the power of her interlocutor,"[203] whereupon she might make a clean breast of things, preparatory to being reincorporated, as the prodigal daughter, into normal, bourgeois life (that life whose constraints and double standards, Carter himself had initially acknowledged, were responsible for hysteria in the first place).
Several aspects of Carter's account of how to tame a hysterical shrew and bring her to "humiliation and shame" are worth noting.[204] For one thing, his psychological reading of hysteria drew heavily upon the idiom and premises of early nineteenth-century psychiatry; Carter explicitly valued "moral management" and "moral therapy."[205] He proposed turning his own abode into a hysterics' asylum, in whose gothic isolation the battle for the mind could be waged. One might gloss this by noting that as a young general practitioner, Carter was in no position to contemplate the laborious investigation of the laws of hysteria as undertaken by Professor Charcot at the Salpêtrière. Economics forced Carter—as to some degree Freud after him—to be concerned with cure rather than scientific exploration, and to have an eye to fees.
Drawing upon contemporary asylum psychiatry, Carter forged a conceptual triangle of elective affinities, profoundly pregnant for the future, linking (1) psychological explanation with (2) female nature and (3) a sexual etiology ("sexual emotions are those most concerned in the production of the disease").[206] In other words, in its grave forms, hysteria was a matter of mental acts (frauds), perpetrated by women , in order to achieve surrogate sexual gratification. By contrast, however, to earlier uterine theories, Carter's hypothesis did not lay blame at the door of
female anatomy: rather what Hack Tuke later called a "paralysis of the will" was at fault. Although Carter noted that "if the state of society permitted free expression"[207] of female sexual desires, hysteria might dissolve away, he produced not a critical sociology of hysteria but a moralizing indictment of self-indulgent women. In this, his idiom explicitly echoed the witch-hunt, as when he remarked that the hysteric who made a hash of faking disease thereby "betrays the cloven foot."[208]
The social histories of Victorian medicine on the one hand, and of women on the other, leave it surely no accident that the prototypical psychogenic theory of hysteria was misogynistic and victim blaming. For the raison d'être of psychologizing hysteria was precisely to deny its authenticity as a malady, exposing it as fraud involving a terrible "degree of perversion of the moral sense."[209] In the history of hysteria, sexual etiologies, genderedness, and victim blaming have ever gone together.
Conclusion
This chapter has been highly selective. In concentrating upon the viewpoint of doctors, it has had little to say about how sufferers represented hysteria to themselves, nor indeed about why people "somatize."[210] It has had nothing to say about intriguing subsets of hysteria—mass hysteria, the hysterical personality—in which mind/body issues also significantly underpin the controversies. It has neither examined the intricacies of Freud's formulations over a period of some twenty years, nor surveyed Freud's contemporaries such as Janet and Babinski.[211] It would, however, seem that the dissolution of the hysteria diagnosis in the wake of Freud may be seen, in part at least, in terms of those shifts in modern ontology mentioned earlier in the discussion of Szasz's contribution. Monique David-Ménard, for instance, has suggested that the Lacanian translation of the location of the psyche from the Freudian mental underground to the domain of language has in effect rendered utterly obsolete most of the mind/body issues so fiercely disputed by the eighteenth- and nineteenth-century doctors discussed in this chapter. Not surprisingly. The psychoanalytical enterprise, unlike the Victorian family or the World War I trench, unlike the nerve sanatorium or the gynecological operating table, is entirely a theater of words.[212]
And this is the point. In the case of hysteria, disease formulations, I have been arguing, go with circumstances: doctors, patients, physical milieux, intellectual and cultural landscapes. My concern has been to argue that hysteria could be fashioned as a disorder, precisely because the culture-at-large sustained tense and ambiguous relations between
representations of mind and body, which were, in turn, reproduced in the hierarchical yet interactive ontologies of morality and medicine, and, yet again, reflected by the sociological interplay of clinical encounters. In hysteria, as with other disorders, different fields of force break in distinctive ways, and medicine plays double games. Sometimes its mission is reductionist, resolving hysteria now into the womb, now into mere willfulness. In other circumstances, medicine seeks to render hysteria real, protecting its mysteries. In hysteria, mind and body may be seen as sublimated representations of doctors and patients.
Four—
Hysteria, Feminism, and Gender
Elaine Showalter1
Hysteria has taken many strange turnings in its long career, but one of the most surprising is the modern marriage of hysteria and feminism, the fascination among feminist intellectuals, literary critics, and artists with what Mary Kelly calls "the continuing romance of hysteria."[1] Feminist understanding of hysteria has been influenced by work in semiotics and discourse theory, seeing hysteria as a specifically feminine protolanguage, communicating through the body messages that cannot be verbalized. For some writers, hysteria has been claimed as the first step on the road to feminism, a specifically feminine pathology that speaks to and against patriarchy. For others, the famous women hysterics of the nineteenth century have been taken to epitomize a universal female oppression. As the French novelist and theorist Hé1ène Cixous melodramatically inquires, "What woman is not Dora?"[2]
This ardent reclaiming of hysteria in the name of feminism is a new twist in the history of the disorder. Throughout its history, of course, hysteria has always been constructed as a "woman's disease," a feminine disorder, or a disturbance of femininity, but this construction has usually been hostile. Hysteria has been linked with women in a number of unflattering ways. Its vast, shifting repertoire of symptoms reminded some doctors of the lability and capriciousness they associated with female nature. "Mutability is characteristic of hysteria because it is characteristic of women," wrote the Victorian physician Edward Tilt. "'La donna è mobile .'"[3] Doctors have tended to favor arguments from biology that link hysteria with femaleness: "Women are prone to hysteria because of something fundamental in their nature, something innate, fixed or
given that obviously requires interaction with environmental forces to become manifest but is still a primary and irremediable fate for the human female."[4] "As a general rule," wrote the French physician Auguste Fabre in 1883, "all women are hysterical and . . . every woman carries with her the seeds of hysteria. Hysteria, before being an illness, is a temperament, and what constitutes the temperament of a woman is rudimentary hysteria."[5] The hysterical seizure, grande hystérie , was regarded as an acting out of female sexual experience, a "spasm of hyper-femininity, mimicking . . . both childbirth and the female orgasm."[6]
In the twentieth century, these views about an essential and organic female biology that produces hysteria have mutated into more psychological portraits that link hysteria with femininity —with a range of "feminine" personality traits. In a psychoanalytic context, women have been seen as disadvantaged in mastering oedipal tasks and thus disposed to hysterical behaviors. Thus, according to the British analyst Gregorio Kohon, "A woman at heart always remains a hysteric."[7] Paul Chodoff notes that hysterical behaviors "may present as . . . unattractive, noisy, emotional displays . . . or as the hysterical (histrionic) personality disorder—a DSM-III diagnostic label, referring to habitual and sustained patterns of behavior characteristic of some women."[8] The diagnosis becomes "a caricature of femininity" but also an exaggeration of the cognitive and personal styles that women are encouraged to develop as attractively "feminine."[9]
Until recently, stories about hysteria were told by men, and women were always the victims in these stories rather than the heroines. In the past few decades, however, the story of hysteria has been told by women historians as well as by male doctors and psychoanalysts. They have argued that hysteria is caused by women's oppressive social roles rather than by their bodies or psyches, and they have sought its sources in cultural myths of femininity and in male domination. What we might call the "herstory" of hysteria is the contribution of feminist social historians to this project, in works that concentrate on the misogyny of male physicians and the persecution of female deviants in witch-hunts.[10]
But as Mark Micale notes, "No line of evolution within the historiography of hysteria is more complicated than the feminist one."[11] The feminist romance with hysteria began in the wake of the women's liberation movement of the late 1960s and the French événements of May 1968, when a young generation of feminist intellectuals, writers, and critics in Europe and the United States began to look to Freudian and Lacanian psychoanalysis for a theory of femininity, sexuality, and sexual difference. They began with the Viennese women who were treated by
Freud and Breuer for hysteria, and who had in a sense given birth to the psychoanalytic method, the "talking cure." Feminist interpretations of hysteria in women offered a new perspective that decoded physical symptoms, psychotherapeutic exchanges, and literary texts as the presentations of conflict over the meaning of femininity in a particular historical context. Hysteria came to figure as what Juliet Mitchell calls "the daughter's disease," a syndrome of physical and linguistic protest against the social and symbolic laws of the Father.[12]
Many Lacanian feminist critics interpret hysteria as a women's language of the body, or pre-oedipal semiotics. Still others see bisexuality as the significance of the syndrome. Thus Jane Gallop writes, "Freud links hysteria to bisexuality; the hysteric identifies with members of both sexes, cannot choose one sexual identity. . . . If feminism is the calling into question of constraining sexual identities, then the hysteric may be a protofeminist."[13] Similarly, Claire Kahane defines "hysterical questions" as questions about bisexuality and sexual identity: "Am I a man? Am I a woman? How is sexual identity assumed? How represented?"[14]
But could hysteria also be the son's disease, or perhaps the disease of the powerless and silenced? Although male hysteria has been documented since the seventeenth century, feminist critics have ignored its clinical manifestations, writing as though "hysterical questions" about sexual identity are only women's questions. In order to get a fuller perspective on the issues of sexual difference and identity in the history of hysteria, however, we need to add the category of gender to the feminist analytic repertoire. The term "gender" refers to the social relations between the sexes, and the social construction of sexual roles. It stresses the relational aspects of masculinity and femininity as concepts defined in terms of each other, and it engages with other analytical categories of difference and power, such as race and class. Rather than seeking to repair the historical record by adding women's experiences and perceptions, gender theory challenges basic disciplinary paradigms and questions the fundamental assumptions of the field.[15]
When we look at hysteria through the lens of gender, new feminist questions begin to emerge. Instead of tracing the history of hysteria as a female disorder, produced by misogyny and changing views of femininity, we can begin to see the linked attitudes toward masculinity that influenced both diagnosis and the behavior of male physicians. Conversely, by applying feminist methods and insights to the symptoms, therapies, and texts of male hysteria, we can begin to understand that issues of gender and sexuality are as crucial to the history of male experience as they have been in shaping the history of women.
In particular, we need to see how hysteria in men has always been regarded as a shameful, "effeminate" disorder. In many early studies the male hysteric was assumed to be unmanly, womanish, or homosexual, as if the feminine component within masculinity were itself a symptom of disease. John Russell Reynolds wrote in A System of Medicine that hysterical men and boys were "either mentally or morally of feminine constitution."[16] in his case studies of male hysteria at the end of the nineteenth century, Emile Batault observed that hysterical men were thought to be "timid and fearful men. . . . Coquettish and eccentric, they prefer ribbons and scarves to hard manual labor." These expectations made it difficult for doctors to accept the hysteria diagnosis in men who seemed conventionally virile. While it might be possible to "imagine a perfumed and pomaded femmelette suffering from this bizarre malady," Batault noted, "that a robust working man has nerves and vapours like a woman of the world" strained credulity.[17]
The prejudices and stereotypes Batault protested at the Salpêtrière are alive and well in the twentieth century. "One gets the impression," an analyst notes, "that a male hysteric is one who behaves 'like a woman.'"[18] Wilhelm Reich described the male hysteric as characterized by "softness and over-politeness, feminine facial expression and feminine behavior."[19] The image of the hysteric in psychiatric literature is such that "the man who would most closely fit the description would be a passive homosexual."[20] Thus discussions of male hysteria, rather than transforming the discourse of hysteria as representing the worst aspects of femininity, actually reinforce the stereotype that it is the disease of weak, passive, overly emotional people, whether female or male.
Gender constructs, moreover, are not restricted to the medical profession. They also inflect the way we write the history of medicine and psychiatry. While feminist literary critics often seem narrow in their use of history, limiting their textual interpretations to a tiny group of famous doctors and patients, historians are rarely sensitive to figurative language and to the inscriptions of gender ideology in medical texts. History can show us where to look for a more accurate and complete picture of hysteria, but literary criticism can show scientists and historians how to read the texts and gender subtexts of medicine, psychiatry, and history itself. For while social historians of hysteria have been sensitive to the ways that attitudes toward women shaped and distorted the work of doctors like Robert Brudenell Carter, Charcot, or Freud, they have written as if they too were not influenced by gender constructs. Issues of sexual difference are relevant to historiography as well as medicine.
Moreover, writing about hysteria is different for women than it is for
men. Because of traditional beliefs about the potential hysteria of all women, women scholars are more conscious of the need to find an objective, impersonal, and scientific language and discourse about the subject. How can one who is potentially hysterical, "at heart always a hysteric," transcend her nature to write about the disorder? Since feminism has often been interpreted as hysteria by male physicians and social critics, women writing about hysteria in the early part of the twentieth century may have avoided feminist interpretations of hysterical phenomena.
On the other hand, men writing about hysteria, in males or females, can masquerade their own emotions as reason, or disguise feeling and prejudice behind other terminologies and self-definitions. In his study L'hystérique, le sexe, et le médecin , the French psychiatrist Lucien Israël discusses the "unconscious complicity between sick men and male doctors to avoid the shameful and infamous diagnosis of hysteria." But when he talks about what he terms "successful hysterics," people who in their adult lives seemed to outgrow their adolescent hysteria, or transformed what had been hysterical symptoms into social causes, Israel mentions only women, such as Mary Baker Eddy, the founder of Christian Science, and Bertha Pappenheim, or Anna O., who became a German feminist leader. He sees their dedication as an evolutionary form of feminine hysteria itself, an obsessive desire to become the maître rather than submit to him, an acting out of fantasies of devotion. Thus female activism becomes merely a constructive pathology, and feminism only a healthier form of hysteria. It does not occur to Israël to label Flaubert or Sartre a successful hysteric, let alone to speculate on the way this scenario might explain the career decisions of male psychoanalysts.[21]
Language has played a major role in the history of hysteria; to pry apart the bond between hysteria and women, to free hysteria from its feminine attributes, and to liberate femininity from its bondage to hysteria, means going against the grain of language itself. To begin with, as Helen King shows in chapter 1, hysteria has always been etymologically linked with women and the feminine because of its name. We can argue that when Freud's Viennese colleague dismissed Freud's talk on male hysteria because men didn't have wombs, he was pathetically out of date; nonetheless, the word itself has become so generically linked with the feminine in popular understanding that we need to specify male hysteria the way we specify women writers, whereas to say female hysteria sounds redundant.
Because of this understanding and the stigma it has carried, throughout the centuries doctors have sought to find other names for hyste-
ria in men. As Israel explains, "The hysteria diagnosis became for a man . . . the real injury, a sign of weakness, a castration in a word. To say to a man 'you are hysterical' became under these conditions a form of saying to him 'You are not a man.'"[22] To avoid such a confrontation, doctors sought unconsciously to mask the hysteria diagnosis under other terms; in France in the nineteenth century, for example, it was known as "neurospasme," "tarassis," "didymalgie," "encéphalie spasmodique," or "neuropathie aigue cérébro-pneumogastrique."
Furthermore, hysteria is invariably represented as feminine through the figures of medical and historical speech. Evelyn Fox Keller, Ludmilla Jordanova, Emily Martin, and Cynthia Russett, among others, have begun in recent years to analyze the gendered rhetoric and epistemology of scientific inquiry, through close reading of the figures, metaphors, and representations that have always been part of medical discourse.[23] Such images are not merely decorative or accidental, they argue, but are a fundamental part of the gendered language that science shares with other human discourses. As Jordanova notes, "the biomedical sciences deploy, and are themselves, systems of representation. If devices like personification and metaphor have been central to scientific thinking, then the notion of representation becomes a central analytical tool for historians."[24] Helen King points out that the history of hysteria depends on a series of texts, on the way language was deployed and translated within these texts, and on the narratives of female power and powerlessness that were based upon them. In order to understand the longevity and cultural force of these narratives, we need to look at terminology, metaphor, and narrative techniques as well as at statistics and theories.
In his recent study, for example, Etienne Trillat discusses the theories of male hysteria that have flourished for several centuries. But his images tell a different story. "All psychoanalytic theory was born from hysteria," he writes, "but the mother died after the birth." Even in denying the sexual etiology of hysteria, thus historiography reinscribes it through language echoing the traditional terminology for hysteria, the "suffocation of the mother" or the "mother."[25]
We could also look at the striking metaphor Breuer used in Studies on Hysteria when he called hysterics "the flowers of mankind, as sterile, no doubt, but as beautiful as double flowers."[26] The image is botanical, sexual, and aesthetic. In cultivated flowers, doubling comes from the replacement of the stamens by petals. Like the double flower, Breuer implies, the hysteric is the forced bud of a domestic greenhouse, the product of luxury, leisure, and cultivation. Her reproductive powers have been sacrificed to her intellect and imagination. Like the curved flowers
of Art Nouveau, or the Jüngenstihl , she is also an aesthetic object, standing in relation to a more sober "mankind" as feminine and decorative. Finally, the hysteric is seductive and attractive, but incapable of maternity or creativity. From Breuer's point of view, as the case studies make clear, the hysteric's sterility and her intense abnormal flowering go together, as if to echo Victorian stereotypes about the incompatibility of uterine and cerebral development.
But from the woman's point of view, sterility may result from being in advance of one's time and unable to find a partner. The same metaphor is used by Olive Schreiner, herself an example of the New Woman who overcame hysterical disorders to lead an important career as a feminist and writer. Schreiner imagined that if sex and reproduction could be separated, human sexuality, especially female sexuality, might become like the cultivated rose, which "having no more need to seed turns all its sexual organs into petals, and doubles, and doubles; it becomes entirely aesthetic."[27] For Schreiner, the hysteric is thus a member of the sexual avant-garde.
Male homosexuals too can be read, perhaps more precisely than women, into Breuer's metaphor of the double flower. They are Schreiner's highly evolved beings who have perforce separated sexuality from reproduction, and who must pour their creativity into art. In his study of Oscar Wilde, for example, Neil Bartlett calls Wilde's green carnation the symbolic flower of the gay man: "A homosexual, like a hothouse flower, declares his superiority to the merely natural. . . . Homosexuals are sterile . . . they blossom in the form of works of art."[28]
It is not surprising that the metaphors of hysteria should contain double sexual messages about femininity and masculinity, for throughout history, the category of feminine "hysteria" has been constructed in opposition to a category of masculine nervous disorder whose name was constantly shifting. In the Renaissance, these gendered binary oppositions were set up as hysteria/melancholy; by the seventeenth and eighteenth centuries, they had become hysteria/hypochondria; in the late nineteenth century they were transformed into hysteria/neurasthenia; during World War I, they changed yet again to hysteria/shell shock; and within Freudian psychoanalysis, they were coded as hysteria/obsessional neurosis. But whatever the changing terms, hysteria has been constructed as a perjorative term for femininity in a duality that relegated the more honorable masculine form to another category.
If we go back to medical records from the early seventeenth century, we find a differentiation between hysteria, a disorder that was believed to have its origins in displacement of the uterus and the accumulation
of putrid humors; and melancholy, a prestigious disorder of upper-class and intellectual men. Vieda Skultans has pointed out that "the epidemics of melancholy which swept the fashionable circle of London from 1580 onwards curiously bypassed women."[29] She sees a connection between the misogynistic literature that flourished during the late seventeenth century and the emergence of hysteria as a significant diagnostic category. By the end of the seventeenth century, melancholy and hysteria had been joined by new fashionable diseases: the spleen, vapours, and hypochondria; and these disorders were also differentiated by gender. Spleen and vapours were seen as akin to hysteria, female maladies that came from the poisonous fumes of a disordered womb. As Roy Porter has discussed in chapter 3, late seventeenth-century accounts of the neurological aspects of hysteria that moved away from the uterine theory also advanced theories of male hysteria. In these accounts physicians were agreed that hysterical men were much rarer than hysterical women, that they behaved in womanish ways, and that their affliction should be called "hypochondriasis." According to Thomas Sydenham, for example, hypochondriacal symptoms were as similar to hysterical symptoms "as one egg is to another" and could be seen in "such male subjects as lead a sedentary or studious life, and grow pale over their books and papers."[30]
In the eighteenth century, there was a gender split in the representation of the body, with the nervous system seen as feminine, and the musculature as masculine.[31] Doctors made a firm gender distinction between forms of nervous disorder, assigning hysteria to women and hypochondria to men. According to the French physician Jean-Baptiste Louyer-Villermay, these categories also corresponded to a psychology of sex differences. Turbulent passions, ambitions, and hate, which were natural to men, predisposed them towards hypochondria, while in women the dominant emotion was that of love.[32] Concern with the feminizing label of hysteria obviously affected diagnosis; when Edward Jenner had hysterical symptoms, he noted that "in a female I should call it hysterical—but in myself I know not what to call it but by the old sweeping term nervous."
In England, most Victorian medical men "had the idea that there was a mental disease for each sex—hypochondriasis for the male and hysteria for the female."[33] By the nineteenth century, the sexual specificity of hysteria and hypochondriasis had become a medical dogma, so that "when hysteria is admitted in men, it is understood nevertheless as a female affliction."[34] Thus the Viennese doctor Ernst von Feuchtersleben in 1824 argued that if women showed signs of hypochondriasis they
must be "masculine Amazonian women," while hysterical men "are for the most part effeminate men."[35] But whereas hypochondriasis had started as a dignified illness that a man might even claim with some masculine self-respect, during the nineteenth century it too gradually became established as a form of mental disorder that carried its own stigma. In the eighteenth century, the man of cultivation and intellect who suffered from a variety of afflictions was universally admired, but when it became embarrassing for men to acknowledge that they were hypochondriacs, and such people, like Jane Austen's Mr. Woodhouse, became figures of fun, a new masculine term was required to set alongside hysteria.
In 1873, this gap in the medical lexicon was filled by the term neurasthenia . "Undoubtedly the disease of the male subject in the late nineteenth century,"[36] neurasthenia was first identified in the United States and linked with the nation's nervous modernity. In American Nervousness , George M. Beard, who named the new disorder, defined neurasthenia as a condition of nervous exhaustion, an "impoverishment of nervous force." He believed that neurasthenia was caused by industrialized urban societies, competitive business and social environments, and the luxuries, demands, and excesses of life on the fast track. In a sense then, neurasthenia was a source of pride and a badge of national distinction and racial superiority. To be stressed was "one of the cardinal traits of evolutionary progress marking the increased supremacy of brain force over the more retarded social classes and barbarous peoples." To Beard, reports of missionaries, explorers, and anthropologists seemed to show that primitive, savage, and heathen groups were simpler and less sensitive than middle-class Americans.[37] Bushmen and Sioux Indians did not become neurasthenic like Boston bankers and New York lawyers.
Like hysteria, neurasthenia encompassed a staggering range of symptoms, from blushing, neuralgia, vertigo, headache, and tooth decay to insomnia, depression, chronic fatigue, fainting, and uterine irritability. But unlike hysteria, neurasthenia was an acceptable and even a valuable illness for men. While it affected both men and women between the ages of fifteen and forty-five, it was most frequent "among the well-to-do and the intellectual, and especially among those in the professions and in the higher walks of business life, who are in deadly earnest in the race for place and power."[38] it was definitely, in short, the neurosis of the male elite. Many nerve specialists, including Beard himself, had experienced crises of nervous exhaustion in their own careers, and they were highly sympathetic to other middle-class male intellectuals tormented by vocational indecision, overwork, sexual frustration, internalized cultural
pressure to succeed, and severely repressed emotional needs. When Herbert Spencer visited the United States in 1882, he was struck by the widespread ill health of American men: "In every circle I have met men who had themselves suffered from nervous collapses, due to stress of business, or named friends who had crippled themselves by overwork."[39] But French and English men, doctors from these countries were quick to argue, could be nervous too. In Paris, Charcot noted that "the young men who graduate from the Ecole Polytechnique, who intend to become heads of factories and rack their brains over mathematical calculations, often become victims of these afflictions."[40] The male patients in Charcot's private practice, who came from the middle and upper classes, were more likely to be called "neurasthenic" than "hysterical."[41]
The social construction of neurasthenia reflected the romance of American capitalism and the identification of masculinity with money and property. Beard's metaphors repeatedly emphasized the economic and technological contexts of American nervousness. Neurasthenics were in "nervous bankruptcy," perpetually overdrawing their account, rather than "millionaires of nerve force."[42] The neurasthenic man
is a dam with a small reservoir behind it, that often runs dry or nearly so through the torrent as the sluiceway, but speedily fills again from many mountain streams; a small furnace, holding little fuel, and that inflammable and combustible, and with strong draught, causing quick exhaustion of materials and imparting unequal, inconstant warmth; a battery with small cells and little potential force, and which with little internal resistance quickly becomes actual force, and so is an inconstant battery, requiring frequent repairing and refilling; a dayclock, which if it be not wound up every twenty-four hours, runs utterly down; evolving a force sometimes weak, sometimes strong, and an engine with small boiler-power, that is soon emptied of its steam; an electric light attached to a small dynamo and feeble storage apparatus, that often flickers and speedily weakens when the dynamo ceases to move.[43]
This epic metaphor vividly suggests the specter of the masculine engine wearing out, the depletion of sperm cells, the lack of ejaculatory force. It reflects late nineteenth-century male sexual anxieties of impotence caused by mental or physical overwork. Herbert Spencer put this idea forward quite straightforwardly in an article written for the Westminster Review in 1852. "Intense mental application," Spencer argued, "is accompanied by a cessation in the production of sperm-cells," while correspondingly, "undue production of sperm-cells involves cerebral inactivity," beginning with headache and proceeding to imbecility.[44]
This theory cut both ways. On the one hand, lack of desire for women
could be explained by devotion to intellectual tasks; on the other hand, overindulgence in sex could lead to intellectual decline. Thus for some male intellectuals, the neurasthenia diagnosis relieved anxiety about lapses from conventional masculine sexuality by classifying them under the manly heading of overwork. Spencer himself was cited by Beard as one of the world's most distinguished neurasthenics, "doing original work on a small reserve of capital force." In 1853, after a vigorous climbing expedition in the Alps, Spencer had noticed odd symptoms—palpitations, insomnia, "cardiac enfeeblement," a "sensation in the head." Although he lived another fifty years, he treated himself as an invalid, pampering himself with rest and recreation, putting in earplugs when a conversation threatened to become too exciting, "keeping up the cerebral circulation" by wetting his head with saltwater and encasing it in flannel and a rubber nightcap. Despite what one might regard today as real social handicaps, Spencer was seen by his male friends as a great marital catch, and with shrewd pre-Freudian insight into his problem, they urged him to take a wife, recommending "gynoepathy" as a cure for his ills. Spencer however resisted, and as Gordon Haight wisely remarks, with neurasthenia "he bought safety from the perils of marriage."[45]
But the construction of neurasthenia as masculine was an illusion. In the United States, equal numbers of male and female patients were reported in the medical journals.[46] However, cases were differentiated in terms of both gender and class. In middle-class men, the disorder was attributed to overwork, sexual excess, anxiety, ambition, sedentary habits, or the use of alcohol, tobacco, or drugs. Beard estimated that one out of every ten neurasthenics was a doctor. In working-class men, sexual excess, trauma, and overwork were cited as the main causes of the disease. And in all women, childbirth and reproductive disturbances came at the top of the list, with overwork a factor for working-class women and attending college a factor for middle-class women.[47] Gosling notes that the case histories of male patients are much more interesting, detailed, and varied than those of women; "because men normally led more varied lives than most women, involving themselves in career, family, and social activities both within and outside the domestic circle, physicians made greater distinctions in the causes to which they attributed male nervousness. Physicians also questioned men in more detail about their habits and personal affairs, partially because they were more likely to suspect men of hidden vice and partially because of the delicacy of raising intimate issues with members of the opposite sex."[48]
In England, neurasthenia quickly lost its sheltering power for men
and became a female malady like hysteria. Indeed, Havelock Ellis estimated that there were fourteen neurasthenic women for every neurasthenic man. Explanations for neurasthenia in women drew on some of the same sources as the explanations about men, but with a different moral emphasis. Edward Clarke in the United States and Henry Maudsley in England drew on new theories of the conservation of energy to argue that mental and physical energy were finite and competing. Women's energy, post-Darwinian scientists believed, was naturally intended for reproductive specialization. Thus women were heavily handicapped, even developmentally arrested, in intellectual competition with men. Nervous disorder would come when women defied their "nature" and sought to rival men through education and work, rather than to serve them and the race through maternity. While competition was a healthy stimulus to male ambition, it was disastrous for women, who furthermore did not have the outlet of athletics to relieve their strained nerves. The higher education of women in universities was obviously then a threat not only to their health but to their reproductive capacities. "What Nature spends in one direction, she must economise in another direction," Maudsley wrote, and thus the young woman who gave herself over to learning would find her sexual and reproductive organs atrophying, her "pelvic power" diminished or destroyed, and her fate one of sexlessness and disease.[49] The neurasthenic Girton or Vassar girl was overworking her brain and uterus into sterility.
The standard treatment for neurasthenia was the rest cure, developed by the American Dr. Silas Weir Mitchell (1829-1914) after his experience in the Civil War. First described in 1873, the rest cure involved seclusion, massage, immobility, and "excessive feeding." For six weeks the patient was isolated from her friends and family, confined to bed, and forbidden to sit up, sew, read, write, or do any intellectual work. She was expected to gain as much as fifty pounds on a rich diet that began with milk and built up to several substantial daily meals. Mitchell was well aware that the sheer boredom and sensory deprivation of the rest cure made it a punishment to the patient: "When they are bidden to stay in bed a month, and neither to read, write, nor sew, and have one nurse—who is not a relative—then rest becomes for some women a rather bitter medicine, and they are glad enough to accept the order to rise and go about when the doctor issues a mandate which has become pleasantly welcome and eagerly looked for."
