AIDS, Gender, and Biomedical Discourse: Current Contests for Meaning
Paula A. Treichler
Introduction: AIDS and the Challenge to Semantic Imperialism
Colin Douglas's 1975 novel The Intern 's Tale (set in a teaching hospital in Edinburgh) savages virtually every aspect of modern academic medicine—including its rampant and unreflective sexism. The book betrays its satire at the end, however, when two of the interns, Campbell and his friend, Mac, hospitalized with hepatitis B, deduce that the source of their infection is that well-known villain, the sexually active, unmarried woman:
Campbell sat silent, with a ghastly sensation of falling and accelerating and knowing that the worst feeling was still to come. When it did it was a horrible realisation.
"Christ! It's bloody Maggie!"
"What is?" said Mac gently.
"Maggie. Spreading it. Giving us bloody hepatitis."
. . ."Christ yes. It all fits." . . .
"Listen," said Campbell. "This is nasty and I'm sorry but it's important. When you were stopping by with old Maggie, did you use . . . what you might call an obstructive method of contraception?"
"Nope," said Mac. "Bareback."
"Charming. Me too. . . . I didn't because she said something about just finishing a period."
"That's not true. Not that week anyway. But she's got something far wrong with her cycle. Always dripping."[1]
It is a commonplace of feminist scholarship to claim that medical discourse represents women's bodies as pathological and contaminated.[2] But as this fictional conversation suggests, these representations bear complex historical burdens. Contamination is certainly one feature of Woman here: Maggie—an unmarried nurse generally regarded as a readily compliant sexual object—is suddenly transformed into an unruly agent of disease, actively "spreading" hepatitis to her sexual partners, including many of the hospital's medical staff. As they compare notes, the interns find she has lied to them, passing off the symptoms of serious pathology as a routine female complaint: Her lie can only succeed, of course, because both interns are ready to attribute the signs of pathology to the expected vicissitudes of the female menstrual cycle.[3] Thus, Maggie, like women elsewhere in the book and elsewhere in the history of medicine, is not what she seems.[4] From the perspective of the interns, she has tricked them into the potentially fatal risk of having intercourse "bareback," without protective contraception. Maggie's sexuality infects them with the possibility of their own mortality; at the same time, they express no concern about hers. For she who appeared to be a victim is now revealed as a deeply duplicitous perpetrator, a mimic of the symptoms and illnesses of others: Her dupes are the interns, whose only crime was to behave like "real men."[5]
The language as well as the narrative itself enacts this judgment. The carrier of "bloody hepatitis" is herself called "bloody Maggie"; the adjective bloody , linking the carrier, or source, of the disease with the disease itself, suggests indeed that Maggie, not a virus, causes hepatitis: she who is infected is simultaneously both infectious (a state or condition) and infecting (an active agent of disease). The word bloody also doubles as a literal description of Maggie's offcycle bleeding and as a broader cultural epithet (in American English, fucking doubles in a similar way). The images of diseased blood and body fluid invoke a long tradition in scientific and medical writing (see Ludvik Fleck's account of the history of syphilis, for example, where "bad blood" was a central concept).[6] With respect to the medical construction of women's bodies, a final point here is that men are the constructors, women the constructed. Despite the attribution of active agency to Maggie as a source of pathology, it is only the two male interns, the physician-scientists, who actively bring mind and knowledge to bear upon the situation. They alone have the right to analyze the situation with an appropriately trained "clinical eye" and to engage in those key activities of privileged theorizing, diag-
nosis of the disease, and authoritative identification of its cause.[7] Heirs of an ancient medical legacy of semantic and gendered imperialism, they define Maggie without hesitation as "bloody" and "always dripping." No longer containable through cultural pressure or moral prescription, freely infecting man after man, the sexually active container must therefore be contained. Their words contain, but also silence her.[8]
This chapter is about the ways that words, or more precisely, discourse, enact and reinforce deeply entrenched, pervasive, and often conservative cultural "narratives" about gender; it is also about how words seek, ultimately, to contain and control women's unruly and "uncontainable" properties. I will focus my discussion, first, on constructions of gender in the biomedical discourse on AIDS and, second, on the reverberations of this discourse in other writing about gender and AIDS.[9] Why AIDS? Because the discourse on AIDS—recent but already voluminous—reenacts many of the semantic battles that have characterized relations between women and biomedical science for at least the last century. AIDS takes us to the heart of feminist inquiry (indeed, of all the "human sciences"), including the question of how sex and sexuality are constructed; it also demonstrates how language can give the illusion of control. In the case of AIDS, however, the epidemic disease is so deeply complex at this point that control is out of the question.
In 1981 the official history of AIDS as a clinically defined entity began. Involving at first a small number of sexually active gay men, AIDS rapidly shifted to involve a larger and more heterogeneous male population, homosexual and nonhomosexual; by mid-1982, people with AIDS included intravenous users of heroin (and other drugs) who shared needles; Haitians; hemophiliacs; and others who had received injected blood or blood products. By early 1983 a small number of women were also diagnosed with AIDS, evidently infected via intravenous drug use or transfusions with contaminated blood, and by mid-1983 via male sexual partners with AIDS. Shortly thereafter heterosexual men with AIDS were identified whose sexual partner(s) had been infected females, demonstrating that women could both infect and be infected with HIV, human immunodeficiency virus. By 1984 there were reports from some central African countries (later fully documented) that almost as many women there had AIDS as men. A relationship between women and AIDS has thus existed for most of the known lifespan of the disease.[10]
This relationship, however, presents us with a series of mysteries. First, given the scientifically documented diagnoses of women with AIDS, why was AIDS simply assumed by the medical and scientific com-
munity to be transmitted only by gay men? Second, given the skepticism toward established science and medicine fostered for two decades by feminist activism and scholarship, why have relatively few feminists challenged biomedical accounts of AIDS or, with the exception of some lesbian writers and activists, called for solidarity with the gay male community? Finally, above all, given the intense concern with the human body that any conceptualization of AIDS entails, how can we account for the striking silence, until very recently, on the topic of women in AIDS discourse (including biomedical journals, mainstream news publications, public health literature, women's magazines, and the gay and feminist press)? As noted above, the real and imagined links between women's bodies and disease—especially infectious and sexually transmitted disease—are many and complex, and have a history reaching back many centuries. This is a subject, then, with heavy baggage—and the bags are already packed. Yet women have repeatedly been told that this time they would not be traveling, that they would not need the bags. If they were in the airport at all, it was for someone else's flight.
In the fall of 1986 all this changed: The Centers for Disease Control (CDC) in Atlanta reclassified a significant number of "unexplained" AIDS cases as having been heterosexually transmitted to and from women.[11] The National Academy of Sciences/National Institute of Medicine issued a blue-ribbon report warning the nation that AIDS was heterosexually transmissible both to and from women and men, making an urgent call for nationwide health education.[12] United States Surgeon General C. Everett Koop held a press conference to announce that he, too, now viewed AIDS as a potential threat to every sexually active person and to advocate the immediate institution of explicit sex education for everyone more than eight years of age.[13] The World Health Organization (WHO) confirmed what many had suspected: AIDS was devastating the populations of at least four African countries, where half of those with AIDS are women. AIDS has now been reported in more than 100 countries around the world and is now considered a pandemic health problem of catastrophic proportions.[14] In the United States, infection with HIV is estimated by some to be increasing among heterosexually active women and men (while rates of infection among sexually active gay men appear to have leveled off, though new AIDS cases and deaths remain high). "Suddenly," proclaimed the cover story of U .S . News and World Report in January 1987, "the disease of them is the disease of us "; and "us" is represented graphically in the magazine by a young, white, urban professional man and woman, a problematic repre-
sentation to which I shall return.[15] The main point here is that the population of people with AIDS now unquestionably includes women who appear to have become infected exclusively by way of sexual contact with infected men.
So, what a surprise to find ourselves in midair over the Atlantic without even a toothbrush packed—let alone a barrier contraceptive. The mystery is: Why were women so unprepared? And why do they continue to take it so quietly?
The construction in the United States of AIDS as essentially a male-only, sexually transmitted disease depends upon the production and reproduction of gendered readings whose reasonings are so outlandish and speculative as to be dizzying. In turn, this "knowledge" of AIDS infection and who can catch it filters out counterevidence in a variety of ways, creating a cycle of invisibility in which women do not believe themselves vulnerable and therefore do not seek medical care or even confidential testing. Despite this clinical history, moreover, women with AIDS have not been readily identifiable in the scientific literature. The pie-shaped charts typically depict the classic 4-H "risk groups"—homosexuals, heroin addicts, hemophiliacs, and Haitians—plus their sex partners, gender often unspecified—plus "Other."[16] To those familiar with feminist theory of the last two decades, the placing of women with AIDS under the literal rubric of "Other" possesses considerable irony and resonates with the ongoing construction of otherness in the history of venereal disease.[17] But, beyond irony, such otherness is dangerous because it creates a category of invisibility and it muddles information, both for those who have been or are at risk and for those who are responsible for identifying AIDS and its multiple manifestations. Thus, even after information about AIDS was widespread, many women did not believe they were at risk. Even today, women who finally seek care from health professionals may not be properly diagnosed, either because they are simply not seen to be at risk (whatever their symptoms) or because they do not display the symptoms (defined by the natural history of the disease in gay men) that officially denote the presence of AIDS and ARC (AIDS-related complex). Women's invisibility is created in other unexpected ways: One New York City writer, having heard in 1987 that "heterosexuals" were now considered at risk for AIDS, quizzed his white, middle-class female acquaintances and reported in the New York Times Magazine not a case of AIDS (or HIV infection) among them; as a nurse at Brookdale Hospital in Brooklyn acerbically pointed out in a subsequent letter to the editor, the writer would have
compiled quite different statistics had he explored the populations of poor people—primarily black and Hispanic, but also white—in the area surrounding her hospital.[18] Such examples of women's invisibility in the AIDS discourse reinforce the widespread perception of AIDS as an illness of sexually active gay men and of illegal-drug users; it is based, then, on scientific constructions that have glossed over the "Other" despite growing evidence that the category includes women (and men) who have been infected with AIDS by way of heterosexual intercourse of the boy-meets-girl/missionary position/no-frills variety.[19]
AIDS is debilitating, lethal, and in many respects still mysterious; some authorities regard it as the greatest health crisis of our era. The scientific label AIDS is normally construed to refer to a real clinical syndrome, an infectious condition caused by a virus and increasingly understood by the scientists and physicians who study it. But the relationship between language and reality is highly problematic, for scientists and physicians as well as for "the rest of us." Although we have come to accept the findings of biomedical science as accurate characterizations of material reality, scientific and medical discourses are always provisional, and only "true" or "real" in certain specific ways—in confirming prior research findings, for example, or in promoting effective clinical treatments. "AIDS" does not merely label an illness caused by a virus. In part, the name constructs the illness and helps us make sense of it. We cannot, therefore, look through discourse to determine what AIDS "really" is. Rather, we must explore the place where such determinations occur: in discourse itself, which is inevitably marked by our struggles to represent what we think AIDS really is and to conceptualize what it really means.
To talk of AIDS as a linguistic construction is not, of course, to claim that it exists only in the mind. Like other phenomena, AIDS is real, and utterly indifferent to what we say about it. Documented by news reports, medical records, photographs and journals, scientific research, conferences, and individual and collective experience, something is happening that real people are dying of. Whatever we call it, however we think about or represent it, we cannot wish AIDS away. Our names and representations can nevertheless influence our cultural relationship to the disease and, indeed, its present and future course. Accordingly, we struggle in many fragmentary and often contradictory ways to grasp the true nature of AIDS; yet, finally, this is neither directly nor fully knowable. It may be tempting, even irresistible, to understand the epidemic as a temporary problem involving incomplete scientific and medical
knowledge—certainly many familiar cultural narratives encourage this view—and to presume that we will eventually be provided a scientific account of AIDS closer to its reality. Moreover, to speak of AIDS as a linguistic construction that acquires meaning only in relation to networks of given signifying practices may seem to be both politically and pragmatically dubious, like philosophizing in the middle of a war zone. But as I have argued elsewhere, making sense of AIDS compels us to address questions of signification and representation.[20] When we deduce from the facts that AIDS is an infectious, sexually transmitted disease syndrome caused by a virus, what is it we are making sense of? "Infection," "sexually transmitted," "disease," and "virus" are also linguistic constructs that generate meaning and simultaneously facilitate and constrain our ability to think and talk about material phenomena. Language is not a substitute for reality; it is how we know it. And if we do not know that , all the facts in the world will not help us.
AIDS and its related conditions present us with an unprecedentedly complex set of social and scientific problems. If we are to address these problems with foresight, intelligence, and decency, it is crucial that we take into account the nature of language and acknowledge AIDS's enormous power to generate meanings we can never fully control. This chapter seeks to illuminate the relationship of AIDS to gender through an analysis of language, meaning, and discourse; I use analytic strategies from the sociology of science, cultural studies, and feminist theory to review the evolving constructions of gender in AIDS discourse and examine how women are situated within that discourse. The chapter is organized, roughly, around the chronology of the AIDS crisis: (1) evolving biomedical understandings of AIDS (1981-1985); (2) Rock Hudson's illness and death as a turning point in national consciousness (July 1985-December 1986); (3) AIDS perceived as a pandemic disease to which sexually active heterosexuals are vulnerable (fall 1986-spring 1987); (4) diversification of discourse about women and AIDS (spring 1987-present); and (5) implications for the future.
Broadly, I seek to explain the paradox sketched above: When history, culture, and language link women to disease in many ways, why, until very recently, were these links to AIDS erased or denied? And now, finally included in the AIDS discourse, will women contest the meanings and implications offered by the past, refuse the scripts from the theater of history? I suggest that an uncompromising feminist analysis can contest the fixed notions of scientific certainty and disrupt the familiar cultural narratives. Where AIDS is concerned, for example, the entrenched
division between "them" and "us"—men and women, guilty and innocent, gay men and "the rest of us"—is deeply problematic. Based on simplified, unitary identities and essentialist biological or social categories that serve only to reinscribe conceptual and ideological divisions, the "us"—"them" division represents a form of semantic imperialism we cannot afford in the present crisis.
Purporting to describe the natural world, this division at first gave women the false belief they were invulnerable. But as evidence of women's potential risk became clear, so did the theoretical schisms in accounts of AIDS. This revelation should have demonstrated how tenuous the current conceptualizations are; it should have fundamentally challenged the validity of any division of "the disease of them" from "the disease of us." Yet most discourse by and about women embraces this division, simply rearranging the contents of the categories to match the latest bulletins from Washington, Atlanta, or Paris, and advising "us" (women) to protect ourselves from "them" (men). It does nothing to unseat the notion that "them" (whoever they are) is an expendable category of people, while "us" is a category of people worth saving. Despite all we have learned about the social construction of sexual difference and how it has been used against women in the past, the categorization process is given little scrutiny in the case of AIDS. By questioning, therefore, what is often taken for granted in discussions of AIDS, I hope to illuminate its multiple dimensions, intricacies, and contradictions, and, in doing so, to contribute toward the development of policies that fully acknowledge the intractable complexity of this crisis.
The Evolving Body of the Gendered "AIDS Patient" in Biomedical Discourse
The existence of AIDS as an official clinical syndrome is generally dated from the report of the deaths of five gay men in Los Angeles from Pneumocystis pneumonia in the June 5, 1981, issue of the Morbidity and Mortality Weekly Report (MMWR ), published by the Centers for Disease Control in Atlanta. The paper, by Drs. Michael Gottlieb and Wayne Shandera of the University of California at Los Angeles (UCLA), had been routed in May by Dr. Mary Guinan to Dr. James W. Curran, head of the CDC's venereal disease division; he returned it to her with a note: "Hot stuff. Hot stuff."[21] Although Gottlieb had initially thought nothing of the fact that his first Pneumocystis patient was gay (he con-
sidered it equivalent to "the fact that the guy might drive a Ford"[22] ), he had decided by the time the paper was written that this was an outbreak of a new illness specific to gay men. The MMWR bulletin put it this way: "The occurrence of pneumocystosis in these 5 previously healthy individuals without a clinically apparent underlying immunodeficiency is unusual. The fact that these patients were all homosexuals suggests an association between some aspect of homosexual lifestyle or disease acquired through sexual contact and Pneumocystis pneumonia in this population."[23] The men who died from these first reported cases were not only gay, they had histories of multiple sexual contacts and of multiple sexually transmitted diseases (STDs). The published report confirmed the suspicions of physicians in other cities: Some of their gay patients were contracting and even dying from very strange diseases, including rare forms of pneumonia and cancer. What had been unofficially called "gay pneumonia" and "gay cancer" and WOGS (the Wrath of God Syndrome) now provisionally came to be called GRID: Gay-related immunodeficiency.
But in the months following the report in the MMWR and subsequently in other journals, these same rare diseases began to be diagnosed in people who were not gay—for example, in intravenous drug users, in hemophiliacs, and in people who had recently had blood transfusions. Despite widespread reluctance to acknowledge possible connections, there were enough nonhomosexual cases to render GRID an unsuitable diagnosis, and in 1982 the name "AIDS" was selected at a conference in Washington, D.C.[24] As it evolved during 1981 and 1982, the official CDC list of populations at risk for AIDS came to consist of the "4-H" group: homosexuals, hemophiliacs, heroin addicts, and Haitians; by 1983 the sexual partners of people within these groups had been added.[25] This list structured the collection of evidence for the next several years and contributed to the view that the major risk factor in acquiring AIDS was being a particular kind of person rather than doing particular things.
Outside the narrow, controlled, official account were disturbing exceptions: reports that in Africa women and men were afflicted with AIDS in equal numbers, observations of babies with AIDS-like symptoms, rumors of AIDS in men who had never used drugs nor had sexual contact with other men, reports of lesbians with AIDS.[26] In retrospect, it makes a tidy story to identify the tensions, ambivalences, and contradictions of this period as something simple: scientific conservatism, homophobia, denial, politicians' fears. Certainly there were instances of
predictable reflex behavior: the Wall Street Journal , like many other publications, published nothing about AIDS until "innocent victims" could be identified.[27] Some representatives of the far right were quick to seize on AIDS as new proof of the evils of a world gone soft on pleasure, communism, or both.[28] The discourse of this period and comprehensive accounts published since then demonstrate the complexity of social responses to a conglomeration of mysterious symptoms and fatal illnesses not yet well conceptualized. This is by no means to deny the profound discrimination that existed then and continues today (to which I shall return) but is rather to emphasize that at this stage many important questions were going unanswered. The conflict and contradictions among gay men, among members of the medical and scientific communities, among government officials, among reporters—all of whom by turns perceived AIDS as a gay disease and then denied that it could be, predicted a spread of AIDS to other groups and then rejected such a possibility—might also be understood as part of the process of making sense of problematic and frightening evidence.[29] It is important for the future that the past not be oversimplified. Although Randy Shilts's comprehensive book on the AIDS crisis, And the Band Played On , for example, demonstrates many points at which bias against and fear of homosexuals hampered public attention and fundraising, Dennis Altman notes that had AIDS first struck intravenous drug users and Haitians rather than the politically sophisticated and well-organized gay community, funding and publicity would undoubtedly have been even more meager and delayed.[30] Policy analyst Sandra Panem, reviewing charges that homophobia delayed federal research efforts, concluded that prejudice against homosexuality per se would not have deterred ambitious scientists from initiating interesting and rewarding research projects. But ignorance, she suggests, does appear to have played a role, citing as evidence a 1984 observation by James W. Curran, by then head of the CDC's AIDS task force, that among scientists there is little widespread research interest in sexuality of any kind and "not much understanding of homosexuality." Indeed, Curran went on to say that many eminent scientists during these early years rejected the possibility that AIDS was an infectious disease because they had no idea how one man could transmit an infectious virus to another; through what orifice could such a virus possibly enter a male body, lacking as it did the vaginal portal approved for the receipt of sperm?[31]
The subsequent scientific and medical obsession with the details of male homosexual practices was in part a compensatory by-product, I
believe, of this dramatic ignorance among many scientists at the outset. But only in part: For a number of scientists and physicians first involved in AIDS were either gay or familiar with the gay community. Many CDC staff members had worked closely with the gay community in the course of research on hepatitis B and had few illusions about sexual practices and sexual diversity, and were aware that not all gay men were active with multiple partners. Further, as the infected population grew, it became clear that gay men were everywhere—in politics, in Congress, on Wall Street, in Hollywood, in far-right organizations. In many cases, they were silent and invisible—unlike women and racial minorities. Part of the shock of AIDS was thus the shock of identity.[32]
Whatever else it may be, however, AIDS in the United States came to be a story of gay men and a construction of a hypothetical male homosexual body. Obsession, a repeated feature of the AIDS story, is also a feature of the fact that, in some ways, the gay man is what Mary Poovey calls a "border case." A "border case" threatens a heavily invested binary division in society (such as the nineteenth-century dichotomy of women by class and how it was threatened by prostitutes) that generates the need for discourse to restore stability. (The voluminous discourse on prostitution during this period, Poovey argues, was thus fundamentally about class.)[33] The ongoing fixation with HIV testing is in part designed to put a stop to gay men's successful passing as straight; refusal to take the HIV-antibody test is therefore similar to pleading the Fifth.[34]
A number of hypotheses and speculations were put forward during this period about the nature of the AIDS epidemic: its dimensions, causes, newness, its theoretical, scientific, and political implications, and its consequences.[35] Despite lack of understanding, scientific and journalistic gatekeeping was evident from virtually the beginning—with one effect being the disinclination of editors and journals to suggest that AIDS was caused by an infectious agent.[36] When the first cases appeared in New York, Los Angeles, and Paris, the early hypotheses tended to be sociological, relating the disease directly to some feature of a supposed "gay male life-style." For example, in February 1982 it was hypothesized that a particular supply of amyl nitrate (or "poppers") might be contaminated. But "the poppers fable," writes French scientist Jacques Leibowitch, became "a Grimm fairy tale when the first cases of AIDS-without-poppers [were] discovered among homosexuals absolutely repelled by the smell of the product and among heterosexuals unfamiliar with even the words amyl nitrate or poppers ."[37] Another view was that sperm itself could destroy the immune system. "God's plan for
1. Steve Bell's satiric cartoon in the Guardian (16 October 1984, p. 29) links
"supply side" Reaganomics with its sexual analogue—a position embodied
nonsatirically in the deliberations of the Meese Commission for the Study of
Pornography (1984-1985). Courtesy of Steve Bell.
man," after all, said conservative Congressman William E. Dannemeyer (R. Calif.), "was for Adam and Eve and not Adam and Steve."[38] A cartoon in 1984 by Steve Bell in the London and Manchester Guardian satirized this position by showing Ronald Reagan declaiming from a podium in similar terms (fig. 1).[39] Women, this story goes, are the "natural" receptacles for male sperm. Their immune systems have evolved over the millennia to deal with these foreign invaders; men, not thus blessed by nature, become vulnerable to the "killer sperm" of other men. AIDS in the lay press became known as the "toxic-cock syndrome."[40] Note the contrast this latter view poses to the earlier one among some scientists that infection could be transmitted only from a penis to an "approved receptacle" (i.e., a vagina); now the "natural" receptacle is somehow seen as magically resistant to infection, while the orifices of the "guys with skirts" and the "AC /DC weirdos" become the preferred targets of killer sperm. (I discuss lesbians, the "gals in pants," below.)
