Chapter Fourteen
Diseases of the Aorta
Diseases of the aorta may affect the function of the heart directly or indirectly. Two congenital abnormalities affecting the left ventricle have already been discussed in chapter 11: coarctation of the aorta and supravalvular aortic stenosis. This chapter offers a brief discussion of the common acquired abnormalities of the aorta.
Atherosclerosis of the Aorta
The most important disease of the vascular system, atherosclerosis, affects the aorta as well as the smaller arteries. Yet the consequences of atherosclerotic disease in the aorta are less pronounced than in the arteries supplying blood to the heart, brain, or kidneys, which may suffer serious damage because of occlusion. Atherosclerotic changes in the intima (inner lining) of the aorta are similar to those in the intima of the smaller arteries but rarely grow large enough to interfere with the blood flow in this vessel. Changes in the aortic intima have no direct effect on its function, although atherosclerotic ulcers may become a source of thrombi, which could break loose and cause emboli in distant organs.
A special situation exists when atherosclerosis of the intima is combined with arteriosclerotic abnormalities of the aorta. The media (middle layer) of the aortic wall can then be weakened to the point that the pressure in the aorta causes a ballooning of a portion of its wall into an aneurysm.
Diseases of the Aortic Root
The aortic root—the portion of the aorta immediately above the aortic value—and its extension, the lower part of the ascending aorta, are vulnerable to diseases other than atherosclerosis. Enlargement of the aortic root may be associated with dilatation of the ring to which aortic valve cusps are attached, thereby producing incompetence of that valve. A variety of conditions may cause abnormal dilatation of the aortic root and the lower ascending aorta—either a diffuse widening or a localized bulge (aneurysm). These include aortitis (inflammation of the ascending aorta), Marfan's syndrome (congenital weakness), and degeneration of the aorta.
Aortitis was once a common sequel of tertiary syphilis (luetic aortitis ). Before antibiotic treatment of syphilis was discovered in the 1940s, aortic aneurysm signaled the terminal stage of that disease. Today it is rarely encountered. Aortitis is now most often associated with autoimmune diseases, such as rheumatoid arthritis, which may produce severe aortic regurgitation.
Marfan's syndrome is a hereditary condition in which the connective tissue is defective, causing structural weakness of various parts of the body. In the aorta it may produce dilatation with aortic regurgitation, aortic aneurysms, and dissection of the aorta.
Atherosclerotic changes in the aorta, as mentioned, may produce aortic aneurysms and become a source of emboli in the systemic circulation.
Aneurysms of the Aorta
Two kinds of aneurysm of the ascending aorta are shown in figure 38, saccular (b) and fusiform (c). A third type is traumatic aneurysm, an occasional sequel of "steering-wheel injury" in automobile accidents, usually affecting the descending thoracic aorta. The commonest location of degenerative aortic aneurysm affecting the elderly is the abdominal aorta. Aneurysm of the abdominal aorta generally produces no symptoms: only rarely does pain result from pressure on abdominal organs. The aneurysm, however, is of concern, for its rupture can cause sudden death due to fatal hemorrhage. Fortunately, rupture is frequently preceded by small openings in the aorta through which blood can escape, infiltrating the
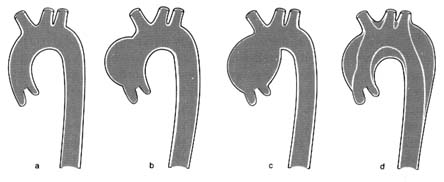
Figure 38. Diseases of the aorta. (a) Normal outline of the aorta. (b) Saccular aortic aneurysm.
(c) Fusiform aortic aneurysm. (d) Dissection of the aorta.
neighboring tissue and producing symptoms; the aneurysm can then be diagnosed and surgically resected in time. The presence of abdominal aneurysms can be detected on physical examination of the abdomen in a slim person but could escape attention in someone obese. Abdominal X ray may suggest the presence of an aneurysm, which can then be outlined by ultrasound. Direct demonstration of the aneurysm by angiography is seldom needed.
Surgical resection of the aneurysm of the abdominal aorta is a common prophylactic operation. There is some controversy about the advisability of performing this operation on persons in their seventies or eighties since at that age it carries a significant risk and often requires a long hospital stay. Unless the aneurysm discovered is large, many experts suggest that its size be monitored over time and the operation performed only if growth is noticed.
Aortic dissection (also called "dissecting aneurysm") is a dangerous condition that can lead to catastrophic emergencies. Dissection means separation of the inner and outer layers of the aorta produced by a tear in the intima; blood can then enter the space between the layers and widen it into a channel (see figure 38d). Blood can flow through the artificial channel parallel to the normal lumen of the aorta and reenter the latter through an exit tear. Once considered a specific disease caused by genetic cystic degeneration of the aortic media, it is now accepted that aortic dissection may be due to the aging process alone. The usual underlying factor for aortic dissection is hypertension.
Various types of dissection are recognized. The tear may develop
in the aortic root and affect only the ascending aorta, with the exit channel in the aortic arch. Another type of dissection involves the entire length of the aorta, with the entry tear in the aortic root and the exit tear in the abdominal aorta, producing a double-lumen aorta. A third type of dissection affects the descending thoracic aorta communicating with the abdominal aorta. This variety may be part of traumatic aortic aneurysm.
The principal danger of aortic dissection is rupture of the rather weak outer wall of the new channel and fatal hemorrhage. Dissection of the ascending aorta has some specific consequences. The artificial channel, in which blood is under high pressure (equal to that in the aorta), may constrict the exit of arterial branches of the aorta, producing decreased blood flow to the head and upper extremities. Furthermore, dissection of the aortic root above the aortic valve may distort the aortic orifice to a point that the normal aortic leaflets can no longer close tightly during diastole; hence, severe acute aortic regurgitation may develop. Occlusion of arterial branches of the aorta from the dissection may include coronary arteries, producing myocardial infarction, or the carotid artery, producing stroke.
The abrupt onset of a tear in the aorta is almost always associated with severe pain in the chest, yet the condition must not be mistaken for myocardial infarction. Even though myocardial infarction is a hundred times more common than aortic dissection, the medical team in an emergency unit must be able to distinguish them if proper lifesaving treatment is to be administered. Since the size of the new channel is related to the elasticity of the adventitia (outer layer) of the aorta, sometimes the channel is narrow, the outer wall firm, and the consequences minimal. The initial chest pain may be ignored or misdiagnosed, and the condition may remain unrecognized until much later (as "chronic" dissection of the aorta).
Treatment of aortic dissection consists of medical management or surgical resection of the dissected portion of the aorta and its replacement with a synthetic graft. This heroic operation carries a high risk; nonetheless, it has been performed in certain cardiac treatment centers with reasonable success. The timing of the operation varies: immediate surgery is indicated if serious consequences of the dissection are in evidence. Medical treatment may include the use of drugs to reduce blood pressure and decrease the force with which the blood is ejected into the aorta.