The rest cure evolved from Mitchell's work with "malingering" soldiers in the Civil War, whom he had assigned to the most disagreeable jobs, so that after a few weeks in the latrines they were eager to return
to the front.[50] But it also depended on his feelings on the differences between men and women and their social meaning:
For me the grave significance of sexual difference controls the whole question, and if I say little of it in words, I cannot exclude it from my thought of them and their difficulties. The woman's desire to be on a level of competition with man and to assume his duties is, I am sure, making mischief, for it is my belief that no length of generations of change in her education and modes of activity will ever really alter her characteristics. She is physiologically other than man. I am concerned with her now as she is, only desiring to help her in my small way to be in wiser and more healthful fashion what I believe her Maker meant her to be, and to teach her how not to be that with which her physiological construction and the strong ideals of her sexual nature threaten her as no contingencies of man's career threaten in like measure or like number the feeblest of the masculine sex.[51]
A determined opponent of higher education for women, a critic of Vassar and Radcliffe and especially of "the horrible system of coeducation,"[52] Mitchell, like other Victorian physicians, believed that the female reproductive system and the brain derived their nourishment from the same source, and that women should not try to learn too much during adolescence when the menstrual function was being established. "I firmly believe," he wrote, "that as concerns the physical future of women they would do better if the brain were very very lightly tasked and the school-hours but three or four a day until they reach the age of seventeen at least."[53] He also advised mothers not to allow their pubescent daughters to take strenuous exercise. The quest for knowledge, he felt, destroyed that subtle and tender feminine charm which was the only source of masculine love: "For most men, when she seizes the apple, she drops the rose."[54]
While Mitchell was aware that hysteria in women of the middle and upper classes was largely caused by "the daily fret and wearisomeness of lives which . . . lack those distinct occupations and aims" that sustained their brothers and husbands, he did not seem to make the connection between his program of female ignorance and passivity, and women's later inability to lead healthy lives.[55] He preferred women patients who were silent and acquiescent to those with inquiring minds. "Wise women choose their doctors and trust them," he wrote in Doctor and Patient . "The wisest ask the fewest questions. The terrible patients are nervous women with long memories, who question much where answers are difficult, and who put together one's answers from time to time and torment themselves and the physician with the apparent inconsis-
tencies they detect."[56] In his novel Roland Blake , Mitchell created such a terrible patient in the figure of Octapia Darnell, a repugnant hysteric whose sickly tentacles wound themselves about her hapless family. He preferred to use women's trust in him in effecting a cure: "If you can cause such hysteric women as these to believe that you can cure them, you enlist on your side their own troops, for as you can create symptoms, so you can also create absence of symptoms."[57]
Furthermore, the treatment assumed that the patient be "pliant and wealthy": one who did not work, or at least did not need to work. Middle-class women were thus the best candidates for the rest cure, since men and the poor were unlikely to be willing to spend six to eight weeks in idleness. Doctors thus modified the treatment for their male patients, who might simply be advised to get to bed early and to travel first-class. As the Chicago neurologist Archibald Church observed, "We cannot put [men] to bed with any expectation that they will stay there. I have tried it repeatedly and have nearly always failed. Men do not take to the recumbent position for any considerable length of time with equanimity. The fact of their being in bed constitutes an aggravation; and irritation is what we wish to exclude."[58]
Women were just as irritated by isolation and enforced idleness as men. Mitchell's patients indeed included many of the leading feminist intellectuals, activists, and writers of the period, including Jane Addams, Winifred Howells, Charlotte Perkins Gilman, and Edith Wharton. For them, feminist scholars have argued, the rest cure seemed like a regression to infancy, in which the patient was forced back into "womblike dependence" on the parental team of godlike male doctor and subservient female nurse, and reeducated to "make the will of the male her own";[59] or a disciplinary treatment that punished unconventional aspirations; or even a pseudo-pregnancy that symbolically put the deviant woman back in her biological place. Forbidden by Mitchell to write or draw, Gilman came close to a breakdown: "I would crawl into remote closets and under beds—to hide from the grinding pressure of that profound distress."[60] Casting Mitchell's advice to the winds, she went to work again, "work, in which is joy and service, without which one is a pauper and a parasite." For Gilman, hysteria was the result of passive acquiescence to the strictures of a patriarchal society, but it could be overcome by purposeful activity, in her case writing. She wrote the chilling short story "The Yellow Wallpaper" (1892), a Gothic tale of a young mother suffering from a "temporary nervous depression—a slight hysterical tendency," who goes mad during a rest cure, as a protest against Mitchell, but there is no evidence that he ever read or responded to it. Similarly,
Dr. Margaret Cleaves insisted on the importance of work for women's mental health, and the dangers of the rest cure: "The hardest cases I have had to take care of professionally," she wrote, "are those who have acquired the rest cure habit. I have a physician under care now, this time a woman, who regrets piteously that she was not given something to feed her intelligence instead of an unqualified rest cure."[61]
But even women doctors did not have the cultural authority to contest medical dogmas. Later Freud did have the authority to criticize Mitchell. In Studies on Hysteria , in a passage that might be seen as a medical acknowledgment of Gilman's experience, he advised combining the rest cure with analysis: "This gives me the advantage of being able . . . to avoid the very disturbing introduction of new psychical impressions during a psychotherapy, and . . . to remove the boredom of a rest-cure, in which the patients not infrequently fall into the habit of harmful daydreaming."[62] Still, the rest cure was not really discredited until World War I, when it was discarded as inappropriate and even harmful as a therapy for men.
The rest cure was one form of fin-de-siècle therapy that asserted male medical domination over the nervous woman. Treatments for hysterical women in the late nineteenth century were even more tyrannical, and doctors found reasons not to apply them to men. In England the model for this approach, based on established notions about the charismatic male physician and the manipulative sickly woman, had been pioneered by Robert Brudenell Carter and described in his book On the Pathology and Treatment of Hysteria (1853). Only twenty-five when he wrote his book, Carter adopted the tone of a much more mature and established man, a persona that was very much part of his whole program for asserting sexual and medical authority over the wayward hysterical girl. While Carter recognized that there were also cases of hysteria in men, he insisted that they were rare and anomalous. Not only were emotional derangements "much more common in the female than the male," but also women were forced by social pressure to conceal their feelings and desires, especially sexual ones. Moreover, the "morbid and insatiable . . . craving for sympathy" that led to sick behavior was "ten times stronger in women than in men."[63]
During a season when he served as the director of an agricultural workhouse, Carter had to contend with a number of young married women who had been separated from their husbands and children. These women had no real outlet for their feelings of loneliness and anxiety, and some had begun to have daily fits of crying and screaming. Carter found the attacks an administrative nuisance and set out to stop
them. Whenever a woman had an attack, he made a large group of the others nurse her, insisting that none of them could have any food until all the symptoms of the attack had subsided. Very quickly the "hysterical" women became so unpopular with the others that the fits ceased to occur.
Carter's attitude toward middle-class hysterics was equally antagonistic, but his methods of managing them had to be more subtle. In his view, the hysterical girl is a clever, persistent, and desperate person who has entered into a sustained deception, and would "lose caste" if exposed. Therefore she is prepared for a long siege against the doctor who would make her well—that is, make her give up her symptoms. While he thoughtfully considers the efficacy of rough treatments for hysterics, such as unpleasant medicines, blows, or buckets of cold water, Carter concludes that most hysterical girls would be able to tolerate such attacks and turn them against the doctor, undermining his authority: "A young woman who is living at home will have too much courage and endurance to be beaten by the torture, and . . . a certain amount of perseverance on her part will exalt her into a martyr in the eyes of her family, and will enable her to bid defiance to professional denunciations."[64] Thus he advocated removing the patient from her family to the doctor's home, where she could be under constant surveillance.
The plan for treatment he outlines is basically a form of blackmail, threatening the hysteric that if she does not reform her ways, the doctor will expose her malingering and disgrace her in the eyes of her family and friends. In fact, by the time this threat is pronounced, the doctor has already secretly told the family his diagnosis and sworn them to secrecy, so the hysteric is operating in the midst of a conspiracy or game in which everyone is collaborating to trick her. Telling the family of the plot is necessary to effect the patient's separation from them. When she is removed from all her accustomed sources of sympathy and support, the doctor can have full power over her habits and treatment.
British attitudes toward the understanding and management of the hysterical woman followed Carter's example. In general, Victorian doctors saw hysteria as a disorder of female adolescence, caused both by the establishment of the menses and by the development of sexual feelings that could have no outlet or catharsis. Adolescence was a risky time for girls, many doctors observed, not only because the reproductive organs had so great an influence on their entire well-being but also because "the range of activity of women is so limited, and their available paths of work in life so few . . . that they have not, like men, vicarious outlets for feelings in a variety of healthy aims and pursuits."[65] While men, wrote
Charles Mercier, had the "safety-valve" of exercise, women's feelings were bottled up, so that in adolescence, "more or less decided manifestations of hysteria are the rule."[66] "All kinds of . . . barriers to the free play of her power are set up by ordinary social and ethical customs," wrote Dr. Bryan Donkin. "'Thou shalt not' meets a girl at every turn."[67] F. C. Skey, who delivered a series of lectures on hysteria to the medical students at St. Bartholomew's Hospital in 1866, noticed that his patients were primarily adolescent girls with domineering parents, girls who "exhibited more than usual force and decision of character."[68]
Despite their sympathy for the plight of Victorian girls, Victorian doctors found their hysterical patients selfish, deceitful, and manipulative. Henry Maudsley denounced the "moral perversion" of hysterical young women who "lie in bed" all day, "when all the while their only paralysis is a paralysis of the will."[69] Skey followed Carter's lead in recommending "fear and the threat of personal chastisement" for hysterical women.[70] In the title of one American medical text, hysteria was a matter of "trials, tears, tricks, and tantrums."[71]
In France, working-class hysterical women patients at the Salpêtrière were regarded with the same hostility by such doctors as Jules Falret. Falret denounced the women as "veritable actresses; they do not know a greater pleasure than to deceive . . . all those with whom they come in touch. The hysterics who exaggerate their convulsive movement . . . make an equal travesty and exaggeration of the movements of their soul, their ideas, and their acts. . . . In a word, the life of the hysteric is nothing but one perpetual falsehood; they affect the airs of piety and devotion, and let themselves be taken for saints while at the same time abandoning themselves to the most shameful actions; and at home, before their husbands and children, making the most violent scenes in which they employ the coarsest and often most obscene language and give themselves up to the most disorderly actions."[72]
Why did hysteria become such a frequent phenomenon in the late nineteenth century? Why were doctors like Carter, Mitchell, Falret, and Skey so contemptuous of their female patients and so dictatorial in their treatments? A number of theories have been advanced to explain the phenomenon of fin-de-siècle hysteria. The feminist historian Carroll Smith-Rosenberg gives an answer that is sympathetic to both hysterical women and their male physicians. She sees female hysteria as stemming from sex-role conflicts that emerged in the nineteenth century. She has argued that the American hysteric was typically the idle middle-class woman, both "product and indictment of her culture." Reared to be weak, dependent, flirtatious, and unassertive, many American girls grew
up to be child-women, unable to cope with the practical and emotional demands of adult life. They defended themselves against the hardships and obligations of adulthood "by regressing towards the childish hyper-femininity of the hysteric." Faced with real responsibilities and problems, these women fled from stress by choosing a sick role in which they won continued sympathy and protection from the family. Thus hysteria provided a solution to the feminine conflict between idealized sex roles and quotidian realities: "The discontinuity between the roles of courted young woman and pain-bearing, self-sacrificing wife and mother, the realities of an unhappy marriage, the loneliness and chagrin of spinsterhood, may all have made the petulant infantilism and narcissistic self-assertion of the hysteric a necessary social alternative to women who felt unfairly deprived of their promised social role and who had few strengths with which to adapt to a more trying one."
Male physicians like Mitchell dealing with these women may sometimes have been harsh and insensitive, Smith-Rosenberg concludes, but they were not necessarily more misogynistic than other men of their time. Their profession made it necessary for them to make analytic statements about femininity, while their gender demanded that they establish an authoritative relationship with their patients. Thus the physician too was a product of his gender and culture, "standing at the junction where the cultural definitions of femininity, the needs of the individual female patient, and masculinity met."[73] If hysterical women were victims of a culture that did not prepare them to meet the responsibilities of adulthood, their doctors too were victims of a sex-role conflict that required them both to identify with the fathers and husbands of their patients, and to provide answers and cures for the problems of the women in a way that threatened to feminize them.
In The History of Sexuality , Michel Foucault suggests that hysteria was a label bestowed on female sexuality by male physicians. Rather than seeing hysteria as a solution to the double binds and dilemmas of fin-de-siècle women, Foucault describes the "hysterization of women's bodies" as one of the crucial features of psychiatric and medical power. Hysterization was "a three-fold process whereby the feminine body was analyzed . . . as being thoroughly saturated with sexuality; whereby it was integrated into the sphere of medical practices, by means of a pathology intrinsic to it; whereby, finally, it was placed in organic communication with the social body . . . the family space . . . and the life of children; the Mother, with her negative image of 'nervous woman,' constituted the most visible form of this hysterization."[74]
Women's needs, roles, conflicts, feelings, and voices have little to do
with the scenario of power outlined by Foucault. Instead, women are passive and apparently powerless bodies and figures who are inscribed by unnamed forces. "It is worth remembering," he insists, "that the first figure to be 'sexualized' was the 'idle' woman. She inhabited the outer edge of the 'world', in which she always had to appear as a value, and of the family, where she was assigned a new destiny charged with conjugal and parental obligations. Thus there emerged the 'nervous' woman. . . . In this figure the hysterization of woman found its anchorage point."[75] Through his use of quotation marks, Foucault casts ironic doubt on the reality of the hysterical woman's idleness or sexuality, but since his focus is on the large anonymous forces of psychiatric power, he does not supply an explanation for the hysteric's collusion or helplessness before such labeling. Nor, unlike Smith-Rosenberg, does he attempt to explain some of the motives doctors might have had for exerting such power over the definition of female hysteria, or the reasons why it became epidemic in the last decades of the century.
Neither of these influential theories can really account for the varieties and causes of hysteria in their respective contexts. To begin with, I need to emphasize once again that they exclude male hysteria from their analysis, although both are aware of its existence. Smith-Rosenberg comments in a footnote that male hysteria does not undermine her arguments about its relation to female experience for four reasons. First, "to this day hysteria is still believed to be principally a female 'disease' or behavior pattern." Second, the male hysteric is "different"—homosexual or working class. Third, "one must hypothesize that there was some degree of female identification among the men who assumed a hysterical role." Finally, she argues, male hysteria had its most typical form in shell shock.[76] These circular arguments, which Smith-Rosenberg did not reconsider when she revised her original essay for publication in the book, make it impossible for the "difference" of male hysteria to modify her concept of the "hysterical role." Male hysteria is simply a subset of female hysteria, and mimics its motives and behaviors. Applying Smith-Rosenberg's model to male hysterics, then, one would see them as childish, weak, and escapist. The alternative approach—analyzing hysterical symptoms as a response to powerlessness—does not come up.
Despite his interest in forms of discursive power, Foucault too does not consider hysteria from the point of view of the patient, although some of his references hint at the dilemma of young hysterics, both male and female, caught between domineering parents and domineering doctors. He quotes Charcot's insistence that hysterical girls and boys must be separated from their mothers and fathers and hospitalized.[77] But the
idea that these power struggles might have contributed to the problems of adolescent patients is extraneous to Foucault's concerns. He is interested instead in mapping the elements by which doctors took control of the definition of sexuality.
Both Smith-Rosenberg and Foucault identify the bourgeois mother as the representative fin-de-siècle hysteric. But this picture does not correspond to the realities they each describe, nor to the clinical picture. Smith-Rosenberg acknowledges that hysteria crossed class and economic boundaries, and that it also affected working-class and farm women, immigrants and tenement dwellers. In her view these women too had failed "to develop substantial ego strengths."[78] But American doctors who treated poor women in their hospitals and dispensaries had a different view. E. H. Van Deusen, who saw many hysterical farm women at his asylum in Michigan, blamed the social isolation and intellectual deprivation of their lonely lives.[79] Similarly, most of the girls and women Falret and Charcot were treating for hysteria at the Salpêtrière came from poor families and had worked since childhood to support themselves. They were neither idle nor, for the most part, mothers. In case after case, they were the victims of poverty, sexual and financial exploitation, and ignorance. The working-class men Charcot treated in his ward, whose hysteria was usually precipitated by some kind of violent accident, seem like the brothers of the women. Foucault's highly schematic and abstract account of discursive power ignores both context and agency; it neither explains why patients manifested symptoms of distress nor explains why physicians were so eager to focus on these complaints in women and to see them as threats to the family and the state.
The "hysterisation" of women's bodies which Foucault describes can also be seen from a feminist perspective as "a reassertion of women's essentially biological destiny in the face of their increasingly mobile and transgressive social roles."[80] That hysteria became a hot topic in medical circles at the same time that feminism, the New Woman, and a crisis in gender were also hot topics in the United States and Europe does not seem coincidental. During an era when patriarchal culture felt itself to be under attack by its rebellious daughters, one obvious defense was to label women campaigning for access to the universities, the professions, and the vote as mentally disturbed. Whether or not women who were labeled "hysterical" were associated with the women's movement, they were often seen by doctors as resistant to or critical of marriage, and as strangely independent and assertive. These characteristics are most vividly present in the Viennese women dissected by Breuer and Freud, but English physicians like Skey and Bryan Donkin also commented on
the intelligence and ambition of their hysterical patients. Any woman manifesting symptoms of hysteria aroused suspicions of a silent revolt against her domestic, class, and reproductive role. Thus nervous women received much more attention than nervous men, and were labeled as "hysterical" or "neurasthenic" in the contexts of a highly charged rhetoric about the dangers of higher education, women's suffrage, and female self-assertion in general.
In every national setting where female hysteria became a significant issue, there were parallel concerns about the ways that new opportunities for women might undermine the birthrate, the family, and the health of the nation. Intellectually competitive women, doctors warned, were sterile flowers doomed to bring forth only blossoms of hysteria and neurasthenia. In the United States, gynecologists warned against the brain-fag, headache, backache, spine-ache, and all-around sexual incompetence that New Women would produce.[81] in France, the femme nouvelle was blamed for the declining birthrate; new divisions of labor seemed to threaten the stability of the family and the state. As women made their first inroads into public and professional space, a fascinating alliance of artists, traditional women, and neuropsychiatrists like Charcot united in a campaign to celebrate maternity and the interiority of Woman.[82] in England the New Woman as neurotic feminist intellectual had become a recognizable type by the 1890s; "the New Woman ought to be aware that her condition is morbid, or at least hysterical," wrote one journalist.[83] She had also become a standard figure in literature, whether Thomas Hardy's Sue Bridehead in Jude the Obscure (1895) or George Gissing's Alma Rolfe in The Whirlpool (1897), whom Ian Fletcher calls "a new type of woman, the névrose , the modern hysteric."[84]
While hysterical girls were viewed as closet feminists and reprogrammed into traditional roles, feminist activists were denigrated as hysterics, sick and abnormal women who did not represent their sex. By the 1880s in England, it had become customary for the term "hysterical" to be linked with feminist protest in the newspapers and in the rhetoric of antisuffragists. As Lisa Tickner notes in her study of the British suffrage movement, "for half a century and more, feminism and hysteria were readily mapped on to each other as forms of irregularity, disorder, and excess, and the claim that the women's movement was made up of hysterical females was one of the principal means by which it was popularly discredited."[85] Women who found a public voice for their concerns were lampooned as "the shrieking sisterhood," a term coined by the antifeminist writer Eliza Lynn Linton, who wrote in 1883 that "one of our quarrels with the Advanced Women of our generation is the hysterical
parade they make about their wants and their intentions. . . . For every hysterical advocate 'the cause' loses a rational adherent and gains a disgusted opponent."[86]
Jean-Martin Charcot's clinic at the Salpêtrière offered the best opportunity to examine the different ways that women and men were diagnosed and treated for hysteria at the turn of the century. Studies of hysteria at the Salpêtrière took their form from Charcot's charismatic style. So powerful was his influence in the 1880s that the Salpêtrière was often called the "Hôpital Charcot," and the group of disciples and admirers around him was known as the charcoterie .[87] They were strongly influenced by his work on male hysterics; although the Salpêtrière had traditionally been a women's hospital, under Charcot's direction a small men's ward was opened; male patients were also seen at the outpatients' clinic. Charcot took pride in his research on male subjects and regarded the study of male hysteria as one of the specialties of his clinic and of late nineteenth-century French medicine. By his death in 1893, he had published sixty-one case studies of male hysterics, and he left notes on many more. In a lecture-presentation on hysteria in men, Charcot noted that:
In some ways, this question of male hysteria is the order of the day. In France it has preoccupied physicians for the past several years. Between 1875 and 1880, there have been five dissertation defenses on male hysteria at the Faculté de Paris, and M. Klein, the author of one of these theses, done under the supervision of M. le Dr. Olivier, was able to catalog 80 cases. Since then have appeared the important publications of M. Bourneville and his students; of MM. Debove, Raymond, Dreyfus, and several others; and all these works tend to demonstrate, among other things, that cases of male hysteria can be found fairly frequently in common practice.[88]
He decried the popular belief that "the characteristic trait of hysteria is the instability and the mobility of the symptoms." Even in women, he explained, there "were hysterias of sturdy, permanent phenomena . . . which sometimes resist all medical intervention." Furthermore, men too were sometimes emotionally erratic or exhibited depression and melancholy.
Charcot's clinic was noted for the large number of female patients who, under hypnosis, produced spectacular attacks of grande hystérie or "hystero-epilepsy," a prolonged and elaborate convulsive seizure. The attack could be induced or relieved by pressure on certain areas of the body—what Charcot called hysterogenic zones—and these were especially to be found in the ovarian region. A complete seizure involved three
phases: the epileptoid phase in which the patient lost consciousness and foamed at the mouth; the phase of "clownism" (Charcot was a great fan of the circus), involving eccentric physical contortions; and the phase of "attitudes passionnelles," or sexual poses. The attack ended with a back-bend called the arc-en-cercle .
It was crucial to Charcot's theory of hysteria that it took the same course in men and women. Thus he insisted that there were "numerous striking analogies" between male and female grande hystérie . Charcot's disciple Emile Batault reported with pleasure that a hysterical young man named Gui "presents the symptoms most characteristic of grande hystérie . The attacks are always preceded by the phenomena of testicular aura; he feels something which mounts from the inguinal region towards the esophagus; he has then a feeling of thoracic constriction which oppresses him, his temples throb violently, he has ringing in his ears and hears heavy noises like the fire of distant cannons. His head spins, he loses consciousness, and the attack begins." Because he was young and athletic, Gui's arc-en-cercle was also a splendid affair, which impressed Batault very mightily, as an "acrobatic performance as beautiful as it was varied."[89] Batault also found a hysterogenic zone on Gui's body located around the right testicle.
Just as it was possible to stop a hysterical attack by compressing the woman's ovaries, doctors at the Salpêtrière were convinced that it should be possible to affect the course of a man's attack by putting pressure on the testicles. But this procedure did not always have the desired effects. The doctors found that the attacks were relieved by the compression of the testicles. Others, however, obtained no effect from putting pressure on the seminal gland, and one doctor discovered, perhaps not to our surprise, that squeezing the patient's testicles made the convulsions stronger.
One of Charcot's most original contributions to the theory of male hysteria was his insistence that it should not carry the stigma of effeminacy. He emphasized the fact that hysteria often appeared among tough manual laborers; most of the cases had occurred in the aftermath of a traumatic accident, either at work or in travel. Furthermore, he stressed the working-class status, physical strength, and virile emotions of his male patients, and he mocked other doctors who had problems accepting both the class and gender of patients who clashed with their stereotypes of hysteria: "One is willing to concede that a young, effeminate man may, after indulging in excessive behavior, suffering heartache, or experiencing deep emotions, exhibit several hysterical phenomena; but that a manly artisan, solid, unemotional, a railway engineer, for ex-
ample, might, following a railway accident, a collision, a derailing, become hysteric, the same way as a woman—this, it appears, surpasses the imagination."[90]
Nonetheless, there were significant sexual differences in Charcot's concept of male hysteria. In terms of language, it was often called "hystérie virile" or "hystérie traumatique" to mark its distinction from female hysteria. Although it followed the same course of behavior in men and women, Charcot believed hysteria had different causes that depended on gender. As Mark Micale observes, "Women in his writings fell ill due to their vulnerable emotional natures and inability to control their feelings, while men got sick from working, drinking, and fornicating too much. Hysterical women suffered from an excess of 'feminine" behaviors, hysterical men from an excess of 'masculine' behaviors."[91]
Moreover, although some of Charcot's male hysterics were as colorful and dramatic as the women, they did not attract as much attention from doctors, writers, artists, and journalists. The "wild man" Lap . . . sonne, for example, was covered with symbolic tattoos, such as a veiled woman he called "the night," and he earned his living eating live rabbits in fairs. But while Blanche Wittmann became the "Queen of Hysterics" performing at the Salpêtrière clinic, Lap . . . sonne is remembered only as a case study. The actual numbers of male hysterics were few; overall, male patients comprised no more than five to ten percent of the whole immense hospital population.[92] On the other hand, during the 1870s, the percentage of women patients at the Salpêtrière diagnosed as "hysterical" rose as high as twenty percent.[93]
In addition to the theoretical and statistical differences between male and female hysteria, there were differences in its representation. As Sander Gilman explains in chapter 5 in this book, the hysterical clinic of Charcot was organized primarily around the visual, the photographic, the theatrical, and the spectacular. He was famed for his probing gaze that seemed to penetrate not only to the heart of the patient but also to the souls of his assistants, interns, and associates. His student and biographer Georges Guillain described the examination sessions in which the naked patient sat like an artist's model while Charcot silently studied every detail of the body.[94] Roger Martin du Gard wrote about Charcot's "piercing, prying gaze" and his "tyrannical way of fixing you with his stare."[95] Havelock Ellis too recalled Charcot's "disdainful expression, sometimes even it seemed, a little sour.[96]
This intensely scrutinizing male gaze mingled the mesmerizing power of the hypnotist and the commanding eye of the artist with the penetrating vision of the scientist piercing the veil of nature. It was very much
associated with masculinity itself. Charcot's stare was contrasted with the downcast eyes of his hysterical women patients, and with the "soft, poetic and languorous" gaze of his hysterical male patients.[97]
Through his theatrical lecture-demonstrations (Sarah Bernhardt, acting in cross-dressed parts at the same time, was often compared to the hysterical queens of Charcot's amphitheater[98] ), and even more through the photographic atelier that captured images of the hysterical women for the volumes of iconographies , Charcot emphasized the visual manifestations of hysteria and the hysterical body as an art object. His representations of gender were allied to aesthetic conventions about the female body, whether in painting, photography, or drama. Charcot not only borrowed from art in making the female body the focus of his investigation, but through his photographic atelier also contributed to the historical emergency of a "regime of representation" in which, according to the art critic Griselda Pollock, "the hysterized body of woman. . . was made the object of pathological scrutiny and deciphered in terms of masculine gaze and speech."[99]
The fascination with the female body as art and symbol extended also to Charcot's influence on his family. His wife and daughters were artists who worked with him in the family atelier. In 1892, Madame Charcot showed her work in the Exhibition of the Arts of Woman in Paris, contributing a large carved and decorated coffer, whose dark surfaces and fantastically painted inner panels suggested both the structure of the mind her husband had studied in hysteria—"a rational facade and an irrational interior"—and the image of woman promoted by the Central Union of the Decorative Arts and the Women's Committee of which she was a member.[100] As Debora Silverman has shown, "a prominent part of the Central Union program in the 1890s was the definition of interior space as distinctively feminine and the promotion of . . . woman as the queen and artist of the interior," in response to "the challenge of the femme nouvelle or 'new woman,' who was perceived as threatening to subvert women's roles as decorative objects and decorative artists."[101] Through the performances of Blanche Wittmann, the "Queen of Hysterics," and other famous hysterics at the Salpêtrière, Charcot too promoted women as artists of the interior, and paradoxically returned them to the status of decorative objects.
Even Charcot's contemporaries, however, were critical of the callous way that Charcot exhibited his hysterical stars and of his exposure of their secrets. In his antimedical satire Les Morticoles (1894), Leon Daudet caricatured Charcot as the voyeuristic neurologist "Foutange," who sadistically interrogates a hysterical girl: "And so, in front of two hun-
dred sniggering persons, these wretches must display their shame, their own, and their families' taints, and reveal their intimate secrets. . . . Foutange penetrates with diabolical skill to the depths of these stunted creatures."[102] Axel Munthe, a Swedish doctor practicing in Paris at the time, gave a vivid description of Charcot's Tuesday lectures, when "the huge amphitheatre was filled to the last place with a multicoloured audience drawn from tout Paris, authors, journalists, leading actors and actresses, fashionable demimondaines." The hypnotized women patients put on a spectacular show before this crowd of curiosity seekers. "Some of them smelt with delight a bottle of ammonia when told it was rose water, others would eat a piece of charcoal when presented to them as chocolate. Another would crawl on all fours on the floor, barking furiously when told she was a dog, flap her arms as if trying to fly when turned into a pigeon, lift her skirts with a shriek of terror when a glove was thrown at her feet with a suggestion of being a snake. Another would walk with a top hat in her arms rocking it to and fro and kissing it tenderly when she was told it was her baby."[103]
Feminists were indignant at Charcot's treatment of women, often comparing it to the atrocities of vivisection. Writing in the English antivivisectionist journal Zoöiphilist , one woman condemned the "no less disgusting experiments practiced on the lunatics and hysterical patients in the Salpêtrière. The nurses drag these unfortunate women, notwithstanding their cries and resistance, before men who make them fall into catalepsy. They play on these organisms. . . on which experiment strains the nervous system and aggravates the morbid conditions, as if it were an instrument. . . . One of my friends told me that she. . . had seen a doctor of great reputation make one unhappy patient pass, without transition, from a celestial beatitude to a condition of infamous sensualment. And this before a company of literary men and men of the world."[104] In an essay in the Revue scientifique des femmes (1888), C. Renoz accused Charcot of a "sort of vivisection of women under the pretense of studying a disease for which he knows neither the cause nor the treatment."[105]
Furthermore, the textual case studies of the hysterical women patients lend themselves to feminist interpretation of oppression and exploitation. Augustine, who spent five years as a patient at the Salpêtrière, is a particularly dramatic example. She came to the Salpêtrière at the age of fifteen in October 1875, suffering from pains in the stomach and convulsive attacks during the night which sometimes left her paralyzed. Although she had not yet begun to menstruate, Augustine had the appearance of a sexually mature woman. One does not have to search far for
the traumatic experiences that had precipitated her hysterical attacks. Beginning at puberty, she had been subjected to sexual attacks by men in the neighborhood, and at the age of thirteen, had been raped by her mother's lover, who had threatened to slash her with a razor if she did not comply. During the seizures which began immediately thereafter, she imagined that she was being bitten by wild dogs or surrounded by rats; sometimes she had hallucinations of the rapist with a knife. Treated with ether and amyl nitrate, Augustine spoke incessantly about her visions, but while the doctors recorded her words, they were not interested in the contexts of her experience. Instead she was repeatedly photographed in revealing hospital gowns demonstrating the various stages of grande hystérie . In 1879, her condition improved and she was taken on as a nurse in the hospital. But the respite was brief; by April 1880 she was once again having frequent attacks, to which the doctors responded with increasingly severe measures: ether, chloroform, strait-jackets, and finally, confinement in a padded cell. Although she was sufficiently improved to attend a concert on the Salpêtrière grounds in June, she used the opportunity to run away, but she was caught on the boulevard outside. Her health grew worse; in addition to the attacks, she injured herself in futile efforts at freedom. The last entry about Augustine is September 9, 1880: she "escaped from the Salpêtrière, disguised as a man."[106]
One cannot help rejoicing at Augustine's escape, and her male disguise seems like a coded statement about hysteria and gender; despite Charcot's insistence on the equality of male and female hysteria, men had an easier time getting out of the Salpêtrière. Victimized by sexual predators, she endured symbolic rapes at the hands of her doctors, who endlessly recorded her menstrual periods, her vaginal secretions, her physical contortions, and her sexual fantasies, but paid no attention to her sense of betrayal by her mother and brother, as well as by the men who had abused her.