Although scientists and physicians tended initially to define AIDS as a problem tied to gay culture, gay men on the whole also rejected the possibility that AIDS was a new, contagious disease. Not only could this make them sexual lepers, it didn't make sense: "How can a disease pick out gays?" they asked; it had to be "medical homophobia."[41] In the gay community, the first reaction to AIDS was disbelief. A gay physician in San Francisco told Frances FitzGerald: "A disease which killed only gay white men? It seemed unbelievable. . . . I used to teach epidemiology, and I had never heard of a disease that selective. I thought, they are
making this up. It can't be true. Or if there is such a disease, it must be the work of some government agency—the FBI or the CIA trying to kill us all."[42] In the San Francisco A .I .D .S . Show , one man is said to have learned of his diagnosis and then wired the CIA: "I HAVE AIDS. DO YOU HAVE AN ANTIDOTE?"[43]
Another explanation proposed in the early 1980s and still regarded as potentially significant is the notion that AIDS is a "multifactorial" condition. According to this view, no single infectious agent or other factor acts alone to cause the problem. Rather, a factor acts in conjunction with others. So-called cofactors range from the biological (e.g., various pathogens, including viruses) and biomedical (clinical history) to the social (poverty, diet), environmental (mosquitoes), psychological (guilt, stress), and spiritual (sin).[44] One hypothesis was that a person who is sexually active with multiple partners is exposed to a kind of bacterial/viral tidal wave that eventually crushes the immune system. Gay men on the sexual "fast track" would thus be particularly susceptible because of specific practices that maximize exposure to multiple pathogens.[45] Finally, a range of other possibilities has been proposed, from biological experimentation run amok to global conspiracy theories.[46] Yet the choice should not be seen as one between a single-agent theory and all other possibilities. With the growing complexity of the clinical and epidemiological picture (including the unpredictable relationship between exposure and infection, between infection and the development of clinical symptoms, and between the appearance of clinical symptoms and "AIDS") it seems, rather, that we should abandon the hope for finding a simple "cause of AIDS" and instead concentrate on making sense of what is already before us.[47]
Many were reluctant to move away from the view of AIDS as a "gay disease." For some, the name GRID would always shape their perceptions.[48] Yet what marked off the first years of AIDS from those that followed was the growing intensity of the search for an infectious agent—probably a virus—that could plausibly be implicated in the development of AIDS. Laboratories at the Pasteur Institut in Paris and at the National Cancer Institutes in the United States isolated a strain of virus that appeared to be associated with AIDS and AIDS-like conditions. I will not detail here the virus's story[49] but will say only that by the end of 1984 there was general consensus among many U.S. scientists that a virus was the major "cause" of AIDS.[50] "A virus," according to a story in National Geographic , "is a protein-covered bundle of genes containing instructions for making identical copies of itself. Pure information.
Because it lacks the basic machinery for reproduction, a virus is not, strictly speaking, even alive."[51] The virus is thus another "border case" that becomes the site—discursive and literal—for ongoing dispute.
Virologists and immunologists clearly considered the AIDS virus as extraordinarily interesting—a retrovirus , actually, that replicates "backwards," transferring genetic information from viral RNA (which becomes a template for transcription) into DNA. In turn, the DNA enters the cell's own chromosomes and, thus positioned within its infected host, may begin producing new viruses immediately or remain latent for years.[52] In the case of "the AIDS virus," now named "HIV" for human immunodeficiency virus, this dormancy can last up to (at present count) fourteen years, followed by a sudden explosion of replication that may kill the host cells (normally the helper T-cell—the conductor, it has been said, of the orchestra that is the immune system), leaving the host vulnerable to outside infections that a normal immune system would repel.[53]
The discovery of the virus by Dr. Robert C. Gallo and his research team was announced with great fanfare, and the promise of quick therapeutic measures was quickly issued by Margaret Heckler, then secretary of health and human services, who also said AIDS must and would be stopped before it spread to the "general population." For this she earned the title in the gay community of secretary of health and heterosexual services; the Reagan administration, for whatever reason, used the public outcry following the press conference as a rationale for reassigning Heckler to the post of ambassador to Ireland.[54] The incidence of AIDS in the gay community also increased, though more was becoming known about transmission, protection, and treatment. But the identification of the virus validated the authority of the Western biomedical research establishment and, as Donna Haraway suggests, enabled AIDS to be transformed from a low-status STD to the realm of High Science and High Theory. At the same time, the body was transformed from a mere combat zone to a communication, control & command center.[55] A virus, after all, is "pure information," and the body is simply the terrain on which it is transcribed.
The identification of the virus also, to some extent, put to rest so-called "spread of AIDS" stories.[56] Although the term virus did suggest possibilities of infection and contagion, the discovery nevertheless quickly acquired the status of a "fact" in scientific understandings of the illness and therefore fulfilled the functions of a "fact" as defined by Ludvik Fleck: "In the field of cognition, the signal of resistance opposing free,
arbitrary thinking is called a fact ."[57] So despite the appropriation of the virus as evidence to support many existing theories (e.g., the view that the CIA or KGB had caused AIDS), together with extant knowledge about viruses (e.g., that they cause colds, herpes, and polio), the overall effect was to concentrate speculation on modes of transmission and mechanisms of infection and destruction. Although sources of media coverage have increased and diversified since this period, particularly since late 1986, modes of representation (as suggested, for example, in a recent study of AIDS metaphors by Hughey, Norton, and Sullivan) have shifted as widespread uncertainty gave way to a better understood, if still greatly feared, illness.[58] In some cases, attempts to achieve certainty and to reduce public panic appeared to oversimplify the problem and to extend false reassurances. Other voices remained cautionary and careful, however, in assessing the data.[59]
As Jean L. Marx summarized the evidence in Science , "sexual intercourse both of the heterosexual and homosexual varieties is a major pathway of transmission."[60] Other articulate voices joined in warning about the public health consequences of treating AIDS as a "gay disease," and separating "those at risk" from the so-called general population.[61] Gary MacDonald, executive director of an AIDS organization in Washington, D.C., put it this way in 1985: "The moment may have arrived to desexualize this disease. AIDS is not a 'gay disease,' despite its epidemiology. Yet we homosexualize it, and by doing so end up posing the wrong questions. . . . AIDS is not transmitted because of who you are , but because of what you do ." MacDonald went on to note that almost a fifth of AIDS patients in the United States are intravenous drug users and another 6 percent never fit any of the high-risk groups. "By concentrating on gay and bisexual men, people are able to ignore the fact that this disease has been present in what has charmingly come to be called 'the general population' from the beginning . It was not spread from one of the other groups. It was there ."[62] As Ruth Bleier reminds us, questions shape answers. Thus, the question, "Why are all AIDS victims sexually active homosexual males?"—which has so dominated research—might more appropriately have been: "Are all AIDS victims sexually active homosexual males?"[63] But in quashing speculation and "hysteria" in the name of reason, expressions of scientific certainty also closed off considerations that women, nongay men, faithfully married couples, and so on could get AIDS. Statistical probabilities about what would happen were allowed to be read as theoretical constraints on what could happen.
Rock Hudson and the Crisis in Gender
Ironically, a major turning point in America's consciousness came in the summer of 1985 when Rock Hudson acknowledged he was being treated for AIDS.[64] Through an extraordinary conflation of texts, Rock Hudson's illness dramatized the possibility that the disease could spread to the "general population." "I thought AIDS was a gay disease," said a man interviewed by USA Today , "but if Rock Hudson can get it, anyone can." Hudson was, I would argue, another "border case" (in Poovey's sense) in which such textual conflations became common: When an event contradicts the perceived natural order of things, it becomes a cultural dispute that generates vast quantities of discourse designed to shore up existing distinctions and resolve contradictions.[65]
Another site of continuous dispute is the mechanism through which the virus is transmitted, as well as the different explanations for the epidemiological finding that AIDS and HIV infection in the United States were appearing predominantly in gay men. One view holds that the prevalence among the latter is essentially an artifact ("simple mathematics") because the virus, for whatever reason, infected gay men first and gay men tend to have sex with each other. The second is that biomedical/physiological factors make sexually active gay men and/or the "passive receiver" more infectable. A third view is that the virus can be transmitted to anyone, but that certain cofactors predispose the development of infection and/or clinical symptoms in particular individuals.[66] There are also speculations about the quantity of virus that is needed to cause infection (virus is both a count and a mass noun). Dr. Mathilde Krim, then of the AIDS Medical Foundation, for example, suggested that because the virus "must be virtually injected into the bloodstream" male-to-female transmission is more likely.[67] Jonathan Lieberson, likewise, concluded in 1986 that infection requires "direct transfusion into the bloodstream."[68] Dr. Jacques Leibowitch, however, relates transmission patterns, on the one hand, to the fact that homosexual men have sex with other homosexual men and, on the other hand, to the male homosexual "duality." A man, that is, can be a "receiver" of the virus from one man and then be a "donor" of the virus to another, in contrast to the "relative intransitivity of heterosexual propagation." By virtue of their "natural anatomy," women receive but do not give.[69] Indeed, many scientists have come to hold the view that, as Nathan Fain put it, "infection requires a jolt injected into the bloodstream, likely sev-
eral jolts over time, such as would occur with infected needles or semen. In both cases, needle and penis are the instruments of contagion."[70]
All this generated considerable confusion as to who was likely, even capable, of becoming infected and just what it was that increased or decreased that likelihood. Much of the uncertainty in the science and medical journals obviously turned (as, indeed, it still does) on the precise mechanisms of transmission. Nevertheless, even in the journal literature, and certainly as presented to the general public, questions about transmission were interpreted in part as questions—anxious questions—about sexual difference (male/female; heterosexual/homosexual; active/passive).
To the rescue came John Langone in the December 1985 issue of Discover magazine. In this lengthy review of research to date, Langone suggests that the virus enters the bloodstream by way of the "vulnerable anus" and the "fragile urethra." The "rugged vagina" (built to be abused by such blunt instruments as penises and small babies), in contrast, provides too tough a barrier for the AIDS virus to penetrate.[71] "Contrary to what you've heard," Langone concludes—echoing a fair amount of medical and scientific writing at the time—"AIDS isn't a threat to the vast majority of heterosexuals . . . . It is now—and is likely to remain—largely the fatal price one can pay for anal intercourse."[72] (This excerpt from the article also ran as the cover blurb.) Detailed cross-sectional drawings of anus, urethra, and vagina illustrated the article's conclusion.
The Discover article reassured many people about the continuing validity of the CDC's original 4-H list of high-risk categories. But categories of risk, of behavioral practice, and of identity may be quite distinct, or may overlap with each other—an ongoing problem in AIDS epidemiology and research. Sociologist Jeffrey Weeks, for example, analyzes the evolution of homosexuality as a coherent identity. "The gay identity," he writes, "is no more a product of nature than any other sexual identity. It has developed through a complex history of definition and self-definition," and "there is no necessary connection between sexual practices and sexual identity."[73] The problems with the CDC list were known to some science reporters, at least to the few who were knowledgeable and tenacious enough to take their analysis beyond the official party line. Ann Giudici Fettner, for example, pointed out in 1985 that "the CDC admits that at least 10 percent of AIDS sufferers are gay and use IV drugs. Yet they are automatically counted in the homosexual and bisexual men category, regardless of what might be known—or not known—about how they became infected."[74] So the "gay" nature of
AIDS was in part an artifact of the way data were collected and reported, though it was generally hypothesized until 1986 that the cases assigned to the category OTHER (or UNKNOWN, or UNCLASSIFIED) would ultimately turn out to be one of the four Hs. As Shaw and Paleo point out, however, the number of women in this category remains much larger than men; they point out, among other things, that the category "homosexual" was not broken down by sex despite potential risk for lesbians via sexual activity and artificial insemination.[75] Data from Africa were showing that women and men were infected in equal numbers; yet the practice of medicine and resources for data collection in Africa, especially outside urban areas, made the data questionable on a variety of grounds.[76] And even as evidence accumulated that transmission could be heterosexual (which begins with the letter H, after all), scientific and popular discourse continued to construct women as "inefficient" and "incompetent" transmitters of HIV, stolid barriers that impede the passage of the virus from brother to brother.[77]
In the discourse of this period (from approximately mid-1985 to December 1986), there were exceptions, which will probably not surprise us. As evidence of AIDS in women mounted, speculation linked the disease to prostitutes, intravenous drug users, and women in the Third World (primarily Haiti and countries in central Africa). It was not that these three groups were synonymous but, rather, that their differentness of race, class, or national origin made speculation about transmission possible—unlike middle-class American feminists, for example. American feminists also by this point had considerable access to public forums from which to protest ways in which they were represented, while these other groups of women were, for all practical purposes, silenced categories so far as public or biomedical discourse was concerned (fig. 2).[78]
Prostitutes—despite their long-standing professional knowledge of STDs and continued activism about AIDS—have long been portrayed as so contaminated that their bodies are, like "bloody Maggie's" in the passage at the beginning of this chapter, "always dripping," virtual laboratory cultures for viral replication.[79] Early failures to find AIDS cases among prostitutes, however, supported the "gay disease" hypothesis.[80] "Women in general," concluded a Johns Hopkins professor of medicine, "seem to be less efficient transmitters of the disease."[81] Immunologist Paula Strickland concurred: "I think AIDS would be containable and would pose no threat to heterosexuals if there weren't any bisexuals in our society."[82]
Commitment to this view of AIDS as a male disease was so strong
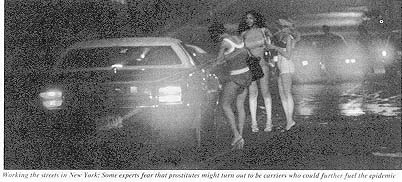
2. Against a dark, ominous background, prostitutes are shown "working the
streets in New York." Despite many qualifiers in the caption and lack of
scientific evidence, Newsweek 's use of this photograph (12 August 1985,
p. 28) lent credibility to the familiar belief that prostitutes would inevitably
figure largely in the spread of AIDS. Courtesy of Ethan Hoffmann Archive.
that when R. R. Redfield and his colleagues reported a study in the Journal of the American Medical Association demonstrating infection in U.S. servicemen who claimed heterosexual contact only—with female prostitutes in Germany—various attempts were made to discredit or dismiss this new evidence:[83] Servicemen, for instance, would be punished for revealing homosexual behavior or intravenous drug use; they really had gone to male prostitutes, and so on.[84] If women were merely passive vessels without the efficient capacities of a projectile penis or syringe for "efficiently" shooting large quantities of the virus into another organism, the transmission to U.S. servicemen from German prostitutes must be only apparent. Indeed, one reader suggested, transmission was not really from women to men but was rather "quasihomosexual": Man A, infected with HIV, had sexual intercourse with a prostitute; she, "[performing] no more than perfunctory external cleansing between customers," then has intercourse with Man B; he is infected with the virus by way of Man A's semen still in the vagina of the prostitute.[85] It was taken for granted that the prostitute took no preventive or cleansing measures, and, one must suppose, that the projectile penis could also function as a kind of proboscis, sucking up quantities of virus from a contaminated pool. A similar metaphor, and one we shall meet again, occurs in a study of urban prostitutes in central Africa; the prostitutes are called "major reservoir of AIDS virus," African heterosexual males are "vectors of infection."[86]
Evidence suggests, however, that prostitutes are not at greater risk because they have multiple sex partners, but because they are likely to use intravenous drugs.[87] Shaw and Paleo, for example, write:
There is no evidence that prostitutes constitute a special risk category. . . . Some prostitutes do get AIDS. To the extent that researchers have been able to isolate prostitution and/or multiple sexual contacts from such issues as IV drug use, however, neither the number of sexual contacts nor the receipt of money . . . seems to put women at a higher risk for getting AIDS. Many women who are in paid sexual activity were concerned about sexually transmitted diseases even before the AIDS epidemic. They protected themselves and continue to protect themselves by being somewhat alert to new medical developments in sexually transmitted diseases and how to avoid them.[88]
COYOTE and other organizations of prostitutes have addressed the issue of AIDS rather aggressively for several years.[89] Some scientists have also attempted to counter the prevailing view that AIDS is predominantly and inherently a gay disease. Virologist William Haseltine, for example, dismisses exotic explanations of the African data: "To think that we're so different from people in the Congo is a more comfortable position, but it probably isn't so."[90] Haseltine successfully used this argument to obtain increased AIDS funding, citing Redfield's data on the U.S. servicemen in Germany at a congressional hearing: "These aren't homosexuals. These aren't drug abusers. These are normal, young guys who visited prostitutes. Half the prostitutes are infected, and these guys got infected."[91] Interestingly, he explicitly separates "normal, young guys" from gays and drug users, shifting in the last clause to the passive voice, a construction that reinforces their lack of culpability, representing them as innocent "receivers" of the infection, not problematic "donors." The "young guys" are the infectees, the prostitutes the infectors (compare this with the syntax of Shaw and Paleo, above, where prostitutes protect themselves and remain alert to medical news).[92]
A second exception were infected female intravenous drug users, or, as they are commonly called, "drug abusers" or "drug addicts" (though it is during use , not necessarily abuse , that transmission occurs).[93] Scientific and popular accounts have tended to show little interest in or sympathy for this group: It should be noted, however, that statistics are problematic in part because these individuals are hard to reach, and in part because drug use is compounded by other conditions. For example, HIV infection in prostitutes is often attributed to sexual contact with multiple partners (and especially to paying multiple partners), although, as I have noted, the sharing of needles in the course of intravenous drug
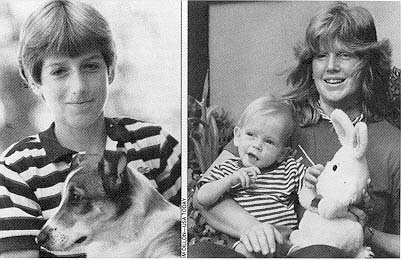
3. Live or stuffed animals in photos of persons with AIDS distinguish the "innocent"
from the "guilty," or at least normalize their "otherness." After Rock Hudson's death,
many publications ran sympathetic stories accompanied by photos of him playing with
his dogs: He had AIDS, ran the subtext, but he was still a good person. In early stories
on AIDS, researchers like the CDC's Jim Curran were often photographed with their
spouses and children: He may study AIDS, but he's as heterosexual as the next guy.
Photograph of Ryan White by Max Winter for Picture Group; photograph of Matthew
Kozup and his mother by Tim Dillon for USA Today . Both ran in Newsweek , 12 August
1985, p. 29.
use is the more likely source of exposure. Of the women with AIDS in New York City, for example, 62 percent are intravenous drug users and most of the others are sex partners of drug users; of the 183 cases of heterosexually transmitted AIDS, 88 percent were identified as sex partners of intravenous users, and fewer than 9 percent as the sex partners of bisexual males. Of the female HIV-positive prostitutes, almost all were intravenous drug users. Of the 156 children with AIDS as of December 1986, 80 percent had one or both parents who were intravenous drug users; the number of infected babies born at risk will rise each year.[94] In San Francisco, where a different epidemiological picture exists, transfusion-related AIDS is the most common source of infection for women; drug use and heterosexual contact come second.[95] Sex partners of "drug addicts," who, like transfusion cases, are often infected without their knowledge (even knowledge that their partner may be at risk for AIDS), are sympathetic "victims"—up to the point that they become
pregnant, when they become baby killers. Mothers with transfusion-caused AIDS remain sympathetic figures (fig. 3). But the CDC's James W. Curran in June 1986 pointed the finger directly at the "invidious transmission" made possible when female drug users and drug users' sex partners allow themselves to get pregnant.[96] With this act the passive receiver again becomes a culpable agent who transmits her infected blood "vertically" to her unborn child or (perhaps) after birth through breast milk. But as Shaw notes, little information is available about this phenomenon or about the effects of pregnancy on the woman herself; pregnant women may be both more likely to get infected if they are sexually active or, if already infected, pregnancy might activate the dormant virus.[97]
A third exception were women from central Africa and other areas of the world (primarily Haiti), where heterosexual transmission is more common. Again, no conceptually coherent explanation was offered for why a sexually transmitted illness should be homosexual in one country and heterosexual in another, although ad hoc speculations supported by virtually no documentation attribute the African statistics to "quasihomosexual" transmission of the kind noted above, refusal by African men to admit to homosexuality or drug use, the practice of anal intercourse as a method of birth control, or the widespread use of unsterilized needles in clinics and hospitals.[98] A debate in the letters column of the New York Times over the role of genital mutilation regarding AIDS in Africa illuminates the phantasmic projections of exotica that AIDS has stimulated. Fran P. Hosken suggested in December 1986 that widespread female "circumcision" (clitoridectomy and infibulation) is the main reason why the disease pattern is different in Africa (a 1: 1 ratio of women to men).[99] Douglas A. Feldman, acting executive director of the Queens AIDS Center, responded as follows: "Certainly, female genital mutilation is a brutal, sexist practice that should be strongly discouraged" but , he argued, the epidemiological pattern does not conform to the hypothesis of a relationship. In the countries where AIDS is widespread—Burundi, the Congo, Rwanda, Tanzania, Uganda, Zaire, and Zambia—clitoridectomies are rare. Where the procedure is common—from Senegal in the west to Somalia in the east—AIDS is generally not found. "However, as AIDS spreads into Kenya and eastern Tanzania, where the removal of the clitoris and labia majora is common, often resulting in genitourinary infections, it is likely that the practice may facilitate the spread of the disease." But after this potentially sensible comment—sensible because a history of infection is known to be rele-
vant to immune-system deficiencies—Feldman embarks on his own speculations, suggesting that the following factors may cause higher AIDS rates in African women: (1) higher rates of prior immunosuppression (but in relation to what? the infections he has just mentioned? poverty, malnutrition?); (2) intestinal parasite infestation; (3) greater likelihood of urban African women to engage in sex during menstruation (greater than rural women, or than American women? and is it yet established that this is relevant?); (4) "possibly the common practice by prepubescent girls in parts of central Africa of elongating the labia majora through continual stretching" (does this make it thin and "fragile" like the anal tract?); and (5) possible existence of an "immunosuppressive viral co-factor" (deuces wild). "But I fear," writes the doctor, "it is just a matter of time before the pattern of heterosexually transmitted AIDS in the singles bars along First Avenue, as well as the sidewalks of Queens Boulevard, will begin to look a lot like the pandemic in Africa today."[100]
This was December 1986, and suddenly the big news—cover stories for the major U.S. news magazines—was the grave danger of AIDS to heterosexuals. Major stories on AIDS as a threat to "all of us" appeared, for example, in Newsweek , U .S . News and World Report , Time , Scientific American , The Atlantic , and the Village Voice .[101] In a four-part series beginning March 19, 1987, the New York Times gave front-page coverage to several dimensions of AIDS; significantly, the boilerplate explanatory paragraph in each story made no mention of gay men or intravenous drug users. Although these groups were mentioned in the stories themselves, they were no longer considered intrinsic to the definition of AIDS.[102] No dramatic discoveries in the intervening year had changed the fundamental scientific conception of AIDS. What had changed was not "the facts" but the way they were now used to construct the AIDS text and the meanings we were now allowed—indeed, at last encouraged—to read from that text.
By the fall of 1986 virtually all theories of AIDS, no matter how remarkable their semantic underpinnings, had to confront the same bottom line: AIDS can be transmitted through heterosexual intercourse and other sexual activities to and from both women and men. It is important to emphasize that the gay community and (especially in New York City) the black and Hispanic communities continue to be most devastated by AIDS and most urgently in need of help. This does not mitigate the need to stress the possibility of widespread heterosexual transmission, and the current obsession with precise statistics—with
whether or not HIV infection is about to "explode" in the "general population," or with whether the entire epidemic itself is over—is, in my view, a dangerous diversion from questions of far greater importance.[103] My own concern continues to be with the evolution of "the facts," how these facts are constructed and represented, and, finally, how it has happened that the politically sophisticated feminist community has remained oblivious so long not simply to the potential risk to women but to AIDS as a massive social crisis.
AIDS Goes Heterosexual
Scientists commonly point out that AIDS arrived at the "right time"—that is, a time when basic science research in virology and immunology could provide a foundation for an intensive research effort on AIDS. They point out that no other epidemic disease has been analyzed so quickly nor its cause so efficiently determined."[104] Despite quarrels with this view (Randy Shilts, for example, calculates that the entire workforce assigned to AIDS was a tiny fraction of the one deployed to deal with the 1982 Tylenol scare in Illinois[105] ), let us concede that a number of biomedical researchers, epidemiologists, and clinicians have greatly contributed to our understanding of AIDS and that they were able to do so in part because of scientific progress in specific fields over the last twenty years. As Simon Watney points out, however, investigations of the last two decades provide a crucial foundation for the analysis of AIDS in the human sciences as well. Such a foundation prepares us to analyze AIDS in relation to questions of language, representation, the mobilization of cultural narratives, ideology, social and intellectual differences and hierarchies, binary divisions, interpretation, and contests for meaning.[106]
Models for such analyses in relation to AIDS have primarily been carried out by members of the gay community, whose interventions have helped shape the discourse on AIDS. As gay activists contested the terminology, meanings, and interpretations produced by scientific inquiry, loaded phrases like "promiscuous" soon gave way to more neutral behavioral descriptions like "sexually active with multiple partners" (many examples of such shifts are demonstrated in the collections of AIDS papers from Science and the Journal of the American Medical Association ). It is interesting that by 1986, when women were more central to the AIDS story, scientists and physicians were speaking of "sexually active" males and "promiscuous females."[107] Other linguistic
practices relevant to the construction of gender and sexuality in AIDS discourse are enumerated by J. Z. Grover.[108] Although such linguistic activism is dismissed by Shilts as misguided public relations efforts on the part of the gay community, it is more accurately seen, as Watney and others have argued, as part of a broad and crucially important resistance to the semantic imperialism of experts and professionals.[109] Challenging the authority of science and medicine—whose meanings are part of powerful and deeply entrenched social and historical codes—remains a significant and courageous action. It also provides an important model for women as evidence accumulates that neither gender nor sexual preference provides magical protection from the virus.
In 1985 and again in 1986 the CDC reviewed the patients who "could not be classified by recognized risk factors for AIDS." Eve K. Nichols, analyzing the CDC review of "unexplained cases" and related research, concludes that "these facts suggest a possible association between a small number of AIDS cases and heterosexual promiscuity in this country."[110] Despite the hedging and the use of the loaded term promiscuity , the conclusion represents a new biomedical construction of AIDS within the official scientific establishment. In December 1986 the CDC officially reclassified 571 cases formerly classified as "none of the above."[111]
What are biomedical scientists now saying about women? In April 1987 another article on women and AIDS appeared, this in the Journal of the American Medical Association .[112] Coauthors Mary Guinan, M.D., and Ann Hardy, Ph.D., M.P.H., review the 1,819 cases of AIDS in women officially reported in the United States between 1981 and 1986. Within the risk group of heterosexual contacts of persons at risk, the percentage of women increased from 12 percent to 26 percent between 1982 and 1986 (heterosexual contact is the only transmission category in which women at present outnumber men). More than 70 percent of women with AIDS are black or Hispanic; more than 80 percent are of childbearing age. As to the "portal of entry" for the virus, it is unclear what is going on and will probably continue to be unclear until we know the precise mechanism(s) of transmission. The distinction between anal versus vaginal "portals," according to Guinan and Hardy, is relevant only if HIV cannot pass through mucous membranes and thus requires broken skin or membranes. But this is still unknown, and "if the virus can pass through intact mucous membranes, the risk of transmission through the vagina or rectum may not be different."[113]
Though its cautionary and provisional stance is welcome, this article is problematic in several ways: First, the women in risk groups are given their "status" only by virtue of their sexual partners—the men they're connected to—not by virtue of their own sexual activities. This kind of assignment appears to constitute a return to an earlier system of sociological categorization, one perhaps not fully theorized in the current situation. Second, the source of infection is determined according to a hierarchy of factors, with sexual contact taking precedence over intravenous drug use and with no dual assignments occurring; in CDC studies, therefore, infection in prostitutes has typically been assigned to contact with multiple sex partners, even though other studies, as well as prostitutes themselves, assign the source of infection to intravenous drug use.[114] And finally, above all, the purpose of studying women, we are told, is twofold: first, to use incidence in women as a general index to heterosexual spread of the virus, and second, to identify women at risk and prevent "primary" infection in them in order to prevent the majority of cases of AIDS in children that would result from these maternal risk groups without intervention.[115] There is thus no intrinsic concern for women as women . Yet, because pregnancy suppresses the immune system, any woman who gets pregnant increases her risk of infection with HIV or, if already infected, possibly increases her risk of developing active AIDS.
It is true that we need to be concerned about "future generations." During the Venetian plague of 1630-1631, ten thousand pregnant women were killed in a period of months, decimating the city's childbearing population.[116] As Shaw and Paleo point out, because the widespread practice of safer sex would drastically reduce the birth rate, childbearing might come under intense scrutiny by the state, and women of childbearing age might be among the first groups to undergo mandatory testing.[117] But surely we are also concerned about women themselves and need to give thought, in policies and practice, to them rather than simply treating them as transparent carriers who house either the future of humanity or small Damiens who will assist in furthering viral replication.
In other biomedical discourse, as I have noted, some scientists and physicians (including William Haseltine, Mathilde Krim, Jean L. Marx, and Constance Wofsy) have for some time noted that HIV may be heterosexually transmitted to and from women; and suggest that despite the small number of cases, woman-to-woman transmission may
also be possible.[118] Because of the still-unanswered questions, these professionals emphasize caution until more is known. What about lesbians, who still figure only fitfully in the biomedical story? Lesbians appear in the abstract to be at relatively low risk for HIV infection—lesbians as a group have a very low incidence of sexually transmitted disease, although the medical literature does include isolated reports, often in letters to the editor, of HIV transmission by way of female-to-female sexual contact.[119] Despite these virtually nonexistent statistics, lesbians were lumped by the public with gay men and considered just as dangerous; although lesbians in many cities are now organizing blood drives, for example, earlier attempts to do so had been defeated by the public perception that lesbians were as likely to be infected as gay men because "AIDS is a gay disease."[120] Ironically, despite many lesbians' long-standing support for and solidarity with gay men on the AIDS question, and despite the time lesbians contribute to AIDS hotlines and task forces, very little "safer sex" literature, whether directed toward homosexuals or heterosexuals is designed specifically for women whose sexual contacts are with other women.
Concerns about women in the general press have also come relatively late in the AIDS crisis. An important exception is Cindy Patton's 1985 Sex and Germs , a social and political analysis of AIDS that addresses the growing connections among contamination phobia, erotophobia, and homophobia, and proposes an agenda for progressive action.[121] Also useful is the work of Ann Guidici Fettner, Katie Leishman, Marcia Pally, Nancy Stoller Shaw, and J. Z. Grover.[122] Important and informed questions about the politics of AIDS and the "risk group" mode of describing vulnerability to HIV have consistently been asked by, among others, Randy Shilts, Peg Byron, Wayne Barrett, Simon Watney, C. Carr, Larry Kramer, and Nancy Krieger.[123] These writers have been notable. Politically oriented prostitutes' organizations have also been vocal in addressing issues of AIDS as they relate to women—advocating not only individual prevention strategies but also government responsibility for assuring safe conditions in a service industry.[124] Though the subject of women and AIDS was regularly covered only by a few women writers—primarily in radical journals in New York, San Francisco, and London—by 1986 most women's magazines had run at least one "What Women Should Do" or "What Women Need to Know" article (e.g., Vogue , New Woman ), and by 1987 mainstream feminist journals and magazines including Ms . in the United States and Spare Rib in Great Britain were providing fairly regular coverage.[125] Still, as Marea Murray
had argued in a 1985 letter to Sojourner , some women, including lesbians, continued to perceive AIDS as a problem "the boys" had brought on themselves,[126] while heterosexual women were still tending to see AIDS as nothing to do with them or as something that "self-help" procedures would guard them against. Of course, in the absence of challenge or resistance, female roles in the AIDS story remained the traditional ones: loving mother, loyal spouse, wronged lover, philanthropic celebrity; one man with AIDS even attributed his apparent remission to "the Blessed Virgin" (figs. 4 and 5).[127] But even here a confusion was evident as to who was guilty, who innocent, who was an active agent of disease, who a victim.[128]
Why was there such resistance to acknowledging women's potential to acquire and transmit AIDS and to deal clinically with AIDS as a woman's illness? One reason is certainly denial: the sheer unthinkability of AIDS unleashed upon the entire world population because, then, as someone put it at the Paris International AIDS Conference in July 1986, "the sky's the limit." Semantic imperialism breaks down in the face of the virus's ability to replicate infinitely. Instead, there is hope that the virus will be able to be "contained" within the populations already infected—i.e., "saturating" the established high-risk groups but not spreading beyond them. Though millions would die, this is still a containable subtotal of the "general population."[129]
A second reason for resistance to the role women play in the transmission of AIDS involves the potential difficulty of feminizing AIDS at this stage, after so long an identification with gay men. Shilts notes resistance to initial reports of infants and children with AIDS because the name GRID "by definition" signified a "gay disease." Yet Shilts himself, whose own account of AIDS begins with the mysterious illness in central Africa of a Danish lesbian physician, nevertheless focuses more intensely on a sexually appetitive Canadian airline attendant, a gay man who came to be identified by the CDC as "Patient Zero." Of course, as soon as the advance publicity on Shilts's book went out, the New York Post 's headline blared: "THE MAN WHO GAVE US AIDS!"[130] Others have pointed out that there is no need for female representation in the AIDS saga because gay men are already substituting for them as the Contaminated Other. Conservative journals like Commentary preserve this place by putting forth clearly and repeatedly the thesis so boldly stated by Langone: "AIDS remains the price one pays for anal intercourse."[131] In addition, Simon Watney and Larry Kramer, among others, observe that the gay community provides most of the volunteer workforce on AIDS
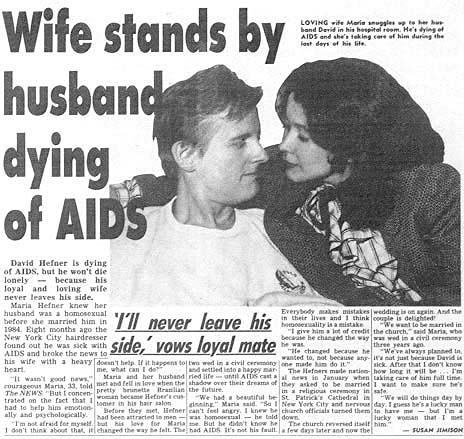
4. Although cases of women with AIDS were reported early on, women rarely appeared in the
official AIDS story except in secondary and traditional roles as mates and caretakers. Maria
Hefner was prototypical: She knew her husband was homosexual, but love conquered all. They
made national news in January 1987 after they learned he had AIDS and sought to be married
in a religious ceremony in St. Patrick's Cathedral. Weekly World News (17 February 1987, p. 17)
shows "loving wife Maria" taking care of David "during the last days of his life."
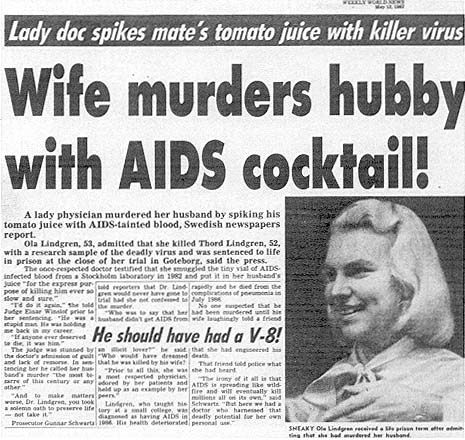
5. A few months later, another wife in Weekly World News (12 May 1987) plays quite a different
part in the AIDS story. Ola Lindgren, a Swedish physician, is reported to have murdered her
husband with virus-laden tomato juice (there is little documentation that oral transmission of
HIV would accomplish this). A photo shows "sneaky" Lindgren smiling, while the story tells
us that this "lady doc" murdered "hubby with AIDS cocktail!" Here was evidence of a female
literally carrying the virus home and giving it to her innocent husband, who gets the tabloid
fate he deserves for having married an ambitious professional woman: an epitaph from
Madison Avenue.
hotlines and other AIDS projects; when public information or television films or advertisements suggest the spread of AIDS to new groups, the "worried well" jam the phone lines beyond the capability of volunteers to answer. There are thus pragmatic reasons, until new groups of volunteers can be enlisted and trained, not to exaggerate the risk to this larger group.[132]
A third reason, I believe, essentially involves a desperate and terrorized effort to control signification. Faced with the nexus of sex and death, its fragmentation into hundreds of allied discourses, the breakdown of coherent categories of sexual identity into postmodernist "bundles of practices," and finally the virus itself with its capacities for infinite replication, who would not resist the entry of Woman, carrying the heavy baggage with which history has equipped her. As historian Allan M. Brandt notes, venereal diseases have typically been assigned a female identity; he cites a number of posters designed for U.S. servicemen, which show the equation of women with venereal disease (in one widely disseminated poster from World War II, for example, a painted prostitute walks down the street, arm in arm between Hitler and Hirohito; the caption reads: "VD: THE WORST OF THESE").[133] In this book and elsewhere, Brandt argues that AIDS has followed the historical pattern of earlier sexually transmitted diseases in generating fears of casual contact, concerns about contagion, stigmatization of victims as agents of the disease, and a search for a "magic bullet." AIDS is not yet, however, a particularly feminized disease, perhaps because, thus far, gay men have served so well as the Contaminated Other. As I have observed elsewhere, HIV is often anthropomorphized as a secret agent, but so far the gender is that of James Bond, not Mata Hari.[134] So long as the virus is characterized as "pure information," belonging to the largely male domain of perfect codes and high theory, it may resist a feminine conceptualization.
We should be aware, however, that language is already traveling from the site of the "sexually active" gay male body to the "promiscuous" female body. Numerous metaphors appearing in newspapers and scientific journals are cited by communication researchers.[135] Water metaphors appearing in 1987 ("IV drug users are the hole in the dike to the general population," "prostitutes are reservoirs of disease," and the "moist, vulnerable mucous membranes" of the female sexual organs) are reminiscent of the gendered tropes of history identified by, for example, Emily Martin and Allan M. Brandt.[136] In the Weekly World News , crème de la crème of supermarket tabloids, a loyal wife who stands by her husband with AIDS contrasts sharply with a new role for
women: a wife—a physician—who adds an HIV-infected blood sample to her husband's tomato juice and, with apparent relish, watches him develop AIDS and die.[137] The film Fatal Attraction , recapitulating Alfred Hitchcock's The Birds , gives us a taste of the consequences of "promiscuity."[138] Meanwhile, biomedical journals record the saga of an "exotic virus" infecting "exotic" African female bodies; now we learn that like this "fragile" AIDS virus our female bodies are "fragile," too, not rugged and tough after all but penetrable, "moist and vulnerable," or riddled with cracks and potholes. Are we now to become the carriers of this epidemic, ruthlessly moving everywhere? Is the female body, in fact, meaning itself, contaminating everything with its reservoirs of possibility and death? Reservoirs breaking down and letting language flow out, uncontainable within definitions? Like the virus, wearing an innocent disguise, are we not double agents, in league with the enemy? The question is how to disrupt and renegotiate the powerful cultural narratives surrounding AIDS. Homophobia, racism, and sexism are inscribed within other discourses at a high level, and it is there that they must be disrupted and challenged.
This leads to a fourth reason for the ambiguous positioning of women in AIDS discourse: Our relative failure—as feminists and as women—to address the problem of AIDS in challenging, theoretically comprehensive, or politically meaningful ways. In a final section, I will suggest some problematic aspects of current AIDS discourse by and about women as well as some useful directions toward a more satisfactory feminist analysis.
Women and AIDS: Toward a Feminist Analysis
Any analysis of AIDS based on a faith in stable boundaries between risk groups ignores everything we know about the realities of human sexual behavior and sexually transmitted infection. It further ignores the growing presence of AIDS as a dominant factor in the social life of the twentieth century in behavior, in law, in policy, in education, in health-care coverage, and in virtually all other areas of experience which, sooner or later, will touch every citizen.
Unless feminists take a broader and more active role in articulating the nature and meaning of the AIDS crisis, what is in store? One answer is that we will not understand the potential consequences of our own everyday sexual behavior, and this, I think, goes for gay as well as
straight women. Sexually liberated from the hegemony of the magical projectile penis, we should not assume the absolute truth of the scientific hypothesis that an "injection" of the virus is the sine qua non of infection. Even if it turns out that a critical mass of HIV is a relevant factor, this may vary in individuals. More crucially, sexual practices vary enormously among gay women as among all other people, and some of these practices may facilitate HIV transmission.
The point, again, is that statistical probabilities should not be transformed into theoretical absolutes. A second answer, however, is that as women become aware of the potential for risk, only a collective, feminist political analysis can contest the purely self-interested, self-help perspective now beginning to emerge in many publications by and /or for women. In April 1987, for example, full-page advertisements for Mentor contraceptives appeared in several women's magazines (fig. 6). A healthy and attractive woman, in full color, looks pensively out at the camera: "I never thought I'd buy a condom." Underneath, the copy reads: "INTRODUCING MENTOR CONTRACEPTIVES. THE SMART NEW WAY TO PROTECT YOURSELF." And at the bottom of the page, under a photo in which the individually packaged condom resembles nothing so much as a container of yogurt: "SMART SEX IN THE 80's."[139] The self-congratulatory tone of this advertisement echoes, in my view, much of what has appeared in publications for women.
Another example: "For some women," writes Erica Jong in the April 1986 issue of New Woman , "the AIDS crisis may be a way to come to terms with the fact that they never really liked multiple-partner sex in the first place." And, she adds playfully, "think of the time saved for working, for playing, for family, for gardening, for needlepoint!" AIDS was not even an issue two years ago, she continues, so the current flood of information on heterosexual transmission is so sudden, it is overwhelming—and hard to assimilate. Given the "plague mentality" of the media, "what's the informed woman to think—and beyond that, to do—about AIDS?" She continues:
By far the sanest and most detailed discussion of the disease I have read was published in Discover magazine's December 1985 issue. Its message to women was for the most part reassuring. Discover concluded that AIDS is 'the largely fatal price one can pay for anal intercourse'; that the virus 'is only borne in the blood and semen'; that AIDS is a difficult disease to catch; and that vaginal intercourse is much less likely than anal intercourse to spread the disease because of the ruggedness of the vaginal lining and its relatively few exposed blood vessels.
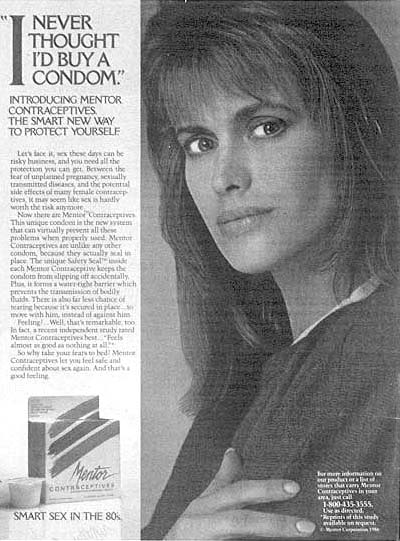
6. In ads in major U.S. women's magazines in the spring of 1987, a beautiful woman
praises a condom that sounds like a Greek god and looks like a container of yogurt.
It is said that AIDS has brought back the 1950s, but back then it wasn't women who
bought the rubbers. DON'T GO OUT WITHOUT YOUR RUBBERS advises another
ad for women, because, "if a woman doesn't look out for herself, how can she be sure
anyone else will?"
So here is Langone's article, with all its problematic, false certainties reproduced intact to reassure women.[140] To make matters worse, Jong highlights a set of boxed "facts" entitled "Good News (for Women) about AIDS." She begins by contrasting our old friends, the vulnerable rectum and the rugged vagina: "moreover, the tissue in the vagina has fewer blood vessels than the rectum, and natural lubrication during intercourse lessens the chances of tears." Then come the alibis (it 's them , officer , not me ; there , not here ):
1. Women with AIDS in Africa actually got it from needles, or anal intercourse (denied by them ), or by contact with bisexuals (also denied by them ).
But heterosexual cases in Africa are now confirmed and appear to be wiping out whole villages .
2. The AIDS virus is fragile and cannot be easily transmitted especially if "simple sexual precautions like not exchanging bodily fluids" are followed.
Considering that organizations like New York City 's Gay Men 's Health Crisis and the San Francisco AIDS Foundation devote entire pamphlets and videos to explicating euphemisms like "exchanging bodily fluids ," it does seem that we might have expected more from the author who once brought us the "zipless fuck ."
3. Most women in the United States whose cases of AIDS are attributed to heterosexual transmission are long-term partners of intravenous drug users. The small number of these cases suggests that AIDS cannot be transmitted heterosexually, but if it can be, Jong quotes a physician who argues that "women who contracted AIDS got it from steady sex partners, not from one-night stands."
The conflation of "safe sex " with monogamy is clearly problematic ; and is the implication here that one-night stands are SAFER than "steady " relationships?