In 1928, Augustine became the pin-up girl of the French surrealists, who reproduced her photographs to celebrate the fiftieth anniversary of hysteria, which they called "the greatest poetic discovery of the end of the nineteenth century." For Louis Aragon and André Breton, Augustine was the "delicious" embodiment of the sexy "young hysterics" they so much admired.[107] In 1982, Georges Didi-Huberman made Augustine the martyred heroine of his study of Charcot, the "masterpiece" of Charcot's hysterical museum.[108] She is also becoming an exemplary figure for feminists. I wrote about her in The Female Malady in 1985; a group of feminist scholars, choreographers, and dancers based at Trin-
ity College in Connecticut have produced a performance work about her called "Dr. Charcot's Hysteria Shows"; and a successful play, Augustine: Big Hysteria , was staged in London in 1991.[109]
But we need to be cautious about seeing Charcot as a misogynist. While he was famous for these performances with women, Charcot also took a liberal position on women's rights. The Salpêtrière journal Progrès Médical campaigned for women's admission to medical school, and some of Charcot's students and externs were women. The first French dissertation on hysteria by a female physician, Hélène Goldspeigel's Contribution à l'étude de l'hystérie chez les enfants (1888) was written under Charcot's supervision at the Salpêtrière.[110]
Indeed, one of the earliest histories of hysteria was Glafira Abricosoff's L'hystérie aux XVIIe et XVIIIe siècles (1897). Abricosoff had been a student of Charcot's and dedicated her book to the memory of "my illustrious master, J.-M. Charcot." As she explained in her introduction, "It is to him that I owe my medical knowledge, and it is, in a sense, out of gratitude for my dear departed master that I have wished to retrace the historical variations of a malady on which his brilliant perspicacity and his penetration have shed so much light.[111] Abricosoff's history makes no special case for women, but rather stresses the existence of male cases. Throughout her book Abricosoff drew attention to those writers such as Joseph Raulin who had observed and described male hysteria, and who had insisted that it could not be an exclusively female disorder. Her book is an example of one form of early feminist history of hysteria.
Another effort by a woman doctor to deal with hysteria was the book of Dr. Georgette Déga, who had studied at the medical faculty of Bordeaux. Déga attributed hysteria to the inadequacies of women's education. Hysteria, she wrote, was "the victory of the lower centers over the higher," and mathematics was the best discipline for hysterical women.[112] One can imagine that she believed medical training to be even better.
It is interesting to speculate on the reasons why Charcot's work on male hysteria did not have a lasting effect on medical discourse, why history has remembered Augustine and forgotten the hysterical men Char-cot described. In the British medical community, there had always been resistance to the idea of male hysteria, which had been camouflaged under other terminologies, organic explanations, and forms of denial and projection. As Micale concludes, "Charcot's hysterization of the male body in the 1880s was sharply at variance with dominant medical models of masculinity, and it ran counter to reigning Victorian codes of manliness. It required from Victorian physicians the application of an ancient and denigratory label to members of their own sex. And per-
haps most disturbing, it suggested the possibility of exploring the feminine component in the male character itself."[113]
Furthermore, Charcot's death in 1893 precipitated a long period of "dismemberment" of his work during which the concept of hysteria fell into disrepute, and some claimed that he had been a charlatan who coached his hysterical female patients in their performances or produced their symptoms through suggestion.[114] Men were omitted from the record. Even Pierre Janet reinforced the belief that all the hysterics were women when he remarked in his lectures at the Harvard Medical School in 1920 that "by a kind of international irony, people were willing to admit, after the innumerable studies made by French physicians, that hysteria was frequent only among French women, which astonished nobody, on account of their bad reputation."[115]
Ironically, the work of Sigmund Freud, Charcot's most famous student, also played a major role in the suppression of male hysteria after Charcot's death. Freud came to Paris to study at the Salpêtrière from October 1885 to March 1886. His original plan for the research trip was quickly changed, as he became overwhelmed by the personality, accessibility, and orginality of Charcot, who became a professional role model as well as a mentor. The ambiance of Charcot's clinic was very different from that which Freud had been used to in Berlin. Charcot was spontaneous, generous, and open to criticism and argument, and Freud found the democratic atmosphere both surprising and stimulating: "The Professor's work proceeded openly, surrounded by all the young men acting as his assistants as well as by the foreign physicians. He seemed, as it were, to be working with us, to be thinking aloud and to be expecting to have objections raised by his pupils. Anyone who ventured might put a word in the discussion and no comment was left unnoticed by the great man. The informality of the prevailing terms of intercourse, and the way in which everyone was treated on a polite footing of equality—which came as a surprise to foreign visitors—made it easy even for the most timid to take the liveliest share in Charcot's examples."[116]
Following Charcot's lead, Freud began by emphasizing that hysteria could affect both sexes, a position that was acceptable to his medical colleagues. On October 15, 1886, when he read his paper "On Male Hysteria" to the Vienna Psychiatric Society, several of the doctors present testified that male hysteria was already well known. Theodor Meynert, who publicly expressed skepticism about Charcot's symptomatology, later "confessed to Freud that he had himself been a classical case of male hysteria, but had always managed to conceal the fact."[117] In 1887-88 Freud translated Charcot's Leçons de Mardi , which contained most of
Charcot's case studies of men. In "Hystérie," an essay he published in a medical encyclopedia in 1888, he further condemned the "prejudice, overcome only in our own days, which links neuroses with diseases of the female sexual apparatus." Here he also noted the incidence of hysteria in both boys and girls, as well as in adult men. Although rarer in men than in women, hysteria, Freud argued, is more disruptive for men, because it takes them away from their work: "The symptoms it produces are as a rule obstinate; the illness in men, since it has the greater significance of being an occupational interruption, is of greater practical importance."[118]
In his work on hysteria, Freud took Charcot's theories to their logical extremes. Whereas Charcot had maintained that male and female hysteria had different causes, but similar effects, Freud argued that all hysteria came from traumatic origins. But the trauma did not have to be a railway accident or an injury in the workplace; it could be a disturbing sexual experience that had been forgotten and repressed. Furthermore, hysteria could be cured by having the patient recall and relive, or abreact, the originating trauma, whether by hypnosis or through the process of dream analysis and free association. The symptoms of hysteria, Freud noted, were created through a process of symbolization, and expressed emotional states.
Although he continued to acknowledge the existence of male hysteria, Freud's work on hysteria in Vienna concentrated on women. In contrast to Charcot, who examined, measured, and observed hysterics, but paid no attention to what they said, Freud and his colleague Joseph Breuer were the first to actually listen to hysterical women and to heed their complaints. In Studies on Hysteria (1895), he and Breuer worked out the fundamental technique of psychoanalysis. Most of their patients were middle-class Jewish women who found themselves imprisoned in traditional roles as dutiful daughters. Frustrated in their intellectual ambitions, expected to stay home and care for their brothers and father until they married, these bright and imaginative young women developed a wide range of symptoms—limps, paralyses, crippling headaches, and most significantly, aphonia, or loss of voice. By encouraging them to talk, to recount their dreams, to recall repressed memories of sexual traumas and desires, Freud and Breuer found that they could cure the women's symptoms. Studies on Hysteria thus seemed to lay the groundwork for a culturally aware therapy that respected women's words and lives.
In the case of Anna O., or Bertha Pappenheim, the connections between hysteria and feminism seemed particularly clear because after her analysis with Breuer in 1882, she went on to become a feminist
activist. She translated Mary Wollstonecraft's Vindication of the Rights of Woman into German, wrote a play called Women's Rights , and was the cofounder and director of the Judischer Frauenbund, the League of Jewish Women. In her hysterical seizures, Anna became unable to speak her native German, and instead spoke either Yiddish, which she called "the woman's German," or a jumble of English, Italian, and French. These linguistic symptoms have been read symbolically by feminist critics as the repression of women's language or its impossibility within patriarchal discourse. Dianne Hunter analyzes Pappenheim's hysterical symptoms as a linguistic protest against the German father tongue. In Anna O.'s case, "speaking German meant integration into a cultural identity [she] wished to reject," the patriarchy in which she was an immobilized daughter.[119] Hunter concludes that Anna O.'s hysteria was a "discourse of femininity addressed to patriarchal thought," signifying both through the body and through nonverbal language the protest that could not be put into words.[120] As she began to verbalize this protest in her conversations with Breuer, and to relive some of her dreams and hallucinations, Anna's symptoms were relieved. But she was not cured until she took complete control of language and subjectivity in her own writing. She remained ill for seven years after her treatment with Breuer, visiting sanatoriums during relapses. Anna O. recovered completely only with the publication of her first book, In the Rummage Store , in 1890. Rather than continuing her role as the passive hysterical patient, through writing she became one who controlled her own cure.[121]
By the turn of the century, the sympathy with women's intellectual and creative frustrations and the openness to their words so marked in Studies on Hysteria had become codified in the interests of Freud's emerging psychoanalytic system, a system that depended very much on domination over the patient. We see this increased rigidity in his famous case history of Ida Bauer, the young Viennese girl he called "Dora." Dora was brought to Freud by her father when she was eighteen. Intelligent and ambitious, Dora was stifled by the requirements of her role as the marriageable daughter of a bourgeois family, when she longed to go to the university and to have a career rather than a husband. Dora was a Viennese version of the New Woman of the 1890s, the feminist who seeks higher education and wishes to avoid marriage. Freud never met Dora's mother, whom he regarded as a boring case of "housewives' neurosis." Although Dora felt contempt for her mother's monotonous domestic life, it was the life for which she too was destined as a woman. Her mother was "bent upon drawing her into taking a share in the work of the house." Dora could find no support for her intellectual aspirations
from either parent. Although she had a governess who was "well-read and of advanced views," Dora believed that the governess was neglecting her and was really in love with her father. She arranged to have the woman dismissed. Afterward, she struggled alone with the effort to keep up her serious reading, and she attended lectures specially given for women. Her older brother, however, went off to the university, and later became a prominent Austrian politician.
Moreover, Dora was treated like a pawn or a possession by her father and denied the rights to privacy or personal freedom. He was having an affair with the wife of a friend, Herr K., who had attempted to seduce Dora when she was only fourteen, and she felt that "she had been handed over to Herr K." by her father in exchange for Herr K.'s complicity in the adultery. Professing to be anxious about her depressive state of mind, but really, Dora believed, afraid that she would betray his sexual secrets, her father then "handed her over" to Freud for psycho-therapeutic treatment. He wanted Freud to persuade Dora that her perceptions were simply adolescent fantasies. He hired Freud hoping for an advocate to "bring her to reason."[122]
As Jeffrey Masson observes, Dora had good reason to be upset: "She felt conspired against. She was conspired against. She felt lied to. She was lied to. She felt used. She was used."[123] Moreover, Freud's determination to label her as a hysteric did not depend upon the severity of her symptoms. Indeed, unlike the other women treated for hysteria by Breuer and Freud, Dora's "symptoms" were few and slight. She had a nervous cough, headaches, depressions. While he acknowledged that Dora's case was no more than "petite hystérie," Freud believed that the very ordinariness of her symptoms made her an ideal subject. Since he was committed from the start to the hysteria diagnosis, Freud interpreted all of Dora's behaviors and statements in accordance with his theories about the origins of hysteria in childhood sexual trauma and repressed desires. Many of his views, such as the belief that "gastric pains occur especially often in those who masturbate" and that masturbation was related to hysteria, are now seen as Victorian sexual superstition. But Freud's interpretations of Dora's fantasies, which have as little basis as his statements about her physical symptoms, are still accepted in psychoanalysis. He told her that she was really attracted to Herr K., in love with her father, and in love with himself. He ignored the appalling circumstances of Dora's family situation, and she finally broke off the therapy.
The conclusion of Dora echoes the endings of many Victorian novels about women: "Years have gone by since her visit. In the meantime the
girl has married . . . she had been reclaimed once more by the realities of life." In fact Dora's problems were not resolved by marriage, although Freud borrows it as a literary device to signify a happy resolution of the therapeutic plot. In the case histories of male patients, however, Susan Katz points out, these closed marriage plots are significantly absent; "the forms of Freud's case histories reflect his ideological positions toward women and men."[124] Similarly, Toril Moi reminds us, when Freud writes about Little Hans, he "never ceases to express his admiration for the intelligence of the little boy," while Dora's intelligence is represented as a form of neurotic resistance.[125]
In addition to its plot and themes, Dora's case had other literary characteristics. While Breuer, in the case of Anna O., commented on the broken language and multilingual nature of the hysteric's speech, Freud himself first drew attention in the Dora case to the fragmentary and discontinuous nature of the hysteric's narrative, and to the physician's responsibility for reorganizing it into a coherent whole. As he explained, hysterics like Dora were unable to tell an "intelligible, consistent, and unbroken" story about themselves. They repressed, distorted, and rearranged information; their volubility about one period of their lives was sure to be followed "by another period in which their communications run dry, leaving gaps untilled and riddles unanswered." And this incapacity to give an "ordered history of their life" was not simply characteristic of hysterics, Freud claimed; it was in a sense the meaning of hysteria. If the hysteric could be brought to remember what was repressed, and to produce a coherent narrative, she would be cured.
Thus the therapist's task was to construct such a narrative for the patient. Freud was confident that no matter how elusive and enigmatic the hysteric's story, the analyst could reconstruct a logical, scientific, and complete narrative. "Once we have discovered the concealed motives," he wrote, "which have often remained unconscious, and have taken them into account, nothing that is puzzling or contrary to rule remains in hysterical connections of thought, any more than in normal ones."[126]
In doing so, moreover, he had not only to fill in the gaps in the hysteric's own story but to overcome her resistance to his narrative interpretations. In order for the therapy to work, the hysteric had to accept and believe the narrative of the analyst. In his later papers on psychoanalytic technique, Freud described the process as one of combat in which "the patient brings out of the armory of the past the weapons with which he defends himself against the progress of the treatment—weapons which we must wrest from him one by one."[127] The analyst, Freud insisted in "The Dynamics of Transference," must win "the victory whose ex-
pression is the permanent cure of the neurosis."[128] But Dora was quite uncooperative in this regard. She flatly denied Freud's narrative embellishments of her story, would not accept his version of her activities and feelings, and either contradicted him or fell into stubborn silence. Finally she walked out on Freud by refusing to continue with therapy at all.
Freud viewed this resistance as the problem of her transference; Dora, he argued, had projected onto him her feelings of erotic attraction for her father and Herr K. and was punishing him with her rejection. If Freud is a reliable narrator, what happened in his exchange with Dora was that he succeeded in penetrating the mystery of her hysterical symptoms. In his terminology, he unlocked her case and exposed her sexual secrets. Unable to face the truth, Dora ran away from her therapy and remained sick for the rest of her life. Freud was a heroic pioneer who was disappointed in his efforts to help.
But if Freud is an unreliable narrator, a very different plot emerges. In this case, Dora is a victim of Freud's unconscious erotic feelings about her that affected his need to dominate and control her. It's significant that Dora has no voice in Freud's text, that we get nothing of her direct dialog, and that her historical and Jewish identity are both suppressed. Unlike Anna O., she never became a subject, only the object of Freud's narrative. His interpretations of her problem reflect his own obsessions with masturbation, adultery, and homosexuality. He never understands her story at all; he simply tries to bully her into accepting his version of events. His vaunted penetration of her secrets is really a kind of verbal rape. Dora's departure is then a heroic gesture of self-assertion and defiance. Her unhappy subsequent life was the result of Freud's failing her and leaving her defenseless in a social environment hostile to intellectual women. His interpretation of her story is more about himself than about her.
Contemporary analysts agree that for a variety of reasons psychoanalysis could only have been developed out of work with hysterics. "I think . . . that psychoanalysis had to start from an understanding of hysteria," Juliet Mitchell writes. "It could not have developed. . . from one of the other neuroses or psychoses. Hysteria led Freud to what is universal in psychic construction and it led him there in a particular way—by the route of a prolonged and central preoccupation with the difference between the sexes. . . . The question of sexual difference—femininity and masculinity—was built into the very structure of the illness."[129] Because hysterics formed strong and explicit transferences to their doctors, they were analyzable and thus were an ideal group from which to gen-
erate a psychoanalytic theory. Kurt Eissler has hypothesized that "the discovery of psychoanalysis would have been greatly impeded, delayed, or even made impossible if in the second half of the nineteenth century the prevailing neurosis had not been hysteria."[130]
What is left unsaid in these claims, however, is that only female hysterics offered these opportunities. The gender of the hysteric was crucial in leading Freud to the theory of sexual etiology of the neuroses. Had his patients primarily been men, had he written a case study of "Dorian" rather than "Dora," the history of psychoanalysis would look very different. The gender difference depends in part on Freud's reliance on cultural myths of masculine and feminine development in shaping his interpretation of hysteria.
At the turn of the century, hysteria was still popularly and medically conjoined with female deviance. In France, despite the "dismemberment" of Charcot, the hysteric was still seen in a theatrical context as a performer: "The hysteric is an actress, a comedienne," wrote P. C. Dubois in 1904, "but we never reproach her, for she doesn't know that she is acting.[131] The most vehement negative statements associating feminism with hysteria came during the militant suffrage campaign. "One does not need to be against women suffrage," the London Times editorialized in 1908, "to see that some of the more violent partisans of that cause are suffering from hysteria. We use the word not with any scientific precision, but because it is the name most commonly given to a kind of enthusiasm that has degenerated into habitual nervous excitement." In a notorious article called "On Militant Hysteria," Dr. Aimwroth Wright traced feminist demands to the "physiological emergencies" that constantly threatened women. Suffragist protest, especially when it involved working-class women, wrote the Daily Chronicle , was simply "hysterical hooliganism."[132] The representations of the militant feminist and the hysteric were conflated in the popular press, reflecting the view that nervous disorders were visible and detectable through study of the physiognomy. As Sander Gilman shows in chapter 5 in this book, the face of the hysteric had been presented as the chief sign of hysterical "difference" through the popularized images and photographs of Charcot's atelier, and through his studies of religious trance and possession in art as hysterical manifestations. Thus, the Daily Mirror wrote on 25 May 1914, the "hysterical ecstasy" of the suffragettes could be seen "unmistakably in the expression of the face."[133]
But with the outbreak of war and the abrupt end of the suffrage campaign, there were expectations that hysteria was dying out. "One doesn't dare any longer to speak of hysteria," wrote one doctor in 1914.[134] But
the Great War changed all this confident prediction with a great epidemic of hysteria among men. There had been scattered warnings of hysteria among soldiers before 1914. During the Boer War, the British surgeon C. A. Morris noted neurasthenic problems among the troops, which he attributed to privation, exhaustion, and mental strain. There were similar instances during the Russo-Japanese War of 1904-1905, and in 1907, the term "war neurosis" was introduced at the Congrès Allemand de Médicine Internationale.[135]
But World War I, in the words of Sándor Ferenczi, offered "a veritable museum of hysterical symptoms."[136] In all the European armies, war neurosis was extensive. In England by 1916, nervous cases accounted for as much as 40 percent of the casualties in the combat zone. By 1918 there were over twenty war hospitals for mental patients in the United Kingdom. And by the end of the war, eighty thousand cases had passed through army medical facilities. One-seventh of all discharges were for nervous disorders. "It is a wonderful turn of fate," marveled the British psychologist W. H. R. Rivers, "that just as Freud's theory of the unconscious and the method of psycho-analysis founded upon it should be so hotly discussed, there should have occurred events which have produced on an enormous scale just those considerations of paralysis and contracture, phobia and obsession, which the theory was designed to explain."[137]
The psychiatric theories that developed around war neurosis reflect the ambivalence of the medical establishment upon confronting hysterical behavior in fighting men. The first problem was in naming the disorder. When Dr. Charles S. Myers saw cases of amnesia, impaired vision, and emotional distress among British soldiers in France, he noted "the close relation of these cases to hysteria." But like doctors before him, Myers did not want to use the feminizing term "hysteria," and thus he argued that the symptoms could be traced to a physical injury to the central nervous system caused by proximity to an exploding shell. He christened the disorder "shell-shock." Later Myers would concede that the lack of evidence of any organic relation between exploding shells and neurotic symptoms made shell shock "a singularly ill-chosen term," but its simplicity, alliteration, and military sound made it the label that won out over such other alternatives as "anxiety neurosis," "war strain," and "soldier's heart."[138] The efficacy of the term "shell shock" lay in its power to provide a masculine-sounding substitute for the effeminate associations of hysteria, and to disguise the troubling parallels between male war neurosis and the female nervous disorders epidemic before the war. French doctors were also reluctant to identify war neuroses as hys-
teria, partly because of the internal struggle over the reputation of Char-cot. They called war neurotics pthiatiques , in Babinski's term, or, more harshly, simulateurs . Military authorities, indeed, regarded shell shock as a form of cowardice or malingering, and some senior army officers thought that patients should be court-martialed and shot.[139]
One of the striking aspects of shell shock was the class difference in symptoms; "shell-shocked officers tended to suffer from chronic anxiety states while men in the ranks generally suffered from acute hysterical disorders."[140] In the ranks, symptoms tended to be physical: paralyses, limps, blindness, deafness, mutism. In officers, symptoms tended toward the emotional: nightmares, insomnia, depression, anxiety attacks. Sexual impotence was widespread in all ranks. Explanations for the differences were class-based. Myers explained that "the force of education, tradition, and example make for greater self-control in the case of the Officer. He, moreover, is busy throughout a bombardment, issuing orders and subject to worry over his responsibilities, whereas the men can do nothing during the shelling but watch and wait until the order is received for an advance."[141] Some British doctors saw a one-to-one cause-and-effect relationship between the hysterical conversion symptom and the trauma that had caused it. According to Thomas Salmon, "A soldier who bayonets an enemy in the face develops a hysterical tic of his facial muscles; abdominal contractions occur in men who have bayonetted enemies in the abdomen; hysterical blindness follows particularly horrible sights; hysterical deafness appears in men who find the cries of the wounded unbearable, and the men detached to burial parties develop amnesia."[142]
There were two major ways of treating shell shock during the war, both designed to get men functioning and back to the trenches as fast as possible, and these treatments were differentiated according to rank. Shell-shocked soldiers were treated with the hostility and contempt that had been accorded hysterical women before the war. As in the nineteenth century, working-class men were linked with hysterical women as the antagonists of doctors. "The case of a psycho-neuropath," wrote Frederick Mott, "really consists of a mental contest, resulting in the victory of the physician."[143] Not only in England but in all European countries, shell-shocked ordinary soldiers were subjected to forms of disciplinary treatment, such as isolation, restricted diet, public shaming, and painful electric faradization, or shocks to the afflicted parts of their bodies. The treatments known as "quick cure," "queen square" (for the London hospital where it was practiced), "torpedoing," "torpillage," "manière forte," "terrorism," or "Uberrümplung" (hustling) were in fact
semi-tortures designed to make the hysterical symptom more unpleasant to maintain than the threat of death at the front. German physicians, for example, were divided between those who looked for the organic lesions of nervous trauma and those who believed the symptoms manifested a wish to escape that was independent of any specific traumatic incident. While in the short term these methods did terrorize patients into dropping their symptoms, when they were returned to the front, more disabling and permanent conditions emerged. H. Stern estimated that out of three hundred soldiers "cured" and sent to the front, less than two percent could be maintained.[144] After the war, a special Austrian commission was appointed to investigate the treatment of war neurotics in the Vienna General Hospital under Professor Julius Warner-Jauregg, who believed all shell-shock cases to be malingerers. In his report for the commission, Freud testified that "there were cases of death during the treatment and suicides as a result of it," but Warner-Jauregg was acquitted.[145]
More advanced psychiatrists adopted psychotherapeutic techniques in the treatment of shell-shocked officers, using abreactive or cathartic methods such as hypnosis, dream analysis, and free association. Officers were given various kinds of rest cures similar to those assigned to neurasthenics. When men were the patients, however, the rest cure had to be revised. Military doctors felt that intense activity was necessary for the restoration of masculine self-esteem. As H. Crichton-Miller advised, "Rest in bed and simple encouragement is not enough. . . . Progressive daily achievement is the only way whereby manhood and self-respect can be regained."[146] The treatment of isolation and rest, G. Elliot-Smith and T. H. Pear reminded doctors, had been developed in civilian life for "well-to-do women living in the lap of luxury" and could not be good for hardy military men.[147] Although the men of the first group of neurasthenic cases treated in English military hospitals were given the Weir Mitchell rest cure, it was later reported that these patients remained ill throughout the war.[148]
In dealing with shell shock, doctors seemed to have forgotten or ignored Charcot's work with male hysterics. They lacked a neutral vocabulary for discussing the cases in the contexts of masculinity; instead, shell shock was described as the product of womanish, homosexual, or childish impulses in men. W. H. R. Rivers had argued that war neurosis was a form of regression to an earlier form of development, either to animal instincts, primitive defenses, or infantile behaviors. Hugh Crichton-Miller also observed that, especially among the ranks, war neurosis produced "a condition which is essentially childish and infantile in its
nature."[149] T. A. Ross suggested that the training of a soldier "tended to make him regress to a childish attitude. . . . The soldier is above all things to learn what he is told at once without argument as a child is."[150] Wartime regression to a lower level of maturity also seemed to explain the proliferation of superstitions, magical beliefs, rituals, and rumors that, as Paul Fussell has shown, made the Great War a "new world of myth."[151]
When doctors dismissed shell-shock cases as malingerers or simulateurs , they were often hinting at the effeminacy that had always been part of the male hysteria diagnosis. Freudians shared this view. Karl Abraham, among the Freudians, was one who argued that war neurotics were passive, narcissistic, and impotent men to begin with, whose latent homosexuality was brought to the surface by the all-male environment.[152] In London, the tiny group practicing Freudian psychotherapy—David Eder, David Forsyth, and Ernest Jones—also argued for a sexual etiology for shell shock.
Their interpretations, however, were greeted with predictable outrage by such anti-Freudian members of the older generation as Charles Mercier. Reporting in The Lancet on a shell-shock patient, Forsyth described him as "a case of unconscious homosexuality with marked anal eroticism." Mercier made an angry response:
Unconscious pain, unconscious homosexuality, unconscious Oedipus complex, and other unconscious states of consciousness of the psychoanalysts. . . were a great mystery to me until I learnt from one of their victims what these expressions meant. This poor man had suffered many things for many months from many psycho-analysts, until at last he turned upon his tormentors . . . with these words: "It is true . . . that I now have these filthy thoughts, but it is you that have put them into my mind ."
The following week, Mercier was seconded by Dr. Robert Armstrong-Jones, who called for the professional outlawing of psychoanalysis. Then came a rebuttal from Forsyth, wondering how "those who still repudiate psycho-analysis and the sexual etiology of the neuroses can remain blind to what must long have been recognized by every thoughtful reader of your paper—namely, that the sexual instinct is clean and pure. It will not do nowadays to dress it up in mid-Victorian prejudices as a repulsive and disreputable bogie to frighten our intelligence."[153]
Some famous shell-shock patients, such as Siegfried Sassoon, Wilfred Owen, and Robert Graves, were indeed homosexual or bisexual. For most, however, the anguish of shell shock included more general but intense anxieties about masculinity and fears of homosexuality, even as
they refused to continue the masquerade of masculinity. What John Lynch has called "the exploitation of courage" in the Great War may be more accurately called the exploitation of manliness.[154] Soldiers were recruited and socialized through appeals to "traditional masculine virtues" and through promises of "the fulfillment of masculinity on the battlefield."[155] In combat, displays of manly stoicism and heroics were expected and encoded. As Paul Fussell notes in his glossary of the romantic vocabulary of World War I, to be "manly" meant not to complain.[156] Martin Stone points out that shell shock was thus generated by the military ethos of masculinity: "The soldier was encouraged to kill at the expense of unleashing infantile sadistic impulses that had previously been successfully repressed. He was encouraged to form close emotional bonds with other men and yet homosexuality was forbidden."[157] If the essence of manliness was not to complain, then shell shock was the body language of masculine complaint, a protest against the concept of "manliness" as well as against the war.
The impact of male hysteria in the field of psychological medicine was complex. On one hand, psychologists who had worked with shell shock challenged Freud's view that sexual factors were basic to the understanding of hysteria. Unable to revise a theory based on female hysteria in the light of male experience, these men instead argued that "shell shock had effectively 'disproved' Freud's theory of sexuality."[158] On the other hand, the Freudian establishment did not take the lessons of shell shock as a clue to expanding the theory of hysteria. Indeed, the theory only rigidified, with psychoanalysts insisting that the cause of hysteria had to be sought in infant traumas and repressed family experiences, rather than modifying their position to take immediate social factors into account.
The one or two voices who might have had something new and important to add to the conversation were prematurely stilled. W. H. R. Rivers was one of these. Rivers was a Cambridge psychologist and anthropologist who had studied in Germany, and who took an interest in the work of Freud. In his early fifties and unmarried when he became a military doctor, he found in the study of shell shock both a rich source of material for his theories of the unconscious and a personal involvement that changed the course of his career. The war, he wrote in Instinct and the Unconscious , had been "a vast crucible in which all our preconceived views concerning human nature have been tested."[159] In his therapeutic practice, Rivers relied on what he called "autognosis," or self-understanding, which involved the discussion of traumatic experiences; and reeducation in which "the patient is led to understand how his newly
acquired knowledge of himself may be utilized . . . and how to turn energy, morbidly directed, into more healthy channels."[160] Rivers's work was tragically abbreviated by his death in 1922.
Rivers may have been particularly effective as a therapist because he shared some of the characteristics of his patients. Speech disorders, especially stammering, were the most common neurasthenic symptom among officers and played a prominent role in the case studies of his patients.[161] Rivers, the son of a speech therapist who specialized in the treatment of stutterers, had stammered all his life, although his biographer speculates that he did not stammer in German. He was also sexually repressed and almost certainly homosexual.
In his postwar writings, Rivers explored the psychoanalytic issues of fear and anxiety which had come out of his war work at Craiglockhart Hospital. Proposing "suggestion-neurosis" as a term for hysteria, he argued that military training reinforced suggestibility, especially in private soldiers. In his view, "the symptoms of hysteria are due to the substitution, in an imperfect form, of an ancient instinctive reaction in place of other forms of reaction to danger." In explaining the mutism that was a frequent feature of shell shock, Rivers made connections to "the suppression of the cry or other sound which tends to occur in response to danger." He also began to apply to female hysteria, or as he called it, "the hysteria of civilian practice," some of the ideas about gender anxiety he had developed in working with men. "We have to discover why hysteria should be so frequent in women, and so rare in men, under the ordinary conditions of civil life . . .," Rivers wrote. "Women are always liable to dangers in connection with childbirth to which men are not exposed, while the danger element, real or imaginary, is more pronounced in them than in the male in connection with coitus."[162]
But theories about women's fears seemed less important by this time because after the war and the passage of women's suffrage in England and the United States, it was believed that female hysteria declined and even disappeared. Edward Shorter has noted that "the image of the dynamic 'New Woman' of the 1920s . . . plays an obvious role in the decline of the hysterical paralyses that once were quite common among young women: the New Woman, who rode motorcycles and smoked in public, simply did not develop a paralysis as a legitimate way of communicating her distress."[163] Other scholars have also pointed to social changes as determinants of the decline. With the gradual emancipation of women, they have argued, the social conditions that had produced hysteria were no longer operative. According to the psychoanalyst Monique David-Ménard, for example, "the repression of sexuality at the end of the nineteenth century" was the cause of hysteria; "through the
spectacular side of hysteria, women expressed what was impossible to say concerning sexuality."[164] If hysteria was the result of the sexual repression of the past, it made sense that it would vanish in our more liberated age.[165]
And indeed for much of this century, female hysteria seemed to be on the wane, as feminism was on the rise. It is striking as well that Freud's female disciples were virtually silent on the question of hysteria. It is not a topic in the works of Karen Horney, Melanie Klein, Anna Freud, or other members of the postwar generation. When a woman analyst, Elizabeth Rosenberg Zetzel, finally did deal with hysteria, she did not question Freudian assumptions and shibboleths. A student of Ernest Jones and D. W. Winnicott, Zetzel trained in psychiatry at Maudsley Hospital during 1938-39 and then served for six years during the war in the Emergency Medical Service and Armed Forces. Zetzel worked with hysterical soldiers and described her experiences in her first analytic paper, "War Neurosis: A Clinical Contribution," published in 1943. The three case studies, she later observed, served "as a model or blueprint" for her major work. Zetzel is quite approving of her male patients: "They were all happily married; they all had a steady work record; they had all shown ambition, social conscience, and a good capacity for sublimation."[166]
In contrast, when she worked with female hysterics in Boston after the war, Zetzel was much more critical. Although the women she called "true good hysterics" were "notably successful in the area of work," they had "failed to achieve a mature heterosexual relationship." Zetzel echoed Freud in her indifference to the double messages in the lives of her hysterical women patients, most of whom were intellectuals and students at various Boston universities. While she noted that "all of these patients have, in addition, been able to make and keep friends," she was certain that their difficulties with men came from their unresolved oedipal conflicts and penis envy, rather than from men's discomfort with gifted ambitious women.[167] Instead of pursuing the paradoxes of their lives, and the apparent uselessness of Freudian therapy in solving them, she focused instead on their analyzability and suitability for treatment. For, she wrote,
There are many little girls
Whose complaints are little pearls
Of the classical hysterical neurotic.
And when this is true
Analysis can and should ensue,
But when this is false
'Twill be chaotic.[168]
In such contemporary psychoanalytic writing by women as deals with hysteria, Freudian dogma has made it difficult for women analysts to accept hysterical symptoms in their male patients. Monique David-Ménard studied psychoanalysis at the Ecole Freudienne in Paris. In her practice, like most women analysts, she sees more women than men patients. David-Ménard claims not to know "what masculine hysteria is. Sometimes I say to myself when I hear a male patient who is very identified with a woman, 'Perhaps that came from hysteria,' but I always end up saying, 'It's not really that.'"[169] Her book Hysteria from Freud to Lacan (1983) is a densely argued philosophical comparison of Freud and Lacan, rather than a feminist reading of their work.
Yet a feminist interpretation of hysteria does not come naturally to women psychoanalysts or historians simply because they are women. David-Ménard, for example, has said in an interview, "I don't define myself as a feminist whether as a philosopher or as a psychoanalyst."[170] A feminist standpoint is situated within a particular cultural and intellectual framework, which offers an interpretative vocabulary and a support network for those who put it to use. Thus we need to read and evaluate women's writings about hysteria within their own historical context and with an understanding of the impact of gender at a particular moment for professional women.
Ilza Veith's Hysteria (1965) is an excellent case in point. According to Mark Micale, the book "established the 'standard' historical view of the subject for an entire generation of French, British, and North American readers."[171] Ilza Veith is one of the pioneering scholars of the history of medicine in the United States. Born in Germany in 1915, she studied medicine in Geneva and Vienna before coming to the United States in 1937. While she had hoped to become a plastic surgeon, "there was no thought in the thirties that a woman could receive a residency or assistantship in surgery."[172] Instead she trained with Henry Sigerist at Johns Hopkins and in 1947 received the first doctorate in the history of medicine in the United States.
For contemporary historians sensitized by feminist scholarship, Veith may seem indifferent to or unaware of the feminist questions in hysteria. She accepts wholeheartedly the Freudian view of hysteria and uses it as the resolution of the book, crediting psychoanalysis with the conquest of hysteria; it was the intensified understanding of the cause of hysteria by leading psychiatrists during this century, she wrote, that "contributed to the near-disappearance of the illness."[173] Roy Porter in chapter 3 questions Veith's uncritical acceptance of Freud and her blindness to the misogyny of prepsychoanalytic therapists like Carter. Mark Micale, too,
points out that although she "might have been expected to respond differently," Veith "maintained a studied silence on the intersexual aspects of the disorder."[174] Yet such a judgment carries its own assumptions about gender, ignores the circumstances in which the book was written, and misses the way that Veith, like many women writing about hysteria, felt pressured to avoid a feminism traditionally linked with the disorder itself.
Veith does indeed point out a number of the intersexual issues of hysteria, albeit in a restrained language. In one of the few metaphors of her book, she comments that "the scarlet thread of sexuality" runs throughout the "tangled skein" of the history of hysteria.[175] She thus presents the issue as sexuality rather than femininity, although the allusion to the scarlet letter (and to the great American heroine Scarlett O'Hara) suggests that this sexuality was in fact related to women. For much of the book, when Veith describes or quotes accounts that link hysteria with female sexuality and reproduction, she generalizes from them to discuss a more universal and ungendered "sexuality." With regard to the Greek origins of the term, for example, she notes that "the association of hysteria with the female generative system was in essence an expression of awareness of the malign effect of disordered sexual activity on emotional stability." Veith's careful neutrality extended also to her discussion of witchcraft and the witch trials. "It is evident from the forgoing that women were the chief targets in the witch hunts," she mildly observes, without speculating further on the clerical misogyny and profound male anxieties that were projected onto women during the witch trials.[176] Veith is similarly tolerant with regard to nineteenth-century medicine. She attributes Robert Brudenell Carter's hostility toward women to his "youthful impatience" with his female patients, and when she talks about the "punitive" aspects of Victorian treatment of hysterical women, calls them "misanthropic" rather than "misogynistic."[177]
In her most substantial discussion of sex roles and attitudes, however, Veith explains that the "manifestations of this disease tended to change from era to era quite as much as did the beliefs as to etiology and the methods of treatment. The symptoms, it seems, were conditioned by social expectancy, tastes, mores, and religion, and were further shaped by the state of medicine in general and the knowledge of the public about medical matters." Women created or reproduced hysterical symptoms in accordance with their age's ideas about femininity: "Throughout history, the symptoms were modified by the prevailing concept of the feminine ideal. In the nineteenth century, especially, young women and girls were expected to be delicate and vulnerable both physically and emo-
tionally, and this image was reflected in their disposition to hysteria and the nature of its symptoms. Their delicacy was enhanced by their illness, and as a result, the incidence of overt manifestations was further increased."[178] This comes very close to contemporary feminist analyses of hysteria.
Yet to judge Veith's work by contemporary feminist standards is to misunderstand the historical nature of gender ideology. Women historians and psychoanalysts of Veith's generation, including Elizabeth Zetzel, had a very different context than our own for their thinking about sexual difference, as several recent studies have illustrated. Joan Scott shows in her overview of American women historians that the post-World War II period saw the emergence of "a new discourse . . . that emphasized the masculine qualities of historians, associating them with the preservation of national traditions and democracy." Veith, like other women historians receiving their doctorates during this period, "had the further challenge of repudiating the disabilities assumed to come with womanhood."[179] Serious historians were judicious, unemotional, objective, impersonal. Similarly, in a series of interviews with women psychoanalysts who trained during the 1920s, 1930s, and 1940s, Nancy Chodorow found a very different gender consciousness from that of the 1980s operative in their views of feminism and psychoanalysis. Gender was not a meaningful or salient category to them; few had noticed discriminatory treatment; they had not thought about the conflicts between Freudian views of femininity and their own professional careers. But rather than accusing them of bad faith, blindness, or repression, Chodorow concluded that "gender-emphasis" or the "relative downplay of gender issues" are "not only objectively determined by a structural situation" but are also "subjective features of identity and culture." The "salience of meaning of gender" was not a historical constant but rather "a highly constructed product of one's time and place."[180]
In Veith's case, her position as a woman academic in a male-dominated profession may have led her to emphasize objectivity, neutrality, and indirection rather than to have taken a forceful and explicit feminist stand. Her book appeared in the last moments of calm before the storm of the women's liberation movement; sexual politics, however, was a term still to be invented by Kate Millett, and feminist scholarship did not yet exist.
Ilza Veith's autobiographical writings cast much light on the circumstances under which she wrote Hysteria and make clear that she was not unaware of sexism and its effects on the female psyche. In describing herself for Who's Who , she wrote, "In a long and severely handicapped
life I have had to live with chronic illness and pain. Thanks to my husband's endless patience and helpfulness, I have learned to accept what cannot be changed, and to change what can be altered. I have had a successful and highly satisfactory academic career in spite of endless obstacles that lie in the way of a woman scholar."
Some of the details behind this summation can be found in Veith's most recent book, Can You Hear the Clapping of One Hand? (1989). Here she describes the severe stroke that she suffered in 1964 while she was completing Hysteria . Just fifty years old, and having moved to California to take up a professorship at the University of San Francisco, Veith woke up one morning to find that her entire left side was paralyzed. She had been experiencing odd symptoms for over a month, including migraine headaches, disturbed vision, and olfactory hallucinations. Yet, despite her training as a medical historian, Veith had not consulted a doctor. Why? Because symptoms like these were frequently attributed in the medical literature to women with "hysterical personality." Veith was embarrassed to think that she herself might be a hysteric, and thus she ignored the warning signals of a serious stroke. Moreover, when she experienced paralysis of the left side—the side usually afflicted in cases of hysteria—Veith was persuaded that she was only hysterical and "deluded myself that if I admitted the hysterical nature of my hemiplagia to myself and others, it would simply go away." Patronized and subtly punished by doctors in the hospital when she refused to behave like a suitably ignorant and docile female patient, Veith learned more about sexism in medicine than has ever been revealed in her professional writing. She has never recovered the use of her left arm.
In contrast to Veith's emphasis on the ungendered nature of hysteria, contemporary feminist critics have argued that while "Freud's assertion that hysteria afflicted both men and women was a liberating gesture in the nineteenth century," the most liberating gesture for feminists today is to reclaim hysteria "as the dis-ease of women in patriarchal culture."[181] Some have argued for a continuity or even a similarity between hysteria and feminism. In the 1970s, it became an important strategy of radical feminism to redefine as terms of female power the hostile labels that had been attached to rebellious or deviant women through history. Thus early women's groups were called the Witches, the highly successful English feminist publishing company is called Virago, and a major French feminist journal was called Sorcières . Feminists saluted the hysterics of the past as heroines of resistance to the patriarchal order.
Dora has indeed become a paradigmatic figure for contemporary feminist criticism. Because she walked out on her psychoanalysis, she has
appeared to some as a defiant figure and precursor, what Mary Jacobus calls "the first feminist critic of Freud."[182] In her manifesto on women's writing, "The Laugh of the Medusa," Hélène Cixous takes Dora's story as a revolutionary discourse of the feminine, saluting Dora as "the indomitable, the poetic body . . . the true 'mistress' of the Signifier."[183] In The Newly-Born Woman (1975), Cixous took the position that hysteria was the "nuclear example of women's power to protest," and that Dora belonged to the pantheon of feminist history: "Dora seemed to me to be the one who resists the system, the one who cannot stand that the family and society are founded on the body of women, on bodies despised, rejected, bodies that are humiliating once they have been used."[184] Cixous's play Portrait de Dora (1976) tries to restore Dora's subjectivity and to reconstitute the other buried female figure in Freud's case history, the mother. Interpretations of Freud's case history are now legion, and the book In Dora's Case brings some of these feminist readings together.
It's important to note, however, that the fascination with Dora and hysteria has also been controversial within feminist theory. In her debate with Cixous in The Newly-Born Woman , Catherine Clement was more skeptical about the ultimate power of hysteria as a form of feminine subversion. She maintained that the hysteric is unable to communicate because she is outside of reality and culture—that, in Lacanian terms, her expression remains in the Imaginary, outside the Symbolic. Thus "hysterical symptoms, which are metaphorically inscribed on the body, are ephemeral and enigmatic. They constitute a language only by analogy." Hysterics should be classed not with feminist heroines, but with deviants and marginals who actually reinforce the social structure by their preordained place on the margin. Indeed, their roles are ultimately conservative: "Every hysteric ends up inuring others to her symptoms, and the family closes round her again, whether she is curable or incurable." With regard to Dora, Clément is cool and level-headed: "You love Dora, but to me she never seemed a revolutionary character."[185] In order to affect the symbolic order, or the material world, she argues, the hysteric must somehow break through her private language and act. Thus for Clément, the "successful hysteric" is one, like Anna O./Bertha Pappenheim, who becomes a writer, social worker, and feminist leader.
Overall it seems paradoxical that Dora, a notoriously unsuccessful hysteric, should have emerged as a feminist heroine in the 1970s, singled out by women writers and intellectuals who had been able to have the education and activity Ida Bauer sought in vain. It is bizarre to find Dora put forward as a feminist ideal and saluted by successful writers like Cixous, when Dora's own aspirations were to become a woman of learning,
perhaps a writer. Historically, Dora never found her own voice. While feminist artists and critics can attempt to re-imagine her story, we must recognize, with Clément, that her rebellion ultimately turned back on the self.
Dora's feminist power, paradoxically, is as a tragic literary figure. Feminist critics have taken up the concept of "hysterical narrative" to describe a story that is fragmented and incoherent, like Freud's case study; or the Lacanian concept of "hysterical discourse" to describe the metaphoric language of the body.[186] The impasse over Dora, feminism, and hysterical narrative, however, needs to be placed within the broader contexts of gender. As Toril Moi has pointed out, what Freud describes as the "incoherence" of the hysteric's story has less to do with the nature of hysteria or with the nature of woman than with the social powerlessness of women's narratives: "The reason why the neurotic fails to produce coherence is that she lacks the power to impose her own connections on her reader/listener."[187] How can Dora's story have plausibility for male ears in a culture when women's plots are so limited? When narrative conventions assign women only the place of object of desire, how can a woman become the subject of her own story?
In order to understand the gender issues in hysterical narrative, we need to have case studies of male hysterics by women analysts. Since "the dominant narrative of a male doctor treating a woman patient maintains the normative structure of men occupying positions of authority over women, the importance of the gender of the participants in the therapeutic dialogue is obscured."[188] Only in the past few years have women psychoanalysts begun to look at the problem of male hysteria and to examine issues of transference and countertransference between male patients and female therapists. Such studies require a "new narrative line that specifically addresses the relationship of boys to their mothers and the quite different meanings of power and sexuality for men and women in our culture."[189] When their case studies are published, we will be able to ask whether the body language, speech, and narrative of the hysteric is a discourse of femininity or a narrative imposed by the man who tells the story.
Other contemporary feminist theories locate in hysteria an attempt to give weight and meaning to aspects of the feminine which are despised or nonfunctional in the patriarchal social order. As Diane Herndl explains, hysteria "has come to figure as a sort of rudimentary feminism and feminism as a kind of articulate hysteria."[190] Juliet Mitchell describes hysteria as a "pre-political manifestation of feminism," an unconscious protest by women "in terms of their definitional and denigrated charac-
teristic—emotionality. If femininity is by definition hysterical, feminism is the demand for the right to be hysterical."[191]
This romanticization and appropriation of the hysteric nostalgically assumes that she is a heroine of the past. "Où sont-elles passées les hystériques de jadis," asked Jacques Lacan in 1977, "ces femmes merveilleuses, les Anna O., les Emmy von N.? . . . Qu'est-ce qui remplace aujourd'hui les symptômes hystériques d'autrefois?"[192] We might answer that the despised hysterics of yesteryear have been replaced by the feminist radicals of today, by contemporary women artists and poets, and by gay activists. In the popular mind, the pejorative association of feminism with hysteria and morbidity has not died yet. In 1983, for example, a controversy erupted in the Times Literary Supplement over the use of "hysterical" as a critical term for the poetry of Sylvia Plath and other "man-hating" feminist poets. Defending her position, Anne Stevenson wrote, "Hysteria is the very stuff of revolutions—and not only female revolutions . . . a passionate single-minded psychological condition which, immune to humour as to reason, fails to achieve the detachment essential for self-criticism."[193]
Moreover, those revolutions connected to gender and race continue to seem more "hysterical" than others. In December 1989, when the AIDS activist group ACT-UP and the abortion rights group WHAM staged a demonstration at Saint Patrick's Cathedral in New York City, interrupting the Sunday Mass, the New York Times editorialized: "Arguments over AIDS, homosexuality and abortion are not going to be advanced by hysterics, threats or the disruption of religious services."[194] What had been hysterical hooliganism in the suffrage campaigns was now attributed to other groups.
Black activists and radicals have also been stigmatized as hysterics and neurotics, leading to distrust of psychotherapy in the 1960s and 1970s among African-Americans.[195] Yet, from another perspective, Freudian insights can illuminate the experience of racism and its effects on the psyche. In his autobiography Dusk of Dawn (1940), W. E. B. Du Bois described the gradual effects of racial segregation on the black mind:
It is as though one, looking out from a dark cave in a side of an impending mountain, sees the world passing and speaks to it; speaks courteously and persuasively . . . [but] it gradually penetrates the minds of the prisoners that the people passing do not hear; that some thick sheet of invisible but horribly tangible plate glass is between them and the world. They get excited; they talk louder; they gesticulate. [Then some persons may become "hysterical."] They may scream and hurl themselves against the barriers. . . . They may even, here and there, break through in blood
and disfigurement, and find themselves faced by a horrified, implacable, and quite overwhelming mob of people frightened for their very own existence.[196]
Du Bois's description of the social origins of hysterical behavior in racism has relevance for other oppressed groups, particularly because it does not minimize the costs of hysteria. When unhappiness and protest go unheard for a long time, or when it is too dangerous for these negative emotions to be openly expressed, people do lose their sense of humor and their powers of self-criticism, whether they are feminists, people with AIDS, black activists, or East Germans, Rumanians, and Bulgarians. Anger that has social causes is converted to a language of the body; people develop disabling symptoms, or may even become violent or suicidal. "Hysteria," as Du Bois knew, is painful and disfiguring; rather than being a romantic ideal, it is a desperate behavior for women or men. It is much safer for the dominant order to allow discontented men and women to express their dissatisfaction through psychosomatic illness than to have them agitating for economic, legal, and political rights. It is thus that Dianne Hunter calls hysteria "feminism lacking a social network in the outer world."[197]
What about hysteria now? In 1986, Etienne Trillat declared, "Hysteria is dead, that's for sure. It carried its mysteries with it to the grave."[198] Phillip Slavney describes his study Perspectives on "Hysteria" (1990) as "perhaps the last book with hysteria in its title written by a psychiatrist." The terms "hysteria, hysteric and hysterical ," he argues, "are on the verge of becoming anachronisms."[199]
These announcements of hysteria's death are surely premature, for they neglect the cultural and symbolic meanings of the term, which cannot be obliterated by professional fiat. To write a history of hysteria at the end of the twentieth century we need also to recognize the correspondence that has developed between the two words. While for centuries the etymological link between "hysteria" and hystera dictated certain assumptions about female sexuality, today the correspondence between "hysteria" and histoire seems much more important. Above all, the hysteric is someone who has a story, a histoire , and whose story is told by science. Hysteria is no longer a question of the wandering womb; it is a question of the wandering story, and of whether that story belongs to the hysteric, the doctor, the historian, or the critic. The stories of race and gender in hysteria still remain to be told, and thus this book cannot be the final narrative, but is only another installment in the long and unfinished history of hysteria in Western civilization.
Five—
The Image of the Hysteric
Sander L. Gilman
The Function of the "Real" Image of the Hysteric in Defining the Nature of Hysteria
In the history of hysteria one image haunts the eye. It is an 1887 painting by André Brouillet of Jean-Martin Charcot presenting his pet hysteric, "Blanche" (Blanche Wittman), to the members of his neurological service at the Salpêtrière.[1] This portrait, clearly standing within the great tradition of Rembrandt's anatomies and echoing the 1876 portrait, Pinel Freeing the Insane , by Tony Robert-Fleury, which hung in the main lecture hall at the Salpêtrière, has one rather anomalous moment. (Brouillet [1824-1908] was after all a student of Gérôme, whose history paintings always hide a mystery.) All of Charcot's staff are men, with the exception of the one nurse, who is about to catch the somnambulistic patient. Only these two women are placed in such a manner so as to see the rear of the hall; all of the male figures have their backs (or sides) to the rear. And on the rear wall is an enlarged drawing by Charcot's colleague Paul Richer of the arc-en-cercle stage of "grand" hysteria. Charcot described this stage in an 1877 lecture: "The patient suddenly falls to the ground, with a shrill cry; loss of consciousness is complete. The tetanic rigidity of all her members, which generally inaugurates the scene, is carried to a high degree; the body is forcibly bent backwards, the abdomen is prominent, greatly distended, and very resisting."[2] In Broulliet's engraving, Richer literally sits at Charcot's right hand, sketching the patient who is replicating his own drawing.[3] Only the women see (and "know," that is, act upon) the image of the hysteric. Their image of the hysteric, both as patient and as health-care practitioner is con-
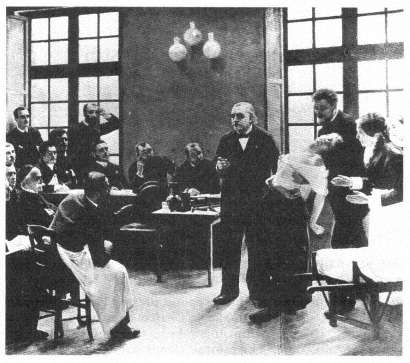
André Brouillet's image of Jean-Martin Charcot presenting his "pet" hysteric,
"Blanche" (Blanche Wittman), to the members of his neurological service at
the Salpêtrière (1887).
(Bethesda, Md.: National Library of Medicine.)
sciously formed by the visual image of the hysteric as created by a male physician.
The late nineteenth century understood such a pattern as the very model for knowing the world. Oscar Wilde suggested that we learn about nature from the work of art. "External nature," according to Wilde, "imitates Art. The only effects that she can show us are effects that we have already seen through poetry, or in paintings."[4] And, we might add, in photographs.[5] This is precisely what Blanche Wittman did at the Salpêtrière, as she learned from the representations of the hysteric how to appear as a hysteric.[6]
This image does not stand alone but is representative of a series of representations of the hysteric during the latter half of the nineteenth century. In the Jacques-Joseph Moreau de Tours 1890 image, Hysterics of the Charité on the Service of Dr. Luys , a wider range of representa-
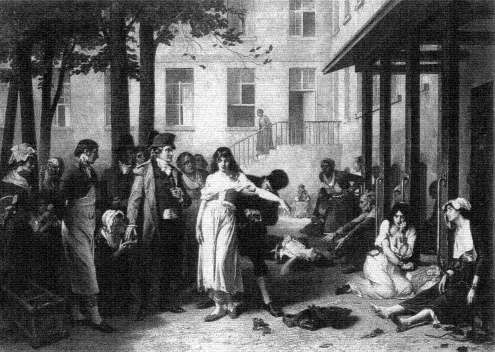
Tony Robert-Fleury's Pinel Freeing the Insane (1876), which hung in the
main lecture hall at the Salpêtrière.
(Paris: The Library of the Salpêtrière.)

Jacques-Joseph Moreau de Tours, Hysterics of the Charité on the Service of Dr. Luys (1890).
(Bethesda, Md.: National Library of Medicine.)
Photo courtesy Yale Medical Library.
tions of the hysteric is present.[7] Dr. J.-B. Luys (1848-1897), the author of an early photographic medical atlas,[8] stands to the rear of the room, with his white mutton-chop whiskers, as his female patients perform. (Moreau de Tour had himself been an intern under J.-É.-D. Esquirol, the creator of the first modern psychiatric atlas, at Charenton.[9] ) Luys had described and photographed the hysterics of the Salpêtrière for his 1887 study of the effects of hypnotism as therapy.[10] All of the patients in Moreau de Tours's image are seemingly oblivious to what immediately captures the eye of the viewer. On the rear wall of this ward, a permanent fixture of the room inhabited by the patients, is a chart recording the different phases of hypnosis, the stages that the patient is expected to pass through as she performs for her male audience. It is part of the world of the patient, a means through which to learn how to structure one's hysteria so as to make one an exemplary patient. Indeed, this is paralleled within the images that are so central to Jules Luys's own work, by the photographs of his pet patients, especially "Esther," taken by his brother Georges, which illustrate his-1887 study of the emotions of the hysteric.[11]
These patients are seen. There is no attempt to mask their identity. In the case studies of the period (even as early as Pinel) there is the use of initials or masked names. But in the visual images that Esquirol brings there is the assumption that the face (its structure or its expression) is so important that it does not need to be masked. But there is also the understanding, given the artistic license of the engraving and the lithograph, that there would be sufficient difference between the image of the patient and the final representation as to mask the patient's identity. (This is not always the case, as one can see in Georges-François-Marie Gabriel's admittedly unpublished image of Eugéne Hugo, the brother of the author.[12] ) The exception to this seems to prove the rule. In the Nouvelle iconographie de la Salpêtrière , Charcot's house organ, there are rarely images of patients that are intentionally masked, usually naked women, such as the image of a young anorexic female reproduced in the fifth volume.[13] (The Nouvelle iconographie de la Salpêtrière is not the only journal of its type. The Revue photographique des Hôpitaux des Paris flourished in the 1870s.)
The importance of the image of the hysteric represented as learning from the medical images that surround her can be gleaned from the following anecdote. In an account of Charcot's experiments with hypnotism in the British Medical Journal of 5 October 1878, Arthur Gamgee, Professor of Physiology at Owens College, Manchester, observed:
One of the patients was suspected of stealing some photographs from the hospital, but she indignantly denied the charge. One morning [Mr.]
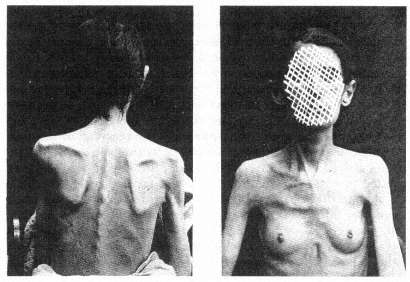
The masked image of the hysteric. From Louis Battaille, "Deux Cas
d'Anorexie Hystérique," Nouvelles Iconographie de la
Salpêtrière 5 (1892), plate opposite p. 277.
Photo courtesy Wellcome Institute Library, London.
Richer, after having made some experiments upon other subjects, found the suspected thief with her hand in the drawer containing the photographs, having already concealed some of them in her pocket. [Mr.] Richer approached her. She did not move; she was fixed—she was transformed into a statue, so to speak. The blows on the gong made in the adjoining ward had rendered her cataleptic at the very moment when, away from the observation of all, she committed the theft.[14]
It is Paul Richer, the creator of the archetypal image, the ornament of the lecture room in which rounds were held, who captures the "cataleptic" woman, a figure so mired in her internalization of his idea of the hysteric that she literally freezes as an incidental occurrence to the "experiment" taking place just beyond her ken.[15] This is not the world of Charcot in the role of Pinel "freeing the insane," whose image graced the public lecture hall in which the so-called Tuesday lectures took place. For here the "insane" patient is captured rather than freed by the intervention, no matter how incidental, by the physician. But why is this woman stealing photographs?[16] And whose photographs are they?
The photographs are those of the exemplary patient taken by Albert Londe, the head of the photographic service at the Salpêtrière, indeed

The hypnotized patient and the tuning fork. From Paul Richer, "Gonflement
du cou chez un hystérique," Nouvelles Iconographie de la Salpêtrière 2
(1889), plate 34.
Photo courtesy Wellcome Institute Library, London.
the first professional photographer to have a full-time appointment in any hospital in Europe. His job was to document the progress and manifestation of the patient's disease, to capture the stages and processes as they represented themselves on the visible surface of the patient, on the patient's physiognomy, posture, actions, as a means of cataloging the disease process. This Linnaean means of describing illnesses through their visible signs and symptoms (to use Jean-Martin Charcot's term, taken from the witch-hunting manuals of the Inquisition, the stigmata of the illness, from the stigmata diaboli that marked the body of the witch) dominated nineteenth-century European, but especially French, psychiatry. To describe was to understand, to describe in the most accurate manner meant to avoid the ambiguity of words, and to rely on the immediate, real image of the sufferer.
But the malleability of the symptoms in hysteria troubled the fin-de-siècle scientist. As Charcot noted, "Symptoms . . . have their destiny: Habent sua fata ." Symptoms, "after having enjoyed a certain degree of favour, doubtless on account of the theoretical considerations connected with [them, have] gone somewhat out of fashion . . ." But this is to be understood from the standpoint only of the physician-nosologist; from the standpoint of the patient, the symptoms are real, even if the patients are duplicitous: "You will meet with [simulation] at every step in the history of hysteria, and one finds himself sometimes admiring the amazing craft, sagacity, and perseverance which women, under the influence of this great neurosis, will put in play for the purposes of deception—especially when the physician is to be the victim. . . . It is incontestable that, in a multitude of cases, they have taken pleasure in distorting, by exaggerations, the principal circumstances of their disorder, in order to make them appear extraordinary and wonderful."[17] This deception is, for Charcot and his time, an absolute sign of the hysteric, and it can only be read correctly by a good diagnostician.