4. Researchers estimate that only 5 to 20 percent of those who test positive for the virus will develop the disease.
Even 5 to 20 percent is an enormous number—half a million to two million depending on who 's counting— but as of January 1988 the estimate was up to 25-50 percent, and it is now considered possible that few will be entirely symptom-free forever. The fact that the virus has now been known to be dormant for as long as fourteen years means it
may take some time before our understanding of the natural history of AIDS is complete. (Indeed, the large number of asymptomatic carriers is a key to the "success" of HIV: The fact that the virus does not kill quickly means there is ample time for it to be conveyed to new hosts via carriers temporarily without symptoms.)[141]
5. "Men haven't been very good to their immune systems" and therefore appear to be more susceptible to AIDS.
But this statement is apparently based on the health histories of men who already have AIDS—it is hardly fair to make it a statement about men in general (and probably not even about men with AIDS ).
And here is Jong's last piece of "good news (for women)": AIDS, she writes, is like the terror of kitchen-table abortions in the 1950s. But maybe this is okay, she says, because it will make sex "a little more mysterious and precious again."
In April 1987, one year after Jong's "good news," AIDS appears in a Ms . magazine special issue on "The Beauty of Health." On the cover, an attractive woman in an orange shirt is eating an orange and smiling (fig. 7). "Wake up and be healthy!" the cover blurb commands, and lists what we should wake up to :
Skin Problems
RU-486 the Unpregnancy Pill
Exercises You Can Do In Bed
Guarding Against AIDS
Why Doncha Smile, Honey?
The two-page story by Lindsy Van Gelder (who earlier wrote a reasonably intelligent piece for Ms . and coauthored a competent article on "AIDS on Campus" for Rolling Stone ) begins with an anecdote in which she asks a sexually active woman friend whether she has asked her male friend to begin using condoms: "Rubbers?? " says the friend, "Yuck!!"[142] But, the author graphically points out, "You sleep not just with him but with all his sex partners." Should you trust him? she asks, and slips into the voice of Seventeen magazine in the old days: "This is a toughie." She offers some straight talk: "Brace yourself for a shocker: men lie to get laid." Van Gelder emphasizes some important points: The term "heterosexuals" is misleading, because "most people who contract
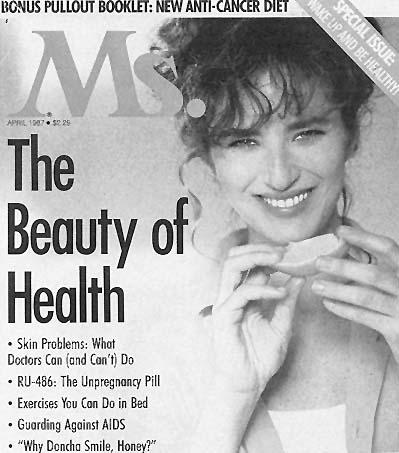
7. An attractive woman in an orange shirt eats an orange on Ms . magazine's April 1987
cover, which urges us to WAKE UP AND BE HEALTHY! Skin, exercise, AIDS: The
special issue offers tips for all kinds of pesky health problems. "Why Doncha Smile,
Honey?" the cover asks. But where AIDS is concerned, there's a better question:
Why is this woman smiling?
AIDS heterosexually are women"; she also argues that "safe sex with many different men is less risky than unprotected sex with one [infected] man," a logical deduction, but one that many writers fail to make. But the article ends with a breezy reinscription of conventional sexual division—that outdated staple of Ms . magazine's version of feminism—us against them (women against men): "How much do you want to bet that if female-to-male transmission begins to be documented in
great numbers, men will be demanding safe sex—with no wimpy worries about turning women off?"
Van Gelder's article is an example of condom journalism, a new genre that ranges from the Village Voice 's "Better Latex Than Never" to the safe-sex kits distributed to all Dartmouth students to the "how to" lessons of New Woman and Spare Rib to the critiques of condoms and condom advertising that have appeared in, among other places, the New York Times .[143] All of which prompts mention of another recent genre, the Heterosexual White Male's commentary on AIDS. Although the New York Times , as the "newspaper of record," has improved its coverage of AIDS (there is now a virtual AIDS page in almost every issue), even recent features in the New York Times Magazine leave a great deal to be desired. Peter Davis, for example, offers familiar insights about AIDS as though he had thought of them all by himself (AIDS connects "sex and death" is a sample) along with a significant amount of misleading information. In his search for heterosexuals reputed to be at risk for AIDS, for instance, he interviews what appear to be an elite assortment of investment bankers, executives, and elegant divorcees (his phrase). Already-infected heterosexual people, in the real kingdom of AIDS, remain invisible as we listen to the voices of Davis's upscale informants: "God," one woman tells him, "I wish I could have just one lunch in the Russian Tea Room where we talk about something besides AIDS." Davis quotes Dr. Mervyn Silverman's prudent advice ("just because there's no reason to panic doesn't mean there's no reason to be careful") but ultimately trivializes the gravity of the problem.[144]Newsweek , which has provided fairly steady coverage of AIDS and rarely downplayed its seriousness, ran a long and moving photo-story on those who died during 1987. Under the photographs ran captions that displayed what journalist Rex Wockner has called "back-door homophobia." The captions of the heterosexuals, for example, tell how they got infected (transfusion, etc.) while those of the gay people state their occupation without any transmission information. It is as though, says Wockner, even the dead must be kept clean from the suspicion of homosexuality.[145] As a final example of publications I consider problematic for women, I will mention sex therapist Helen Singer Kaplan's 1987 book The Real Truth About Women and AIDS . The book is both depressing and interesting. Geared toward heterosexual middle-class women and their "unborn babies," the book is depressing because it retrogressively asserts, in the name of saving women from a fate synonymous with death, that AIDS is caused by who you are, not by what
you do. The advice to "avoid unsafe practices," says Kaplan, is "nonsense!" Rather: "avoid infected partners." The only way to "avoid sexual exposure to high-risk males" is to (1) make any candidate take the ELISA test; (2) wait; (3) make him get tested again; and if he's clean and you still want to (4) go ahead and have a sexual contact.[146] And then, presumably, (5) handcuff him to you for the rest of your life.
An interesting feature of Kaplan's book, however, is her inclusion, in an appendix, of the transcript of a telephone conversation between a woman caller and a New York AIDS hotline. This transcript not only graphically dramatizes the complex and, as Kaplan points out, often problematic understandings of AIDS-related concepts, but it also lets us see AIDS as it is constructed in everyday talk.[147] Likewise, a BBC special on AIDS, broadcast around the world in September 1987, wove together commentary from professionals and from women on the front lines of the AIDS crisis: A Kenyan health care worker describes her workshops on AIDS and safer sex for prostitutes in Nairobi; a British woman, who, like her roommates, formerly used drugs and now tests HIV positive, talks about living with the knowledge of infection; a woman from a prostitute's organization describes her group's concerns about AIDS and preventive techniques, pointing out that prostitutes have extensive knowledge about alternative sexual practices that they could usefully be sharing with other women.[148]
In recent months (at any rate, in the September 1987 issue), Ms . finally got serious and published a photo-essay called "Facing AIDS" made up of photographs and words of women with or facing AIDS (fig. 8). This is not to say that such a representation is unmediated or closer to the "true experience" of AIDS, but it is a welcome departure from the chipper good news/bad news tone of other articles. The Spare Rib series initiated in 1987 also expressed a determination to begin—as women and feminists in alliance with others and in a larger social and economic context—confronting and working through the numerous questions and problems that AIDS creates (fig. 9).[149] Likewise, the 1987 Gay and Lesbian March on Washington moved dramatically toward the integration of the AIDS issue with broader cultural issues: the refusal to be extinguished, the refusal to die.[150] At the same time, as AIDS moves out of scientific journals, news stories, and print journalism and becomes increasingly a focus in the arts and mass culture, we can expect the continued diversification of discourse and resources.[151]
To sum up, then. A body of evidence suggests that AIDS is like other sexually transmitted diseases, capable of infecting women and men in
equal numbers and now spreading as rapidly by way of heterosexual contact as it once did by way of homosexual contact. Current data suggest, in other words, that the consequences of ignoring earlier evidence of heterosexual transmission may be devastating. Large numbers of people are already infected; many will die. Just as male homosexuals and intravenous drug users in the 1970s and early 1980s engaged in behavior that gave them pleasure without thinking it could kill them, many people today are engaging in activities that a few years from now may kill them.
My general argument is not that biomedical scientists have been "irresponsible" or that "the media" have created a sense of false security (or false terror), or that we can never truly know the biological "facts" about AIDS. What is important is that even scientific characterizations of the reality of AIDS are always partly founded upon prior and deeply entrenched cultural narratives. One step is to ask, as new narratives and new meanings are produced, such questions as the following:
How and why is knowledge about AIDS being produced in the way that it is?
Who is contributing to the process of knowledge production? To whom and by whom is this knowledge disseminated?
What are the practical and material consequences of any new interpretation? Who benefits? Who loses?
On what grounds are facts and truth being claimed?[152]
Any characterization of AIDS has a history, it has a vocabulary, origins, and consequences. Even a seemingly innocent and straightforward term like "the AIDS virus"—a term that now permeates technical and general AIDS discourse—is in fact profoundly misleading. Simon Watney, for example, scrupulously insists on calling the virus HIV and, speaking of a person known to be infected, HIV-positive . His point is not that what we call "HIV" is "real," but that this term is a much more preferable representation . What we call "AIDS," he argues, consists of some thirty diverse clinical entities and conditions. Although a virus may initiate the breakdown of the body's immune system, which in turn makes possible the development of one or more of the thirty diseases and conditions, it does not cause "AIDS."[153] Suppose a thief enters your house, ties you up, cuts your phone cord and burglar alarm, steals your silver, and uses your credit cards to catch the next plane to Copenhagen.
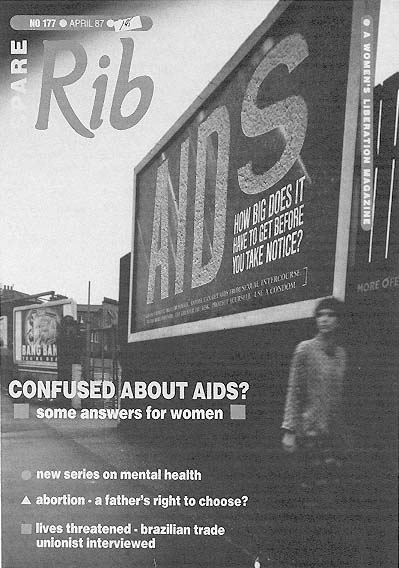
8. In April 1987 the British feminist magazine Spare Rib initiates a series on women and
AIDS that calls for a broad analysis of the AIDS crisis and coalitions with others. Authors
Susan Ardill and Sue O'Sullivan "attempt to focus on the impact AIDS is primarily having,
or will have, on us as women—through our sexuality, sexual practices and sexual identities."
Rather than pretending to have total knowledge and control, the authors urge readers to ask
questions, and "from there to go on and ask more questions, loudly and clearly" ( Spare Rib
177 [April 1987]: 14-19). Courtesy of Spare Rib , London.
9. Ann and Juliette at New York City annual AIDS vigil, 1985. In September
1987, Ms. runs a different kind of story on AIDS, a photo-essay by Jane Rosett
and Gypsy Ray, two women who work with AIDS; in photos and text, the darker,
exhausting dimensions of AIDS emerge. Courtesy of Jane Rosett, Brooklyn.
Because you're still tied up, you can't do anything when the microwave explodes and starts a fire. Is the thief an arsonist?[154] In the end, we cannot look "through" language to obtain knowledge about AIDS. Rather, we must examine how language itself produces what we think we know; and if we are to intervene, language is one place where that intervention must take place. Thus we can also ask:
What are the origins and implications of the language used to talk about such concepts as behavior, risk, persons at risk, modes of transmission—interpersonally and "epidemically" (Greek for among the people )—agents of transmission, health and illness?
What is the nature of the bodies said to be most "at risk" for AIDS? How are these bodies gendered? What is their discursive history?
What are the differences between "dominant" and "oppositional" accounts of this complex phenomenon?[155]
My argument in this essay is a simple one. Contests over meaning come into stark relief in the case of AIDS, which in multiple, fragmentary, and often contradictory ways we (as feminists perhaps, certainly as global citizens) struggle to understand. The name AIDS—and indeed the entire biomedical discourse that surrounds it—in part constructs the disease and helps make it intelligible. The construction of AIDS as a "gay disease," for example, is not based on "material reality"—which challenges any stable division between male and female, gay and straight, "promiscuous" and monogamous, guilty and innocent. Yet the construction inscribed again and again throughout our cultural discourses radically contains and controls this diverse and contradictory data, producing and reproducing monolithic identities of those "at risk" or not at risk, depending on their official classification.
The feminist community, or the communities of feminisms, have only recently begun to address the AIDS crisis. Feminists, who have learned to analyze and theorize about complex and contradictory data, can usefully contribute to an analysis of AIDS that brings together the collective insights of feminist scholarship and feminist theory to date. These would include historical description and analysis of women's experience during past epidemics and panics over sexually transmitted disease; critiques of conventional sociological categories in which women are inexorably linked to their male partners and to the diseases they contract; the intersections of gender, race, and class in relation to an
illness profiled in terms of nonintersecting categories; and theoretical work on the nature and history of gendered representation and on the evolution of Woman as a constructed identity. Finally, we might wish to ask whether the call for a "feminist analysis" is theoretically paradoxical: AIDS is complex, after all, in part because it exposes the artificiality of the categories and divisions that govern our views of social life and sexual difference. It challenges the existence of "women" as a monolithic sisterhood and as a meaningful linguistic entity. But feminist theory also suggests why a feminist analysis remains imperative: for women are both linguistic and material subjects who exist within language and history. Even as we work to deconstruct and perhaps finally to dissolve the linguistic subject, we must nonetheless keep our attention fixed relentlessly on the inequities still embodied in the material one.[156]
At the very end of The Intern 's Tale , after the scene I quoted when I began this chapter, one of the interns—Mac—dies, and Campbell, the protagonist, suggests that Maggie should be told. He learns she has read about Mac's death in the newspaper and called the hospital to inform them that she is a carrier of the virus but never developed the full-blown disease. The following morning she is found dead from an overdose of sleeping pills. Like many of the deaths of diseased women in history and literature, Maggie's suicide destroys, in a single gesture, the treacherous host—that is, the conscious subject, the material body required for replication—of the virus, of sexuality, of children, of life, of mind, of desire. Such self-extinction is part of women's discursive and historical legacy. We must therefore be alive to its potential incarnations in this latest social crisis. Nancy Shaw and Lyn Paleo point out, for example, that as more childbearing women become infected and more babies develop AIDS, childbearing may come under even more intense scrutiny by the state: Because if everyone practices safer sex, no babies will be born at all. Women, not gay men, may thus be among the first groups tested for HIV antibodies (with, presumably, a subsequent separation of the "clean" from the "dirty"). They also note that women, as caretakers in this epidemic, have thus far not felt they could protest sexism as they would under less life-threatening conditions.[157] And what of Kaplan's message that women must refuse to be the "bridges" between one infected pool and another; is there something of an extinction process working here? Meanwhile, a film like Fatal Attraction recapitulates for women the message gay men received when AIDS first occurred: What you have done for twenty years is wrong, what you desire is evil, sexuality is wrong, you are sick, you are dangerous, you must be punished.[158]
Maggie's death is the symbolic conclusion we must find ways to challenge and disrupt. This means, it seems to me, that we need to refuse the appeal of "binary division," of them versus us, of distinguishing ourselves from gay men and members of other "high-risk" groups. If we, as women, are to cope with AIDS in any reasonable and intelligent way, we must unequivocally see ourselves connected to it and refuse the lie that our own identities and gender offer magical protection against the invasions of that alien Other.
Notes
Research for this chapter was made possible in part by grants from the National Council of Teachers of English and the University of Illinois at Urbana-Champaign Graduate College Research Board and by a residency at the Ragdale Foundation in fall 1987. An earlier version was presented at the Colloquium on Women, Science, and the Body: Discourses and Representations, Society for the Humanities, Cornell University, May 1987. My thanks for comments or other assistance to Douglas Crimp, Elizabeth Fee, Daniel M. Fox, Mary Jacobus, Stephen J. Kaufman, Teresa Mangum, Emily Martin, John Mirowsky, Meaghan Morris, Cary Nelson, M. Kerry O'Banion, Eve Sedgwick, Daniel Tiffany, Simon Watney, Michael Witkovsky, and Leslie Kirk Wright. This chapter is part of an ongoing project entitled "Authority, Feminism, and Medical Discourse: Current Contests for Meaning."
1. Colin Douglas, The Intern ' s Tale (1975, New York: Grove, 1982), 180-181.
2. Two useful recent collections are Catherine Gallagher and Thomas Laqueur, eds., The Making of the Modern Body : Sexuality and Society in the Nineteenth Century (Berkeley and Los Angeles: University of California Press, 1987); and Susan Rubin Suleiman, ed., The Female Body in Western Culture (Cambridge: Harvard University Press, 1986). Mary Poovey, for example, "'Scenes of an Indelicate Character': The Medical 'Treatment' of Women," in Making of the Modern Body , ed. Gallagher and Laqueur, 137-168, documents the "longevity of [the] male aversion to female bodies" in quoting a nineteenth-century Boston physician who takes Hippocrates as his authority on women's illnesses ("What is woman?" asked Hippocrates: ''Disease.") and adds approvingly that "the wise old physician was not far wrong in his judgment" (166). See also Alain Corbin, "Commercial Sexuality in Nineteenth-Century France: A System of Images and Regulations," in Making of the Modern Body , ed. Gallagher and Laqueur, 209-219. Other useful sources on the historical specificity of representations of women include G. J. Barker-Benfield, The Horrors of the Half-Known Life : Male Attitudes Toward Women and Sexuality in Nineteenth-Century America (New York: Harper & Row, 1976); Caroll Smith-Rosenberg, Disorderly Conduct : Visions of Gender in Victorian America (New York: Knopf, 1985), 197-216; Mary Jacobus, "In Parentheses: Immaculate
Conceptions and Feminine Desire" (Paper presented at the Colloquium on Women, Science, and the Body: Discourses and Representations, Cornell University, May 1987); Ludmilla Jordanova, "Nature Unveiling before Science: Images of Women and Knowledge" (Paper presented at the Colloquium on Women, Science, and the Body: Discourses and Representations, Cornell University, May 1987); Jordanova, "Natural Facts: A Historical Perspective on Science and Sexuality," in Nature , Culture and Gender , ed. Carol P. MacCormack and Marilyn Strathern (Cambridge: Cambridge University Press, 1980), 42-69; Judith Walzer Leavitt, ed., Women and Health in America (Madison: University of Wisconsin Press, 1984).
Additional discursive links between women's bodies and disease are documented by Allan M. Brandt in No Magic Bullet : A Social History of Venereal Disease in the United States since 1880 , rev. ed. (New York: Oxford University Press, 1987). Venereal disease, in particular, has historically been given feminine personifications. One World War II army poster that Brandt reprints (following p. 164) shows the face of an attractive young woman. "SHE MAY LOOK CLEAN," the poster warns, "BUT PICK-UPS, 'GOOD TIME' GIRLS, PROSTITUTES SPREAD SYPHILIS AND GONORRHEA. You can't beat the Axis if you get VD." See also Cindy Patton, Sex and Germs : The Politics of AIDS (Boston: South End Press, 1985).
The characterization of women and women's bodies as diseased or pathological is not necessarily explicit. Sander L. Gilman, Difference and Pathology : Stereotypes of Sexuality , Race , and Madness (Ithaca, N.Y.: Cornell University Press, 1985) shows that even scientific and medical texts are pervaded by implicit cultural narratives about women's bodies (and black bodies). Emily Martin, The Woman in the Body : A Cultural Analysis of Reproduction (Boston: Beacon, 1987), identifies linguistic devices (metaphors, for example) in nineteenth- and twentieth-century medical texts used to describe human sexuality and reproduction; Martin's meticulous comparison of passages about women with comparable passages about men demonstrates the ways in which female functions are conceptualized negatively (for example, menopause is viewed as a breakdown in "production" or, in some recent texts, as a breakdown of "authority" and efficient communication) while male functions remain heroic and full of energy; her manipulation of the texts demonstrates how the same passages could be rewritten (but rarely are) to reverse the traditional conceptualizations.
Ruth Herschberger's Adam ' s Rib (1948; New York: Harper & Row, 1970), demonstrated earlier that a traditional—supposedly "objective"—account of male and female biological development is revealed as "patriarchal" only when a "matriarchal account" is created and placed beside it (75-82). Hilary Allen, ''At the Mercy of Her Hormones: Premenstrual Tension and the Law," m/f 9 (1984): 19-43, draws on the language and logic of recent British court decisions to show that they are founded on an implicit assumption that women are always already pathological (thus "premenstrual tension" is essentially a permanent—and potentially disqualifying—condition). Bryan Turner, The Body and Society (London: Basil Blackwell, 1984), 2-3, writes that disorders of the body, especially women's bodies, are often treated as disorders of society; order is pre-
served by the control of women's bodies under a system of patriarchy (see also 115-176, 204-226). See also Barbara Ehrenreich and Deirdre English, Complaints and Disorders : The Sexual Politics of Sickness (Old Westbury, N.Y.: Feminist Press, 1973).
The long-standing deployment of the human body as an image of society takes on special apocalyptic force in some recent "postmodern" accounts: like contemporary society, the body too is increasingly commodified and diseased, and frequently this diseased society / body is conceptualized as female: see, for example, Christine Buci-Glucksmann, "Catastrophic Utopia: The Feminine as Allegory of the Modern," in Making of the Modern Body , ed. Gallagher and Laqueur, 220-229; Arthur Kroker and David Cook, The Postmodern Scene : Excremental Culture and Hyper-Aesthetics (New York: St. Martin's, 1986); and Edward Shorter, A History of Women ' s Bodies , chap. 10 (New York: Basic Books, 1982).
3. Thomas Laqueur, "Orgasm, Generation, and the Politics of Reproductive Biology," in Making of the Modern Body , ed. Gallagher and Laqueur, 31-32; and Martin, Woman in the Body , 35, cite the vivid language of Walter Heape, a nineteenth-century antifeminist, antisuffrage zoologist at Cambridge, to suggest how extreme male views of menstruation could become. In menstruation, writes Heape in the late nineteenth century, the entire epithelium is torn away, "leaving behind a ragged wreck of tissue, torn glands, ruptured vessels, jagged edges of stroma, and masses of blood corpuscles, which it would seem hardly possible to heal satisfactorily without the aid of surgical treatment" (Heape was the first to use the term estrus , a neologism from Latin for gadfly to mean ''frenzy, rut, heat"). As Laqueur notes, Heape did represent an extreme, but Martin observes that the 1977 edition of a widely used textbook of medical physiology disrupts its characteristically "emotionally subdued prose" to inform the reader that "to quote an old saying, 'menstruation is the uterus crying for lack of a baby."'