For hysteria must be "seen" to have observable symptoms, such as the changes of the skin or the wasting of the body, to be understood as a real disease: "Hysteria is a real disease, as real as small-pox or cancer, and . . . it has a physical basis, probably of a chemical nature, although this is yet very imperfectly understood."[18] As an early review of the first major journal from the Salpêtrière devoted to the visual representation of the insane noted, the camera was as necessary for the study of hysteria as the microscope was for histology.[19] This fantasy of realism captured the belief of the nineteenth century, both the doctor's and the patient's. For the doctor, the image is the patient, as it is for the patient. This search for an ontological representation of illness parallels the undertak-
ing of the exemplary fin-de-siècle scientist, Louis Pasteur, whose germ theory of contagious disease relied on the visibility of the germ for its power.[20] As Georges Canguilhem notes: "After all, a germ can be seen, even if this requires the complicated mediation of a microscope, stains and cultures, while we would never be able to see a miasma or an influence."[21] To see the patient means to develop the technique for seeing, a technique that is "scientific"; the patient, in turn, as the object of the medical gaze becomes part of the process of the creation of an ontological representation of the disease, a representation that is labeled hysteria. This does not deny the underlying pathology of the hysteric; it reflects only the meaning attributed to the symptoms created to represent the pathology as a disease.
One can speculate on whether the official nosology of American (and increasingly, world) clinical psychiatry, the DSM-IIIR (soon to be DSM-IV), in its restructuring of hysterical neurosis into conversion disorder, dissociative disorder, histrionic personality disorder, and brief reactive psychosis, did more than relabel an existing disease or whether these new labels are the self-conscious description of the manifestation of the hysteric in the 1980s.[22] But at least the compilers of DSM-IIIR saw their undertaking as the description of the disease, rather than as the search for its etiology. This does not mean, however, that the physician and the patient place any less reliance on the meaning of these definitions in order to shape our contemporary sense of the patient. How many patients today learn to have "conversion disorders" or "factitious disorders with psychological symptoms" from the medicalized world in which they—the sufferers from the dis-ease of hysteria—must function?
For the patient knows how to be a patient, as we see mirrored so well in André Brouillet's image of Charcot, only from the representation of the way the physician wishes to see (and therefore to know) the patient as the vessel of a disease, not any disease, but the disease of images and imagining, hysteria. It is this shared sense of the importance of the image, for the doctor as well as for the patient, which is reflected in the image of the hysteric.
Toward a Theory of "Realistic Representation" in Nineteenth-Century Thought
In my work on Hugh W. Diamond's mid-nineteenth-century introduction of photography into the treatment of the mentally ill, I was struck by the fact that Diamond believed he could cure at least some of his patients by exposing them to photographs of themselves. The "realism"

Hugh W. Diamond, a portrait of a case of "religious
melancholy."
(London: Royal Society of Medicine.)
of the photograph was assumed to have a therapeutic function because of its mode of representation. Such a view underlined the importance of all images for the alienists of the nineteenth century. Thus there was a constant striving for verisimilitude, not only for nosological purposes (that is, in order to categorize the illness) but also for therapeutic reasons. Seeing one's own difference provided the "healthy" aspect of the mind with the juxtaposition between the "normal" and the "abnormal." The desire to see the absolute border between these states encouraged the nineteenth-century scientist to seek out and "see" the difference. As Friedrich Nietzsche put it (paraphrasing Claude Bernard): "It is the
value of all morbid states that they show us under a magnifying glass certain states that are normal—but not easily visible when normal."[23] Disease itself is seen as a means of "seeing" the normal. And normality is an unself-conscious state like that of observers, who are never aware of that role until they self-consciously begin to think of themselves as observers through their training as "scientists" and, therefore, become aware of the meaning attached to the act of seeing.
But it was only with the introduction of the photograph that the power of such contrast—for the patient—was clearly articulated. Diamond stated in his 1856 paper "On the Application of Photography to the Physiognomic and Mental Phenomena of Insanity," read before the Royal Society, that "there is another point of view in which the value of portraits of the insane is peculiarly marked—viz. in the effect which they produce upon the patients themselves—I have had many opportunities of witnessing this effect—In very many cases they are examined with much pleasure and interest, but more particularly in those which mark the progress and cure of a severe attack of Mental Aberration."[24]
Diamond's course of treatment was straightforward. He presented his patients with images of themselves that seemed to startle them into an awareness of their madness, because of the radically realistic image of them as demented. Through this confrontation with a "realistic" image of their insane physiognomy, they began to realize their own altered perception of reality. In his talk, he presented the case of "A. D., aged 20," whose "delusions consisted in the supposed possession of great wealth and of an exalted station as a queen."[25] He photographed her. Her reaction to the images she saw reflected the "startle" effect inherent in the newness of the medium of photography: "Her subsequent amusement in seeing the portraits [of herself in various stages of her illness] and her frequent conversation about them was the first decided step in her gradual improvement, and about four months ago she was discharged perfectly cured, and laughed heartily at her former imaginations."[26] If we can extend Diamond's argument, we can suppose that the nineteenth-century alienist saw the patient-observer as sharing the implication of the photographic image, the startle effect that accompanied the introduction of this new medium of representation.
In further work on the use of photography as a means of psychotherapy, I discovered that other alienists of the period, such as Sir William Charles Hood, the director of the Bethlem Asylum, undertook similar applications of photography. I initially extrapolated certain broader generalities about the reaction to the photograph by the first generation to see photographs after their invention in 1839. (This first period oc-
curred a full decade later in Great Britain than in the rest of Europe because both Daguerre's and Fox Talbot's methods of fixing images were under patent during the 1840s only in Great Britain. In the rest of Europe, the daguerreotype at least was in the public domain by the early 1840s.) I believed that the earliest photographs were such a radical mode of representing the reality of the self as different that they had some type of psychological shock effect. That is, they so disoriented patients as to where the already distorted line between what is real or unreal lay, that patients were forced to reexamine their own psychological confusions. I was convinced, however, that it was the perception of the self, the image of the self as the mad person, which caused the "startle" effect.[27] And that was the radical difference of the photograph, as perceived by those in this first generation to see photographs.
George S. Layne, in an essay in 1981, contradicted this finding, while still supporting my sense of the radical break with existing models of perception.[28] He uncovered the fact that the brothers William and Frederick Langenheim provided lantern slides for the "moral" treatment of the patients in the Philadelphia Hospital for the Insane a year before (1851) Diamond exposed his patients to their own images in the Surrey County Lunatic Asylum. But the Langenheim images were not of the patients, but rather were general images such as landscapes and street scenes, yet they had shock value in treating the patients. So it seemed to be not the image of the self but the radical newness of the medium that caused the "startle" effect.
One of the reasons that the "startle" effect was so pronounced as to be useful in therapy in the public asylums was that the working-class inmates of the asylums did not share the bourgeois and upper-class tradition of seeing and understanding visual objects which had developed out of the "realistic" philosophy of Enlightenment art. Even prints and engravings, understood as aesthetic objects, had been, for the most part, out of the financial reach of the proletariat. Theirs was a world with limited access to images—the absence of cheap illustrated newspapers (soon to appear in Great Britain in the middle-class form of the Graphic and the Illustrated London News ) meant that their world of images was the crude broadside with its lithographed (or indeed woodcut) image. But the middle and upper classes had a tradition of seeing and speaking about art, at least in terms of the reproduction of the work of art as engravings (such as the Broulliet and Moreau de Tours images). For them, even if the "startle" effect occurred (or perhaps because it occurred), the objects recorded were understood in terms of a historical continuity of perceiving aesthetic images. And, indeed, the entire history
of early photography is full of references to the continuity of the photograph with earlier modes of representation. A letter from Elizabeth Barrett Browning as late as 1843 reflects both the "startle" effect and the language in which it was articulated:
My dearest Miss Mitford, do you know anything about that wonderful invention of the day, called the Daguerreotype?—that is, have you seen any portraits produced by means of it? Think of a man sitting down in the sun and leaving his facsimile in all its full completion of outline and shadow, steadfast on a plate, at the end of a minute and a half! The Mesmeric disembodiment of spirits strikes one as a degree less marvellous. And several of these wonderful portraits . . . like engravings—only exquisite and delicate beyond the work of the engraver—have I seen lately—longing to have such a memorial of every Being dear to me in the world. It is not merely the likeness which is precious in such cases—but the association, and the sense of nearness involved in the thing . . . the fact of the very shadow of the person lying there fixed for ever! It is the very sanctification of portraits I think and it is not at all monstrous in me to say what my brothers cry out against so vehemently . . . that I would rather have such a memorial of one I dearly loved, than the noblest Artist's work ever produced.[29]
Such photographic images were perceived as a clear continuation of other, older means of the reproduction of images. Elizabeth Barrett Browning's vocabulary is initially taken from that of one of the fine arts, engraving. She is startled by the perceived realism of the image, but she places it within the Victorian model of progress in the reproduction of visual images. The photograph seems to her to be "exquisite and delicate beyond the work of the engraver." And yet her perception of this new medium is such that it draws on the science of the day, mesmerism, with its own "startle" effect, as its initial analogy. And, indeed, the "art" of engraving is the most highly mechanical of all the fine arts of the period. These associations, first between the various modes of creating and reproducing images, and then between the aesthetic and the scientific, dominate the discourse of the first generation to view photographs.
Alexander von Humboldt, in a letter dated 7 January 1839 to the Duchess Friederike von Anhalt-Dessau, stresses this admixture: "Objects that express themselves in inimitable fidelity, light fixed by the art of chemistry to leave enduring traces within a few minutes and to circumscribe clearly even the most delicate parts of contours—to see all of this magic (admittedly without color) . . . certainly speaks incontrovertibly for reason and the power of imagination."[30] The mix of the language of science and the language of art is clear here with Humboldt's
perception of the photograph as the product of a science rooted in the imagination, but producing aesthetic objects (which he sees as flawed in part because of their colorlessness). Edgar Allan Poe, in one of his 1840 essays on the daguerreotype, makes many of the same verbal associations.[31] Thus the articulation of the "startle" effect in the middle and upper classes points to a confusion in the vocabulary in which this effect was to be addressed: Is it a continuation of the older forms of representation (and therefore to be considered "art") or is it a new and different mode of representation (and therefore to be considered "science")? What all were agreed upon in that first generation was that the images were "real." It was that "realism," prefigured by the aesthetic theory of the Enlightenment, which framed the perception of the photograph and which provided the vocabulary in which the "startle" effect was articulated. The presence of the "startle" effect would seem to be a universal among those individuals exposed to the first photographs. It is no surprise that the first photographer-physicians, such as Hugh Diamond, who incorporated the "image" within their mode of treatment, were also constrained to see (and to know) the photograph in terms of its "startle" effect.
It is with the general understanding of the function of the photograph that the aesthetic tradition of representing the mentally ill begins to be submerged and there evolves a sense of collaboration—already implicit in the meaning given to the realism of the photograph by doctor and patient alike—about the educative function of images. But it is in the different function of images of the patient and images of the physician that the application of this problem in the history of seeing is to be found. For with the craze for the carte-de-visite, which began in the 1850s, all gentlemen and gentlewomen had to have their pictures taken. Indeed, as I have argued elsewhere, the very absence of photographs of those who understood themselves to be part of the world of society is an interpretable fact.[32] How very different for those whose images are taken from them, the mentally ill, the criminal, the maimed. For their images do not grace the storefronts of the photographers; their images become ersatz representations of the nosology that they represent. These "real" images, these images that startle, are images of the disease and not of the patient. And again it is the movement from the aesthetic to the real, from the artistic to the therapeutic, from the image of the patient to the definition of the patient's reality that lies at the center of this world of images. The image is the essence of the patient, it gives the patient form. The patient, or at least the presentation of the patient, quickly becomes the creation of the physician's sense of the cor-
rectness of the patient's disease. With the hysteric, the very nature of the illness provides for the patient a demand for the forming touch of the authority, for the control implicit in the worldview that generates "real" images. For hysteria is the classic disease of the imagination—not of the uterus—as Charcot (and then Freud[33] ) understood. But the shaping of the imagination through the "realism" of the photograph lies behind the pilferage described in Gamgee's account of the Salpêtrière incident. For can we imagine that the patient in the Salpêtrière is stealing back her identity, her sense of self, in removing the image of the hysteric from the grasp of the physicians?
Medical and Aesthetic Models for the Representation of the Hysteric
The image of the hysteric does not simply arise out of Jean-Martin Char-cot's personal interest in the visual representation of the hysteric at the Salpêtrière.[34] Charcot does not invent the act of "seeing" hysteria. His own interests in capturing the visual aspect of his patients combined with his own perception of his hysterical patients to record the image of his patients as early as his first years at the Salpêtrière, the 1860s. Charcot comes to his task of understanding his patient with a long personal need to see and represent the patient. But his view is not unique, it is part of a long-standing European tradition of representing the insane, into which the image of the hysteric must be fitted. Indeed, it is a tradition which is as much popular as it is scientific. For Moreau de Tours's image provides us with another context for the structuring of the hysteric—the world of the hypnotizable patient, the image of the mesmerizable female. For hysteria, from the eighteenth century, is a disease of the imagination, not a disease of the womb.
The image of the patients of the Viennese physician Franz Anton Mesmer and his students during the 1780s provides one of the keys to the representation of the hysteric at the end of the 1800s.[35] After his arrival in Paris in the winter of 1778, the representation of Mesmer becomes part of the tradition of representing the insane. In a contemporary cartoon reflecting a mesmerist session, it is not merely that the quack physician is indicated by his ass's ears. More important is that the patients gathered about the mesmerist's "tub" are represented in the traditional pose of the melancholic (with head on hand on knee) and the lovesick (swooning in the chair). The latter becomes identified retrospectively with the arc-en-cercle position of the hysteric (in some of the historical writing of the mid-twentieth century), because of the associa-
The image of the mesmerist.
(Paris: Bibliothèque nationale: Cabinet of Prints.)
tion of the hysteric with the sexual (in many different ways), while the melancholic vanishes from any consideration as a forerunner of the image of the hysteric. The visual representation of the mesmerist and the patient are all means of limiting the scope of the diseased to the identifiable individual.
The suppression of the political radicalism associated with one of the most influential groups under Nicolas Bergasse after the French Revolution meant that there was a general tendency to see the mesmeric patient as an asocial being who only shammed illness out of a sense of social uselessness. Likewise, the mesmerist was understood, not as a force for change, but as a quack. The cartoons of the patient and the physician from the 1780s had already carried that message. In one such image a mesmeric healer, wearing an ass head, begins to mesmerize a young, female sufferer.[36] Her position echoes the association of disease and sex-
The "ass-mesmerists."
(Paris: Bibliothèque nationale: Cabinet of Prints.)
uality in the arc-en-cercle position of the grand hysteric, as she begins to lie back in her chair as her moral seduction begins. Mirrored in the background is the representation of the sexual exploitation of the female patient by the mesmerist, warned against in the secret appendix to the Report of the Royal Commission on Mesmerism. Here the physician is as hypersexual as the patient.
In another image the conceit of the ass-mesmerists is repeated.[37] They are being driven out of the scene by the shining truth of the report of the Royal Commission held by Benjamin Franklin. What is central to this image is that the mesmerists are represented as a compound sign. They are both madmen and devils. They are viewed as a parody of the images of the demonic evil spirits released from the mad as healed by Christ (and his saints) in the traditional iconography of madness. Here the split-hoofed image of the devil as well as the broomsticks associated with flying witches are employed. But this image of the healer is also that of the insane, for the split-hoofed figure is brandishing a scourge, which is one of the traditional icons of the insane. The figure of the arc-en-cercle in the representation of the patient is here reversed. The blindfolded, naked patient is seen in the closed mesmeric tub, not arched but collapsing inward. This can be seen as antithetical to another image of the mes-
merist healing process, the circle of "magnetized" hands, in which a seemingly unconscious female is represented in the left foreground; balancing the portrait of Mesmer, the healer, in the right foreground.[38] The imagery of this representation is tied to an understanding of the "meaning" of mesmerism and the mesmerist treatment in the course of the nineteenth century. The disrepute of the mesmerist, labeled as insane or demonically possessed, and thus in need of the sort of control represented by Franklin, Antoine-Laurent Lavoisier, and the Royal Commission, is carried over into the disrepute associated with the very naming of the treatment. The image of the physician, as well as the patient, is drawn into question in these associations. Such images remain associated with the idea of the hysteric through the visual representation of the patient.
The mesmerism patient is understood at the close of the nineteenth century to be one of the precursors of the fin-de-siècle hysteric. The image of the physician, as in the portraits of Charcot and Luys, must be quite different from that of the mesmerist; it must be separated from the image of the quack. Rather this image must be associated with the heroic image of the alienist, the image of Pinel as a force of social change (like Franklin). Merely changing the label of the mode of treatment from mesmerism to hypnotism or electrolization was not sufficient. The very relationship between the hysteric and the physician must be merged into the highest level of institutionalized medical representation—that of the image of science in the science of creating images.
The image of the hysteric in the medical literature of the nineteenth century is an essential image of deviance. It is an image that is taken—at least in its most radical form—out of another context. The central image of the hysteric, the essential attitudes passionnelles in Charcot's vocabulary of images, is a sign of quite a different disease—tetanus. The arc-en-cercle stage of Richer's image of grand hysteria (and its retrospective reading of the image of the swooning mesmerist patient) was consciously modeled on an image taken from the literature on the representation of anatomy and pathology for artists, rather than from a purely medical source.[39] Taken from the second edition of Sir Charles Bell's Essays on the Anatomy and Philosophy of Expression (1824), this image is rooted in a specific understanding of the nature of medical semiotics. Bell notes:
I throw in this sketch to remind the painter that in convulsion , although there may appear to him an accidental and deranged action of the muscular frame, there is no such thing in nature. It is a disease he is representing, which has definable symptoms, and it will ever present itself with the same characters.[40]
The range of the positions of the hysteric. Given best in Paul Richer, Études
cliniques sur le grande hystérie ou hystéro-épilepsie
(Paris: Delahaye & Lecrosnier, 1881), plate 5.
(Bethesda, Md.: National Library of Medicine.)

The opisthotonic position. From Sir Charles Bell's Essays on the
Anatomy and Philosophy of Expression (London: John Murray, 1824), p. 101.
(Bethesda, Md.: National Library of Medicine.)
Bell's observation may well hold true for tetanus, but the opisthotonic position chosen by him to represent the unalterability of the relationship between sign and causation is adapted by Charcot and later by Freud and given specific meaning in regard to the representation of the illness of the nerves and mind in the hysteric. One must note that Charcot is not the first "modern" scientist to call upon tetanus as his ontological representation for "seeing" the body. John Brown (1735-1788), in evolving the concept of the irritability of the muscles from the work of Albrecht von Hailer, argues that health and disease are not at all different states since the forces that produce each have the same action.[41] His example is a comparison of the normal contractions of the muscles and the pathological appearance of the opisthotonus in tetanus. The opisthotonus is one of the most striking manifestations of any disease. But it is also an almost infallible sign for the physician, since its outcome is almost surely negative. In a world in which the power of the physician lay, not in the ability to cure, but in the ability to foretell the course of a disease, the meaning of this sign for doctor and patient alike was clear. Thus Brown, Bell, and Charcot all call upon the image of the opisthotonus as a sign of the visual interpretability of disease and, therefore, the power of the physician's insight over the disease. At the end of the nineteenth century there was still a clear need to provide differential diagnosis between tetanus and hysteria for the practitioner. Among other signs, tetanus was described as presenting "persistent rigidity with
tendency to opisthotonos . . ." while hysteria presented "opisthotonos persistent, and intense rigidity between convulsions."[42] In seeing the patient, little distinction was made between organic and functional deficits.
Charcot in seeing the hysteric evolves his own system of representing the disease. He sees the hysteric as suffering from a weakness of the nerves and the disease as being caused by a trauma (such as an accident or violence). Thus the hysteric patient was predisposed to the disease—at least once he or she was exposed to some traumatic event. It is clear that Charcot evolved this view through his treatment of the patients at the Salpêtrière—epileptic and hysterical female patients who were as different from him (and his class) as was possible.[43] The counterargument to this view was evolved by John Hughlings Jackson, whose initial interest was sparked by his wife's epilepsy. This view was one of universal susceptibility. Seeing the disease as a pattern of the dissolution of the higher functions of the nervous system through the presence of a lesion, Jackson understands the symptoms of the hysteric as signs of the lower (and therefore earlier) functions of the nervous system. This evolutionary model sees the symptoms of the hysteric as signs of the structure of the more primitive psychic organization. Both views—the view that calls upon trauma and biological predeterminism as well as the view that calls upon the model of the nervous system being layered to represent the evolutionary history of the mind—come to be absorbed in the fin-de-siècle debates about hysteria.[44]
As early as 1888, Sigmund Freud calls up the figure of the opisthotonus in the context of attacks of hystero-epilepsy.[45] He continues this argument as late as 1908 when he understands coition to be a form of "minor epilepsy." For "a hysterical attack is the reflex mechanism of the act of coition—a mechanism which is ready to hand in everybody, including women, and which we see coming into manifest operation when an unrestrained surrender is made to sexual activity."[46] Thus Freud explains the opisthotonus as the antithesis of the embrace—the internalized enactment of coitus. But this is an image that does not vanish, but is rather consistently transmuted.
Freud uses the image of the opisthotonus as the antithetical image to coitus within his initial reworking of Charcot's nosological criteria. Seeing the reality of the opisthotonus as the key to the somatic nature of hysteria meant understanding the concept of trauma as existing in real experience rather than in fantasy. Sándor Ferenczi, in his clinical diary of 1932, can call upon "a case in which in relaxation ('trance') opisthotonic positions did appear: when contact could be established with the patient, she reported that the position was a reaction to a feeling of
painful excitation in the genital passage, which the patient described as painful hunger: in this position, psychic unpleasure and defense against ardent desire are simultaneously represented."[47] Ferenczi traces this reaction formation back to the actual seduction of the female child by her father. All of these references—and Charcot's own vocabulary of images, especially the opisthotonus—stem from a vocabulary of images which clearly (at least in the medical literature of the nineteenth century) defined the line between the healthy and the diseased. The opisthotonus is a sign of the presence of a disease—whether a form of hysteroepilepsy or a signifier of pathological sexuality or a real seduction.
There is a one-to-one relationship between the sign and the meaning. Given Freud's own complicated formulas for the generation of symbolic meaning, already documented in detail in his 1900 Interpretation of Dreams , it is striking that in returning to the subject matter of the hysteric, which he and Josef Breuer had begun to explain in 1895 as the result of the suppression of real traumatic events—that is, precisely the sort of seduction of children by adults in authority (parents) to which Ferenczi, quite opposed by Freud, returns some three decades later—he reverts to a pattern of explanation that relies on the meaning of the visual image.
The association between images of the tetanal opisthotonus is in no way limited to the neurological literature coming out of the Salpêtrière or out of the Viennese schools of psychoanalysis. During World War I, Arthur F. Hurst reflected on the relationship between the hysterical etiology of "war contractures" ("battle fatigue" or posttraumatic neurosis) as opposed to those contractures which have their origin in a localized infection.[48] For Hurst the question of the differential diagnosis of hysterical contracture (here localized in contrast to the full-body opisthotonus) as opposed to localized tetanus is questionable. It is clear that in time of war the duration of the cure—a "single sitting by persuasion and reeducation" in the first case or "months of treatment" in the latter—would place emphasis on seeing the majority of such cases as quickly healable. The assumption in Hurst's presentation is that the confusion between real (i.e., somatic) and hysterical contractures advocated by continental neurologists such as Josef Babinski and Jules Froment marks a faulty distinction between a biological and a psychological illness.[49] Such an argument would be parallel to Freud's attempt to collapse the distinction between real epilepsy and hysterical epilepsy. The images of the case of tetanus as opposed to the hysteric are, however, quite illuminating. For the half-body portrait of the soldier with his wound prominently displayed relates the image of the contracted arm
to the entire individual; the hysterical arm stands alone. Here the role of the representation of the arm comes to play a central role. The case described, that of "Sergt. M" who "was wounded in the right forearm on April 10, 1917," is "recognized as hysterical. . . as the deformity was identical with that shown in a photograph of a so-called reflex contracture in Babinski and Froment's book." It is the representation of the hysteric which defines the disease and which defines both the treatment of the disease and the patient's response: "On the day of admission the hand was continuously manipulated, the patient being persuaded at the same time that it would rapidly relax. In ten minutes complete relaxation was obtained and the deformity disappeared." The relationship between seeing correctly and the patient's response is here made absolute. As Elaine Showalter notes, the transition from the image of the female pet patient of nineteenth-century clinical psychiatry to the image of the male sufferer from traumatic neurosis (shell shock) meant a drastic realignment of the presuppositions of gender.[50] Hurst sees the male hysteric as ill but as quickly curable, a factor that sets the soldier apart from the long tradition of more or less professional (i.e., long-term) female patients at the Salpêtriére. What he teaches his hysterics is to see themselves as "men"—to confront their illness and return to service.
Jean-Martin Charcot (and his colleague Paul Richer) provide the reader (and viewer) of these late nineteenth-century images of the hysteric with a set of antecedent images from sources other than the unspoken one of the mesmerist.[51] In their study of the representation of the insane—specifically the hysteric in the art of the West—they create their own history and conclude it with a clinical chapter outlining their "universal" nosological categories of hysteria, which they see as "valid for all countries, all times, all races."[52] Charcot and Richer begin by outlining the representation of possession in religious art from the early middle ages through the seventeenth century. They offer sixty-seven illustrations, often in line form, to provide visual proof of the continuity between the images of the Catholic mystic and the modern hysteric. Beginning with the fifth-century representation of possession in the Romanesque mosaics of Ravenna to images of Saint Catherine of Sienna, Charcot and Richer begin to build their case for the parallel (and therefore the universality) of their visual categories of hysteria.
The assumption is that there is an explicit continuity between Catholic religious experience, as represented by the practitioners, and the neurological pathologies of nineteenth-century France.[53] Thus the aesthetic representation of ecstasy becomes a clinical sign of psychopathology. Their movement is however not merely on the level of the equation of

The image of the possessed as the hysteric. From J.-M. Charcot
and Paul Richer, Les Dénoniaques dans l'art (Paris: Adrien Delahaye
et Emile Lecrosnier, 1887), p. 4.
Photo courtesy Wellcome Institute Library, London.
the religious-aesthetic and the clinical. For they cite one image (and text) from the general realm of medicine, and that is Sir Charles Bell's image of opisthotonus. The passage they quote is identical to the one cited above. Their argument is that the image of opisthotonus is parallel to a number of the images of possession that they offer, specifically the early seventeenth-century image of Saint Nilus by Domenicho Zampieri called Domenichino (1581-1641). Like their discussion of a sketch for the child in Raphael's Transfiguration , there is a stated assumption that the reality of the symptoms of hysteria are exactly parallel to the immutable reality of the symptoms of tetanus. In their final chapter, on the contemporary representation of the hysteric, Charcot and Richer draw on the images of the stages of the "hysterical convulsion" which Charcot had established in the 1880s. The parodies of religious experiences, from the position of prayer to the position of crucifixion find their visual representations in this chapter,[54] as does the classic arc-en-cercle position of the opisthotonus taken from Bell.[55]
What is most striking from the viewpoint of the history of the representation of the hysteric is that there is a continuity to the overall reception of the image of the hysteric which transcends the school of the

One of the topoi used to depict the history of the hysteric is this sketch
for the child in Raphael's Transfiguration . From J.-M. Charcot and Paul
Richer, Les Démoniaques dans l'art (Paris: Adrien Delahaye et Emile
Lecrosnier, 1887), p. 29.
Photo courtesy Wellcome Institute Library, London.
The self-crucified hysteric. From J.-M. Charcot and Paul Richer, Les
Démoniaques dans l'art (Paris: Adrien Delahaye et Emile Lecrosnier, 1887),
p. 100, lower image.
Photo courtesy Wellcome Institute Library, London.
Salpêtriére. Thus if we return to the British images taken from Arthur F. Hurst's study of hysterical contractures, we can see that Charcot and Richer, in citing images from Louis Basile Carré de Montgeron's account of the Jansenist miracles,[56] had already set the stage for the representation of the nonfunctional limb as a primary sign of hysteria. The link between the female and the victim of shell shock is made through the representation of the body part that makes them unable to be mobile in a society that demands mobility as a sign of group identity. The meaning ascribed to mobility from the eighteenth century to the twentieth century is quite different (the middle-class woman becomes a full member of the new religious sect when she is healed; the soldier returns to his fighting unit when he is healed). But central to the image of cure is the image of mobility. The visibly nonfunctional limb, with the alteration in gait or in posture, marks the hysteric as diseased. The images taken from the history of religion have already provided a model for the representation of the affected area as the target for healing. The analogy between the mentally ill and the enthusiastic and/or rigorous fundamentalism of religious schismatics such as the Jansenists had already been made by Philippe Pinel in the wake of the French Revolution. Citing a range of British sources in a French Catholic context, Pinel was forced to see the hypermoralism of the Jansenists as setting them apart from French society. He labeled them the pathological equivalents of the Methodists.[57] Charcot's citation of Jansenism as the central visual clue to the history of hysteria ties the image of the hysteric, not merely
The religious cure of the "hysteric." From Louis Basile Carré de Montgeron,
La verité des miracles operés par l'intercession de M. de Pêris et autres
appellans demontrée contre M. L'archevêque de Sens , 3 vols. (Cologne: Chez
les libraires de la Campagie, 1745-47), as reproduced in J.-M. Charcot and Paul
Richer, Les Démoniaques dans l'art (Paris: Adrien Delahaye et Emile Lecrosnier,
1887), p. 81.
Photo courtesy Wellcome Institute Library, London.
to "religion" but to the religion of spiritual excess, to religions such as Methodism and, in a specific manner that will be discussed below, to the mystical religion of the Eastern Jews.[58]
The religious rigidity and the enthusiasm of the Jansenists came to stand for the perversion of the spirit which was as pathological as the diseases of the hysteric. Paul Regnard brings a series of the attitudes passionnelles in his photographs of Augustine from the second volume of the Iconographie de la Salpêtriére .[59] These images mimic the positions of the Jansenists, but they are without doubt images of pathology. The parallels make both sets of images pathognomonic.[60] As with the images of the Jansenists, the images of the hysterics are closely associated with visual hallucinations, with the seeing of what is not there as a sign of the falsification of the imagination. William Hammond, in his 1876 history of hysteria, continued this "liberal" discourse of the Salpêtriére which associated disease and religion. He noted that "in these undeveloped forms of both diseases, as noticed among the Jansenist convulsionnaires, the affected individuals appeared as if struck by the sight of some object before unseen, and the contemplation of which filled them with the most ravishing joy."[61] Here the pathologization of seeing is the mirror image of the clinical gaze of Charcot, who sees the disease, the disease of the fantasy, the disease of religion.