4. The duplicitous female body is also signaled in The Intern ' s Tale when another woman successfully deceives Campbell into thinking she is a virgin and still another woman's apparent indigestion turns out to be appendicitis. This long-standing equation of women with acting is echoed in filmmaker Lizzie Borden's comment on Working Girls , her 1987 release about prostitutes: "Men's bodies are exposed and therefore vulnerable, whereas women have this ability to conceal. On some level, women have always dealt with theater" (Katherine Dieckmann, "Lizzie Borden: Adventures in the Skin Trade," Village Voice , 10 March 1987, 33).
5. Poovey, "'Scenes of an Indelicate Character,"' cites a variety of ways in which women and their bodies are judged to be duplicitous, including the view of hysteria as mimicry, the "periodicity" of the menstrual cycle as creating inherent "instability," and the invisibility and mysteriousness of the origins of many "women's illnesses"; the female body, wrote one physician, "mocks the reality of truth," and another wrote of hysterics that "these patients are veritable actresses" whose lives are "one perpetual falsehood." Duplicity and change-ability are also typically attributed to venereal diseases, most classically to syphilis, the "Great Imitator," with its diverse array of symptoms; "if you know syphilis," it used to be said, "you know medicine." Writes Ludvik Fleck, Gene-
sis and Development of a Scientific Fact , ed. Thaddeus J. Trenn and Robert K. Merton, tr. Fred Bradley and Thaddeus J. Trenn (1935; Chicago: University of Chicago Press, 1979), 12, "Syphilis is an extremely pleomorphic disease of many aspects. We read in many treatises that it is a 'proteoform' disease, since with its many forms, it reminds one of 'Proteus or Chameleon.' . . .There was hardly any disease or symptom that was not attributed to syphilis." Mark Thomas Connelly, "Prostitution, Venereal Disease, and American Medicine," in Women and Health in America , ed. Leavitt, 196-221, 284, argues that early twentieth-century education, conceptualization, and views on regulation of venereal disease were curiously inconsistent: On the one hand, the antiprostitution crusade and call for premarital testing for both women and men clearly assumed that both women and men could transmit disease; this assumption was contradicted by the widespread view that men are always the authors of these social crimes, women always their victims. Connelly argues that ''to insist that women could not spread venereal disease simply because they were women embodied an attitude that, even by 1915, was becoming increasingly absurd."
6. Blood and other liquids figure prominently in the history of sexually transmitted diseases. Fleck, Genesis and Development , discusses "bad blood" as a central concept in the history of syphilis. Brandt, No Magic Bullet , 23, quotes early twentieth-century physician Homer Kelly's description of the city as a massive civic circulatory system, its "countless currents flowing daily in our cities" distributing morality and disease equally throughout the body politic. The "rising tide" of venereal disease was thus linked to urbanization and to immigration—the "incessant inpouring of a large foreign population." Brandt notes that a "rare blood disease" was the euphemism of choice for venereal disease in the press. Connelly, "Prostitution, Venereal Disease, and American Medicine," 214, cites early twentieth-century rhetoric that linked syphilitic blood to insanity: "The red mills grind out men's brains." Patton, Sex and Germs , 23, observes that as old myths about blood resurface, AIDS triggers not only homophobia but also hemophobia—fear of hemophilia. As members of a still feared and stigmatized group, many people with hemophilia have chosen to keep it a secret; getting AIDS, one man with hemophilia told Patton, had forced him out of the "clot closet." In turn, when the National Hemophilia Foundation established a "gay blood ban" in 1983, the executive director of the National Gay Task Force objected: "I don't have to tell you what 'gay blood—bad blood' could mean to a community that has been historically discriminated against" ("National Gay Task Force, Others, Decry Gay Blood Ban by National Hemophilia Foundation," The Advocate , 20 January 1983, 8).
7. Mary Ann Doane, "The Clinical Eye: Medical Discourses in the 'woman's film' of the 1940s," in The Female Body , ed. Suleiman, 152-174.
8. Poovey, "'Scenes of an Indelicate Character,"' discusses at length the role of silence in the nineteenth-century medical debates about the use of chloroform during childbirth, specifically, the value of the "quiet and unresisting body" for the physician. Above all, Poovey argues, "the silenced female body can be made the vehicle for any medical man's assumptions and practices because its very silence opens a space in which meanings can proliferate" (152); she describes this as the "metaphorical promiscuity of the female body" (153).
9. Sources for this analysis of gender in AIDS discourse are deliberately diverse, though primarily Anglo-American, and may be categorized as follows: (1) leading scientific and medical journals, (2) scientific and medical journals for general readers, (3) general circulation magazines and newspapers, (4) books and reports on AIDS and AIDS-related topics, (5) conservative journals, (6) leftist journals, (7) gay and lesbian journals and newspapers, (8) general circulation women's magazines, (9) feminist journals, (10) supermarket tabloids, (11) national radio and network television programs on AIDS; and (12) other specialized print media. By the term "biomedical discourse about AIDS" I mean, unless otherwise specified, writings and statements about AIDS found in leading U.S. medical and scientific journals as well as public statements made by AIDS researchers, clinicians, and public health officers (i.e., examples are drawn primarily from categories (1) to (4) above). It is within this discourse that what is now the Received View on AIDS (its viral etiology) has evolved. For definition and discussion of the evolution, politics, and coverage of AIDS, see Dennis Altman, AIDS in the Mind of America (Garden City, N.Y.: Anchor / Doubleday, 1986). David Black, The Plague Years : A Chronicle of AIDS , the Epidemic of Our Times (New York: Simon and Schuster, 1986) and Randy Shilts, And the Band Played On : People , Politics , and the AIDS Epidemic (New York: St. Martin's, 1987). (Conservative commentators typically consider "the AIDS Establishment" to include scientists and physicians, public health officials, government officials, gay activists, and the American Civil Liberties Union—all in league to sacrifice the health of "innocent citizens" for the civil rights of "AIDS victims." Nat Hentoff's list, for example, in "The New Priesthood of Death,'' Village Voice , 30 June 1987,35, includes "public health officials and researchers, supervisory hospital personnel, bioethicists, liberal members of Congress, and a representative of the National Gay and Lesbian Task Force.")
10. A San Francisco female prostitute who died in 1978 appears to have been one of the earliest AIDS cases in the United States. Shilts, Band Played On , begins his chronicle of AIDS with the 1976 case of the Danish lesbian surgeon Grethe Rask, who became ill working in Zaire, describes AIDS's subsequent appearance and evolution in the United States—though in the United States only—as a "gay disease," and documents widespread resistance to evidence that women and babies could also develop AIDS. Ironically, however, the only entry for women in Shilts's detailed index is to the film Women in Love . Black, Plague Years , 74, reports one researcher who jokingly called the CDC's risk list the "4-H Club": "homos, heroin addicts, Haitians, and hookers." Several early studies explored whether prostitutes were at risk: Joyce Wallace, for example, "Acquired Immune Deficiency Syndrome (AIDS) in Prostitutes," in The Acquired Immune Deficiency Syndrome and Infections of Homosexual Men , ed. Pearl Ma and Donald Armstrong (New York: Yorke Medical Books, 1984), 253-258, concludes that despite normal T-cell ratios, working prostitutes in New York City could be at risk to develop AIDS; more precise studies (based on tests for HIV antibodies), however, remain inconclusive as to prostitutes' sexual risk because of high incidence of intravenous drug use in the same population (more on this below). When hemophiliacs and transfusion recipients started be-
coming ill, they bounced "hookers" off the 4-H list and simultaneously brought conventional "respectability" to the list. On the development of risk groups and conceptualization of AIDS, see Altman, Mind of America , esp. 30-37. Lawrence K. Altman, "Heterosexuals and AIDS: New Data Examined,'' New York Times , 22 January 1985, 1, 19, reports researchers' puzzlement over the heterosexual nature of AIDS in Africa as well as the small but confirmed number of heterosexually transmitted cases in the United States, and their disagreement over whether the public should be informed. There is still no real consensus among researchers or the public as to precisely why women may be "at risk," but evidence is now clear that women can become infected and can infect others. See Margaret A. Fischl et al., "Evaluation of Heterosexual Partners, Children, and Household Contacts of Adults with AIDS," Journal of the American Medical Association 257 (1987): 640-644; Mary Guinan and Ann Hardy, "Epidemiology of AIDS in Women in the United States: 1981 through 1986," Journal of the American Medical Association 257 (1987): 2039-2042; Constance B. Wofsy, "Human Immunodeficiency Virus Infection in Women," Journal of the American Medical Association 257 (1987): 2074-2076; and Marsha F. Goldsmith, "Sex Experts and Medical Scientists Join Forces against a Common Foe: AIDS," Journal of the American Medical Association 259 (1988): 641-643. See also Marilyn Chase's summary, "Spread of AIDS among Women Poses Widening Challenge to Medical Field," Wall Street Journal , 26 June 1986, and Matt Clark (with Mariana Gosnell) and Mary Hager, "Women and AIDS," Newsweek , 14 July 1986, 60-61. This information and more was amplified in Katie Leishman, "Heterosexuals and AIDS: The Second Stage of the Epidemic," The Atlantic (February 1987), 39-58. But Scott S. Smith's letter to the editor, The Atlantic (January 1988), 9-10, argues that the small number of women with AIDS to date hardly warrants the common "bubonic plague" comparison; Leishman replies that even with Smith's qualifiers (i.e., the "women" he counts are white, do not use intravenous drugs, never received transfusions, and are not sexual partners of high-risk men), the number represents only women with AIDS now, not the number who may be infected. A politically astute analysis is offered in Diane Richardson, Women and AIDS (New York: Methuen, 1987).
11. The question of how AIDS is defined by the CDC, the agency responsible for surveillance, exemplifies the nontransparent nature of language in relation to reality: as knowledge of the "reality" of AIDS increases, redefinition is regularly called for; but a new definition reorganizes the reality now under surveillance. The 1986 reclassification of AIDS cases is reported in Centers for Disease Control, "Update: Acquired Immunodeficiency Syndrome—United States," Morbidity and Mortality Weekly Report 35 (12 December 1986): 757-760, 765-766, and discussed in Eve K. Nichols, Mobilizing Against AIDS : The Unfinished Story of a Virus (Cambridge: Harvard University Press, 1986); reports in the general media include Kathleen McAuliffe et al., "AIDS: At the Dawn of Fear," U . S . News and World Report , 12 January 1987, 60-69; and Associated Press, "571 AIDS Cases Tied to Heterosexual Cases," Champaign-Urbana News-Gazette , 12 December 1986, A-7.
12. David Baltimore and Sheldon M. Wolff, Confronting AIDS : Directions for Public Health , Health Care , and Research (Washington, D.C.: National Academy Press, 1986).
13. U.S. Surgeon General, U . S . Surgeon General ' s Report on Acquired Immune Deficiency Syndrome (Washington, D.C.: Public Health Service, 1986).
14. See Thomas W. Netter, "Cases of AIDS Rise around the World," New York Times , 5 October 1986, 7. By May 1987 WHO reported at a press conference that 112 countries had reported cases of AIDS (see "Official Warns of 'Racist, Fascist' Approaches to AIDS," American Medical News , 12 June 1987, 19).
15. See the cover of U . S . News and World Report , 12 January 1987, and the story in that issue by McAuliffe et al., "AIDS: At the Dawn of Fear." Accompanying the story, a graph showing rising numbers of AIDS cases cuts across a two-page photograph of the roofs of Manhattan apartment buildings, while a boxed insert lists U.S. "Hot Spots"—cities with high numbers of cases. These dual allusions to real estate and vacation spots function to domesticate AIDS for an upscale New York City readership.
16. Pie-shaped charts (see, for example, the overview in Issues in Science and Technology 2 (1986): 2) "hid" cases of AIDS among women within the category "Other"—meaning unknown, no known risk factor, risk factor could not be established. Leslie Kirk Wright suggests that "Other" has moved from a benign euphemism for presumed heterosexuals in earlier publications to newly undesirable ''others" (personal communication). Stephanie Poggi, " In These Times : With Friends Like Us, Who Nee [sic] ," Gay Community News , 12-18 July 1987, 3, satirizes the ubiquitous AIDS pie-shaped charts in her attack on the leftist publication In These Times ' s endorsement of mandatory HIV testing.
17. The extensive feminist literature on Woman as Other includes Simone de Beauvoir, The Second Sex , trans. and ed. H. M. Parshley (New York: Knopf, 1953); Shari Benstock, ed., Feminist Issues in Literary Scholarship (Bloomington: Indiana University Press, 1987); Luce Irigaray, Speculum of the Other Woman , trans. Gillian C. Gill (Ithaca, N.Y.: Cornell University Press, 1985); Virginia Woolf, A Room of One ' s Own (New York: Harcourt, Brace, 1929); Cary Nelson, "Envoys of Otherness: Differences and Continuity in Feminist Criticism," in For Alma Mater : Theory and Practice in Feminist Scholarship , ed. Paula A. Treichler, Cheris Kramarae, and Beth Stafford (Urbana: University of Illinois Press, 1985); Jonathan Culler, On Deconstruction : Theory and Criticism after Structuralism (Ithaca, N.Y.: Cornell University Press, 1982), 43-64; Toril Moi, Sexual Textual Politics : Feminist Literary Theory (New York: Methuen, 1985); and Catherine Belsey, Textual Practice (New York: Methuen, 1980).
Brandt, in No Magic Bullet , cites "otherness" in the history of venereal diseases, which are always said to originate in other races, other places, other classes; among the poor, among immigrants; among aliens. See also Judith Walkowitz, Prostitution and Victorian Society : Women , Class , and the State (New York: Cambridge University Press, 1983). During the Black plague of the fourteenth century, Jews were accused of "poisoning the wells" and were massacred. In the fifteenth and sixteenth centuries, the Spanish called syphilis "the
Portuguese disease," the Portuguese called it "the Moroccan disease" (Ladislav Zgusta, personal communication). According to Leslie Kirk Wright, "A Disease of the Other: AIDS Discourse and Homophobia" (Paper presented at the International Scientific Conference on Gay and Lesbian Issues, Amsterdam, December 1987), and Jamie Feldman, "Social Dialogue, Public Dilemma: French Research Perspectives on AIDS'' (Paper presented at the Medical Humanities and Social Sciences Seminar, University of Illinois College of Medicine, Urbana, January 1988), in France, where AIDS was at first called "the Moroccan plague," French researchers and clinicians have little difficulty incorporating Africans with AIDS into the French / European population of people with AIDS; American gay men, however, seem to remain the Other. In central Africa, meanwhile, AIDS is always said to have originated in one of the other countries. In Japan, "the other" is not homosexuals but foreigners; because Japan has never allowed "foreign" blood of any kind to be given to Japanese people, transfusion-related AIDS cases are nonexistent; see "AIDS Carrier's Baby Free from Virus, Gov't Confirms," Japan Times , 19 April 1987. On AIDS, plague, and Judaism, see Robert Kirschner, "Keeping AIDS in Perspective," Reform Judaism (Fall 1986): 12-14, and Angela Graboys, "The Courage of Sunnye Sherman," Reform Judaism (Fall 1986): 14-15, 36. Edward Albert, "Acquired Immune Deficiency Syndrome: The Victim and the Press," Studies in Communication 3 (1986): 135-158, reviews accounts of the general process through which communities create distinctions between the normal and the deviant; he uses this division to discuss media accounts of AIDS. For a theoretical account, see Gilman, Difference and Pathology .
18. Peter Davis, "Exploring the Kingdom of AIDS," New York Times Magazine , 31 May 1987, 32-40; Patricia M. O'Kane, R.N., letter to the editor, 28 June 1987, 78.
19. See Leishman, "Heterosexuals and AIDS"; Associated Press, "Doctors: Case Shows AIDS Can Spread Heterosexually," Champaign-Urbana News-Gazette , 10 April 1986, A-7; Thomas C. Quinn et al., "AIDS in Africa: An Epidemiologic Paradigm," Science 234 (November 1986): 955-963; Thomas A. Peterman et al., "Risk of Human Immunodeficiency Virus Transmission from Heterosexual Adults with Transfusion-Associated Infections," Journal of the American Medical Association 259 (1 January 1988): 55-58; L. H. Calabrese and K. V. Gopalakrishna, "Transmission of HTLV-III Infection from Man to Woman to Man," letter to the editor, New England Journal of Medicine 314 (1986): 987. Numerous papers on heterosexual transmission were presented at the Second International AIDS Conference, Paris, June 1986 (e.g., see the report by Lawrence K. Altman, "Study Says AIDS in Haiti Spreads Mainly by Heterosexual Activity," New York Times , 29 June 1986. Questions about routes of transmission continue; Daniel J. Lehmann and Suzy Schultz, "4 Women among New Cases Here in August," Chicago Sun-Times , 3 September 1987, 3, report that one woman was infected through heterosexual intercourse with a man who used intravenous drugs, two women were infected through blood transfusions, "and the fourth did not acknowledge risk factors for [AIDS]." To stress the potential danger of heterosexual relationships, graphic artist Milton Glaser designed a symbol for use in a World Health Organization AIDS prevention cam-
paign; the symbol shows two overlapping red hearts, and a blue skull within the intersecting space; Glaser said the image suggests that "the consequence of uncontrolled coupling is fearful" ("Official Warns of 'Racist, Fascist' Approaches to AIDS," 19).
20. Paula A. Treichler, "AIDS, Homophobia, and Biomedical Discourse: An Epidemic of Signification," Cultural Studies 1 (1987): 263-305. (Reprinted, October 43 [1987]: 31-70.) Connections between viral and linguistic contamination were paradigmatically, indeed clairvoyantly, represented by William S. Burroughs in Electronic Revolution (Cambridge, England: Blackmoor Head Press, 1971). In the AIDS crisis a 1987 MacNelly cartoon for the Chicago Tribune shows Ronald Reagan pulling on plastic gloves as he peers into a room marked "Speechwriters" and asks "The AIDS speech ready?" A 1987 AIDS public service announcement sponsored by Esprit clothing likewise links the two epidemics through its slogan "Spread the word, not the virus" (as Julian Halliday has suggested to me, this AIDS message seems to be framed by Esprit's larger interest in promoting the notion that health, like Esprit clothing, makes you look good). On the general question of the linguistic construction of scientific reality, see Susan Sontag, Illness as Metaphor (New York: Farrar, Straus & Giroux, 1978); Bruno Latour and Steve Woolgar, Laboratory Life : The Construction of Scientific Fact (Cambridge: Cambridge University Press, 1985); David Bloor, Knowledge and Social Imagery (London: Routledge & Kegan Paul, 1976); Barry Barnes and David Bloor, "Relativism, Rationalism and the Sociology of Knowledge,'' in Rationality and Relativism , ed. Martin Hollis and Steven Lukes (Cambridge: MIT Press, 1982), 21-47; Roger Cooter, "Anticontagionism and History's Medical Record," in The Problem of Medical Knowledge : Examining the Social Construction of Medicine , ed. Peter Wright and Andrew Treacher (Edinburgh: Edinburgh University Press, 1982), 87-108. With respect to the media, see Tony Bennett, "Media, 'Reality,' Signification," in Media , Culture , Society , ed. Michael Gurevitch, et al. (London: Methuen, 1982), 287-308; and Todd Gitlin, The Whole World Is Watching : Mass Media in the Making and Unmaking of the New Left (Berkeley and Los Angeles: University of California Press, 1980). Gitlin, 251, writes that news is, among other things, "the exercise of power over the interpretation of reality."
21. Shilts, Band Played On , 67.
22. Ibid., 43.
21. Shilts, Band Played On , 67.
22. Ibid., 43.
23. Centers for Disease Control, " Pneumocystis Pneumonia—Los Angeles," Morbidity and Mortality Weekly Report 30 (5 June 1981): 250-252.
24. Shilts, Band Played On , 171, describes the coining of the acronym AIDS. In Africa, posters warn against "'Slim' Disease / AIDS." Right-wing Lyndon LaRouche supporters in the Montreal airport post signs that play on the French acronym for AIDS: "Give our children SDI [Strategic Defense Initiative, or Star Wars], not SIDA." Joanne Edgar, "Iceland's Feminists: Power at the Top of the World," Ms . (December 1987), 30, notes that to preserve the purity of the Nordic languages, official policy in Iceland prohibits borrowed words; instead of the word AIDS, a public opinion poll chose the Icelandic word eydni "wasting" or "destruction." Black, Plague Years , 60, comments that CDC task force director James Curran called the new name "reasonably descriptive without
being pejorative"; but, Black adds, "names have power." According to Jim D. Hughey, Robert N. Norton, and Catherine Sullivan, "Confronting Danger: AIDS in the News" (Paper presented at the Annual Meeting of the Speech Communication Association, Chicago, November 1986), several companies have removed the word aid from their titles; Jennifer Dunning, ''Suit Filed over Benefit for AIDS," New York Times , 27 August 1987, 20, reports that an organization that raises funds for young adults with cancer through an annual benefit called Dance for Life is suing an organization planning an AIDS benefit called Dancing for Life. A spokesperson for the Dance for Life group said, "If we lose our primary funding source and our identity because we are identified with Dancing for Life, then it is the equivalent of our death." George Whitmore, "Bearing Witness," New York Times Magazine , 31 January 1988, reports that some black and Hispanic people prefer the specific diagnosis of Kaposi's sarcoma or Pneumocystic carinii pneumonia to AIDS. Whatever term is used acquires its own power. Patton, Sex and Germs , 24, writes that one man put a pink triangle on his hospital door with the sign "AIDS Camp."
25. On the evolution and some of the problematic issues in characterizing "risk groups" for AIDS, see Keewhan Choi, "Assembling the AIDS Puzzle: Epidemiology," in AIDS : Facts and Issues , ed. Victor Gong and Norman Rudnick (New Brunswick, N.J.: Rutgers University Press, 1986), 15-24; and Ann Guidici Fettner and William Check, The Truth about AIDS : Evolution of an Epidemic (New York: Holt, Rinehart and Winston, 1985). Harry Schwartz, "AIDS in the Media," in Science in the Streets : Report of the Twentieth Century Task Force on the Communication of Scientific Risk (New York: Priority Press, 1984), 92, describes the complexity of "the Haitian connection." Catherine Ross and John Mirowsky, "Theory and Research in Social Epidemiology" (Paper presented at the Second Conference on Clinical Applications of the Social Sciences to Health, University of Illinois at Urbana-Champaign, October 1980), note that using discrete categories to measure variables that actually exist along a continuum "represents a loss of information that may make results ambiguous." Gender yields discrete categories; but sexual practice, such as heterosexual or homosexual behavior, in many cases does not.
26. See Choi, "Assembling the AIDS Puzzle"; "Update: Acquired Immunodeficiency Syndrome" MMWR 35 (12 December 1986); "AIDS: What Is to Be Done?" Forum section, Harper ' s (October 1985), 39-52; and Altman, "Heterosexuals and AIDS."