Thus Charcot and Richer undertake what many scientists of the nineteenth and twentieth centuries do—to write the history of their own discovery in order to show its universality across time (if not across cultures). But this history of the representation of hysteria, drawing on the power of the new secularized religion of science in displacing its antecedent Christianity, becomes the model through which the hysteric is visually categorized. This tradition does not stop with Richer and Charcot. Students of Charcot's provide some of the later material. Henry Meige (after 1901 the editor of the Nouvelle Iconographie de la Salpêtriére ) and Jean Heitz both contribute essays to the Nouvelle Iconographie de la Salpêtriére on the artistic image of the hysteric well into the twentieth century.[62] Within the German tradition, the physician-historian-art critic Eugen Holländer incorporates many of these images in writing his history of the image of the impaired in classical art.[63] Holläinder quotes liberally from the same visual sources as Charcot and Richer—citing Raphael and the various images of religious possession. Jean Rousselot continues this image in his study of medicine in art into the post-World War II era.[64] His work begins with the representation of the Greeks, such as the Bacchic scene of "dying Bacchante," now in the Uffizi. He comments in his caption: "In point of fact, a depiction of hysteria. At

The representation of religious ecstasy as pathological sign. From
Paul Regnard, Les maladies épidémiques de l'esprit: sorcellerie magnétisme,
morphinisme, délire des grandeurs (Paris: E. Plon, Nourrit et Cie., 1887), p. 95.
The image is an engraving of a photograph taken from the Iconographie
de la Salpêtriée .
(Bethesda, Md.: National Library of Medicine.)
the far right, a hysterical woman, her body bent in the shape of an arc." All of these works assume a continuity of the meaning of the image of the hysteric from the ancient Greeks to their contemporaries. And all of them stress the continuity between the ancient representation of religious experience (rather than images of pathology) and modern experiences of disease (rather than religion). This asymmetry provides a powerful subtext for the association between images of religion and those labeled in the popular mind as being associated with categories constructed as or labeled as religious ones—such as the Catholic (or at least the Catholic cleric) and, in an equally complex manner, the Jew.
The "warfare between theology and science," to paraphrase the title of A. D. White's classic nineteenth-century study,[65] which is played out within the secularized Christian discourse of late nineteenth-century psychopathology, is nowhere more clearly evident than in Paul Regnard's 1887 monograph (with 120 images) on the visual relationship between magnetism, morphinism, and madness, which begins with the visual equation between the witch and the mad.[66] Regnard, a physician and the professor of physiology at the National School of Agronomy, was the coeditor (with Désire-Magloire Bourneville of the Bicêtre) of the original, three-volume edition of the Iconographie photographique de la Salpêtriére[67] as well as a well-received medical atlas.[68] His study of 1887, which is dedicated to "cher maitre," Charcot, assumes the interrelationship of all forms of mass hysteria. His first example is the witch. He provides a series of plates from Abraham Palingh's study of witchcraft to document the visual representation of the witch as the "grand hysteric."[69] In this context Regnard brings in other images of demonic possession from the Renaissance to the seventeenth century (p. 41), including—as one of the images that becomes standard to the repertoire of visual proof—the figure of the boy from Raphael's Transfiguration (P. 59).
It is assumed that these pathological positions are indicative of the association with other forms of possession, such as hysteria. To make this absolutely clear in the reader's eye, he reproduces, in the form of drawings which thus resemble the format of the earlier images he has reproduced, a series of photographic images from the Iconographie photographique de la Salpêtriére . Of these the image of the gaze, the hallucination as experienced by the observer rather than the hysteric, stands as the icon of pathology (p. 87). Regnard makes similar visual claims in associating the image of the hysteric with that of the sleepwalker, the drug addict, and the person suffering from monomania. Images are produced that draw on the visual association of abnormal states—there is
The image of the witch. From Abraham Palingh, 't Afgeruckt Mom-Aansight
der Tooverye: Daar in het bedrogh der gewaande Toverye, naakt ontdeckt,
en emt gezone Redenen en exemplen dezer Eeuwe aangewezen wort (Amsterdam:
Andries van Damme, 1725), p. 50, as used in Paul Regnard, Les maladies êpidémiques
de l'esprit: sorcellerie magnétisme, morphinisme, délire des grandeurs (Paris: E. Plon,
Nourrit et Cie., 1887), p. 19.
(Bethesda, Md.: National Library of Medicine.)
The representation of a visual hallucination, the centrality of the eye
and the gaze. From Paul Regnard, Les maladies êpidémiques de l'esprit:
sorcellerie magnétisme, morphinisme, délire des grandeurs (Paris: E. Plon,
Nourrit et Cie., 1887), p. 87.
(Bethesda, Md.: National Library of Medicine.)
always the assumption that there is a normal image of the productive, healthy human, and the deviant is marked by external signs, such as position, clothing, handwriting, and so on. These signs represent the symptoms of mental disorder, and all are interrelated because the signs are interrelated. But more than this is shown by moving from the witch (and the torture and cruelty inflicted on the witch [p. 33] to the miracles associated [as in Charcot] with healing the hysteric, to use his term [pp. 133, 135]. Religion and its hypocrisy, its antithetical relationship to the act of modern medical healing, are cited, and the cures of the church are ascribed to the nature of the disease entity—to hysteria. The cure of the disease of hysteria is the mass hysteria of religion. The model for this is the antiquated one of homeopathic medicine—like curing like. It is clear that Regnard, like Charcot and Richer, is looking for a more modern approach to therapy—to electrization or to the newly relabeled science of hypnotism—for their cure, not to religion. For the church, representing the institutionalization of religion in contemporary society, is the root cause of the hysteria, not its cure.
The other central model cited by Charcot and Richer in their scientific work is the model of the epileptic.[70] Stemming from Charcot's initial observations on his patients in the Salpêtriére showing the symptoms of "hystero-epilepsy" (his own composite category, which Freud borrowed), the visual image of the difference of the hysteric stems to no little degree from the tradition of representing the epileptic.[71] The image of the epileptic is in many ways parallel to that of the hysteric. Thus the "simulation" of the hysteric is paralleled by the "contradictions and exaggerations of sentiment [which] are salient characteristics of epileptics," according to Cesare Lombroso. He continues: "Epilepsy has a disastrous effect on the character. It destroys the moral sense, causes irritability, alters the sensations through constant hallucinations and delusions, deadens the natural feelings or leads them into morbid channels."[72] This need to see the pathological character of the epileptic as parallel to his or her disease is replicated in the visual image of the epileptic. While many of the visual images of the epileptic in the medical literature of the nineteenth century deal with the problems of localizing the brain lesion,[73] there is also a tradition of representing the symptoms of epilepsy through representing the patient. Charles Féré, in the Nouvelle Iconographie de la Salpêtriére , represents hysteria as literally written on the skin of the hysteric.[74] The parallel image is to be found in the representation of hysterical ulceration.[75] If one examines L. Pierce Clark's argument from 1898 that there are "tetanoid seizures in epilepsy," one can see the argument coming full circle to the organic model

The sensitive skin of the epileptic becomes a tabula rasa upon which
the disease can be inscribed. From Charles Féré, "Note sur un cas de
mélanodermie récurrente chez un épileptique apathique," Nouvelle
iconographie de la Salpêtriére , 10 N.F. (1897): 332-339.
(Bethesda, Md.: National Library of Medicine.)
of tetanus.[76] Indeed, the fascination with the marking of the signs and symptoms of disease on the body permeates the image of the epileptic in ways other than the search for the Jacksonian brain "lesion" that must necessarily cause the seizures.[77] Thus there are images of the malformed hands of an epileptic woman or of the corporeal asymmetry of the epileptic female.[78]
The image of the epileptic is also found within the tradition of representing the physiognomy of the insane. Thus William Alexander provides the reader with a photograph of each of the patients whose cases he reports in his 1889 study in order to present their physiognomy.[79] It is the visual appearance of the epileptic that provides the clue to his or her special, hidden flaw. The lesion must, in some overt way, write itself on the body. Some essays, such as on the baldness[80] or the altered appearance of the hair[81] of an epileptic man as a sign of his illness, are more than reminiscent of the extraordinary images of the "plinca polonica" or "Judenkratze," the fantasy skin disease attributed by Western dermatologists to the Jews of the East. In some of the recent historical literature on the history of epilepsy, much of the same tradition cited by Charcot and Richer reappear—now in the context of documenting the ongoing history of epilepsy. Thus images of religious ecstasy and possession from the early Middle Ages appear as precursors of the image of the epileptic.[82]
All of these images relate to the idea of the hysteric as continuous over time and across cultures. This is the basic assumption of the definition of a positivistic disease entity at the close of the nineteenth century. Disease is real only if it is universal. And it is universal only if it can be seen and the act of seeing reproduced. This latter axiom is rarely stated (except by the head of the Salpêtriére's photographic service, Albert Londe), but it is assumed. Thus the image of the impaired patient is the touchstone for the reality of the disease.
Creating a Composite Image of the Hysteric
It is vital to understand that the creation of a history of the image of the hysteric is not the same thing as Charcot and Richer's attempt to place the diagnostic criteria applied to hysteria in the distant past (while ignoring the more recent past). What can be undertaken in a limited way (because of the extraordinary range of visual sources) is to sketch the visual aspects associated with the idea of hysteria at the turn of the century as a means of delineating the scope of the image. Thus this section will be devoted to a catalog of those visual qualities ascribed to the hys-
On the image of asymmetry of the epileptic, see plate XLI: "Asymetrie du
corps chez une epileptique," in F. Raymond and Pierre Janet, "Malformations
des mains en 'pinces de humard,'" Nouvelle iconographie de la Salpêtriée 10
(1897 ): 369-373 (an extract from their book Nécroses et idées fixes [Paris: F.
Alcan, 1898]).
Photo courtesy Wellcome Institute Library, London.
teric. We shall seek to sketch the boundaries of the representation of the visual nature of the hysteric in fin-de-siécle medical literature.
It is central to any understanding of this composite image that the desire of all of these studies, no matter what their national context, is to place themselves within the myth of the realism of the act of represen-

The face of the epileptic. From William Alexander, The Treatment of
Epilepsy (Edinburgh and London: Young J. Pentland, 1889), p. 107.
Photo courtesy Wellcome Institute Library, London.
tation and the highly specialized role that the physician (as interpreter) plays in reproducing and "reading" the image of the patient. And this reading has a clear relationship with the means of reproducing and disseminating the image of the hysteric. The startle effect has now blended into an idea of a realism that indicates a control by the scientist and the scientist alone over the new medium. (As anyone could make and possess photographs after the mid-1890s, it became more and more important for the scientific photograph to be the object of scientific interpretation. This attitude permitted many interpreters of the photograph of the patient seamlessly to become the interpreters of the new hermeticism of the X ray when it was introduced in 1895.) The reading of the photograph had also blended in with the aesthetic (or, perhaps better, artistic) tradition into which the "new" science of representation had placed the image of the hysteric. Charcot and Richer, in a paper they first published in the Journal of Nervous and Mental Disease in 1883, stated the case best. In noting the "immobile" physiognomy of a hysterical patient whose facial muscles had been electrically stimulated, they
Images of the alteration of the hair in the mentally ill are already evoked
in Darwin's study of the nature of expression. Here the image of the altered
appearance of the hair evokes older images of the diseases of the Eastern Jews.
From Dr. Räiuber, "Ein Fall von periodisch wiederkehrender Haarveräinderung
bei einem Epileptiker," [Virchows] Archiv für pathologische Anatomie und
Physiologie 97 (1884): 50-83, plate no. 2.
(Bethesda, Md.: National Library of Medicine.)
observe: "The physiognomy retained immobile, in a state of catalepsy. The same is true of the attitude and the gesture that accompanied it. The subject of this transformed into a sort of expressive statue, a motionless model, representing with striking accuracy most varied expressions, which artists, without doubt, might avail themselves of to a very great extent. The immobility of the attitudes thus provoked is eminently favorable to photographic reproduction."[83] They then reproduce a series of these photographs. This argument is similar to that critique by Walter Benjamin in his essay from the mid-1920s on the reproducibility of images in the age of technology.[84] For it is important to understand that observing is not sufficient. Charcot (and Richer) turn the object observed (the hysteric) into the work of art and then are able to commodify this work of art through the reproduction of her image within the scientific text. This is not quite like the cinematic examples that Benjamin brings. It is much more similar to the extensive photographic reproductions of "great works of art" which dominated the middle-class market for art during the 1880s and 1890s. Benjamin's discussion of the "exchange of glances" between the observed and the observer creates a critical context for the learning experience of the hysteric. For it seems that the exchange of glances in this system of representation is one between an aware hysteric and an unaware physician. But the Salpêtriére gave birth to other means of seeing difference and also of recording it.
In many of these images the confusion between acquired pathognomonic signs and inherent ones is manifest. There evolves in the finde-siécle discussion of the physiognomy the assumption that there is an absolute relationship between the form of the skull and the shape of the face.[85] And given the emphasis on craniometric measurements as a means of speaking about the nature of the mind/psyche it is clear that the relationship between the structure of the face and the mind, already present in the physiognomy of Johann Caspar Lavater (and his predecessors) becomes an easy one. Francis Warner summarizes many of the discussions of his contemporaries, such as Charles Darwin, in The Expression of Emotions in Men and Animals (1872).[86] Warner stresses the "results of cerebral action upon muscles" rather than the "shape of the brain case" in seeking to find the source for the asymmetry on the face of the hysteric. She describes, however, the existence of faces that "express intellectuality" and others that express "vulgarity." The latter are an example of the "coincident defective or coarse development of the brain-case and face." The former are the result of "the nerve-muscular condition of the face" and are "more directly indicative of the intellectuality of the brain; hence we should study a face as the index of the brain, when it
is seen in action as well as when at rest." This view can be seen as representative of the medical literature of physiognomy at the turn of the century. The stress on the asymmetry of the face, an asymmetry caused by the forces of the mind, rather than the marked "vulgarity" of the mental defective, can be traced back to Philippe Pinel and his representation of the "manic" and the "idiot" at the very beginning of the century. The concept of asymmetry (indeed all faces become asymmetrical with the passage of time) can introduce the importance of an aesthetics of the face of the hysteric.
James Shaw stresses the "swelling of the upper lip" in cases of "chronic hysterical insanity" as well as a "facial expression [that] often indicates the presence of migraine."[87] The face of the hysteric, specifically the hemiplegia that marks the face of the hysteric at the Salpêtriére, is an overt sign of difference. It is a distortion of the normal face—the baseline for the "beauty" of the individual.[88] Anthropological literature of the eighteenth and nineteenth centuries had debated the meaning of the varieties of beauty, especially female beauty, throughout the world.[89] The consensus was that there was a "great chain of beauty" running from the beautiful down to the ugly races which was paralleled within each race by a normative—that is, healthy—appearance as opposed to a sick appearance. This pathology of appearance underlies the representation of the asymmetrical, unaesthetic face of the hysteric. In a paper by Hurst (1918) on battle fatigue, the face of the hysteric marks the individual who can be quickly cured and sent back into battle.[90]
But if the face is marked, it is the eyes that provide the real clue. The stigmata that mark the face are most apparent in the representation of the eyes. For both the "look" of the hysteric and the gaze of the physician mark the hysteric. Building upon the nosology of hysterical blindness developed by Charcot as well as the Philadelphia ophthalmologist George Edmund de Schweinitz, Walter Baer Weidler traces the qualities of the eyes from the "contractures, spasms and palsies" of the "eyelids and extra-ocular muscles" (i.e., the representation of the appearance of the eye) to the manifestation of hysterical blindness (amblyopia or amaurosis, partial or complete loss of vision).[91] In the work of L. Lattes and A. Sacerdote from the 1920s, similar changes in the quality of the face are described in the case of a hysterical pseudo-hemorrhage of the eye.[92] It is the quality of the gaze in the photographs of the patients that is striking. The physical anomalies represented also provide the signs for the meaning read into the physiognomy. The drooping lids or the black eye add a quality of the abnormal, of the pathological, to the gaze of the patient, marking him or her as diseased.
A sculpture of a case of hemiplegia from the teaching
collection of the Salpêtriére.
(Paris: The Salpêtriére.)
The disease that is sought is not in the eye. It is in the central nervous system, in the neural network that controls the eye. It is in the brain, the source of all hysteria, that the source of hysteria is to be found. The image of the brain becomes the image of the internal error of the hysteric. Jules Luys, in a paper of 1881, stresses this in both his text and in the accompanying images of localization.[93] E. Siemerling and J. Grasset see "cerebral-spinal degeneracy" as the source of hysteria.[94] In the work of the Hamburg physician Paul Steffens the localization of the lesion is represented in the post-mortem image of the brain.[95] All of these searches evoke the specter of the brain mythology that dominated much of the localization studies at the end of the century. The search after
The eyes and the sight of the hysteric. From Walter Baer Weidler,
"Some Ocular Manifestations of Hysteria," International Clinics ,
22d ser. 2 (1912): 249-261. Plate (fig. 5) opposite p. 252.
Photo courtesy Wellcome Institute Library, London.
the source of the anomalous appearance of the hysteric was quite parallel to the search after the origins of other neurological disorders. A. Alzheimer represented such a search in his 1911 paper on cerebral plaques, using photographs of dyed brain specimens as his visual proof of their existence.[96]
All of these images were seen as having parallel value. Each of them demanded (according to their interpreter) a trained eye to see and represent the source of the error. The interrelationship between the scientific drawing and the photograph, both understood as veridical in localizing the source of the pathology, stressed the gaze of the scientist, in seeing the nature of the brain through the interpretation of the symptoms.
For the hysteric, the symptoms are often written on the body. The
The brain of the hysteric. From Jules Luys, "Recherches nouvelles
sur les hémiplégies émotives," L'Encephale: Journal des Maladies
Mentales et Nerveuses 1 (1881): 378-398, plate 7.
(Bethesda, Md.: National Library of Medicine.)
The brain structure of the hysteric. From C. von Höb lin and A.
Alzheimer, "Ein Beitrag zur Klinik und pathologischen Anatomie der
Westphal-Strümpellschen Pseudosklerose," Zeitschrift für die
gesamte Neurologie und Psychiatrie 8 (1911): 203.
Photo courtesy Wellcome Institute Library, London.
function of the skin as the map of the body is one of the oldest topoi of medicine. Reading the skin meant reading into the nature of the patient, his or her actions, and his or her resultant diseases. The nineteenth-century literature on masturbatory disease is full of such images,[97] as is, not surprisingly, the literature on hysteria. The ability of the hysterics to record written images on their skin, the hypersensitivity to touch, became one of the most fascinating symptoms for the fin-de-siécle physician. In the "modern" Revue de l'hypnotisme a striking image of such "skin writing" appears.[98] In Saint Petersburg the fin-de-siécle image of the hysteric was brought into the context of the stigmata, not Charcot's, but the stigmata of Christ.[99] The discussion of the patient presented in this "difficult case of hysteria" centered on the suggestibility of young Roman Catholic girls. The search after unique or strange manifestations
The ulcerated skin of the hysteric. From S. Weir Mitchell, "Hysterical
Rapid Respiration, With Cases; Peculiar Form of Rupial Skin Disease
in an Hysterical Woman," Transactions of the College of Physicians of
Philadelphia 14 (1892): 233.
(Bethesda, Md.: National Library of Medicine.)
of hysteria led S. Weir Mitchell, whose rest cure had been generally accepted as the treatment of choice by the end of the century, to examine a case of a hysterical ulcer in a twenty-four-year-old woman.[100] The differential diagnosis to this ulcer was to the ulceration of syphilis, which was "verified by the microscope." S. Róna continued the work that Moriz Kaposi had begun in Vienna, looking at specific forms of the manifestation of skin eruptions which could be labeled hysteric.[101] Thomas D. Savill, in London, undertook a similar study of the skin of his child patients and saw their hysteria inscribed thereupon.[102] In 1900 Dr. Bettmann from the Heidelberg Clinic of Wilhelm Erb described a further case of "atypical" skin inflammation in the hysteric; in 1901, a case of hysterical gangrene was described in Buffalo; in 1919, a similar case in Pisa. By 1930 a major survey of the nature of hysterical skin diseases was produced by Roberto Casazza in Pavia.[103] All of these studies (and more) are extensively illustrated. All of them relate, on one level or another, to the general assumption (countered by Jean-Martin Charcot in his theory of hysteria) that syphilis or the predisposition to syphilis played a major role in the risk for hysteria.
Many of these studies of the skin (such as that of Weir Mitchell) relate the appearance of the skin to the state of the genitalia, either in
The association between the syphilitic and the hysteric was made as
much on dermatologic evidence (as seen on the skin) as on psychological
evidence. From Thomas D. Savill, "A Clinical Lecture on Hysterical Skin
Symptoms and Eruptions," The Lancet (January 30, 1904): 273-278, p. 276.
(Bethesda, Md.: National Library of Medicine.)
terms of gynecological examinations that are part of the case study or in terms of a discussion of the appearance of the skin in the genital regions. Charcot associated hysteria with the area of the ovaries, those areas of heightened sensitivity in the hysteric, a touch upon which could actually create hysterical episodes. This fascination with the compression of the ovaries as therapy as well as etiology is linked in the medical discourse of the period with the fascination about hysterical ischuria, the retention of urine and feces. The number of charts of the genital regions are legion, yet the number of detailed (and illustrated) studies of the form and structure of the genitalia are few. De Sinéty, a histologist at the College de France, published a series of unillustrated case studies of the genitalia of female hysterics in the mid-1870s, supporting Charcot's thesis of the centrality of sexual stimulation for the creation of the hysterical episode.[104] With the introduction of X-ray analysis there was even an attempt to represent the pelvic structure of the hysterical female, as a means of representing the disease.[105] The X ray was but a technical innovation. For the fantasies about internalized hysteria had existed prior to Charcot.[106] In 1847 Eliogoro Guitti had presented an illustrated study of the hysterical gut.[107]
The representation of the extremities, especially the hand and the foot, reflect not only the importance laid upon the hand and foot as signs of religious possession (stigmata, paralysis) but also the physical signs associated with epilepsy. Paul Sollier presents a case of contracture of the hand in a male hysteric in the fourth volume of the Nouvelle Iconographie de la Salpêtriére .[108] Some of the studies, such as those of Hurst, concentrate on the problem of hysterical contractures, such as Charcot's "glove anaesthesia" in the hysterical traumatic paralysis of the hand; others on the appearance of the hand, its coloration (usually blue, according to Gilles de la Tourette[109] ) and marked swelling.[110] The legs are similarly examined for the contractures of "hysterical paraplegia" (and their cure).[111] The images taken from Charcot's schematic representation of areas of anesthesia reappear over and over again to illustrate cases of the diminished ability to feel (and often to move) the limbs.[112]
The visual representation of posture and paralysis is used as a mode of visual proof of Charcot's nosological categories.[113] In an essay from the very first issue of the Nouvelle Iconographie de la Salpêtriére in 1888, by Georges Gilles de la Tourette, we are not only made to see the hemiplegic patient but also his gait, through a schematic representation.[114] In this case, described by Henri Lamarque and Emile Bitot, there is a comment on the plate that they had intended to use a photograph but an accident at the last moment ruined the plate and they were forced to
The X ray permitted the physician to see within the hysteric.
From Jose M. Jorge, "Coxalgia histérica," Revista de la Asociacion
Medica Argentina 32 (1920): 18-29, plate opposite p. 80.
(Bethesda, Md.: National Library of Medicine.)
use a photolithograph. The form of the representation becomes central to its message. For the photograph remains more real than any other mode of representing the hysteric. Thus in an essay by Byrom Bramwell—one of the leading Scottish specialists on nervous diseases such as hysteria and, one can add, one of the leading believers in a set pathognomonic representation of disease—the photograph remains the central proof for the differential diagnosis between "hysteria" and its contractures and other forms of organic disease.[115] But this photograph has been quite evidently cut to remove the presence of the physician or nurse whose hands remain supporting the patient. A similar undertaking can be seen in the photograph contracture represented in the essay by A. Steindler in Iowa City, except here the patient is given a staff on which to rest.[116]
The realism of the photograph concentrates the gaze of the physician-reader on the representation of the disease in the image of the patient. Peter Davidson follows this lead with his presentation of a case of hystero-catalepsy from Liverpool.[117] The number and range of Davidson's
The hysterical gut as an internal manifestation of the disease.
Eliogoro Guitti, "Osservazioni Cliniche," Giornale per Servire ai
Progressi della Patologia e della Terapeutica , 2d ser. 22 (1847): 229-258,
plate following p. 258.
(Bethesda, Md.: National Library of Medicine.)
cases (running from rheumatoid arthritis to hystero-catalepsy) would have enabled the author to illustrate any (or indeed all) of his cases. He chose to illustrate the case of hystero-catalepsy. As late as in 1930, in an essay by Prince P. Barker, at the Veterans' Hospital in Tuskegee, Alabama, the image of the hysteric black comes to represent the image of the hysteric whose limbs are frozen.[118] Using Charcot's categories ex-
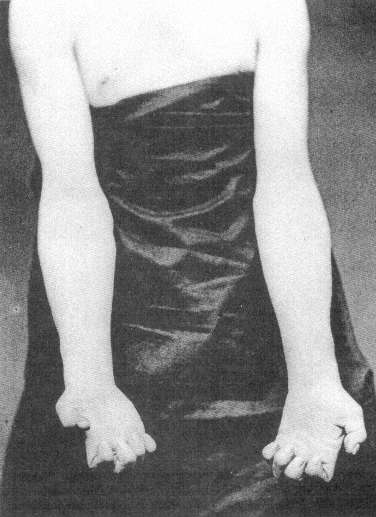
The hand of the male hysteric. From Paul Sollier, "Contracture Volontaire
chez un Hystérique," Nouvelles Iconographie de la Salpêtriére 4 (1891): 100-106,
plate opposite p. 106.
Photo courtesy Wellcome Institute Library, London.
The posture of the schematic "patient." From Henri Lamarque and
Emile Bitot, "Sur un cas d'hystérotraumatisrne chez l'homme,"
Bulletins de la Société d'Anatomie et de Physiologie Normales et
Pathologiques de Bordeaux 9 (1888): 242-257, plate with
figures 6 and 8.
(Bethesda, Md.: National Library of Medicine.)
A "doctored" photograph of the hysteric. From Byrom Bramwell, "Clinical
Lecture on a Case of Hysterical Contracture," Edinburgh Medical Journal ,
ns 1 (1897): 128-138, plate 5.
(Bethesda, Md.: National Library of Medicine.)
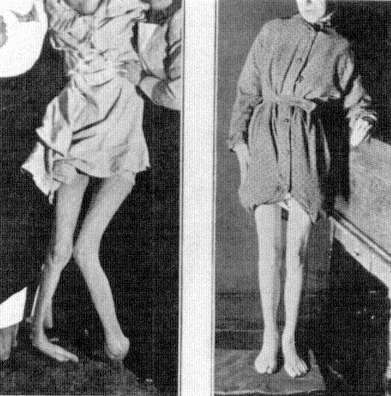
Above and verso: The hysteric posed. From A. Steindler, "On Hysterical
Contractures," International Clinics , 4th ser. 45 (1935): 221-229, fig. 2,
opposite p. 222.
Photos courtesy Wellcome Institute Library, London.
pressly, Barker shows three images. First, an image of the "normal," that is, pathological, posture of the patient; second, an image that in its blurred state is to represent the range of motion in the patient; and finally, an image of the body restored through "etherization and suggestion." Here the impact of the cinema on the idea of realism is evident. Whereas in the work of Lamarque and Bitot such an image would be understood as ruined, here it reveals a further aspect of the realism associated with the act of photographing.
One last form of realistic representation of the hysteric should be discussed. For throughout the vast literature of hysteria (and other forms of mental illness) in the nineteenth century there are uncountable
The illusion of movement in representing the hysteric. From Prince P.
Barker, "The Diagnosis and Treatment of Hysterical Paralysis," United
States Veteran's Bureau Medical Bulletin 6 (1930): 663-670, 3 plates
following p. 670.
(Bethesda, Md.: National Library of Medicine.)
charts, graphs, and statistical tables. It is virtually unimportant what source one uses. From the medical periodicals in France[119] to those in Japan[120] or Germany,[121] one consistent image of the hysteric is that of the scientific reduction of the sufferer and the disease to schematic representations. The cry of these images is that they are the real, transcendent image of the hysteric. Like Galton's composite photographs (which will be discussed below), they give the observer an image of the totality of the disease. This fantasy of reducing the complexity of hysteria to statistics or charts rests on a notion of nineteenth-century science that everything is reducible to nonverbal form (read: mathematical), and that is precisely the claim of the photograph. For once, it is said, you eliminate narrative, you remove the subjective aspect from the evaluation of the disease and you have a real representation of the patient. Thus the use of charts and statistics in representing the hysteric is another visual means of creating an image of the disease, as sure as the images of the skin, or brain, or cellular structure of the hysteric.
Hysteria, Race, and Gender
Sigmund Freud's reading of the ancient Greek myth of the wandering womb, which, when lodged in the throat, created the globus hystericus , can serve us as a detailed example of the problems attendant to "seeing" the hysteric. It is well known that Freud, in the autobiographical account he wrote of the occasion some forty years after the event, recalled the bad reception that his initial paper on male hysteria had when he presented it before the Viennese Society of Physicians on 15 October 1886.[122] Returning from his work with Jean-Martin Charcot in Paris and desiring to present his newly acquired insights about male hysteria to his home audience in Vienna, Freud presented his paper. His powerful recollection was that his hearers thought that what he "said was incredible. . . . One of them, an old surgeon, actually broke out with the exclamation: 'But, my dear sir, how can you talk such nonsense? Hysteron [sic] means the uterus. So how can a man be hysterical?'"[123] Freud's angry memory was aimed at the narrow-minded claim of the Viennese establishment, that it, and it alone, had command of Greek. It was the young, French-trained Freud who knew that the concept of hysteria was tied to universals (which, at that point, he understood as trauma) and was not merely a reflex of the biological uniqueness of a subgroup. It was hysteria (the hallmark of the new science) that Freud wished to rescue from the crabbed claws of a Viennese medical establishment that could not even get its Greek correct, for hystera is the correct form of the Greek noun
The chart as the representation of the male hysteric in Japan, as in
the image of psychic forces in H. Nishi, "[Male Hysteria Cured by
Suggestion]," Chugai Iji Shinpo 405 (1897): 5-9; 406 (1897): 11-16,
image on p. 9.