27. A reporter for the Wall Street Journal wrote a piece on the epidemic in 1981 that the editors refused to print; in February 1982 the paper did accept a story centered around twenty-three heterosexual cases, primarily intravenous drug users. According to Shilts, Band Played On , 126, publication thus occurred only after "bona fide heterosexuals" had been infected; the story was headlined "New, Often-Fatal Illness in Homosexuals Turns Up in Women, Heterosexual Males." Geoffrey Stokes, "Press Clips," Village Voice , 15 October 1985, argues that a similarly misleading focus was evident on "60 Minutes" that same month when Diane Sawyer interviewed Pat Burke, a heterosexual with hemophilia who became infected through contaminated blood products and subsequently infected his pregnant wife; their son also became infected.
Stokes suggests that Sawyer's focus undermined the fact that hemophiliacs represent a tiny percentage of the population.
Edward Albert, "AIDS: The Victim and the Press," and Brian Becher, "AIDS and the Media: A Case Study of How the Press Influences Public Opinion" (Research paper, University of Illinois College of Medicine-Urbana, 1983) discuss media treatment across a range of publications. Julie Dobrow, "The Symbolism of AIDS: Perspectives on the Use of Language in the Popular Press'' (Paper presented at the International Communication Association annual meeting, Chicago, May 1986) notes the dramatic and commercial appeal of the common "cultural images" in popular press scenarios of AIDS. A theoretical analysis of media accounts in relation to questions of identity and desire is offered by Simon Watney, Policing Desire : Pornography , AIDS , and the Media (Minneapolis: University of Minnesota Press, 1987). Continued monitoring of AIDS coverage is provided by Geoffrey Stokes in his Village Voice column "Press Clips" (e.g., 11 October 1985, 3, 10).
28. In "An Epidemic of Signification," I note far-right beliefs that AIDS is God's punishment for homosexuals and that communists or the KGB introduced the virus into the United States to weaken the blood supply. See William F. Buckley, Jr., "Crucial Steps in Combating the AIDS Epidemic: Identify All the Carriers," New York Times , 18 March 1986, and Lyndon LaRouche, Jr. "My Program against AIDS," pamphlet (Washington, D.C.: LaRouche Democratic Campaign, 7 February 1987). As a number of commentators have pointed out, if AIDS is God's punishment to gay men, then lesbians, who are virtually AIDS-free, must be God's favorites. Hughey, Norton, and Sullivan, "Confronting AIDS." Compare Governor Lester Maddox's remark that drought was God's way of punishing everyone in Georgia.
29. For a reminder of how much was unknown in the early stages of the AIDS story, see Ruth Kulstad, ed., AIDS : Papers from Science , 1982-1985 (Washington, D.C.: American Association for the Advancement of Science, 1986); American Medical Association, AIDS : From the Beginning (Chicago: American Medical Association, 1987); and Fettner and Check, The Truth About AIDS .
30. Altman, Mind of America ; Black, Plague Years . Other comprehensive accounts include Fettner and Check, The Truth About AIDS ; Jacques Leibowitch, A Strange Virus of Unknown Origin , trans. Richard Howard, introd. Robert C. Gallo (New York: Ballantine, 1984); John Green and David Miller, AIDS : The Story of a Disease (London: Grafton, 1986); Patton, Sex and Germs ; Richardson, Women and AIDS ; and Shilts, Band Played On . Brandt, No Magic Bullet , 199, summarizes the ways that AIDS thus far recapitulates the social history of other sexually transmitted diseases: the pervasive fear of contagion, concerns about casual transmission, stigmatization of victims, conflict between the protection of public health and the protection of civil liberties; increasing professional control over definition and management; and the search for a "magic bullet." Despite the supposed sexual revolution, Brandt writes, we continue through these social constructions "to define the sexually transmitted diseases as uniquely sinful" (202). This definition is inaccurate but pervasive: and as long as disease is equated with sin, "there can be no magic bullet."
31. Sandra Panem, "AIDS: Public Policy and Biomedical Research," Hastings Center Report , special suppl., 15 (August 1985): 23-26. Public health policy is also addressed in Office of Technology Assessment, Review of the Public Health Service ' s Response to AIDS : A Technical Memorandum [Congress of the U.S.] (Washington, D.C.: Government Printing Office, 1985).
32. See Larry Kramer, "1, 112 and Counting," New York Native , March 1983, 14-27; Michael Lynch, "Living with Kaposi's," Body Politic (November 1982), 88; and Richard Goldstein, ''Heartsick: Fear and Loving in the Gay Community," Village Voice , 28 June 1983, 13-16. The questioning of established authority had occurred earlier in the struggle over whether homosexuality was to be officially classified as an illness by the American Psychiatric Association. See Ronald Bayer, Homosexuality and American Psychiatry : The Politics of Diagnosis (New York: Basic Books, 1981), as well as Jeffrey Weeks, Sexuality and Its Discontents : Meanings , Myths and Modern Sexualities (London: Routledge & Kegan Paul, 1985). (Albert, "AIDS," 140, notes, however, that of 2,500 psychiatrists polled almost ten years after the official change, 69 percent still defined homosexuality as "pathological.") In any case, AIDS first struck members of a relatively seasoned and politically sophisticated community (many of whom were also professionals in science, medicine, and government) at a time when American culture at large was contesting medical and scientific authority—points addressed by Altman, AIDS in the Mind of America , and Daniel M. Fox, "AIDS and the American Health Polity: The History and Prospects of a Crisis in Authority," The Milbank Quarterly , suppl., 64 (1986): 7-33. As Shilts notes, 16, 356, AIDS is a real threat to closeted gay men, serving in a sense as a "double diagnosis" that jeopardizes their anonymity and their lives. This dilemma took the form of an early AIDS sick joke, reported by Black, Plague Years :
Q:" What's the hardest thing about getting AIDS?
A: Convincing your mother you're Haitian.
Elizabeth Kastor explores this problem in the case of conservative fundraiser Terry Dolan (head of the National Political Action Committee, NCPAC) and others, "The Conflict of a Gay Conservative," Washington Post National Weekly Edition , 8 June 1987, 11-12.
33. Mary Poovey, "Speaking of the Body: A Discursive Division of Labor in Mid-Victorian Britain" (Paper presented at the Colloquium on Women, Science, and the Body: Discourses and Representations, Cornell University, May 1987). Poovey argues that in nineteenth-century Britain, womanhood was legally categorized with regard to both property and sex. Single women could own property but could not engage in sexual activity with men; married women could have sexual relations but could not own property. Prostitutes, Poovey argues, who could both own property and have sexual relations, can be seen as a "border case"—a case that contradicts or disrupts existing conceptions and stable dichotomies and generates discourse that is designed to restore a stable dichotomy.
34. Leslie Kirk Wright suggests that some linguistic features of "the AIDS scare" seem to be modeled on the "red scare" of the McCarthy era, including
the notion of the virus as fellow traveler, secretly using cells to build power (cf. Peter Jaret, "Our Immune System: The Wars Within," National Geographic (June 1986), 702-735, 723, 724: "This strategy makes it even easier for the virus to pass from cell to cell undetected"; "the normal cell turns traitor''). Actor Dack Rambo drew an explicit parallel: "I am convinced we are seeing the return of witch-hunting and McCarthyism because of the fear AIDS has generated" (quoted by Scott Haller, "Fighting for Life," People , 23 September 1985, 28-33).
35. Hypotheses about AIDS are reviewed by Altman, AIDS in the Mind of America ; Baltimore and Wolff, Confronting AIDS ; Kevin M. Cahill, ed., The AIDS Epidemic (New York: St. Martin's Press, 1983); and Gong and Rudnick, eds., AIDS : Facts and Issues .
36. Journalistic gatekeeping in AIDS research is discussed by Shilts, Band Played On ; he notes, for example, 157, that by May 1982 one paper, "hypothesizing an infectious agent as the cause of GRID, had now been rejected by every major scientific journal in the country" because it contradicted the then—dominant view that AIDS was a "life-style" problem. Dorothy Nelkin, "Managing Biomedical News," Social Research 52 (1985): 3, discusses the so-called Ingelfinger rule of the New England Journal of Medicine , which prohibits release of findings prior to publication; Arnold Relman, however, the journal's current editor, discusses suspension of the Ingelfinger rule and other changes in editorial policy designed to speed up publication of AIDS-related research ("Introduction," Hastings Center Report , special suppl. (August 1985): 1-2—but see also Lawrence K. Altman, "Medical Guardians: Does New England Journal Exercise Undue Power on Information Flow?" New York Times , 28 January 1988, 1, 13).
On another front, Simon Watney, in "AIDS: The Outsiders," Marxism Today (January 1988), discusses censorship in the United Kingdom, where the government's aggressive prevention campaign is undermined by its other activities, including the recent banning of all "safer sex" instruction materials as pornography (because they "promote homosexuality"). On the role of institutionalized scientific authority and existing scientific networks during the AIDS crisis, see David Black's discussion of "the AIDS Mafia" and AIDS "gestapo" in Plague Years , 113, and Shilts, Band Played On . Shilts obtained thousands of government documents through the Freedom of Information Act and shows that despite bitter behind-the-scenes disagreements, most of the scientists connected with federal agencies have tended to display unanimity in public. Outside the federal health-care network, evidence of gatekeeping fuels charges of an AIDS "party line" and conspiracy theories from left, right, and center. Joseph Sonnabend, M.D., for example, a discoverer of interferon and former scientific director of the AIDS Medical Foundation, founded the Journal of AIDS Research to print scientific articles he believed were being suppressed because they argued for a multifactorial cause rather than a single virus (see Black, Plague Years , 112-118, for discussion). Raymond Keith Brown, author of AIDS , Cancer , and the Medical Establishment (New York: Robert Speller, 1986), has chaired two symposia on controversial aspects of AIDS.
37. Leibowitch, Strange Virus , 5.
38. Congressman William E. Dannemeyer (R.-Calif.), October 1985, during a legislative debate on a homosexual rights bill (quoted by Langone, "Latest Scientific Facts," 29).
39. Anthropologist Carole S. Vance, who observed the Meese Commission on Pornography throughout its hearings and deliberations, analyzes the recurrent obsession with "natural receptacles" in her forthcoming book, A Vagina Surrounded by a Woman : The Meese Commission on Pornography , 1984-1985 . Compare the position on orifices held by Lyndon LaRouche, Jr., in "My Program against AIDS": ''I hold it to be true, that Creation has endowed our bodies with certain functions, including the body's orifices, each to be used in one way, and not contrary ways; . . . AIDS demonstrates afresh . . . that if society promotes the violation of the principles of our bodies' design, that society shall suffer in some way or another for this obscenity" (6). Whether blood transfusions violate "the principles of our bodies' design" is not addressed.
40. Black, Plague Years , 29. Jaret, "The Wars Within," 731, posits that sperm, ejaculated into a woman, are "foreigners in a hostile body" who must deploy several strategies to "accomplish their mission."
41. Black, Plague Years , 40.
42. Frances FitzGerald, Cities on a Hill : A Journey Through Contemporary American Cultures (New York: Simon and Schuster / Touchstone, 1987), 98.
43. "The A.I.D.S. Show-Artists Involved with Death and Survival," documentary produced by Peter Adair and Rob Epstein, directed by Leland Moss, based on production at Theatre Rhinoceros, San Francisco; aired on PBS, November 1986.
44. A "cofactor" is something that causes, contributes to, or makes possible an illness. Resistance and susceptibility are typically influenced by age, general health status, nutrition, exposure to environmental toxins, and presence of other infectious or parasitic agents. As Fettner observes in "Bad Science," 26, the notion really means that illness involves the interaction between unique genetic programing and a lifetime of environmental influences and cannot be analyzed in a vacuum. Reviewing the cofactors presently thought most likely to contribute to HIV infection and clinical symptoms, Fettner suggests that genetics ultimately may be most important.
45. Shilts, Band Played On , 131-132, reports that some gay men interviewed in the very early years were estimated to have had as many as twenty thousand sexual contacts; coupled with the likelihood of such men having a history of STDs and of going to bathhouses, the number of contacts created a network of men who were broadly exposed to numerous infectious agents. Some scientists came to use the term "amplification" to describe the role of the bathhouses in facilitating HIV infection and its geometric increase.
46. Examples of "conspiracy theories" include Gary Null with Trudy Golobic, "The Secret Battle against AIDS," Penthouse (June 1987), 61-68; John Lauritsen, "Saying No to HIV," New York Native , 6 July 1987, 17-25; and Charles L. Ortleb, "HTLV in Lake Tahoe" (subtitled: "Disease Worse than Originally Thought. Is It AIDS?"); New York Native , 11 May 1987, 6-8. Alternative views among scientists outside the core federal AIDS network receive little attention; several of these, including Peter H. Duesberg, "Retroviruses as
Carcinogens and Pathogens: Expectations and Reality," Cancer Research 47 (1 March 1987): 1199-1220, are discussed by Lauritsen, "Saying No to HIV," and Ann Guidici Fettner, "Bad Science Makes Strange Bedfellows," Village Voice , 2 February 1988, 25-28.
47. On the growing complexity of the clinical and epidemiological picture, see David G. Ostrow et al., "Classification of the Clinical Spectrum of HIV Infection in Adults," in Information on AIDS for the Practicing Physician , vol. 1 (Chicago: American Medical Association, July 1987), 7-16; Lawrence K. Altman, "AIDS Virus Always Fatal?" New York Times , 8 September 1987, 15-16.
48. In February 1982 Dr. Arye Rubinstein, a pediatrician at Albert Einstein College of Medicine in the Bronx, was seeing sick babies who seemed to have all the symptoms then considered characteristic of AIDS. He sent a paper on the subject to the New England Journal , but heard nothing; meanwhile, other scientists were calling his hypothesis "improbable if not altogether impossible. By its very name, GRID was a homosexual disease, not a disease of babies or their mothers" (Shilts, Band Played On , 124).
49. The titles of Nichols's Unfinished Story of a Virus and Leibowitch's A Strange Virus of Unknown Origin follow in the classic Microbe-as-Hero tradition of such biographers as Hans Zinsser, Rats , Lice and History : The Biography of a Bacillus (Boston: Little, Brown, 1934). In her interviews with French AIDS researchers, Jamie Feldman ("Social Dialogue, Public Dilemma") confirmed their perception of AIDS as the story of the virus (Feldman also concludes that for the French AIDS also became the story of "the underdogs outsmarting the big shots." Many famous French virologists and immunologists initially rejected the retrovirus theory of AIDS: "If it were a virus, the Americans would already have discovered it.")
50. See Treichler, "An Epidemic of Signification," for perspectives on the uncertainties, politics, and competing accounts that established the virus as the "cause" of AIDS and stabilized it as a legitimate scientific "fact"; Latour and Woolgar in Laboratory Life provide a fuller account of the scientific process through which facts are constructed. Self-conscious attention to the construction and interpretation of biomedical science is also provided by Black, Plague Years ; Altman, Mind of America ; and Marek Kohn, ''Face the Virus: Essential 1980s Biology," The Face (April 1987), 64-71.
51. Jaret, "The Wars Within."
52. A summary of the scientific account of retroviruses is provided in my "Epidemic of Signification" as well as in many sources cited here. The HTLV-I, isolated by Gallo in 1980, was the first retrovirus to be identified with a human disease (June E. Osborn, "The AIDS Epidemic: An Overview of the Science," Issues in Science and Technology 2 (Winter 1986): 40-55).
53. The name HIV specifies the pathological / clinical effect of the virus (immune deficiency) rather than (as HTLV or LAV does) the type of cell it attacks. The term HIV infection is now sometimes used as a generic name to signify the entire spectrum of possibilities (from asymptomatic infection to full-blown AIDS). Brown, AIDS , Cancer , and the Medical Establishment , objects to the name HIV as being "conciliatory" but too nonspecific because all microbes associated with AIDS are immunosuppressive. Duesberg, "Retroviruses," also
argues that HIV is at most a precipitating agent in AIDS; Duesberg told John Lauritsen of the New York Native that many respected scientists agreed with him in private but were afraid to do so in public.
54. See "AIDS: What Is to Be Done?" and Shilts, Band Played On .
55. Donna J. Haraway, in "The Biological Enterprise: Sex, Mind, and Profit from Human Engineering to Sociobiology," Radical History Review 20 (Spring-Summer 1979): 206-237, suggests a transformation within the field of immunology from the military combat metaphors of World War II to postwar conceptions of the body compatible with the postmodern cold war period in which communication and information are played for the highest stakes. (Cf. Jaret, "The Wars Within," 728: "Interleukin-2 is a lymphokine, one of a dozen or so known chemical 'words' with which immune cells communicate during battle."
56. AIDS media coverage is discussed in William Check, "Public Education on AIDS: Not Only the Media's Responsibility," Hastings Center Report , special suppl. 15 (August 1985): 27-31; Barbara O'Dair, "Anatomy of a Media Epidemic," Alternative Media 14 (Fall 1983): 10-13; Jonathan Alter, "Sins of Omission," Newsweek , 23 September 1985, 25; Jay A. Winsten, ''Science and the Media: The Boundaries of Truth," Health Affairs 4 (Spring 1985): 5-23; Watney, "Visual AIDS: Advertising Ignorance," New Socialist (March 1987), 19-21; Simon Watney and Sunil Gupta, "The Rhetoric of AIDS: A Dossier Compiled by Simon Watney, with Photographs by Sunil Gupta," Screen 27 (January-February 1986): 72-85; Watney, Policing Desire . Schwartz, "AIDS in the Media," concluded that despite problems, the press had in the end not encouraged hysteria. One deduces that Shilts, Band Played On , would argue that a little hysteria might have helped. Leishman, too, in the September 1987 Atlantic , argues forcefully that overconcern is necessary. See also Simon Watney, "People's Perceptions of the Risk of AIDS and the Role of the Mass Media," Health Education Journal 46 (1987): 62-65.
57. Fleck, Genesis and Development , 101, emphasis in original.
58. Hughey, Norton, and Sullivan, "Confronting Danger."
59. Public statements by scientists intended to reduce AIDS panic include Merle A. Sande, "Transmission of AIDS: The Case against Casual Contagion," New England Journal of Medicine 314 (6 February 1986): 380-382; and Erik Eckholm, "U.S. Officials Stress AIDS Is Not Spread by Casual Contact," New York Times , 27 June 1986, reports the strong statement issued by federal health officials asserting that "the AIDS virus cannot be spread through casual contact in the workplace."
60. "Strong New Candidate for AIDS Agent," Science 230 (May 1984): 147.
61. On the public health consequences of separating people "at risk" from the "general population," see Mathilde Krim, "AIDS: The Challenge to Science and Medicine," in "AIDS: The Emerging Ethical Dilemmas," Hastings Center Report , special suppl. 15 (August 1985): 2-7.
62. In "AIDS: What Is to Be Done?" 51.
63. Science and Gender (London: Pergamon, 1986), 4.
64. Rock Hudson permitted a statement to be made in Paris confirming his diagnosis on 25 July 1985; Michael Gottlieb, his physician in Los Angeles, issued an official confirmation on 30 July, and it is at this point that Shilts ends And the
Band Played On , for he considers it the major turning point in public perception of and response to the AIDS epidemic. Hudson died on 2 October 1985.
65. The treatment of Hudson's illness and death in the tabloids is revealing in this respect. The perceived natural division between the sexes ("women are women and men are men") is obviously challenged by the knowledge that Rock Hudson, a highly masculine screen actor, was homosexual. Discourse devoted to rendering this contradiction unproblematic takes the form of stories detailing Hudson's suffering from his gayness ("The Hunk Who Lived a Lie"), his supposed desire for a "normal" life with a wife and children, and his wish to be reunited with his mother. His underlying ''normalcy" is often signaled by showing him with his dogs (e.g., George Carpozi, Jr., "Rock: His Years of Triumph and Tragedy—In His Own Words," Star , 15 October 1985, 27-30). Indeed, a key figure in AIDS redemption stories is a pet; the presence in a photograph of a dog or a cat, or even a stuffed animal, seems designed to infantilize and render sympathetic the person with AIDS. In reporter George Whitmore's personal account of his struggle with HIV infection ("Bearing Witness"), a teddy bear functions as a recurrent talisman of hope, while a large color photograph shows Whitmore with his cat.
66. Both sexual transmission and blood-borne transmission continue to raise questions, primarily because no consensus about the actual mechanisms of transmission has been achieved. See the report of recent public surveys in Science (January 1988).
67. Krim, "AIDS: The Challenge to Science and Medicine," 4.
68. Jonathan Lieberson, "The Reality of AIDS," New York Review of Books , 16 January 1986, 44.
69. Leibowitch, Strange Virus , 72-73.
70. Nathan Fain, "AIDS: An Antidote to Fear," Village Voice , 1 October 1985, 35.
71. John Langone, "AIDS: The Latest Scientific Facts," Discover (December 1985), 40-41.
72. Langone, "The Latest Scientific Facts," 52. Though more vivid and apodictic (i.e., presented as unarguable), Langone's conclusion parallels the conclusions of many scientists. (Joan K. Kreiss et al., "AIDS Virus Infection in Nairobi Prostitutes: Spread of the Epidemic to East Africa," New England Journal of Medicine 314 [13 February 1986]: 417, suggest that a history of STDs in homosexual men may "cause mucosal or squamous epithelial discontinuity or bleeding," thus compromising "epithelial integrity" as a barrier to viral transmission.)
73. Weeks, Sexuality and Its Discontents ; see also Jeff Minson, "The Assertion of Homosexuality," m/f 5-6 (1981): 19-39; Wright, "A Disease of the Other"; and Mariana Valverde, Sex , Power and Pleasure (Philadelphia: New Society, 1987), ch. 4; "Bisexuality: Coping with Sexual Boundaries," 109-120. Valverde's discussion supports an argument that bisexuality, by challenging the binary normal / deviant model, furnishes another "border case."
Some health professionals and AIDS counselors avoid the word "gay" because for many people this implies a kind of identity or life-style; even "bisexual" may mean a kind of life-style. Although "homosexually active" is offi-
cially defined as having a single, same-sex sexual contact over the past five years, many who have had such contact do not identify themselves as "homosexual," and therefore as not at risk for AIDS. Nancy S. Shaw, "Women and AIDS: Theory and Politics" (Paper presented at the Annual Meeting of the National Women's Studies Association, University of Illinois, Urbana, June 1986), suggests that for women, too, the homosexual / heterosexual dichotomy confuses diagnosis and treatment in addition to the perception of risk. Many other examples of this fact have emerged in the course of the AIDS crisis.
74. Fettner, in "AIDS: What Is to Be Done?" 43.
75. Shaw and Paleo, "Women and AIDS."
76. Langone, "The Latest Scientific Facts," summarizes why many were skeptical about the African data. See also Patton, Sex and Germs ; Lieberson, "The Reality of AIDS"; and Altman, "Heterosexuals and AIDS."