(Bethesda, Md.: National Library of Medicine.)
The chart as the representation of the hysteric in Germany, as in the
evaluation of operations on the heating of the hysteric in K. Rudolphy,
"Ohroperationen bei Hysterischen," Zeitschrift für Ohrenheilkunde
und für die Krankheiten der Luftwege 44 (1903): 209-221, plate 17,
opposite p. 220.
(Bethesda, Md.: National Library of Medicine.)
for uterus. Thus the young Jew (and Freud understood himself from his exposure to the virulent "scientific" anti-Semitism of the Viennese University as a Jew) showed his command over not only the language of science (represented by Charcot's discourse on hysteria) but also the language of culture (Greek). (The significance of this factor will be shown in the course of this analysis.) Freud's understanding, like the understanding of his time, was that hysteria did not manifest itself as a disease of the womb but of the imagination. This did not absolve the female from being the group most at risk, however, for the idea of a pathological human imagination structurally replaced the image of the floating womb as the central etiology of hysteria. What was removed from the
category of hysteria as Freud brought it back to Vienna was its insistence on another group, the Jews, which replaced the woman as essentially at risk.
The idea of the hysteric was a central one for the imaginative world of Sigmund Freud as it was close to his self-definition. For at the close of the nineteenth century the idea of seeing the hysteric was closely bound to the idea of seeing the Jew—and very specifically the male Jew.[124] For if the visual representation of the hysteric within the world of images of the nineteenth century was the image of the female, its sub-text was that feminized males, such as Jews, were also hysterics, and they too could be "seen." The face of the Jew was as much a sign of the pathological as was the face of the hysteric. But even more so, the face of the Jew became the face of the hysteric. Let us quote from one of the defenders of the Jews against the charge of being tainted by hysteria. Maurice Fishberg's The Jews: A Study of Race and Environment (1911) states the case boldly: "The Jews, as is well known to every physician, are notorious sufferers of the functional disorders of the nervous system. Their nervous organization is constantly under strain, and the least injury will disturb its smooth workings."[125] The origin of this predisposition is neither consanguineous marriage ("the modern view . . . [is that they] are not at all detrimental to the health of the offspring") nor the occupations of the Jew ("hysteria [is] . . . met with in the poorer classes of Jews . . . as well as in the richer classes").[126] It is the result of the urban concentration of the Jews and "the repeated persecutions and abuses to which the Jews were subjected during the two thousand years of the Diaspora."[127] These influences, found at the turn of the century primarily among Eastern Jews, according to Fishberg show the predisposition of these specific groups of Jews to illnesses such as hysteria: "Organic as well as functional derangements of the nervous system are transmitted hereditarily from one generation to another."[128] It is not all Jews who are hysterics, but Eastern Jews, and primarily Eastern male Jews, according to Fishberg: "The Jewish population of [Warsaw] alone is almost exclusively the inexhaustible source for the supply of specimens of hysterical humanity, particularly the hysteria in the male, for all the clinics of Europe."[129] Here Fishberg, an American Jew, misquotes the French psychiatrist Fulgence Raymond, who had stated that Jews of Warsaw formed a major sector of the mentally ill of that city.[130] It was Fishberg's misquote of Raymond that became the standard view in German psychiatry.[131] It appeared within Freud's circle when Isidor Sadger noted at the 11 November 1908 meeting of the Vienna Psycho-
analytic Society: "In certain races (Russian and Polish Jews), almost every man is hysterical."[132] It is the male Jew from the East, from the provinces, who is most at risk for hysteria.
This view had been espoused by Charcot, who diagnosed on 19 February 1889 the case of a Hungarian Jew named Klein, "a true child of Ahasverus," as a case of male hysteria. Klein had a hysterical contracture of the hand and an extended numbness of the right arm and leg. It was Klein's limping that Charcot stressed. Klein "wandered sick and limping on foot to Paris" where he arrived on 11 December 1888. He appeared at the Salpêtrière the next day, "his feet so bloody that he could not leave his bed for many days." Klein "limped at the very beginning of his illness." Charcot reminded his listeners that the patient "is a Jew and that he has already revealed his pathological drives by his wanderings." His "travel-mania" could be seen in the fact that "as soon as he was on his feet again, he wanted to go to Brazil."[133] Klein also suffered from the standard numbness ascribed to the hysteric on half of his body. Wandering and limping mark the hysterical Jew as diseased, and diseased because of incestuous intermarriage.
H. Strauss of Berlin, in one of the most cited studies of the pathology of the Jews, provides a bar chart representing the risk of the Jews for hysteria.[134] It shows that male Jews suffer twice as often from hysteria as do male non-Jews. While it is clear that women still are the predominant sufferers from the disease, it shows a clear "feminization" of the male Jew in the context of the occurrence of hysteria. Freud's teacher, the liberal-Jewish neurologist Moriz Benedikt, also links the "American" quality of life with the appearance of hysteria, a disease that he understood as "a uniquely feminine nervous disease"—in men.[135] The struggle for life in the city causes the madness of the male Jew: "Mental anxiety and worry are the most frequent causes of mental breakdown. They are all excitable and live excitable lives, being constantly under the high pressure of business in town."[136] The reason for this inability to cope with the stresses of modern life lies in "hereditary influences," that is, their being Jews.[137]
And that is written on their faces, as on the faces of women. William Thackeray, in Codlingsby , his parody of Disraeli's novels, has his eponymous protagonist revel in the aestheticized sight of the "ringlets glossy, and curly, and jetty—eyes black as night—midsummer night—when it lightens; haughty noses bending like beaks of eagles—eager quivering nostrils—lips curved like the bow of Love" of the Jews.[138] "Every man or maiden," looks Jewish, but also looks feminine; "every babe or matron in that English Jewry bore in his countenance one or more of these
The Jewish hysteric, as represented by a chart from H. Strauss,
"Erkrankungen durch Alkohol und Syphilis bei den Juden," Zeitschrift
für Demographie und Statistik der Juden , 4 N.F. (1927): 33-39;
chart on p. 35.
(Bethesda, Md.: National Library of Medicine.)
The idealized "Jewish face," in a drawing by the famed fin-de-siècle
Viennese Jewish artist Ephraim Moses Lilien, is that of the female. In
Maurice Fishberg, The Jews: A Study of Race and Environment
(London: Walter Scott Publishing Co., 1911), p. 95.
Photo courtesy Wellcome Institute Library, London.
characteristics of his peerless Arab race." Codlingsby muses: "How beautiful they are!" when the jarring voice of Rafael Mendoza breaks his revery: "D'you vant to look at a nishe coat?" But the accent is not a true sign of the Jew's difference: "All traces of the accent with which he first addressed Lord Codlingsby had vanished, it was disguise: half the Hebrew's life is a disguise. He shields himself in craft, since the Norman boors persecuted him." The association between the falsity of the language of the Jews (which is not merely accented but duplicitous) is balanced by the "true" sight of the Jews—a factor that Thackeray parodies. What remains is that the "sight" of the Jew—the registration of the external signs of Jewishness—is a truer indicator of the nature of the Jew (or at least the perception of the Jew's nature in Thackeray's relativistic manner of representing the Jew) than is the mutable sign of the Jews' language, a language that is corrupted by as well as corrupting the world in which the Jew in the Diaspora lives.
Francis Galton actually tries to capture this "Jewish physiognomy" in his composite (i.e., multiple exposure) photographs of "boys in the Jews' Free School, Bell Lane." Galton provides types generated by multiple exposures. There he sees the "cold, scanning gaze" of the Jew as the sign of their difference, of their potential pathology.[139] It is in the Jews' gaze that the pathology can be found. This view is at least as old as Robert Burton's Anatomy of Melancholy , where Burton writes of the "goggle eyes" of the Jews, as well as "their voice, pace, gesture, [and] looks" as a sign of "their conditions and infirmities."[140] But it is not merely that Jews "look Jewish" but that this marks them as inferior: "Who has not heard people characterize such and such a man or woman they see in the streets as Jewish without in the least knowing anything about them? The street arab who calls out 'Jew' as some child hurries on to school is unconsciously giving the best and most disinterested proof that there is a reality in the Jewish expression."[141] The gaze of the non-Jew seeing the Jew is immediately translated into action.
The complexity of the Jewish response to this view can be measured in Joseph Jacob's discussion of Galton's finding of the absolute Jewish-ness of the gaze:
Cover up every part of composite A but the eyes, and yet I fancy any one familiar with Jews would say: "Those are Jewish eyes." I am less able to analyze this effect than in the case of the nose. . . . I fail to see any of the cold calculation which Mr. Galton noticed in the boys at the school, at any rate in the composites A, B, and C. There is something more like the dreamer and thinker than the merchant in A. In fact, on my showing this to an eminent painter of my acquaintance, he exclaimed, "I imagine that
Francis Galton's "composite" and "component" images of the Jew
(here the Jewish male stands as representative for the Jew). Frontispiece
to Joseph Jacobs, Studies in Jewish Statistics (London: D. Nutt, 1891).
Photo courtesy Wellcome Institute Library, London.
is how Spinoza looked when a lad," a piece of artistic insight which is remarkably confirmed by the portraits of the philosopher, though the artist had never seen one. The cold, somewhat hard look in composite D, however, is more confirmatory of Mr. Galton's impression. It is noteworthy that this is seen in a composite of young fellows between seventeen and twenty, who have had to fight a hard battle of life even by that early age.
For the Jewish social scientist such as Jacobs the inexplicable nature of the Jewish gaze exists (even more than the "nostrility" that characterizes the Jewish nose) to mark the Jew. His rationale is quite different than that of Galton—he seeks a social reason for the "hard and calculating" glance seen by Galton, but claims to see it nevertheless. This view reappears within the medical literature in the work of Jewish physicians, such as Moses Julius Gutmann, who writes of the structure of the Jewish face, of its typical form, as being the result of a combination of features that produce "the melancholy, pained expression" (the nebbish face) that is associated with the Jew. For Gutmann, and others, it is the result of the "psychological history of the Jew."[142]
Sigmund Freud's own fascination for Galton's "family" photographs must also be stressed. For Freud the composite photograph is virtually the representation of the dream in his Interpretation of Dreams (1990). It is an obsessive metaphor, which recurs throughout the course of his work.[143] The centrality of this metaphor is a residue of Freud's earlier acceptance of Charcot's reliance on the act of seeing as the privileged form of diagnosis. It is not seeing the unique but rather the universal. And yet hidden within those claims for universality are the images of race which Galton produces parallel to his other composites, in which the eyes of the Jew (read: Sigmund Freud) and his gaze are pathologized. The clinical gaze of the Jewish physician now becomes the object of the gaze of study. The image of the eyes, found in the calculating glance of the hysteric and the epileptic, reappears in the context of race.
In Henry Meige's dissertation of 1893 on the wandering Jew in the clinical setting of the Salpêtrière, the image of the Jew and the gaze of the Jew become one.[144] Meige undertakes to place the appearance of Eastern European (male) Jews in the Salpêtrière as a sign of the inherent instability of the Eastern European Jew. He sketches the background to the legend of the wandering Jew and provides (like his supervisor, Char-cot) a set of visual "images of Ahasverus." He then provides a series of case studies of Eastern (male) Jews, two of which he illustrates. The first plate is of "Moser C. called Moses," a forty-five- or forty-six-year-old Polish Jew from Warsaw who had already wandered through the clinics in Vienna and elsewhere; the second plate is of "Gottlieb M.," a forty-two-year-old Jew from Vilnius, who likewise had been treated at many of the psychiatric clinics in Western Europe. Given the extraordinary movement of millions of Eastern Jews through Western Europe, beginning in the early 1880s, toward England and America, the appearance of these few cases of what comes to be called "Munchausen syndrome" should not surprise. Without any goal, these Jews "wandered" only in the sense that they were driven West, and that some should seek the solace of the clinic where they would at least be treated as individuals, even if sick individuals, should not make us wonder. What is striking is that Meige provides images and analyses that stress the pathognomonic physiognomy of the Jew—especially his eyes. The images gaze at us, informing us of their inherent hysterical pathology. The Jew is the hysteric; the Jew is the feminized Other; the Jew is seen as different, as diseased. This is the image of the hysteric with which the Jewish scientist was confronted. His "startle" effect was to see himself as the Other, as the diseased, but most important as the feminized Other, the altered form of his circumcised genitalia reflecting the form of that of the woman.
The "wandering Jew" as the model for the psychopathology of
the Eastern Jew. From Henry Meige, Étude sur certains
néuropathes voyageurs: Le juif-errant a la Salpêtrière
(Paris: L. Battaille et cie., 1893), p. 17.
(Bethesda, Md.: National Library of Medicine.)
No wonder that Jewish scientists such as Jacobs, Fishberg, and Freud—in very different ways—sought to find the hysteric outside of their own self-image. For that image was immutable within the biology of race. Fishberg quotes the accepted wisdom (in order to refute it for himself and project it onto the Eastern Jew) when he cites Richard An-
The image of "Moser C. called Moses," one of the modern "wandering Jews,"
gazes at the reader. From Henry Meige, Étude sur certains néuro-pathes
voyageurs: Le juif-errant a la Salpêtrièe (Paris: L. Battaille et cie., 1893), p. 25.
(Bethesda, Md.: National Library of Medicine.)
dree: "No other race but the Jews can be traced with such certainty backward for thousands of years, and no other race displays such a constancy of form, none resisted to such an extent the effects of time, as the Jews. Even when he adopts the language, dress, habits, and customs of the people among whom he lives, he still remains everywhere the same. All he adopts is but a cloak, under which the eternal Hebrew survives; he is the same in his facial features, in the structure of his body, his temperament, his character."[145] And this constancy of character, with its de-
The physiognomy and the gaze of "Gottlieb M.,"
a forty-two-year-old Jew from Vilna, "proves" the
psychopathology of the Jew. From Henry Meige,
Étude sur certains néuropathes voyageurs:
Le juif-errant a la Salpêtrière (Paris:
L. Battaille et cie., 1893), p. 29.
(Bethesda, Md.: National Library of Medicine.)
viant sexual nature, leads to the disease that marks the Jew, that leads to hysteria. Because the etiology of the Jew's hysteria, like the hysteria of the woman, was to be sought in "sexual excess."[146] Specifically in the "incestuous" inbreeding of this endogenous group: "Being very neurotic, consanguineous marriages among Jews cannot but be detrimental
to the progeny."[147] Jews (especially male Jews) are sexually different; they are hysterical and they look it.
The clinical gaze of the Jewish physician now becomes the object of the gaze of study. The image of the eyes attributed to the Jew reappears in the context of the science of race. It is this biological definition of all aspects of the Jew that helps form the fin-de-siècle idea of the Jew. The scientific gaze should be neutral. The scientific gaze should be beyond or above all of the vagaries of individual difference.[148] As George Herbert Mead put it: "Knowledge is never a mere contact of our organisms with other objects. It always takes on a universal character. If we know a thing, explain it, we always put it into a texture of uniformities. There must be some reason for it, some law expressed in it. That is the fundamental assumption of science."[149]
But race is but one of the categories of the visualization of the hysteric that played a role in shaping the image of the hysteric in the course of the nineteenth century. For the construction of seeing the hysteric took many different forms in providing a composite image of the hysteric, an image in bits and snatches, an image that revealed the "truth" about the hysteric's difference to him- or herself. The nosology of the "categories" of difference are really quite analogous to Charcot's construction of the visual pattern of the actions of the hysteric. One can argue that Freud's intellectual as well as analytic development in the 1890s was a movement away from the meaning of visual signs (a skill that he ascribes to Charcot in his obituary of 1893) and to the interpretation of verbal signs, from the crudity of seeing to the subtlety of hearing.[150] Charcot understands the realism of the image to transcend the crudity of the spoken word. In a letter to Freud on 23 November 1891 he commented concerning the transcription of his famed Tuesday lectures that "the stenographer is not a photographer."[151] The assumption of the inherent validity of the gaze and its mechanical reproduction forms the image of the hysteric. The central argument that can be brought is that this vocabulary of seeing remains embedded in Freud's act of understanding the hysteric, who must be seen to be understood. This is not present in the earliest papers on hysteria written directly under Charcot's influence, such as Freud's differential diagnosis of organic and hysterical paralysis written in 1886.[152] For Freud the rejection of Charcot's mode of seeing the hysteric is also a rejection of the special relationship that the Jew has with the disease. The theme of the specific, inherited risk of the Jew for hysteria (and other forms of mental illness) was reflected in the work of Charcot which Freud translated.[153] But even more so this general claim about the hereditary risk of the Jew was
linked to a diagnostic system rooted in belief in external appearance as the source of knowledge about the pathological. For the seeing of the Jew as different was a topos of the world in which Freud lived. Satirical caricatures were to be found throughout the German-speaking world, which stressed the Jew's physical difference, and in the work of Charcot (and his contemporaries) these representations took on pathological significance.
Indeed, Freud's purchase of a lithograph of Brouillet's painting of Charcot in August of 1889 can well be understood as a compensation of Freud's rejection of Charcot's mode of seeing and representing the hysteric. Indeed, it must also be understood as a compensation for his abandonment of his identification with the anti-Semitic Jean-Martin Charcot[154] —for whom Jews, as the essential "moderns," were at special risk as hysterics—and his new alliance with the provincial Jew Hippolyte Bernheim.[155] Such a movement parallels the abandonment of ideas of trauma—still for Charcot the cause of hysteria (in women as well as in Jews)—and its replacement with the etiology of hysteria in the psyche. As Freud states:
For [the physician] will be able to convince himself of the correctness of the assertions of the school of Nancy [Bernheim] at any time on his patients, whereas he is scarcely likely to find himself in a position to confirm from his own observation the phenomena described by Charcot as "major hypnotism," which seem only to occur in a few sufferers from grande hysterie .[156]
It is the scientific "observation," the gaze of the Jew rather than the gaze directed at the Jew, which marks the distinction between Charcot and Bernheim. Freud's conversion to Bernheim's mode of seeing the "usual" rather than seeing the "unique" also marks the beginning of his rejection of reducing the origin of hysteria to the single, traumatic event.
This returns us to the problem of defining the visual precursors for Charcot and for Freud. We must trace the image of the epileptic and the meaning of trauma—two clearly linked images in Freud's vocabulary of the hysteric—to see how Freud's reading of the hysteric is linked through these images of trauma to the central image of difference, the Eastern European Jews as hysterics (or perhaps more accurately, provincial Jews as parvenus, out of their minds because they are out of their natural place). It is the discourse on the relationship between trauma and hysteria that provides the key to Freud's—and many of his contemporaries'—ambivalence concerning models for therapy.
Trauma is not a neutral concept. There has been a general acceptance
of the historical model of the "railway spine," hysterical trauma resulting from railway accidents, as a means of understanding the traumatic nature of hysteria at the turn of the century.[157] Indeed, in much of the early work on hysteria these images haunt the literature. The hysteric is the sufferer from traumatic neurosis similar to that caused by experiencing a train accident, as outlined by Herbert Page in his classic work, Injuries of the Spine and Spinal Cord (1883), and accepted in toto by Charcot in his work on the neurosis of fright or shock. Both men and women are therefore equally at risk for such forms of psychopathology. Hysteria is thus merely the direct (brain or spinal cord lesion) or indirect (shock) result of trauma. And here the confusion between the models of hysteria evolved by Charcot and Hughlings Jackson must be stressed. For the traumatic event causes hysteria only in those who are predisposed to being hysteric (Charcot), but the lesion caused by trauma also releases those subterranean aspects of our earlier evolution held in check by the highest order of neurological organization (Hughlings Jackson). The Jew is predisposed to hysteria both because of hereditary and consanguinity (incestuous inbreeding) and, as we shall see, by the trauma of civilization as represented by the Jews' predisposition to the somatic diseases linked to hysteria, such as syphilis.
The fin-de-siècle image of trauma is one with modern civilization, with the train. As Sir Clifford Allbutt, Professor of Medicine at Cambridge University, stated in an essay in the Contemporary Review of 1895:
To turn now . . . to nervous disability, to hysteria . . . to the frightfulness, the melancholy, the unrest due to living at a high pressure, the world of the railway, the pelting of telegrams, the strife of business . . . surely, at any rate, these maladies or the causes of these maladies are more rife than they were in the days of our fathers? To this question . . . there is, I know, but one opinion on the subject in society, in the newspapers, in the books of philosophers, even in the journals and treatises of the medical profession.[158]
And thus the railroad, railway accidents, and the speed of modern life all collaborate to create the hysteric. But nineteenth-century "railway" medicine faced a dilemma that later faced Sigmund Freud. Trauma—such as involvement in a railway crash—is the cause of hysteria, but why do not all individuals who are involved in railway crashes become hysteric? This question was answered in part by the neurologist C. E. Brown-Séquard, who, as early as 1860, had argued that there were hereditary transmissions of acquired injuries, as in the case of "animals born of parents having been rendered epileptic by an injury to the spinal
cord."[159] This view quickly becomes a standard one in the literature on "railway spine."[160]
The image of the hysteric being at risk because of his or her inheritance limited the field from which the hysteric could be drawn. Thus the physician could, under most circumstances, see him- or herself as a separate category, as distanced from the hysteric as from the child of alcoholics or criminals. But not the Jewish physician. For the Jewish physician is at risk no matter which theory of hysteria one accepted.[161] Some views using the model of biological determinism had it that the Jew was at risk simply from inheritance; some views sought after a sociological explanation. But both views, no matter what the etiology, saw a resultant inability of the Jew to deal with the complexities of the modern world, as represented by the Rousseauean city. The trauma of "modern life" was closely linked to the image of the city. For nineteenth-century medicine (whether psychiatry or public health), cities are places of disease and the Jews are the quintessential city dwellers, the Americans of Europe. Richard Krafft-Ebing believed that civilization regularly brings forth degenerate forms of sexuality because of the "more stringent demands which circumstances make upon the nervous system," circumstances that manifest themselves in the "psychopathological or neuropathological conditions of the nation involved."[162] For him (and for most clinical psychiatrists at the turn of the century) the Jew is the ultimate "city person" whose sensibilities are dulled, whose sexuality is pathological, whose materialistic, money-grubbing goals are "American," whose life is without a center. It is also the city that triggers the weakness hidden within the corrupted individual. It is its turbulence, its excitement, what August Forel in The Sexual Question (1905) calls its "Americanism," that leads to illnesses such as hysteria:
Americanism.—By this term I designate an unhealthy feature of sexual life, common among the educated classes of the United States, and apparently originating in the greed for dollars, which is more prevalent in North America than anywhere else. I refer to the unnatural life which Americans lead, and more especially to its sexual aspect.[163]
This is an image seen by physicians of the period as "Jewish" in its dimensions. Jews manifest an "abnormally intensified sensuality and sexual excitement that lead to sexual errors that are of etiological significance."[164] Jewish scientists, when they address this question directly, seek for a developmental rather than a hereditary reason for this evident higher rate of hysteria. They seek out the two-thousand-year Diaspora as the origin of trauma.[165] But this does not free them. Given the views
of Brown-Séquard, there is really little escape no matter what the cause. The Jew becomes the hysteric and the hysteria is measured by the sexual abnormality of the Jew.
Thus when we turn to Freud's case studies, either in the collaborative Studies in Hysteria of 1895 or in his later and much more complex studies, such as his study of Dora (1905 [1901]), we face the question of Freud's (and Breuer's) representation of the Jew—of his "seeing" (or, perhaps better, "hearing") the Jew. In an earlier study I argued that the image of Anna O. in Breuer's case-study contribution to the Studies in Hysteria masked the "Jewishness" of Bertha Pappenheim.[166] In Freud's own contributions (such as the case of Katherina or Miss Lucy R.) there is the attempt to universalize the image of the hysteric through the citation—not of cases of male hysteria—but those of non-Jewish hysterics. But the common qualities ascribed to the hysteric and the Eastern, male Jew remain central to the representation of this nosological category for Freud.
This can be seen in a close reading of what has become the exemplary "case of hysteria" for our contemporary reading of the history of hysteria, Freud's case of Dora.[167] Seen by contemporary feminist critics, such as Hélène Cixous, as "the core example of the protesting force of women,"[168] it is also the classic example of the transmutation of images of gender and race (masculinity and "Jewishness") into the raceless image of the feminine. Freud used the case of Dora to argue not only for the necessary publication of case studies, but also for the needed masking of the analysand. The disguising of the identity of Dora is complete. There is no sign in the case study of the "racial" identity of Ida Bauer, the Eastern European Jewish daughter of Philip Bauer, whose syphilis was treated by Freud some six years before the beginning of Dora's analysis. Charcot (and Freud) had attempted to distance the diseases of syphilis and hysteria, and yet a relationship between the two patterns of illness remained. This omission, such as Josef Breuer's omission of his patient's "racial" identity in his narrative of Anna O.'s case, while including it in his case notes, masks a salient aspect of the case. We can best quote Freud in this regard, when he returns to the 1895 case of Katherina in 1924 and observes concerning his replacement of the relationship with the patient's father with the word "uncle": "Distortions like the one which I introduced in the present instance should be altogether avoided in reporting a case history."[169]
Perhaps as important for our reading of the suppressed aspects of the case of Dora (Ida Bauer) is the fact that her beloved brother Otto Bauer was one of the founders of the Austrian Socialist Party. His attitude toward his Jewish identity is of importance. For Austro-Marxism
advocated cultural-national autonomy for all people within the diverse Hapsburg Empire—except for the Jews. These Marxists saw assimilation as inevitable and positive, and they tied assimilation to a distinct distaste for Yiddish (and subsequently Hebrew) as linguistic signs of a negative separatism (a sign that took on positive meaning when ascribed to Czech or Hungarian as "national" languages). While Otto Bauer was an "Eastern Jew" himself, as he was born of Bohemian ancestry in Vienna, he was ambivalent about the idea of race. "Race" was an acceptable label for the other national groups, since it was associated by them with positive ideas of autonomy, but for the Jews (especially Eastern Jews) it was always a sign of the pathological.[170] Bertha Pappenheim, Breuer's Anna O., stated it quite baldly in an essay published at the turn of the century. Raised in an orthodox Jewish home, for her the German-language schools developed in the Eastern reaches of the Hapsburg Empire were "a stronghold, often conquered in battle, in the fight against the malaise from which Galician Jewry suffers as from a hereditary disease."[171] It is the cure of this hereditary disease that Freud undertakes in treating Dora (and thus treating an aspect of his own identity). This is, indeed, the hidden meaning of the development of the idea of transference and countertransference which is nascent in the case of Dora and why Freud's own understanding of this process is blocked in this case.
The centerpiece of Freud's study of Ida Bauer is, according to Freud's argument, the attempt to explain the origin of a case of hysteria through the analysis of the Oedipal triangle as perceived by a patient whose object of attraction is of the same sex. The complex relationships are between her father (Philip), her mother (Käthe), and Dora; the father's lover (Frau K.) and her husband (Herr K.), the attempted seducer of Dora, who has traditionally been the focus of the interpretation of the study. Much time and effort has been expended to understand Freud's complex misreading of this case. What is clear is that there are a number of misreadings by Freud in the text. Jacques Lacan pointed out one of the central ones: that the globus hystericus manifested by Dora is interpreted by Freud as the symbolic representation of orality within a specific context in the case study. The lover's seduction of the impotent father is described in Freud's analysis as an act of fellatio rather than being understood as cunnilingus.[172] This displacement is, however, not merely the shift of Freud's focus from the genitalia of the female to those of the male. Rather it is a double displacement—for the act of fellatio is also the emblematic act of male homosexual contact. What such a displacement means can be found if the "scientific" context of the meaning of the act of fellatio in the medical debates of the nineteenth
century are followed. Through such a contextualization we can outline Freud's understanding of the transmission of a "disease" (the collapse of language as represented by the symptom of the globus hystericus in Ida Bauer) as necessarily associated with the act of sucking a male's penis.
Let us begin with this misreading as a sign of Freud's representation of the idea of race in the guise of the representation of the feminine, as it replaces the male's genitalia as the object of attraction—and, therefore, sight—with the woman's. For Freud the act of seeing one's genitalia is one which is especially "feminine": "The pride taken by women in the appearance of their genitals is quite a special feature of their vanity; and the disorders of the genitals which they think calculated to inspire feelings of repugnance or even disgust have an incredible power of humiliating them, of lowering their self-esteem, and of making them irritable, sensitive, and distrustful."[173] The special quality of seeing the female's genitalia, genitalia normally understood by Freud as presence in the fantasy of their absence, points toward the other genitalia, the male genitalia, seen by the male, which when "disordered" points toward pathological nature of the male. But what is this disorder? In the case study it is, on one level, the origin of Ida Bauer's understanding about the diseased nature of her genitalia, the syphilitic infection of her father. One of the most interesting qualities ascribed to the father from the very beginning of the case study is the fact that he was syphilitic. The relationship between the physical trauma of syphilis and the image of the syphilitic is central to understanding the image of the hysteric which Freud evolves in his study. In the case of Dora's father, his "gravest illness . . . took the form of a confusional attack, followed by symptoms of paralysis and slight mental disturbance."[174] Freud diagnoses this as a case of "diffuse vascular affection; and since the patient admitted having had a specific infection before his marriage, I prescribed an energetic course of antiluetic treatment."[175] Four years later the father brings his daughter to Freud for treatment. Freud argues in a footnote for the retention of the relationship between the etiology of hysteria in the offspring and the syphilitic infection of the father. "Syphilis in the male parent is a very relevant factor in the etiology of the neuropathic constitution of children."[176] Here is the trauma—this case of hysteria is a form of hereditosyphilis transmitted by the father. Freud's emphasis on this line of inheritance is not solely because Ida Bauer's father had evidently (according to the account in the case study) infected her mother (and therefore his daughter), but because the general laws of the inheritance of disease which were accepted during this period argued that the son inherits the diseases of the mother (and therefore her father) while the daughter in-
herits the diseases of the father (and therefore his mother).[177] Freud later uncovers another sign of this biological predisposition in the fact that "she had masturbated in childhood."[178] This is the link that brings together the trauma (the syphilitic infection of the father), the mode of transmission (sexual intercourse with a circumcised penis), the Jewishness of the father as represented in his pathological sexuality, and the hysterical neurosis of the daughter. The merging of various forms of illness, from syphilis to hysteria, is through the model of inherited characteristics. The "real" disease is the degeneracy of the parent, and its manifestation in specific illness can vary from individual to individual.[179] Thus syphilis and hysteria are truly forms of the same pattern of illness.
One reading of the case would be to say that hypersexual Jewish males pass on their Jewish disease to their daughters in the form of hysteria. But this discourse is present in Freud's text only if we contextualize the meaning of syphilis within the context of Freud's self-definition as a Jew and that of his patient, Ida Bauer.