77. Leibowitch, Strange Virus , 72-73.
78. The question of silence pervades discussions of venereal disease. The "medical secret" of Victorian society referred to the collusion of "physicians and male patients, either husbands or prospective husbands, which resulted in unsuspecting women being infected with venereal disease" (Connelly, "Prostitution," 202). Feminist challenges to traditional medical conceptions of women and women's health—designed to make women's voices heard—have long since entered the mainstream of American society to change standard medical practice in such areas as breast-cancer treatment, childbirth, and prescription of psychoactive drugs. This is an extensive body of literature, yet one in which the voices of middle-class white women continue to predominate. As general background for the present discussion, see Elizabeth Fee, "Women and Health Care: A Comparison of Theories,'' in Women and Health : The Politics of Sex in Medicine , ed. Elizabeth Fee (Farmingdale, N.Y.: Baywood, 1982), 17-34. For Fee, and others in this collection, "women" is not taken as a white, middle-class category but one that is, rather, continually intersecting with race and class.
79. The history of prostitutes in disease discourse is reviewed by Brandt, No Magic Bullet . Connelly, "Prostitution," 196, quotes Lavinia Dock's 1910 nursing manual which states that prostitution "is now as certainly the abiding place and inexhaustible source of . . . venereal disease, as the marshy swamp is the abode of the malaria-carrying mosquito, or the polluted water supply of the typhoid bacillus." The idea of marriage, Connelly argues, 200, and especially the middle-class married woman, was at the focal point of early twentieth-century discussions of venereal disease: "It was the fate of the married woman that became a master symbol of the disastrous consequences of venereal disease, its transmitters—profligate men—and its source—prostitution."
80. Shaw and Paleo, "Women and AIDS"; Erik Eckholm, "Prostitutes' Impact on Spread of AIDS Debated," New York Times , 5 November 1985, 15, 18; Lawrence K. Altman, "Study Examines Prostitutes and AIDS Virus Infection," New York Times , 27 March 1987; Centers for Disease Control, "Antibody to HIV in Female Prostitutes," MMWR 36 (27 March 1987): 157-161.
81. Quoted in Langone, "The Latest Scientific Facts," 51-52.
82. Quoted in ibid., 50.
81. Quoted in Langone, "The Latest Scientific Facts," 51-52.
82. Quoted in ibid., 50.
83. See R. R. Redfield et al., "Heterosexually Acquired HTLV-III / LAV Dis-
ease (AIDS-Related Complex and AIDS): Epidemiologic Evidence for Female-to-Male Transmission," Journal of the American Medical Association 254 (1985): 2094-2096; and R. R. Redfield et al., "Female-to-Male Transmission of HTLV-III," Journal of the American Medical Association 255 (1986): 1705-1706.
84. John J. Potterat, Lynanne Phillips, and John B. Muth, "Lying to Military Physicians about Risk Factors for HIV Infections," letter to the editor, Journal of the American Medical Association 257 (3 April 1987): 1727, offer plausible evidence that servicemen do lie to officials. As I have indicated above, however, independent evidence exists for female-to-male transmission; lying, in other words, can account for only a portion of cases thought to be heterosexually transmitted.
85. Harold Sanford Kant, "The Transmission of HTLV-III," letter to the editor, Journal of the American Medical Association 254 (1985): 1901.
86. Kreiss et al., "AIDS in Nairobi Prostitutes," warn that urban prostitutes may well "constitute a major reservoir of AIDS virus in such African capitals as Nairobi, Kigali, and Kinshasa," with "heterosexual men serving as vectors of infection" throughout the African continent (417). See also L. J. D'Costa et al., "Prostitutes Are a Major Reservoir of Sexually Transmitted Diseases in Nairobi," Sexually Transmitted Disease 12 (1985): 64-67; P. Van de Perre et al., ''Female Prostitutes: A Risk Group for Infection with Human T-cell Lymphotropic Virus Type III," The Lancet 2 (1985): 24-27; P. Piot et al., "Acquired Immunodeficiency Syndrome in a Heterosexual Population in Zaire," The Lancet 2 (1984): 65-69.
87. Studies continue to suggest that HIV infection in U.S. prostitutes is brought about primarily by intravenous drug use and not by sexual contact with multiple partners (see Shaw and Paleo, "Women and AIDS"). Kreiss et al., "AIDS in Nairobi Prostitutes," found, similarly, that among the ninety female prostitutes they studied in Nairobi, HIV antibody was not significantly associated with the number of sexual encounters per year; other nonrelevant factors included age, duration of prostitution, nationality, history of immunizations, injections of medication within the past five years, transfusions, scarification, operations, induced abortions, or dental extractions. Sexual exposure to partners of different nationalities, however, was associated with HIV seropositivity.
88. Shaw and Paleo, "Women and AIDS," 144.
89. Stephanie Salter, "AIDS, Rights," San Francisco Examiner , 16 August 1987, quotes Carol Leigh, a representative of COYOTE (Call Off Your Old Tired Ethics, a prostitutes' activist organization based in San Francisco) and of Citizens for Medical Justice. Leigh argues that studies linking HIV infection in prostitutes to multiple sexual contacts are not borne out by empirical evidence. Brandt, No Magic Bullet , reviews the historical links of prostitutes to disease and the conceptual separation of infected prostitutes (and other voluntarily sexually active women) from "innocent victims." In her important 1975 essay on sociological discourse, "She Did It All for Love: A Feminist View of the Sociology of Deviance," Marcia Millman observes that studies of male deviance often portray their subjects (e.g., jazz musicians) as interesting and articulate people; in contrast, studies of prostitutes (for researchers, the primary category
of "deviance" in women) silence their female subjects by quoting male "authorities" as often as the women themselves—even "in a supposedly empathetic study of prostitutes, the pimps are treated as more intelligent, observant, and trustworthy than the subjects of the study themselves!", in Another Voice : Feminist Perspectives on Social Life and Social Deviance , ed. Marcia Millman and Rosabeth Moss Kanter (Garden City, N.Y.: Anchor / Doubleday, 1975), 261; 251-279.
90. Quoted in Langone, "The Latest Scientific Facts," 50.
91. Associated Press, "AIDS Funding Boost Requested: Increase Would Bring $200 Million to Bear on the Disease," Daily Illini , 27 September 1985, 7. See also AIDS Hearing , House Committee on Energy and Commerce , Subcommittee on Health and the Environment , 17 September 1984, serial no. 98-105 (Washington, D.C.: Government Printing Office, 1985).
92. John Green and David Miller, AIDS : The Story of a Disease (London: Grafton, 1986), 110, urge "extreme caution" in interpreting evidence that anal intercourse is more efficient than vaginal intercourse and that therefore male-to-male transmission is more efficient than male-to-female. Wofsy, "HIV Infection in Women," points out that we must be concerned for women both as potential "infectees" and ''infectors."
93. On terminology and stereotyping connected with intravenous drug use, see Barrett, "Straight Shooters," Peg Byron, "Women with AIDS: Untold Stories," Village Voice , 24 September 1985, 16-19, and Steve Ault, "AIDS: The Facts of Life," Guardian , 26 March 1986, 1, 8. The list of drugs that can be "used" intravenously is long and by no means confined to either illegal or street drugs (e.g., prescription medications may also be injected). And as students of medical history-taking have long known, both the vocabulary and placement of questions can influence a client's answers (e.g., "Do you use medications?" and "Do you use drugs?" are not interchangeable, nor is the latter understood the same way when grouped with questions about the patient's current illnesses as opposed to questions about smoking and alcohol use).
94. Studies in New York and San Francisco show a greater increase in HIV infection among intravenous drug users than among gay men. Stephen C. Joseph, "Intravenous-Drug Abuse Is the Front Line in the War on AIDS," letter to the editor, New York Times , 22 December 1986, 18; Ronald Sullivan, "Addicts' Deaths from AIDS Are Termed Underreported," New York Times , 26 March 1987, 15; "Pro and Con: Free Needles to Addicts," New York Times , 20 December 1987, 20; Chris Anne Raymond, "Combatting a Deadly Combination: Intravenous Drug Abuse, Acquired Immunodeficiency Syndrome," Journal of the American Medical Association 259 (January 1988): 329, 332. Francis X. Clines, "Via Addicts' Needles, AIDS Spreads in Edinburgh," New York Times , 4 January 1987, 8, describes a situation in which the demographics of intravenous drug use and AIDS infection are very different from those of New York; with blacks and Hispanics most heavily infected in New York and white working-class youth in Edinburgh, Clines notes that, in Glasgow, heroin addiction in this population is high but AIDS infection is low, presumably as a result of the decision to provide free sterilized needles—a decision recently reversed in response to conservative pressure.
95. Shaw and Paleo, "Women and AIDS," discuss differences in AIDS epidemiology among women across the United States. Blood products and artificial insemination, for example, are the leading factors in HIV infection among women in California, whereas intravenous drug use is the leading factor in New York.
96. Quoted in Robert Pear, "Tenfold Increase in AIDS Death Toll Is Expected by '91," New York Times , 13 June 1986, A1, A17.
97. Shaw, "Women and AIDS: Theory and Politics."
98. Restrained discussions of the statistics and potential causes of AIDS and HIV infection in Africa include Lawrence K. Altman, "Linking AIDS to Africa Provokes Bitter Debate," New York Times , 21 November 1985, 1, 8; Kreiss et al., "AIDS in Nairobi Prostitutes"; Jean L. Marx, "New Relatives of AIDS Virus Found''; Science 232 (April 1986): 157; June E. Osborn, "The AIDS Epidemic"; Patton, Sex and Germs ; Sam Siebert with Alma Guillermo and Ruth Marshall, "An Epidemic Like AIDS," Newsweek , 27 July 1987, 38; Blaine Harden, "AIDS May Replace Famine as the Continent's Worst Blight," Washington Post Weekly Review , 15 June 1987, 16-17. More problematic accounts include Jonathan Lieberson, "Reality of AIDS," and Robert E. Gould, "Reassuring News About AIDS: A Doctor Tells Why You May Not Be at Risk," Cosmopolitan (January 1988), 146-204; the latter is a particularly reckless example of unfettered speculation reassuring Cosmo readers that "ordinary sexual intercourse" would not place them at risk for infection. According to Gould, heterosexual AIDS in Africa exists because "many men in Africa take their women in a brutal way, so that some heterosexual activity regarded as normal by them would be closer to rape by our standards."
99. Fran P. Hosken, "Why AIDS Pattern Is Different in Africa," letter to the editor, New York Times , 15 December 1986.
100. Douglas A. Feldman, "Role of African Mutilations in AIDS Discounted," letter to the editor, New York Times , 7 January 1987.
101. See, for example, Newsweek , 3 November 1986, 66-67, and 24 November 1986, 30-47; Jennifer Dunning, "Women and AIDS," New York Times , 3 November 1986, 22; McAuliffe, "AIDS: At the Dawn of Fear"; and Mortimer B. Zuckerman, "AIDS: A Crisis Ignored," U . S . News and World Report , 12 January 1987, 76; Leishman, "Heterosexuals and AIDS," and "Science and the Citizen," Scientific American 256 (January 1987): 58-59.
102. James W. Carey, "Why and How? The Dark Continent of American Journalism," in Reading the News , ed. Robert Karl Manoff and Michael Schudson (New York: Pantheon, 1986), 146-196, discusses the reduction in continuing news stories of explanations to "boilerplate, a continuing thread of standard interpretation inserted in every story" (185). In a number of publications, including the New York Times , the boilerplate paragraph for AIDS began in 1984 to include mention of a viral etiology and in 1987 to talk about "sexual" rather than "homosexual" transmission.
The public's understanding of AIDS and HIV infection remains tenuous. By late 1987 an astonishing 99 percent of the cross-section of U.S. citizens surveyed had heard of AIDS, yet a substantial percentage expressed the belief that one could "catch" AIDS via giving blood, toilet seats, physical proximity to an in-
fected person, or mosquitoes. The AIDS story is complicated and fluid enough to require regular reporters assigned to "the AIDS beat." This was clear when Jeffrey Levi, director of the National Gay and Lesbian Task Force, addressed the National Press Club on 9 October 1987 during the Gay and Lesbian March on Washington, D.C. Following Levi's address, a clear but essentially generic review of familiar AIDS facts and issues, at least two reporters in the audience were uninformed enough to ask the following questions: (1) "Isn't AIDS a media disease? A few years ago the government tried to give people shots for Barré . . . Gwillian . . . and they got paralyzed. Isn't AIDS a media invention?" and (2) "What is an 'op-por-tu-nis-tic infection'?" The first question presumably referred to the government's swine flu vaccination program in which a small number of people developed Guillan-Barré syndrome as a side effect; the second question was asked with heavy skepticism, as though to imply that Levi had concocted the term for political purposes.
103. As of January 1988 reported cases of AIDS in the United States totaled 50,265, 1,987 of which were reported to be caused by heterosexual transmission; 1,074 of this group were women. For a review of knowledge, statistics, and estimates of HIV infection in the United States as of December 1987, see MMWR 36, 18 December 1987, 801-804; the full report is available as MMWR , suppl., 36, 18 December 1987, S-6. Interviewed in January 1988, James W. Curran, director of the AIDS program at the CDC, predicted that although current "estimates of the total number of people infected remains complex and inexact, and the approaches used to compute a national HIV prevalence cannot be considered definitive. . . . The epidemic will get much worse before it gets better, both here and throughout the world." He continued: "We can expect the number of American AIDS cases to increase for the rest of this decade and that the problem will be with us for the rest of this century. Our best estimate is that between one million and 1.5 million Americans have been infected with the human immunodeficiency virus, and I am confident that this figure is neither too high nor too low." "Interview with James W. Curran," American Medical News , 15 January 1988, 1, 33-35. For more on current estimates and their potential consequences, see Klemens B. Meyer and Stephen G. Pauker, "Screening for HIV: Can We Afford the False Positive Rate?" New England Journal of Medicine 317 (July 1987): 238-241; and Gene W. Matthews and Verla S. Neslund, ''The Initial Impact of AIDS on Public Health Law in the United States—1986," Journal of the American Medical Association 257 (January 1987): 344-352.
The CDC has never predicted that AIDS or HIV infection would "explode" in the heterosexual population; though Harold Jaffe's denial of such an explosion was widely quoted in such a way that it appeared to reflect new evidence, Jaffe himself stressed that he was making "deductions" from current known evidence that 4 percent of AIDS cases were heterosexual, primarily in IV drug users; in line with previous CDC statements, Jaffe predicted that "the virus is more likely to spread gradually over a period of years, rather than explosively, into the heterosexual population." Lawrence K. Altman, "Anxiety Allayed on Heterosexual AIDS," New York Times , 5 June 1987, 11. See Redfield et al., "Heterosexuals and AIDS," and Warren Winkelstein, Jr., et al., "Sexual Prac-
tices and Risk of Infection by the Human Immunodeficiency Virus: The San Francisco Men's Health Study," Journal of the American Medical Association 257 (January 1987): 321-325, for predictions based on current distribution of HIV antibodies.
104. See Relman, "Introduction"; June E. Osborn quoted in Erik Eckholm, "Broad Alert on AIDS: Social Battle Is Shifting," New York Times , 17 June 1986, 19-20; Morton Hunt, "Teaming Up Against AIDS," New York Times Magazine , 2 March 1986, 42-51, 78-83; "AIDS: Science, Ethics, Policy,'' Forum section, Issues in Science and Technology 2 (Winter 1986): 39-73; Robert C. Gallo, "The AIDS Virus," Scientific American 256 (January 1987): 47-56. Jaret, "The Wars Within," 723, writes: "Indeed, had AIDS struck 20 years ago, we would have been utterly baffled by it."
105. Shilts, Band Played On , 191.
106. Simon Watney, "A.I.D.S. U.S.A.," Square Peg (Autumn 1987), 17.
107. Kulstad, ed., AIDS : Papers from Science ; AMA, AIDS : From the Beginning .
108. J. Z. Grover, "The 'Scientific' Regime of Truth," In These Times , 10-16 December 1986, 18-19. Grover points out a number of problematic terms and assumptions that recur in scientific writing about AIDS: (1) the term "AIDS victim" presupposes helplessness (the term "person with AIDS," or PWA, was created to avoid this), prevention and cure are linked to a conservative agenda of "individual responsibility," sex with multiple partners and / or strangers is equated with "promiscuity," and "safe" sexual practices are conflated with the cultural practice of monogamy; (2) it emphasizes the differences between "caregivers" and "victims," between scientific / medical expertise and other kinds of knowledge, between "those at risk" and "the rest of us"; and (3) it notes but fails to challenge existing inequities in the health care system.
109. On the subject of "AIDSspeak," see Richard Goldstein, "Visitation Rites: The Elusive Tradition of Plague Literature," Voice Literary Supplement 59 (October 1987); Leibowitch, Strange Virus ; Walter Kendrick, "AIDSspeak," Voice Literary Supplement 59 (October 1987); Patton, Sex and Germs ; Shilts, Band Played On , esp. 315-316; and Watney, "AIDS: The Cultural Agenda." Nor are texts the only point of debate. Some members of the San Francisco gay community complained early that public health warnings used euphemistic language ("avoid exchange of bodily fluids") and through innocuous pictures subverted the fact that AIDS was a deadly and physically ravaging disease (FitzGerald, Cities on a Hill ).
110. Nichols, ed., Mobilizing against AIDS .
111. Centers for Disease Control, "Update: Acquired Immunodeficiency Syndrome," MMWR 35 (December 12, 1986): 757.
112. Guinan and Hardy, "Epidemiology of AIDS in Women."
113. The mucous membrane is revisited by Helen Singer Kaplan, The Real Truth about Women and AIDS (New York: Simon and Schuster, 1987), 78: "the moist vulnerable mucous membranes" of the female genital organs. ACT-UP (AIDS Coalition to Unleash Power) protested an article by Dr. Robert E. Gould in the January 1988 Cosmopolitan magazine (described in n. 98) for promoting a sense of false security in women readers by claiming that there was
virtually no danger of contracting AIDS through "ordinary heterosexual intercourse." Condoms, Gould noted parenthetically, were relevant only to "anyone not sure whether she has any open vaginal lesions or infections." ACT-UP's protest flyer, however, counters that "in fact, most women have infections and internal lacerations that are asymptomatic and often caused by childbirth, IUDs, tampons, Herpes II, sex without lubrication, and other sexually transmitted diseases." Similarly, Ann Johnson, a London AIDS specialist quoted on the August 1987 BBC radio special, emphasized that "No trauma need be seen . . . There may be tiny areas of bleeding such as erosion on the neck of the womb which would be quite adequate for the virus to get into the bloodstream."
114. Shilts, Band Played On , describes the CDC's discussions of how to establish categories and classifications for AIDS, how to arrange risk factors in a hierarchy, what to do about overlapping categories, and how to keep track of phenomena with no official relationship as yet to AIDS. Guinan and Hardy, "Epidemiology of AIDS in Women," demonstrate some of the consequences of these decisions. The question of how best to define and classify AIDS and AIDS-related conditions—which involve some thirty different clinical entities and a spectrum of symptoms—also complicates the identification of health problems and assessment of the scope of the crisis. Not only has the CDC's initial surveillance definition been revised and broadened, but continuum models of symptoms (not necessarily progressive in time) have in general replaced former classifications by discrete disease (e.g., Kaposi's sarcoma).
An overview of current systems is given by David G. Ostrow, Steven L. Solomon, Kenneth H. Mayer, and Harry Haverkos, "Classification of the Clinical Spectrum of HIV Infection in Adults," in Information on AIDS for the Practicing Physician , vol. 1 (Chicago: American Medical Association, July 1987), 7-16. The authors remark, however, that "none [of these systems] satisfies all of the criteria required by public health officials, epidemiologists, clinicians, and researchers. . . . The desire to have an ironclad system that fully explains the progression of immunodeficiency and clinical symptomatology after HIV infection is understandable; however, it is not realistic at this time" (14-15).
115. The relatively few studies of women and AIDS are typically justified on the grounds that infected women may bear infected children and / or that measurement of infection in women provides an "index" to the spread of heterosexual AIDS. Guinan and Hardy, "Epidemiology of AIDS in Women," and the several studies by Redfield et al. use these justifications; similarly, Virginia Lehman and Noreen Russell, "Psychological and Social Issues of AIDS," in AIDS : Facts and Issues , ed. Gong and Rudnick, 246-263, mention women in a number of contexts but always under another heading-e.g., Children , or AIDS and Minorities . In part, this has to do with the politics of publishing and the convention of beginning scholarly articles with a clear and accepted raison d'être; thus, because research builds on other research, the invisibility of women in the AIDS narrative to date reinforces their invisibility in the future.
It is therefore important that researchers—those, at any rate, who do believe in the intrinsic importance of women—break this lineal citation pattern and insist on inserting women as women into biomedical discourse on AIDS. But the politics of pregnancy is also at work here. This emerges in a letter to JAMA
regarding the evolution of the CDC guidelines for preventing transmission of perinatal AIDS in HIV-positive women; Dr. David A. Grimes describes a series of meetings in which recommendations for counseling women about abortion as an option were progressively watered down and finally omitted altogether in the published version ( MMWR 34 [6 December 1985]: 721-726). Grimes's letter appeared in Journal of the American Medical Association 259 (January 1988): 217-218.
116. Stephen R. Ell, "The Venetian Plague of 1630-1631: Assessment of a Human Disaster," Medical Heritage 2 (March-April 1986): 151-156. "The disease spared no one," writes Ell (155); "primitive epidemiologic data" indicate that in Venice and its surrounding area there were 93,661 mortalities (or about one-third of the total population), among them 11,486 pregnant women, "a catastrophic blow to the reproductive capacity of the city. Yet, this inclination toward pregnant women is quite in keeping with the fact that pregnancy acts as a non-specific immune-suppressant." Barbara Tuchman, A Distant Mirror : The Calamitous 14th Century (New York: Ballantine, 1978), 92-125, provides a dramatic account of the Black Death, tracing the social and economic consequences of curtailed reproduction (consequences borne out by modern epidemiology).
117. Shaw and Paleo, "Women and AIDS," 150. We do not really know the clinical relevance of pregnancy, though one recent study of 120 pregnant women, reported in Center to Center 1 (1987): 5, concluded that HIV did not affect the clinical course of pregnancy, or vice versa.
118. See Patton, Sex and Germs . In January 1983 the CDC officially added heterosexual partners of people with AIDS to the list of high-risk groups. The MMWR cited two known cases of AIDS in women who were long-time partners of men with AIDS, noting also forty-three reports of previously healthy women who had developed Pneumocystis or other AIDS-related conditions, primarily after sexual contact with intravenous drug users—none of whom, however, had yet developed AIDS. Shilts, Band Played On , 225, suggests that this was one turning point in AIDS media coverage.