Freud creates very early on a differential diagnosis between tabes dorsalis (a label for one of the late manifestations of syphilis) and hysteria, at least when it appears in a woman who is infected with syphilis. He undertakes this in an extended footnote at the very beginning of the study in which he documents the central diagnostic thesis of this case study: that it is the ordered narrative of the patient about her illness which is disrupted in the hysteric. In other words, the hysteric lies: "The patient's inability to give an ordered history of their life insofar as it coincides with the history of their illness is not merely characteristic of the neurosis. It also possesses great theoretical significance."[180] The relationship between the sexual etiology of the hysteric and the hysteric's discourse represents the underlying shift from an image of race to one of gender (for as we shall see, the discourse of the Jew is a primary marker of difference). The counterexample is brought in Freud's notes, a case study of a patient who "had been for years . . . treated without success for hysteria (pains and defective gait)." She narrates her "story . . . perfectly clearly and connectedly in spite of the remarkable events it dealt with." Freud concludes this "could not be . . . [a case] of hysteria, and immediately instituted a careful physical examination. This led to the diagnosis of a fairly advanced stage of tabes, which later was treated with Hg injections (Ol. cinereum) by Professor Lang with markedly beneficial results."[181] Here the image of the "defective gait," which is one of the hallmarks of the "hysteric" in the nineteenth century (and the history created for this image at the Salpêtrière), recurs, only to be revealed
as the final stages of syphilis. The irony is that it is Joseph Babinski whose neurological work at the Salpêtrière provided the clue for such an analysis of the impaired plantar reflex[182] and Charcot himself, in his work on intermittent claudication, who provided the racial context for such impairment.[183] (And, indeed, there is a link of intermittent claudication to the image of the hysteric.)[184] In this case of Dora, it is revealed only at the very close of the case that one of Dora's primary symptoms was that "she had not been able to walk properly and dragged her right foot. . . . Even now her foot sometimes dragged."[185] Freud sees this "disorder, the dragging of one leg," as having a "secret and possibly sexual meaning of the clinical picture."[186] Freud interprets this as a sign of the "false step" that Dora had imaged herself to have taken during the attempted seduction by Herr K. at the lake. Later Felix Deutsch, who treated Ida Bauer after she broke off her analysis with Freud, observed with surprise that the "dragging of her foot, which Freud had observed when the patient was a girl, should have persisted twenty-five years."[187] This remained a central sign for her affliction, a sign that is not solely the association between the accident she had as a child and the bed rest that accompanied it. For the incapacity of gait is also a racial sign in Ida Bauer's Vienna and is associated with the "impairment" of the Jew. For it is the Jew, in a long Austrian tradition as old as the eighteenth century, who is at greatest risk in having both impaired gait[188] and syphilis. It is this image in the case of Dora that links the impairment of the syphilitic and the hidden image of the Jew.
The association of the syphilitic infection of the father and the neurosis of the daughter is linked by Freud in his analysis of the physical symptom of leukorrhea, or genital catarrh, an increased "disgust[ing] . . . secretion of the mucous membrane of the vagina."[189] Dora associates this with her lesbian "disgust" toward Herr K.'s attempted heterosexual seduction (in Freud's reading) and the feeling of his "erect member against her body."[190] Freud's conclusion is that for Ida Bauer "all men were like her father. But she thought her father suffered from venereal disease—for had he not handed it on to her and to her mother? She might therefore have imagined to herself that all men suffered from venereal disease, and naturally her conception of venereal disease was modelled upon her one experience of it—a personal one at that. To suffer from venereal disease, therefore, meant for her to be afflicted with a disgusting discharge."[191] Freud thus interprets one of two dreams narrated to him by Dora in terms of the connection among the "disgusting catarrh," the wetness of bed-wetting and masturbation, and her mother's compulsive cleanliness. "The two groups of ideas met in
Charcot's diagnostic category of intermittent claudication was used
as a marker for racial difference. From P. Olivier and A. Halipré, "Claudication
intermittente chez un homme hystérique atteint de pouls lent permanen," La
Normandie Médicale 11 (1896): 23.
(Bethesda, Md.: National Library of Medicine.)
this one thought: 'Mother got both things from father: the sexual wetness and the dirtying discharge.'"[192] In the recurrent dream the connection (right word) is made through the symbolic representation of the "drops," the jewels that her mother wishes to rescue from the fire that threatens the family.[193] Freud interprets the "drops"—the jewelry [Schmuck ]—as a switch-word, while "jewelry" [Schmuck ] was taken as an equivalent to "clean" and thus as a rather forced contrary of "dirtied."[194] Freud stresses that the "jewels" become a "jewelcase" in the dream and that this term (Schmuckkasten ) is "a term commonly used to describe female genitals that are immaculate and intact."[195]
One can add another layer of misreading. As I have shown, there is a subtext in the hidden language of the Jews. In Viennese urban dialect, borrowed from Yiddish, Schmock has another meaning. Schmock even in German urban ideolect had come to be the standard slang term for the male genitals. The hidden meaning of the language of the Jews is identical to the lying of the hysteric, the central symptom of hysteria, according to Freud. This transference can be seen in Freud's early description of the discourse of two Eastern male Jews in a letter to his friend Emil Fluss on the return trip from Freiburg to Vienna in 1872:
Now this Jew talked the same way as I had heard thousands of others talk before, even in Freiburg. His face seemed familiar—he was typical. So was the boy with whom he discussed religion. He was cut from the cloth from which fate makes swindlers when the time is ripe: cunning, mendacious, kept by his adoring relatives in the belief that he is a great talent, but unprincipled and without character. I have enough of this rabble.[196]
The misreading of the text is a repression of the discourse of the male Eastern Jew—the parvenu marked by his language and discourse as different and diseased. Hidden within the female genitalia (the Schmuckkasten ) is the image of the male Jew as represented by his genitalia (the Schmock ). The replacement of the "Jewish" penis—identifiable as circumcised and, as we shall see, as diseased, by the "German" vagina stands at the center of Freud's revision of the identity of Ida Bauer.
In my study Jewish Self-Hatred , I have extensively shown that an ancient Western tradition labels the language of the Jew as corrupt and corrupting, as the sign of the inherent difference of the Jew.[197] This tradition sees the Jew as inherently unable to have command of any "Western"—that is, cultural—language (indeed, even the "holy language," Hebrew). The Jew is not only "not of our blood," as Monsignor Joseph Frings of Cologne expressed it in 1942, but also "does not speak our language."[198] For the acculturated Eastern Jew in Vienna, mauscheln ,
the speaking of German with a Yiddish accent, intonation, or vocabulary, is the sign of this difference. And this is the language of Freud's mother, Amalia Freud née Nathanson, the invisible woman in all of his autobiographical accounts. As Freud's son Martin noted, she was a Galician Jew from Brody who remained a typical Polish Jew, "impatient, self-willed, sharp-witted and highly intelligent." She retained the language, manner, and beliefs of Galicia:
[She was] absolutely different from Jews who had lived in the West for some generations. . . . These Galician Jews had little grace and no manners; and their women were certainly not what we should call "ladies." They were highly emotional and easily carried away by their feelings. . . . They were not easy to live with, and grandmother, a true representative of her race, was no exception. She had great vitality and much impatience.[199]
It is in the image of the mother that the qualities ascribed to the hysteric, to Ida Bauer, can be found. In suppressing the shift of language, Freud also suppresses the "hidden" reference to the "Jewish" penis. The hidden discourse of the Jew, hidden within the high German culture discourse, is ignored.
This "misreading" of the female for the male organ is in truth a "misseeing" of the genitalia as Freud traces the origin of Ida Bauer's knowledge of the act of fellatio, the "seeing" as well as sucking of the male member. Freud understands this "so-called sexual perversion" as being "very widely diffused among the whole population, as everyone knows except medical writers upon the subject. Or, I should rather say, they know it too; only they take care to forget it at the moment when they take up their pens to write about it. So it is not to be wondered at that this hysterical girl of nineteen, who had heard of the occurrence of such a method of sexual intercourse (sucking at the male organ), should have developed an unconscious phantasy of this sort and should have given it expression by an irritation in her throat and by coughing."[200] Freud reports that Dora's governess, to whom she was evidently as attracted as she was to Frau K., "used to read every sort of book on sexual life and similar objects, and talked to the girl about them, at the same time asking her quite frankly not to mention their conversations to her parents, as one could never tell what line they might take about them."[201] But it is clear according to Ida Bauer's account that she did not only "hear" about such sexual activity but learned about it in quite another way. Later in the case study, after Freud had begun to explain the homosexual attraction which Dora felt for Frau K., this narrative shifts.
After Dora's father writes to Herr K. to demand an explanation of his actions toward his daughter, Herr K. "spoke of her with disparagement, and produced as his trump card the reflection that no girl who read such books and was interested in such things could have any title to a man's respect. Frau K. had betrayed her and had calumniated her; for it had only been with her that she had read Mantegazza and discussed forbidden topics."[202] It is the book, a foreign book, that "infects" her, and makes her "sick," that is, "hysteric." Like her governess, Frau K. had used her to get access to her father. This "error" in Freud's image of the etiology of hysteria is a displacement of the image of the infected and the infecting onto the world of high culture—not "German" high culture (Bildung ), of course, but the medical culture of the sexologist.
Paolo Mantegazza (1831-1901) was one of the standard ethnological sources for the late nineteenth century for the nature of human sexuality. His three-volume study of the physiology of love, the hygiene of love, and the anthropology of love was the standard popular introduction to the acceptable social discourse on sexuality in late nineteenth-century Europe.[203] His importance for Freud should not be underestimated. One of a group of physician-anthropologists (such as Cesare Lombroso), Mantegazza had pioneered the introduction of the study (and enjoyment) of Erthroxylon coca and its derivative, cocaine, in the late 1850s. Following the publication of Darwin's Descent of Man , Mantegazza became one of Darwin's most avid correspondents (and sources), supplying Darwin with a series of "anthropological" photographs that Darwin used for his later work.
Mantegazza's work, like that of Charcot, emphasized the "seeing" of difference, a view that is epitomized in Mantegazza's basic study of physiognomy and expression of 1885. But for late nineteenth-century science the controversial centerpiece of Mantegazza's work is his trilogy on love and sex: Fisiologia dell' amore (1872), Igiene dell' amore (1877), and Gli amori degli uomini (1885).[204] Cited widely by sexologists from Cesare Lombroso, Richard Krafft-Ebing, Havelock Ellis, and Iwan Bloch to Magnus Hirschfeld, Mantegazza remained one of the accessible, "popular" sources for scientific knowledge (and misinformation) for the educated public at the turn of the century. It is clear that Ida Bauer could have read (and probably did read) either Mantegazza or similar texts, whether under the tutelage of her companion or on her own initiative. What is of interest is how Freud reads this contradiction in her account: Did she read them, or only hear about their content? What is inherently dangerous about Mantegazza from the standpoint of Freud's refusal to relate to the accusation that Ida Bauer had read him? If we turn to
the trilogy, it is clear (and Madelon Spregnether agrees[205] ) that the text that best fits the pejorative description of Herr K. is the final text in this series, on the anthropology of sexuality.[206] There one finds an extended discussion of "the perversions of love," including "mutual onanism," "lesbianism and tribadism," as well as "histories" of these practices. (However, there are similar discussions in the seventh chapter of Mantegazza's study on the "hygiene of love," which details the "errors of the sexual drive.")
Now this is clearly what Freud should have understood—given his reading—as of importance to Ida Bauer, but what in this volume would have been of importance to Sigmund Freud? If we turn to the chapter after the one on "perversions," we come to a detailed discussion of the "mutilation of the genitals," which recounts the history of these practices among "savage tribes" including the Jews. Indeed, it is only in Mantegazza's discussion of the Jews that the text turns from a titillating account of "unnatural practices" into an Enlightenment polemic against the perverse practices of that people out of their correct "space" and "time"—the Jews:
Circumcision is a shame and an infamy; and I, who am not in the least anti-Semitic, who indeed have much esteem for the Israelites, I who demand of no living soul a profession of religious faith, insisting only upon the brotherhood of soap and water and of honesty, I shout and shall continue to shout at the Hebrews, until my last breath: Cease mutilating yourselves: cease imprinting upon your flesh an odious brand to distinguish you from other men; until you do this, you cannot pretend to be our equal. As it is, you, of your own accord, with the branding iron, from the first days of your lives, proceed to proclaim yourselves a race apart, one that cannot, and does not care to, mix with ours.
It is circumcision that sets the (male) Jew apart. In his dissertation of 1897 Armand-Louis-Joseph Béraud notes that the Jews needed to circumcise their young males because of their inherently unhygienic nature, but also because the "climate in which they dwelt" otherwise encouraged the transmission of syphilis.[207] The Jew in the Diaspora is out of time (having forgotten to vanish like the other ancient peoples); is out of correct space (where circumcision had validity). His Jewishness (as well as his disease) is inscribed on his penis.
But what does circumcision mean for a Viennese Jewish scientist at the end of the 1800s? The debates within and without the Jewish communities concerning the nature and implication of circumcision surfaced again in Germany during the 1840s. German Jews had become
acculturated into German middle-class values and had come to question the absolute requirement of circumcision as a sign of their Jewish identity. Led by the radical reform rabbi Samuel Holdheim in Germany and responding to a Christian tradition that denigrated circumcision, the debate was carried out as much in the scientific press as in the religious one.[208] There were four "traditional" views of the "meaning" of circumcision since the rise of Christianity. Following the writings of Paul, the first saw circumcision as inherently symbolic and, therefore, no longer valid after the rise of Christianity (this view was espoused by Eusebius and Origen); the second saw circumcision as a form of medical prophylaxis (as in the writing of Philo but also in the work of the central German commentator of the eighteenth century, Johann David Michaelis); the third saw it as a sign of a political identity (as in the work of the early eighteenth-century theologian Johann Spencer); the fourth saw it as a remnant of the early Jewish idol or phallus worship (as in the work of the antiquarian Georg Friedrich Daumer—this view reappears quite often in the literature on Jewish ritual murder).
In the medical literature of the time, two of these views dominated. They were the views that bracketed the images of "health" and "disease." These views saw circumcision either as the source of disease or as a prophylaxis against disease—and in both cases syphilis and masturbation, the two "diseases" that dominate the case of Dora, play a major role. Mantegazza notes that "the hygienic value of circumcision has been exaggerated by the historians of Judaism. It is true enough that the circumcised are a little less disposed to masturbation and to venereal infection; but every day, we do have Jewish masturbators and Jewish syphilitics. Circumcision is a mark of racial distinction; . . . it is a sanguinary protest against universal brotherhood; and if it be true that Christ was circumcised, it is likewise true that he protested on the cross against any symbol which would tend to part men asunder." The opposing view of circumcision in the scientific literature of the time saw circumcision as a mode of prevention that precluded the transmission of sexually transmitted diseases because of the increased capacity for "cleanliness."[209] It is classified as an aspect of "hygiene," the favorite word to critique or support the practice. (This view is closely associated with the therapeutic use of circumcision throughout the nineteenth century as a means of "curing" the diseases caused by masturbation, with, of course a similar split in the idea of efficacy: circumcision was either a cure for masturbation, as it eliminated the stimulation of the prepuce and deadened the sensitivity of the penis, or it was the source of Jewish male hypersexuality.)
A detailed medical literature links the very act of circumcision with
the transmission of syphilis, so that the prophylaxis becomes the source of infection. The literature that discusses the transmission of syphilis to newly circumcised infants through the ritual of metsitsah , the sucking on the penis by the mohel , the ritual circumciser, in order to staunch the bleeding, is extensive and detailed.[210]
The metsitsah was understood by the scientific community of the nineteenth century as a "pathological" one, as it was labeled as the source of the transmission of disease from the adult male to the male child. In the establishment of the Viennese Jewish community during the course of the early nineteenth century the debate on the abolition of circumcision was heard as loudly as anywhere else in Central Europe. Isaac Noah Mannheimer, the rabbi of the Seitenstettengasse synagogue and the de facto "chief rabbi" of Vienna (although this title did not officially exist), while a follower of Reformed Judaism, opposed the more radical "reforms" of theologians such as Samuel Holdheim. He strongly advocated the retention of Hebrew as the language of prayer (even though he had preached in Danish during his tenure in Copenhagen) and opposed mixed marriages and the abolition of circumcision. (The link among these three central issues in the self-definition of Viennese Jewry at mid-century should be stressed.) While no compromise was found on the first two issues (Hebrew was maintained as the language of the liturgy and mixed marriages were not authorized), a striking compromise was found in the third case. Together with Rabbi Lazar Horowitz, the spiritual leader of the orthodox community in Vienna, they abolished the practice of the metsitsah .[211] Although Horowitz was a follower of the ultraorthodox Pressburg Rabbi Moses Sofer, the abolition of the metsitsah became a marker between the practices of Viennese Jewry (which did not permit it for "hygienic" reasons) and the tradition of Eastern Jewry, such as the Jews of Pressburg and Freiburg (where Freud was circumcised).
Here is the link between the emphasis on fellatio in Freud's reading of the case of Dora and the syphilis that haunts the image of the (male) Jew in the case. It is the male sucking the penis of a male in the act of circumcision. Especially in the Viennese debates concerning the retention or abolition of circumcision, this "act" played a special role. For Freud the act of fellatio would be a sign not only of "perversion" but also of the transmission of disease; it would also be a sign that incorporated his own relationship between his racial identity with his coreligionists and, indeed, with other male authority figures. Thus the act of the female sucking on the penis of the male, a "pathological" act as it represents the spread of disease (hysteria) to the daughter, is a sub-
limation of the act of the male sucking on the penis of the male and spreading another disease, syphilis. It also represents, in the period during which Freud was writing and rewriting the case of Dora, Freud's own articulation of the end of his "homosexual" (i.e., homoerotic) relationship with Wilhelm Fliess, whose theories about the relationship between the nose and the penis are echoed in this case study as well as elsewhere in the fin-de-siècle work of Freud.[212]
But reading Mantegazza, we can go one step farther in our analysis of Freud's understanding of the meaning of sexually transmitted disease and its relationship to hysteria. For Mantegazza introduces his discussion of the exclusivity of the Jews with the following discussion:
It is altogether likely that the most important reason that has led men of various ages and of varying civilizations to adopt the custom of cutting off the prepuce has been that it was felt to be necessary to imprint upon the human body a clear and indelible sign that would serve to distinguish one people from another and, by putting a seal of consecration upon nationality, would tend to impede the mixture of races. A woman, before accepting the embraces of a man, must first make sure, with her eyes and with her hands, as to whether he was of the circumcised or the uncircumcised; nor would she be able to find any excuse for mingling her own blood-stream with that of the foreigner. It had, however, not occurred to the legislator that this same indelible characteristic would inspire in the woman a curiosity to see and to handle men of a different sort.
The seduction of the Jewish woman by the Other—whether the non-Jew or the lesbian—is the result of the "seeing" of the difference in the form of the genitalia. The need to "see" and "touch" the Other is the fault of the circumcised (male) Jew, whose very physical form tempts the female to explore the Other. Here we have another form of the displacement of the act of touching (sexual contact) with the permitted (indeed, necessary) act of seeing, but given a pathological interpretation. The rejection of mixed marriage and conversion by even "godless" Jews such as Sigmund Freud at this time is a sign of the need to understand the separateness of the Jew as having a positive valence. The labeling of converts as "sick" becomes a widely used fin-de-siècle trope.[213]
Ida Bauer's act of seeing her father is the act of seeing the (male) Jew. Central to the definition of the Jew—here to be understood always as the "male" Jew—is the image of the male Jew's circumcised penis as impaired, damaged, or incomplete and therefore threatening. The literature on syphilis—which certainly played a role in Freud's understanding of her father's illness as well as that of the daughter—contains a substantial discussion of the special relationship of Jews to the transmission and
meaning of syphilis. For it is not only in the act of circumcision that this association is made—it is in the general risk of the Jews as the carriers of syphilis and the generalized fear that such disease would undermine the strength of the body politic. Central to the case of Ida Bauer is a subtext about the nature of Jews, about the transmission of syphilis, and about the act of circumcision.[214] Both are associated with the image of the hysteric. It is Jewishness that is the central category of racial difference for the German reader and writer of the turn of the century.[215]
For the Jew in European science and popular thought was closely related to the spread and incidence of syphilis. Such views had two readings. The first model saw the Jews as the carriers of sexually transmitted diseases who transmitted them to the rest of the world. And their location is the city—Vienna. Here the link between the idea of the Jew as city dweller, as the disease that lurks within the confinement of the urban environment, becomes manifest. The source of the hysteria of the city is the diseased sexuality of the Jew. This view is to be found in Adolf Hitler's discussion of syphilis in turn-of-the-century Vienna in Mein Kampf (1925). There he (like his Viennese compatriot Bertha Pappenheim[216] ) links it to the Jew, the prostitute, and the power of money:
Particularly with regard to syphilis, the attitude of the nation and the state can only be designated as total capitulation. . . . The invention of a remedy of questionable character and its commercial exploitation can no longer help much against this plague. . . . The cause lies, primarily, in our prostitution of love. . . . This Jewification of our spiritual life and mammonization of our mating instinct will sooner or later destroy our entire offspring.[217]
Hitler's views also linked Jews with prostitutes and the spread of infection. Jews were the archpimps—Jews ran the brothels—but Jews also infected their prostitutes and caused the weakening of the German national fiber.[218] But also, Jews are associated with the false promise of a medical cure separate from the social cures that Hitler wishes to see imposed—isolation and separation of the syphilitic and his or her Jewish source from the body politic. Hitler's reference is to the belief that especially the specialty of dermatology and syphilology was dominated by Jews, who used their medical status to sell quack cures.
The second model that associated Jews and syphilis seemed to postulate exactly the opposite—that Jews had a statistically lower rate of syphilitic infection—because they had become immune to it through centuries of exposure. In the medical literature of the period, reaching across all of European medicine, it was assumed that Jews had a notably
lower rate of infection. In a study of the incidence of tertiary lues in the Crimea undertaken between 1904 and 1929, the Jews had the lowest consistent rate of infection.[219] In an eighteen-year longitudinal study H. Budel demonstrated the extraordinarily low rate of tertiary lues among Jews in Estonia during the prewar period.[220] All these studies assumed that biological difference as well as the social difference of the Jews were at the root of their seeming immunity.
Jewish scientists also had to explain the statistical fact of their immunity to syphilis. In a study of the rate of tertiary lues, the final stage of the syphilitic infection, undertaken during World War I, the Jewish physician Max Sichel responded to the general view of the relative lower incidence of infection among Jews as resulting from the sexual difference of the Jews.[221] He responds—out of necessity—with a social argument. The Jews, according to Sichel, show lower incidence not only because of their early marriage and the patriarchal structure of the Jewish family, but also because of their much lower rate of alcoholism. They were, therefore, according to the implicit argument, more rarely exposed to the infection of prostitutes, whose attractiveness was always associated with the greater loss of sexual control in the male attributed to inebriety. The relationship between these two "social" diseases is made into a cause for the higher incidence among other Europeans. The Jews, because they are less likely to drink heavily, are less likely to be exposed to both the debilitating effects of alcohol (which increase the risk for tertiary lues) as well as the occasion for infection. In 1927 H. Strauss looked at the incidences of syphilitic infection in his hospital in Berlin in order not only to demonstrate whether the Jews had a lower incidence but also to see (as in the infamous Tuskegee experiments among blacks in the United States) whether they had "milder" forms of the disease because of their life-style or background.[222] He found that Jews had indeed a much lower incidence of syphilis (while having an extraordinarily higher rate of hysteria) than the non-Jewish control. He proposes that the disease may well have a different course in Jews than in non-Jews. The marker for such a view of the heightened susceptibility or resistance to syphilis is the basic sign of difference of the Jews, the circumcised phallus.
The need to "see" and "label" the Jew at a time when Jews were becoming more and more assimilated and therefore "invisible" in Germany made the association with socially stigmatizing diseases that bore specific visible "signs and symptoms" especially appropriate. Mantegazza's view links the act of "seeing" the Jew sexually with the defamed practice of circumcision. In the German empire of the late nineteenth century all of the arguments placed the Jew in a special relationship to
syphilis and, therefore, in a very special relationship to the healthy body politic that needed to make the Jew visible. (The central medical paradigm for the establishment of the healthy state was the public health model that evolved specifically to combat the evils of sexually transmitted disease through social control.) Western Jews had been completely acculturated by the end of the nineteenth century and thus bore no external signs of difference (unique clothing, group language, group-specific hair and/or beard style). They had to bear the stigma of this special relationship to their diseased nature literally on the skin, where it could be seen. Not only on the penis where (because of social practice) it could be "seen" only in the sexual act. And then, because of the gradual abandonment of circumcision, be "seen" not to exist at all!
Just as the hysteric is constructed out of the perceived ability to categorize and classify categories of difference visually, the syphilitic Jew has his illness written on his skin. The skin of the hysteric, like the physiognomy of the hysteric, reflects the essence of the disease. Thus the skin becomes a veritable canvas onto which the illness of the hysteric is mapped. Seeing the hysteric means reading the signs and symptoms (the stigmata diaboli ) of the disease and representing the disease in a manner that captures its essence. It is the reduction of the ambiguous and fleeting signs of the constructed illness of the hysteric (constructed by the very nature of the definition of the disease in the nineteenth century). If the idea of the hysteric is tied to the idea of the feminization of the healthy Aryan male, or his "Jewification" (to use one of Hitler's favorite terms), then the representation of the disease must be in terms of models of illness that are convertible into the images of the feminized male. But these images of feminization are also tied to other, salient, fin-de-siècle images of race. For Jews bear the salient stigma of the black skin of the syphilitic, the syphilitic rupia .
The Jews are black, according to nineteenth-century racial science, because they are "a mongrel race which always retains this mongrel character." That is Houston Stewart Chamberlain arguing against the "pure" nature of the Jewish race.[223] Jews had "hybridized" with blacks in Alexandrian exile. They are, in an ironic review of Chamberlain's work by Nathan Birnbaum, the Viennese-Jewish activist who coined the word Zionist , a "bastard" race the origin of which was caused by their incestuousness, their sexual selectivity.[224] But the Jews were also seen as black. Adam Gurowski, a Polish noble, "took every light-colored mulatto for a Jew" when he first arrived in the United States in the 1850s.[225] Jews are black because they are different, because their sexuality is different, because their sexual pathology is written upon their skin. Gurowski's
"German-Jewish" contemporary, Karl Marx, associates leprosy, Jews, and syphilis in his description of his archrival Ferdinand Lassalle (in 1861): "Lazarus the leper, is the prototype of the Jews and of Lazarus-Lassalle. But in our Lazarus, the leprosy lies in the brain. His illness was originally a badly cured case of syphilis."[226] The pathognomonic sign of the Jew is written on the skin; it is evident for all to see.
The pathological image of the Jew was part of the general cultural vocabulary of Germany. Hitler used this image over and over in Mein Kampf in describing the Jew's role in German culture: "If you cut even cautiously into such an abscess, you found, like a maggot in a rotting body, often dazzled by the sudden light—a kike! . . . This was pestilence, spiritual pestilence, worse than the Black Death of olden times, and the people were being infected by it."
"Plague" (Seuche ) and pestilence (Pestilenz )—a disease from without, which, like syphilis, rots the body—was the model used to see the role of the Jew. The syphilitic weakening of the racially pure Germans by the Jews was likened by Hitler to the corruption of the blood of the race through another form of "mammonization," interracial marriage:
Here we have before us the results of procreation based partly on purely social compulsion and partly on financial grounds. This one leads to a general weakening, the other to a poisoning of the blood, since every department store Jewess is considered fit to augment the offspring of His Highness—and indeed the offspring look it. In both cases complete degeneration is the consequence.
If the Germans (Aryans) are a "pure" race—and that is for turn-of-the-century science a positive quality—then the Jews cannot be a "pure" race. Their status as a mixed race became exemplified in the icon of the Mischling during the 1930s. The Jewishness of the Mischling , to use the term from racial science that is parallel to "bastard" (the offspring of a "Black" and a "White" "race"), "looks" and sounds degenerate. They can have "Jewish-Negroid" [jüdisch-negroid ] features.[227] And this is often associated with their facile use of language, "the use of innumerable foreign words and newly created words to enrich the German language in sharp contrast to the necessary simplicity of the language of Germanic students."[228] The Jew's language reflects only the corruption of the Jew and his or her discourse. It is the sign of the "pathological early development" of the Mischling , who, as an adult, is unable to fulfill the promise of the member of a pure race. The weakness, but also the degenerate facility, of the Mischling is analogous to the image of the offspring of the syphilitic. And thus we come full circle. For the Jew is contaminated
by hysteria, whether it is the result of the trauma of infection or of heredity. And this weakness of the race is hidden within the corrupted (and corrupting) individual. Thus Hitler's image of the Mischling is on the offspring of a "Jewish" mother and an "Aryan" father—hidden within the name and Germanic lineage of the child is the true corruption of the race, the maternal lineage of the Jew. And as Jews claimed their lineage through the mother (rather than through the father as in German law) the Mischling becomes the exemplary hidden Jew just waiting to corrupt the body politic.
The image of the Mischling , the person impaired because of his or her heritage, brings us back full circle to the world of Ida Bauer. For here we have all of these themes of Jewish disposition and racial diagnosis summarized. The images that haunt Freud's representation of Ida Bauer—her language, the sexual acts of her imagination, their source, the relationship between pathology and infection—are all "racially" marked (at least notionally) in turn-of-the-century medical culture. For Freud, abandoning the act of seeing, an act made canonical in the work of his anti-Semitic mentor Charcot, is an abandonment of the associations of sight within this discourse of sexual difference. The case of Dora is an example of the power over language, of Freud's control over the language of his text, which reveals him not to be an Eastern Jew. Like his critique of the bad Greek of his critics when he held his first talk on male hysteria in Vienna, Freud is the master of the discourse of science and culture. Freud is a scientist who uses language as a scientist. In introducing the question of the nature of Ida Bauer's attraction to Frau K. he remarks: "I must now turn to consider a further complication, to which I should certainly give no space if I were a man of letters engaged upon the creation of a mental state like this for a short story, instead of being a medical man engaged upon its dissection." The act of writing the story is the sign of his special control of a "neutral" language, one that, as we have shown, is hardly neutral when it comes to placing Freud, the Eastern male Jew, at its center of risk. The meaning of the act of seeing for the Jewish physician shows the inherent truth of Robert Reininger's claim that "Unser Weltbild ist immer zugleich ein Wertbild,"[229] that we construct our understanding of the world from our internalized system of values.