119. Reports of female-to-female transmission of HIV include Maria T. Sabatini, Kanu Patel, and Richard Hirschman, "Kaposi's Sarcoma and T-cell Lymphoma in an Immunodeficient Woman: A Case Report," AIDS Research 1 (1984): 135-137, on the case of a non-Haitian, non-drug-using thirty-seven-year-old black female who was a "lifelong homosexual" (as was her partner), and conclude that "this would suggest that females may harbor the AIDS agent as healthy carriers"; Michael Marmor et al., "Possible Female-to-Female Transmission of Human Immunodeficiency Virus," letter to the editor, Annals of Internal Medicine 105 (December 1986): 969. See also Vada Hart, ''Lesbians and AIDS," Gossip 2 (1986); and Ann Bristow, Andrea Devine, and Denise McWilliams, "AIDS and Women in Prison," Gay Community News , lesbian prisoner suppl., 23 August-5 September 1987, 10-11, who provide safer-sex guidelines for lesbians.
120. In 1983 the women members of a San Francisco gay Jewish congregation, Sha'ar Zahev, donated blood as a way of expressing solidarity with gay men. In 1984 the Blood Sister Project of San Diego collected blood from hun-
dreds of lesbians to contribute to the diminishing supply in blood banks. As a group with virtually no cases of AIDS-related disorders, lesbians were among the very safest of donor groups. Nevertheless, the association of "gay" with "blood supply" triggered gender-blind homophobia: Not only were there objections within individual communities to this contamination of the blood supply by homosexuals but conservative groups flooded the White House with telegrams demanding that Assistant Secretary for Health Edward Brandt be fired if he attended a Fund for Human Dignity dinner to present the award to the San Diego group. See Altman, AIDS in the Mind of America , 95; Shilts, Band Played On , 455-456; and Richardson, Women and AIDS , 88-89. Today, Blood Sisters chapters exist in many cities.
121. Altman, AIDS in the Mind of America , 94, notes both the "enormous energy and generosity" with which many lesbians have responded to the AIDS crisis. At the same time he suggests that solidarity has not been the uniform response: "Many lesbians feel resentment that gay men, who never showed any interest in questions of women's health, now seem to expect total commitment to AIDS activity from them."
122. Examples include Cindy Patton, "Feminists Have Avoided the Issue of AIDS," Sojourner (October 1985), 19-20, Cindy Patton and Janis Kelly, Making It : A Woman ' s Guide to Sex in the Age of AIDS (Boston: Firebrand, 1987); Richardson, Women and AIDS ; Byron, "Untold Stories"; Grover, ''Scientific Regime of 'Truth',"; Katie Leishman, "Two Million Americans and Still Counting," New York Times Book Review , 27 July 1986, 12; Katie Leishman, "Heterosexuals and AIDS: The Second Stage of the Epidemic," The Atlantic (February 1987), 39-58; Marcia Pally, "AIDS and the Politics of Despair: Lighting Our Own Funeral Pyre," The Advocate , 24 December 1985,8; Nancy S. Shaw, "California Models for Women's AIDS Education and Services," Report, San Francisco AIDS Foundation [333 Valencia St., 4th fl., San Francisco, CA 94103], 1986, and "Women and AIDS."
123. Examples include Altman, Mind of America ; Wayne Barrett, "Straight Shooters: AIDS Targets Another Lifestyle," Village Voice , 26 October 1985, 14-18; Richard Goldstein, "The Hidden Epidemic: AIDS and Race," Village Voice , 10 March 1987; Cindy Patton, "Resistance and the Erotic: Reclaiming History, Setting Strategy as We Face AIDS," Radical America , 68-78; Kramer, "Taking Responsibility for our Lives," Nancy Krieger and Rose Appleman, The Politics of AIDS (Oakland: Frontline Pamphlet, 1986). Kramer remains regularly enraged in print at what he perceives is the gay community's failure to play hardball politics (see, for example, "Taking Responsibility," as well as Watney's critique of it) and, after leaving Gay Men's Health Crisis, helped found ACT-UP, an activist zap group whose motto is SILENCE = DEATH. Both Patton and Watney have critiqued the left's general failure (despite differences in the United States and Britain) to contribute meaningfully to an AIDS political agenda.
124. See Background Paper, 1985 COYOTE convention summary, San Francisco, 30 May-2 June 1985; World Wide Whores ' News , report of the 1985 conference; Laurie Bell, ed., Good Girls / Bad Girls : Feminists and Sex Trade Workers Face to Face (Seattle: Seal Press Toronto: Women's Press, 1987); Frederique Delacoste and Priscilla Alexander, eds., Sex Work : Writings by
Women in the Sex Industry (Pittsburgh: Cleis, 1987); Lizzie Borden, Working Girls ; Judith Miller, "Prostitutes Make Appeal for AIDS Prevention," New York Times , 5 October 1986, 6. See also Barrett, "Straight Shooters." In the BBC AIDS special on women and AIDS, Louise Hansen, a British prostitute, reports the growing desire by clients for alternatives to high-risk sex, including condoms, "nonpenetrative sex," fantasy scenes, lesbian scenes, and argues—as does Carol Leigh (interviewed in Salter, "AIDS, Rights")—that ''people can learn a lot from the working skills that prostitutes have—like how to be assertive and alternative sexual practices." Prostitutes, they argue, should be seen as a valuable resource for information about sexual practices.
125. Erica Jong, "Women and AIDS," New Woman (April 1986), 42-48; Ellen Switzer, "AIDS: What Women Can Do," Vogue (January 1986), 222-223, 264-265; Jane Sprague Zones, "AIDS: What Women Need to Know," The [National Women ' s Health] Network News 11 (November-December 1986): 1, 3.
126. "Too Little AIDS Coverage," letter to the editors, Sojourner 10 (July 1985): 3.
127. Traditional roles available to women in the cultural narratives of AIDS include mother, spouse, lover, celebrity, Blessed Virgin, and, in the words of conservative Theresa Crenshaw (member of the White House AIDS commission), "mainstays in the resistance to this epidemic."
128. Confusion as to innocence and guilt in relation to infection is evident in a 12 April 1987 story in Japan Times , reporting that a baby born to an infected woman did not itself appear to be infected ("Baby Born to AIDS Carrier Infection Free," 2); in an odd sentence construction that appears to separate "the AIDS carrier" from "the mother," the report added that the government's "public health division said that there is little danger that Japan's first baby born to a [AIDS] carrier was infected in the mother's womb." The story indicates that after the infected woman insisted on bearing her child against medical advice, a special medical team was appointed both to reduce the chances that the virus would be transmitted to the baby during delivery and to protect the mother from AIDS; but the story describes only the procedures and rationale for protecting the baby.
129. On "saturation," see Altman, "Heterosexual Fears Allayed."
130. Shilts, Band Played On , 124, reports that scientific papers about pediatric AIDS were rejected in 1982 by scientific and medical journals because of the widespread conception that "by its very name, GRID was a homosexual disease, not a disease of babies or their mothers." Yet even in 1987, when Shilts's book was published and publicized, attention was given to "Patient Zero," a figure of gay sex rampant in the person of a Canadian airline flight attendant who, Shilts suggests—and the media at large appear to have concluded—was the "man who brought us AIDS."
Yet Shilts's account begins in December 1976 with the story of the Danish lesbian physician Grethe Rask, who contracted Pneumocystis carinii pneumonia working in Zaire and died in December 1977; though her case was reported in a letter to The Lancet 2 (1983): 925, by her medical colleague and friend Dr. Ib Bygbjerg, her case has received little attention. For further analysis
of Shilts's book, see Douglas Crimp, "How to Have Promiscuity in an Epidemic," October 43 (1987). (In his letter, Bygbjerg, citing Robin M. Henig's discussion of AIDS as a tropical disease ["AIDS: A New Disease's Deadly Odyssey," New York Times Magazine , 6 February 1983, 28], notes the existence of endemic disease related to three ''acutely deadly viruses of central African origin" as well as Rask's exposure, through her work as a surgeon, to "blood and excretions of African patients"; he suggests possible connections to AIDS and urges investigation by U.S. and European epidemiologists and virologists.)
131. A growing literature documents the placement of gay men in AIDS writing as the Contaminated Other, and there seems evidence that in some respects they do fill the role that women, especially prostitutes, have played in the past. It is not clear what effect AIDS is having on notions of masculinity and femininity in the gay community. Gay men's creation of the term "AIDS widows" to designate the men who survive their lovers is a small but positive use by men of a "feminine" linguistic form. On the other hand, sexism remains entrenched. Ned Weeks, the author's persona in Larry Kramer's play The Normal Heart (New York: Samuel French, 1985), denounces the members of Gay Men's Health Crisis for preferring deathbed scenes over politics: "I thought I was starting a bunch of Ralph Naders or Green Berets, and at the first instant they have to take a stand on a political issue and fight, almost in front of my eyes they turn into a bunch of nurse's aides" (62). Shilts, Band Played On , 556-557, discusses the play but makes no comment on the implicit sexism in lines like these.
In "Taking Responsibility," Kramer charges that gay men's failure to demand their rights "proves they are the sissies people have always accused them of being." Michael Musto, "Mandatory Macho," Village Voice , 30 June 1987, 30, deplores the repressive effect of this compulsory masculinity on the flamboyant drag tradition within gay life. On the general topic of relations among the sexes within the gay community, see Donald Mager, "The Discourse about Homophobia, Male and Female Contexts" (Paper presented at the Annual Meeting of the Modern Language Association, New York, December 1986), and Craig Owens, "Outlaws: Gay Men in Feminism," in Men in Feminism , ed. Alice Jardine and Paul Smith (New York: Methuen, 1987), 219-232.
132. Watney observes that after any media message to heterosexuals, the phone hotlines—still staffed primarily by gay volunteers—are jammed far beyond their capacity by the mainly straight "worried well"; the same thing occurred after a 20 May 1987 front-page story by Robert Pear appeared in the New York Times : "3 Health Care Workers Found Infected by Blood of Patients with AIDS." Wofsy, "HIV Infection in Women," argues that although media representations of AIDS striking middle-class white women provide an important message to be careful, they reinforce the invisibility of, and may thus promote denial among, members of the groups most at risk—black and Hispanic women.
133. No Magic Bullet , following p. 164.
134. Treichler, "Epidemic of Signification," 281-282, 297, n. 28. The tendency of male scientists to keep themselves textually clean is well-documented. Martin, for example, in Woman and the Body , 50, notes that menstruation is commonly described in medical and scientific texts as a form of hemorrhaging,
and menstrual flow as "blood mixed with endometrial debris"; Martin points out that seminal fluid, too, picks up shredded material as it moves through various male ducts but is never characterized by so negative a term as "debris."
135. Various metaphors in AIDS discourse are identified in Hughey, Norton, and Sullivan, "Confronting Danger"; Dobrow, "Symbolism of AIDS"; and Albert, ''AIDS: The Victim and the Press."
136. June E. Osborn, quoted in Clark et al., "Women and AIDS," called intravenous drug users "the great gaping hole in the dike," and compared the spread of the virus through the drug-using community to "dropping red dye into a pond." Turner, Body in Society , 221, writes that "venereal disease is popularly conceptualized as an invasion of the body by alien germs, but the mechanism which, so to speak, opens the sluice-gates permitting nature to invade culture is the deviance of human populations from morality." Other common liquid metaphors about AIDS include waves , pools , islands , oceans , streams , reservoirs , pouring , spilling , and icebergs . Metaphors about liquid appear to flow easily into metaphors about women and disease: drain the red-light district, it was frequently argued in the venereal disease debates, and you drain the swamp (Brandt, No Magic Bullet , 72). Corbin, "Commercial Sexuality," 87, notes that the prostitute was considered to have a body that smelled bad and had rotten blood. One nineteenth-century analogy likened the body to a house and the prostitute to the house's cesspool; more broadly, her body is the sewer into which the social body excretes its excess (as a nineteenth-century physician put it, "the seminal drain"). Prostitutes therefore serve a crucial function in keeping the surrounding countryside clean.
137. These roles are played out most graphically in the supermarket tabloids.
138. The resurgence of discourse on "female promiscuity" raises pressing questions about women's health and women's pleasure. Opening a panel discussion on the erosion of civil rights and affirmative action under Reagan, Betty Friedan pointed to the film Fatal Attraction to suggest a widespread backlash against "liberated" women and the feminist agenda (The Sag Harbor Initiative, Maine, 10-12 October 1987). Gould, "Reassuring News," recycled data and old theories to reassure Cosmo readers that "ordinary sexual intercourse" would not place them at risk for AIDS; as noted above (n. 98), he explains heterosexual AIDS in Africa as the result of rough sexual practices. The inaccuracy, irresponsibility, racism, and sexism of Gould's article provoked ACT-UP to organize an international boycott of the magazine, asking women and men everywhere to "SAY NO TO COSMOPOLITAN." The need for such feminist commentary, activism, and discussion is pressing. Neither the search for safety nor the search for pleasure should be abandoned. As Carole S. Vance has eloquently argued on many occasions, "It is not safe to be a woman, and it never has been. Female attempts to claim pleasure are especially dangerous, attacked not only by men, but by women as well." "Pleasure and Danger," in Pleasure and Danger , ed. Carole S. Vance (New York: Routledge & Kegan Paul, 1984), 1-27.
139. Leslie Kirk Wright reports that in early 1987 a small company introduced a device that enables women to urinate standing up. Advertisements appearing extensively in the MUNI Metro System (and particularly aimed, apparently, at the Financial District crowd) urged women to "Stand UP! for hygiene,"
and showed a smartly (but sedately) dressed woman holding a smallish box suggestive of tampons. Wright suggests to me that, like the condom ads aimed at women, this may reflect an appeal to the "new freedom."
140. Other publications were quick to spread Langone's word. Speaking to audiences and friends (gay and straight, in many cities) who do not stay daily apprised of AIDS developments, I have found Langone's argument still widespread.
141. HIV is believed to be a relative newcomer on earth (the presence of antibodies in stored blood now goes back to 1959 in samples collected in Africa, to 1973 in U.S. blood—though a case in St. Louis in 1968 has recently been verified). Though, from our perspective, the AIDS virus is indeed virulent, killing quickly, in fact, the long latency between infection and the appearance of clinical damage provides plenty of time—often years—for the virus to replicate and infect a new host. For the time being we are sufficiently hospitable so that this virus can live off us relatively "successfully"; if mutation occurs, our relationship to the AIDS virus could evolve into something relatively benign or mutually disastrous.
142. "AIDS," Ms . (April 1987), 64-71. (See, in contrast, Lindsy Van Gelder and Pam Brandt, "AIDS on Campus," Rolling Stone (December 1986), 89-94.
143. For examples of this burgeoning genre, see Mary Cantwell, "Who's Responsible for 'Safe Sex'?" New York Times , 8 July 1987,26, and Anna Quindlen, "For Women, the Condom Campaign Is a Bit Tardy," New York Times , 17 June 1987, 17, 19.
144. Heterosexual white male commentary about AIDS comes from left and right. See Peter Davis, "Exploring the Kingdom of AIDS," and Nat Hentoff, "The New Priesthood of Death" for the former; William F. Buckley, Jr.'s, "Crucial Steps" and other columns on AIDS, and Michael Fumento's articles in Commentary .
145. Peter Goldman, "The Face of AIDS," Newsweek , 10 August 1987, 22-37. Rex Wockner, "Back-door Homophobia," Chicago Outlines (Summer 1987). In contrast, Michael Shnayerson, "One by One," Vanity Fair (April 1987), 91-97, 152-153, uniformly captions each photo with occupation and age only.
146. Chris Norwood, Advice for Life : A Woman ' s Guide to Aids Risks and Prevention (New York: Pantheon, 1987) and Helen Singer Kaplan, The Real Truth about Women and AIDS : How to Eliminate the Risks Without Giving Up Love and Sex (New York: Simon and Schuster, 1987). The two books are similar in their orientation toward white middle-class heterosexual childbearing women, for whom they recommend safe partners over safe practices. Kaplan is less skeptical in her analysis of official sources. For Norwood, one "risk" of AIDS for women is that they will find its name, in those four big capital letters, frightening, so she forswears the acronym in favor of user-friendly Aids .
147. Kaplan, The Real Truth , app. C, 157-164. Kaplan does not provide information about the circumstances of the call.
148. "Women and AIDS," radio program produced in London by the BBC, aired 13 September 1987 in central Illinois.
149. Susan Ardill and Sue O'Sullivan, "AIDS and Women: Building a Feminist Framework," Spare Rib (May 1987), 40-43 (first in a projected series).
150. Increasingly, other voices are demanding a forum for discourse on AIDS. Minority and women's organizations and journals now cover AIDS conferences, and do so vocally. An August 1987 federal conference on AIDS and minorities, for example, provoked nearly 100 of the black delegates to adopt and make public a resolution critical of the level and quality of information made available; as one spokesperson said, "They gave us a lesson in AIDS 101 when all of us traveled here for a graduate course" (Jon Nordheimer, "U.S. Officials Criticized on Efforts to Curb AIDS among Minorities," New York Times , 10 August 1987, 1, 9).
The involvement of intravenous drug users is also beginning. Though as William Check wrote in 1985 ("Public Education on AIDS," 28), that "it sometimes appears that the only risk group that hasn't raised a ruckus is the IV drug users, who are not organized," some organization is now taking place—in New York at any rate. Gay Men's Health Crisis, aware that some drug users may avoid AIDS information centers perceived as gay, as well as medical authorities, has been working with former addicts, who in turn go to "shooting galleries" and other hangouts and teach drug users how to clean needles with bleach.
151. Only a suggestion of this diversification of AIDS discourse can be included here. Dooley Worth and Ruth Rodriguez, "Latina Women and AIDS," Radical America 20 (1987): 63-67, argue that AIDS education and risk reduction for U.S. Hispanics must begin using appropriate cultural forms: "Writers, newscasters, artists, actors, and producers, who successfully reach Latino households through Spanish language radio and television soap operas, 'foto-novelas' (a popular comic-book style depicting romantic stories with photographs), posters, and printed materials, must be tapped in developing an education campaign that is based on a firm understanding of the cultural possibilities for adaptive behavior," 67. Archie Comic Publications, Inc., plans a year-long AIDS education campaign in 1988.
Lisa H. Towle, "Learn to Read with 'Word Warriors,"' New York Times , 31 January 1988, 21. Jaret, "Wars Within," 705, describes a "Killer T-Cell Video Game" for cancer patients. AIDS : You Can ' t Catch It Holding Hands , written and illustrated by Niki de Saint Phalle (San Francisco: Lapis, 1987), is essentially an AIDS education and prevention manual, suitable for kids, with laminated jacket and drawings that are something like a combination of Matisse, subway graffitti, and the Babar books. AIDS is beginning to figure centrally in novels; several that feature women who are infected through heterosexual contact are Joseph Hansen's Early Graves (New York: Mysterious, 1987), Armistead Maupin's Significant Others (New York: Harper & Row, 1987), and Margaret Atwood, The Handmaid ' s Tale (Boston: Houghton Mifflin, 1986).
152. Knowledge about AIDS is being produced, interpreted, and put to use in vastly diverse contexts, and to assume a simple, linear model of communication is not useful. Watney, in "AIDS: The Outsiders," writes that "for those of us living and working in the communities most devastated by AIDS it seems as if the rest of the population are like tourists, wandering casually through the
height of a blitz, totally unaware of what is going on all around them," and, indeed, stumbling through a blitz may be a more useful image when we try to account for the multiplicity of understandings and unpredictable cultural realignments that the AIDS crisis continues to generate. A well-known media researcher, for example, commenting on the unexpected consequences of his own research on AIDS, said, "I never dreamed as a communications scholar I'd be teaching people how to shoot up correctly with heroin" (Annual Meeting, International Communication Association, Chicago, May 1986).
The crisis has created widespread interest, even obsession, with scientific and medical information. Many journals, for example, have provided a short course in virology (Kohn, "Face the Virus"). As a gay composer in New York said to me recently, "Whoever thought I'd be reading about the glucose coatings on viruses and how to interpret T-cell ratios." Meanwhile, however, CDC interviews with members of two heterosexual singles clubs in Minneapolis documented that as of late 1986 this already-infected population had made virtually no modifications in their sexual practices (Centers for Disease Control, "Positive HTLV-III / LAV Antibody Results for Sexually Active Female Members of Social / Sexual Clubs—Minnesota," MMWR 35 (14 November 1986): 697-699. Ralph J. DiClemente, Jim Zorn, and Lydia Temoshok, "Adolescents and AIDS: A Survey of Knowledge, Attitudes and Beliefs about AIDS in San Francisco,'' American Journal of Public Health 76 (1986): 1443-1445, found that many adolescents in San Francisco, a city where public health information about AIDS has been extensive, were not well informed about its seriousness, causes, or prevention.
153. See Simon Watney, "A.I.D.S. U.S.A.," for comments on the noncritical use of AIDS-related terminology among U.S. gay activists.
154. See J. Z. Grover, "A Critique of AIDS Terminology," October 43 (Winter 1987).
155. Models for this kind of attentive questioning, which is at once dense, critically self-conscious, and politically informed, can be found in writing about women and AIDS by Cindy Patton, Donna J. Haraway, and Diane Richardson. Far from being "idealist," it seems to me such questions set the stage for materialist interventions.
156. The following "joke" illustrates a disjunction between women as ideal and socially constructed entities and women as "real people" who are subject to particular historical conditions:
A" guy named Joe was a regular at his neighborhood bar and one night he told his drinking buddies he was going to have sex-change surgery. "I just feel there's a woman inside me," he said, "and I'm going to let her out."
Joe" showed up at the bar a few months later transformed into a woman who introduced herself to her old buddies as Jane. The regulars recognized her, gave their welcomes, bought her a beer, and began asking questions about the surgery.
"What" hurt the most?" they asked. "Was it when they cut your penis?"
"No,"" said Jane, "that wasn't what hurt the most."
"Was" it when they cut your testicles, then?"
"No," that wasn't what hurt the most."
"Well," what was" it" that hurt the most?"
"What" hurt the most was when they cut my salary."
See Christine Brooke-Rose, "Woman as a Semiotic Object," in Female Body in Western Culture , ed. Suleiman, 305-316, and Teresa De Lauretis, Alice Doesn ' t : Feminism , Semiotics , Cinema (Bloomington: Indiana University Press, 1984).
157. Shaw and Paleo, "Women and AIDS," discuss society's view of the preciousness of childbearing women and their likelihood of being among the first groups tested. They cite women's current reluctance, as caretakers in this life-and-death crisis, to raise concerns about sexism.
158. Laurie Stone, "The New Femme Fatale," Ms. (December 1987), 78-79, 79, writes that Fatal Attraction "says good women stay at home . . . while single, working women are damaged, barely even human, and want to destroy the family they secretly covet . . . . This is a fairy tale for the age of AIDS if there ever was one," she concludes, and observes of the pathological femme fatale character that "we're meant to hate her so much we want her dead."